

Identifying Solitary Granulomatous Nodules from Solid Lung Adenocarcinoma: Exploring Robust Image Features with Cross-Domain Transfer Learning
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
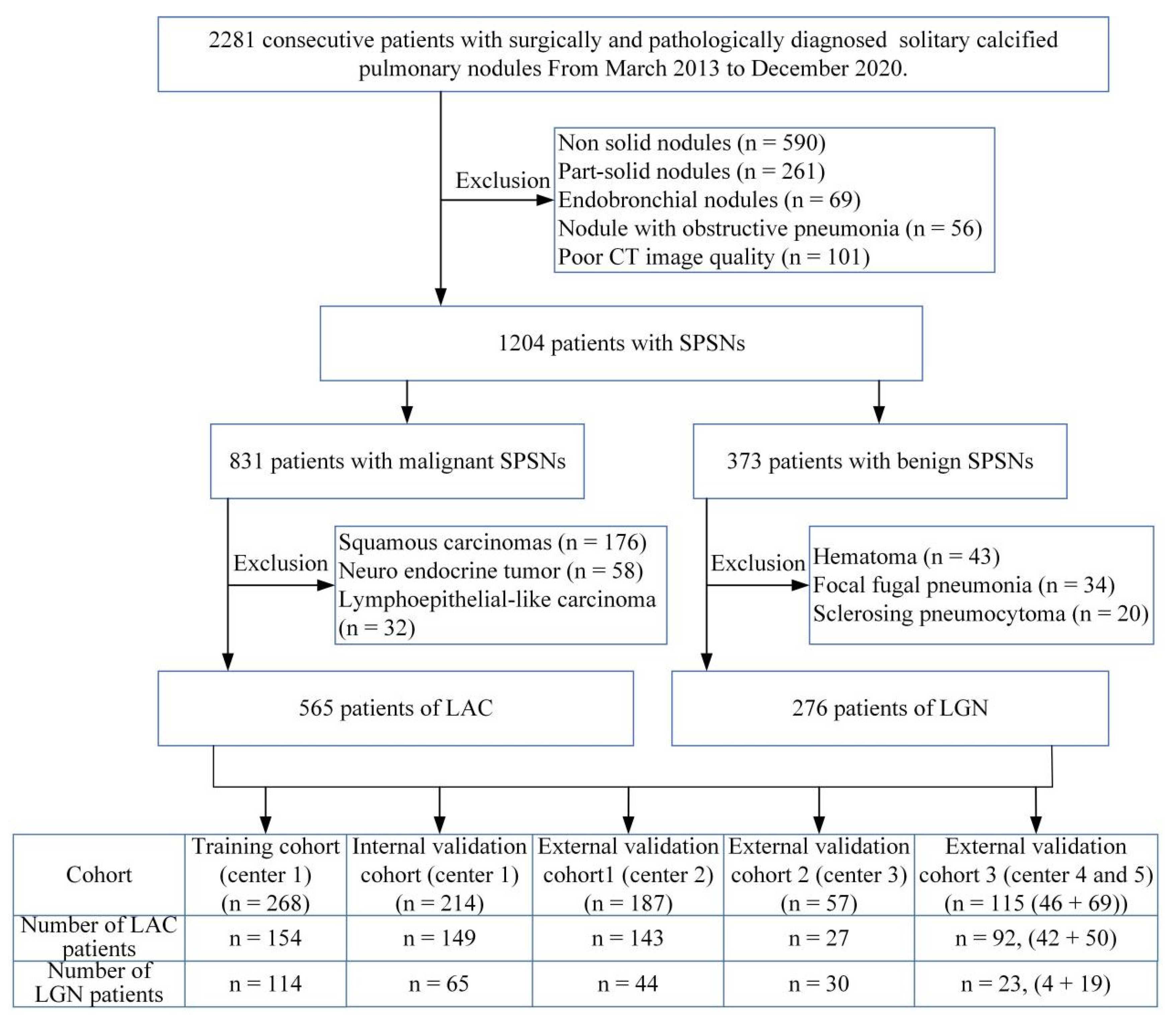
2.1. Patients
2.2. CT Scanning Parameters
2.3. Evaluation of Subjective CT Findings
2.4. Building the Transfer Learning Signature (TLS)
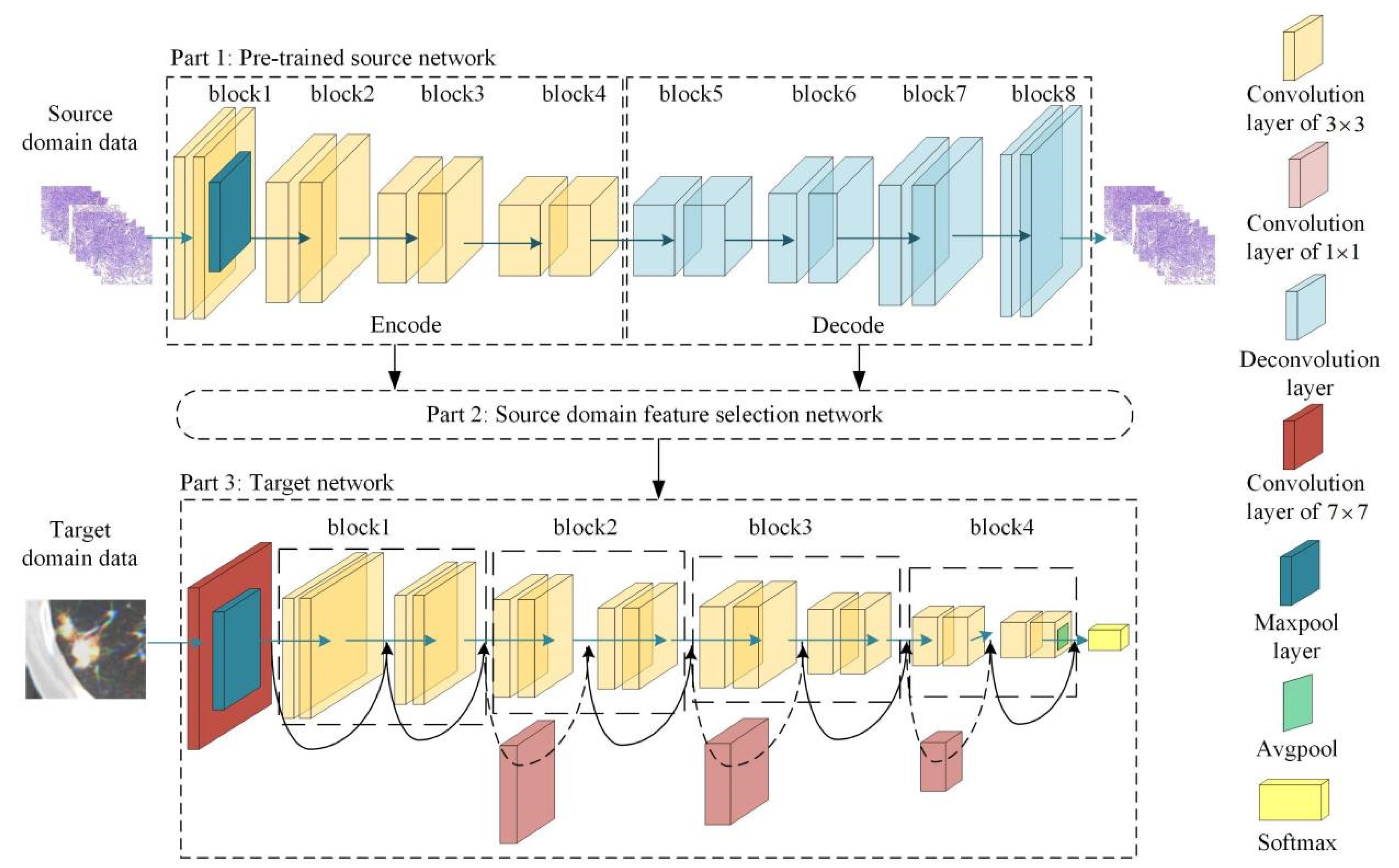
2.4.1. Transfer Learning Feature Extraction Based on an Adaptive Cross-Domain Transfer Learning Model
2.4.2. Building the TLS Based on Transfer Learning Features
2.4.3. TLS Comparison Based on Different Source Domain Data
2.5. Building the TLRM
2.5.1. Building the TLRM
2.5.2. TLRM Evaluation and Comparison
2.6. Prospective Clinical Validation
2.7. Model Evaluation Index
3. Results
3.1. Clinical Factors and Subjective CT Findings Analysis
3.2. Comparison and Selection of TLS Based on Different Source Domain Data
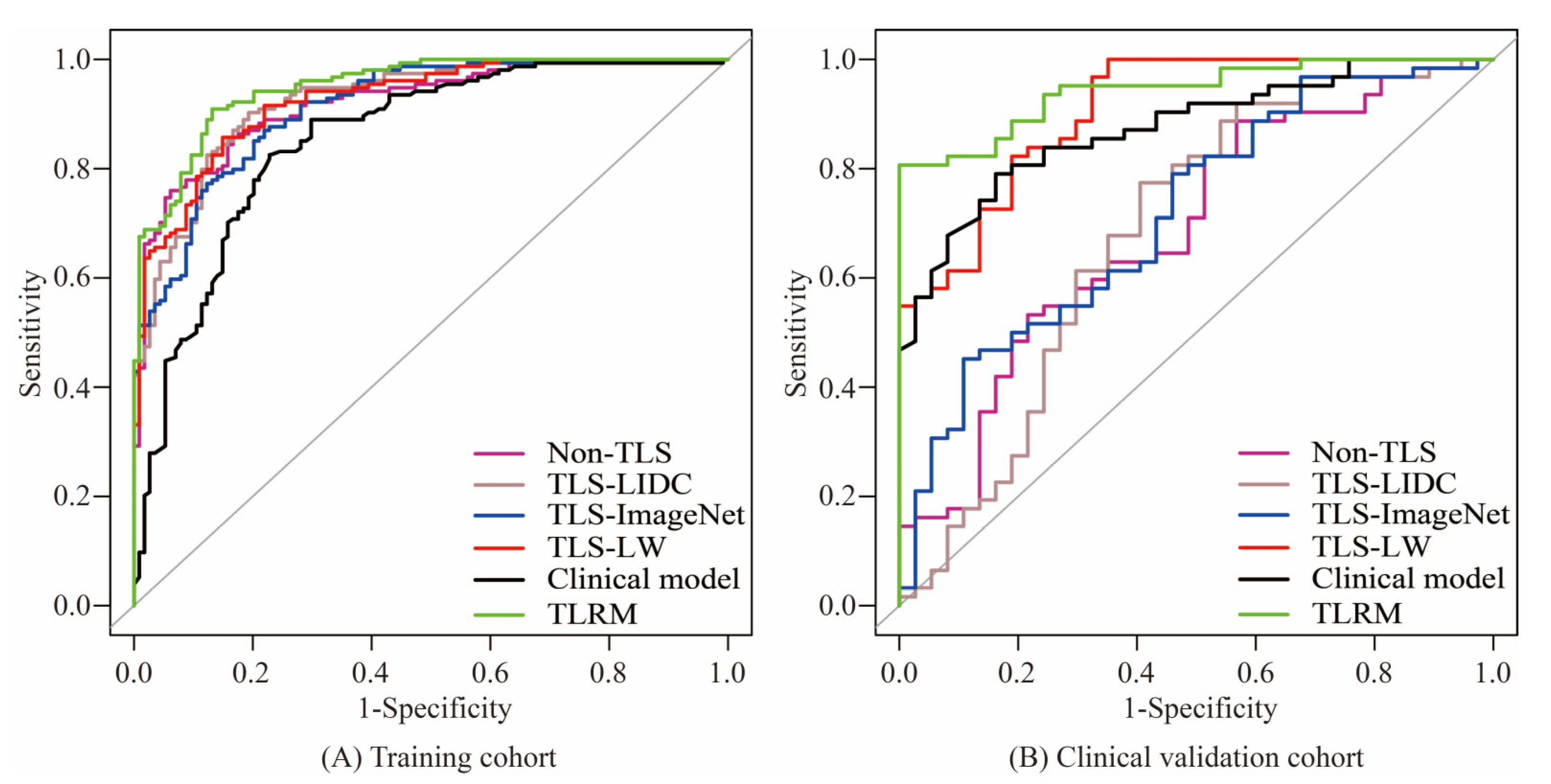
3.2.1. TLS Based on Different Source Domain Data vs. Non-TLS
3.2.2. Comparison and Selection of TLS Based on Different Source Domain Data
3.3. TLRM Construction and Evaluation
3.3.1. TLRM Construction
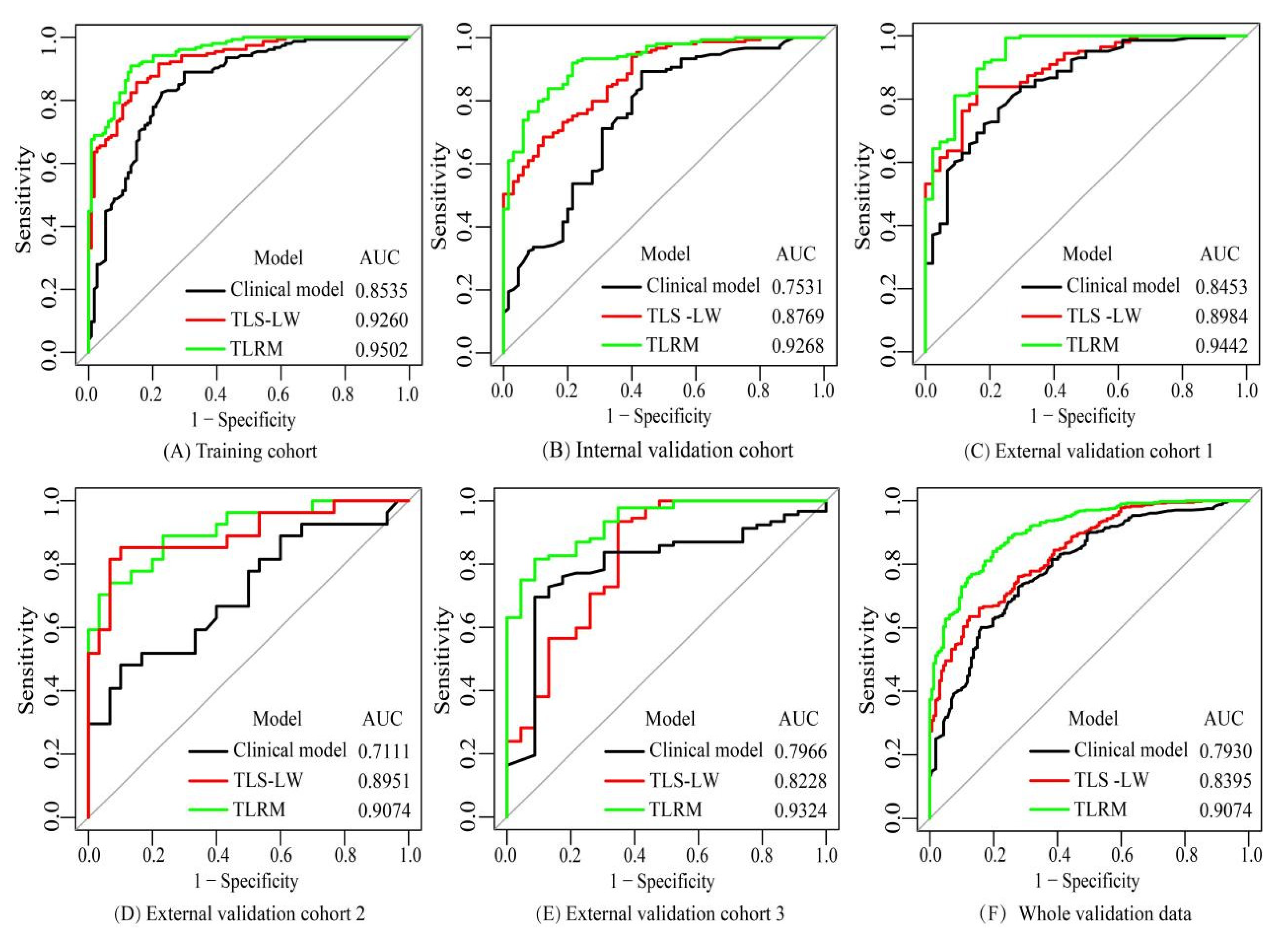
3.3.2. TLRM vs. TLS-LW and Clinical Model
3.3.3. Stratified Analysis of TLRM
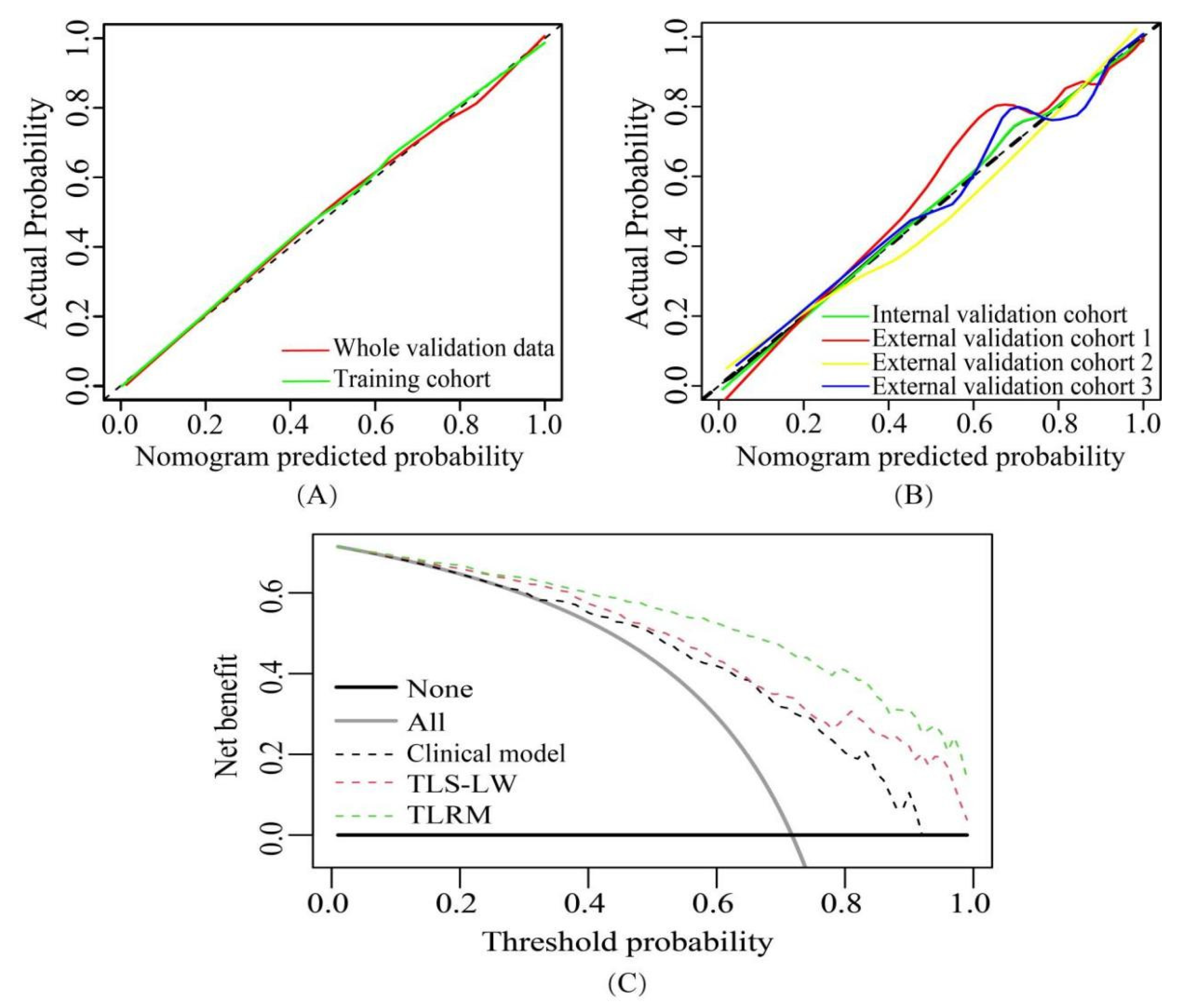
3.3.4. Clinical Use
3.4. Prospective Clinical Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Henschke, C.I.; Salvatore, M.; Cham, M.; Powell, C.A.; DiFabrizio, L.; Flores, R.; Kaufman, A.; Eber, C.; Yip, R.; Yankelevitz, D.; et al. Baseline and annual repeat rounds of screening: Implications for optimal regimens of screening. Eur. Radiol. 2017, 28, 1085–1094. [Google Scholar] [CrossRef] [PubMed]
- Niyonkuru, A.; Chen, X.; Bakari, K.H.; Wimalarathne, D.N.; Bouhari, A.; Arnous, M.M.R.; Lan, X. Evaluation of the diagnostic efficacy of 18 F-Fluorine-2-Deoxy-D-Glucose PET/CT for lung cancer and pulmonary tuberculosis in a Tuberculosis-endemic Country. Cancer Med. 2020, 9, 931–942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dennie, C.; Bayanati, H.; Souza, C.A.; Peterson, R.; Shamji, F.M. Role of the Thoracic Radiologist in the Evaluation and Management of Solid and Subsolid Lung Nodules. Thorac. Surg. Clin. 2021, 31, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Shetty, N.; Noronha, V.; Joshi, A.; Rangarajan, V.; Purandare, N.; Mohapatra, P.R.; Prabhash, K. Diagnostic and Treatment Dilemma of Dual Pathology of Lung Cancer and Disseminated Tuberculosis. J. Clin. Oncol. 2014, 32, e7–e9. [Google Scholar] [CrossRef] [PubMed]
- D’souza, M.M.; Mondal, A.; Sharma, R.; Jaimini, A.; Khanna, U. Tuberculosis the great mimicker: 18F-fludeoxyglucose positron emission tomography/computed tomography in a case of atypical spinal tuberculosis. Indian. J. Nucl. Med. 2014, 29, 99–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starnes, S.L.; Reed, M.F.; Meyer, C.A.; Shipley, R.T.; Jazieh, A.R.; Pina, E.M.; Redmond, K.; Huffman, L.C.; Pandalai, P.K.; Howington, J.A. Can lung cancer screening by computed tomography be effective in areas with endemic histoplasmosis? J. Thorac. Cardiovasc. Surg. 2011, 141, 688–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Riel, S.J.; Sánchez, C.I.; Bankier, A.A.; Naidich, D.P.; Verschakelen, J.; Scholten, E.T.; de Jong, P.A.; Jacobs, C.; van Rikxoort, E.; Peters-Bax, L.; et al. Observer variability for classification of pulmonary nodules on low-dose CT images and its effect on nodule management. Radiology 2015, 277, 863–871. [Google Scholar] [CrossRef]
- Zhang, J.; Han, T.; Ren, J.; Jin, C.; Zhang, M.; Guo, Y. Discriminating Small-Sized (2 cm or Less), Noncalcified, Solitary Pulmonary Tuberculoma and Solid Lung Adenocarcinoma in Tuberculosis-Endemic Areas. Diagnostics 2021, 11, 930. [Google Scholar] [CrossRef]
- Zhuo, Y.; Zhan, Y.; Zhang, Z.; Shan, F.; Shen, J.; Wang, D.; Yu, M. Clinical and CT Radiomics Nomogram for Preoperative Dif-ferentiation of Pulmonary Adenocarcinoma from Tuberculoma in Solitary Solid Nodule. Front. Oncol. 2021, 11, 701598. [Google Scholar] [CrossRef]
- Silver, D.; Schrittwieser, J.; Simonyan, K.; Antonoglou, I.; Huang, A.; Guez, A.; Hubert, T.; Baker, L.; Lai, M.; Bolton, A.; et al. Mastering the game of Go without human knowledge. Nature 2017, 550, 354–359. [Google Scholar] [CrossRef]
- Kann, B.H.; Hosny, A.; Aerts, H.J. Artificial intelligence for clinical oncology. Cancer Cell 2021, 39, 916–927. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; He, J.; Wang, J.; Li, W.; Liu, C.; Gao, D.; Guan, Y. CT-based radiomics signature for differentiating solitary granulomatous nodules from solid lung adenocarcinoma. Lung Cancer 2018, 125, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Yang, J.; Ni, B.; Bi, D.; Sun, Y.; Xu, M.; Li, M. Toward automatic prediction of EGFR mutation status in pulmonary adeno-carcinoma with 3D deep learning. Cancer Med. 2019, 8, 3532–3543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Shi, J.; Ye, Z.; Dong, D.; Yu, D.; Zhou, M.; Liu, Y.; Gevaert, O.; Wang, K.; Zhu, Y.; et al. Predicting EGFR mutation status in lung adenocarcinoma on computed tomography image using deep learning. Eur. Respir. J. 2019, 53, 1800986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashraf, S.F.; Yin, K.; Meng, C.X.; Wang, Q.; Wang, Q.; Pu, J.; Dhupar, R. Predicting benign, preinvasive, and invasive lung nodules on computed tomography scans using machine learning. J. Thorac. Cardiovasc. Surg. 2021, 163, 1496–1505.e10. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.; Huang, L.; Liu, Y.; Chen, Y.; Zhou, H.; Yu, T.; Xue, H.; Chen, Q.; Zhou, T.; Kuang, Q.; et al. A Transfer Learning Radiomics Nomogram for Preoperative Prediction of Borrmann Type IV Gastric Cancer from Primary Gastric Lymphoma. Front. Oncol. 2022, 11. [Google Scholar] [CrossRef]
- Nam, J.G.; Park, S.; Park, C.M.; Jeon, Y.K.; Chung, D.H.; Goo, J.M.; Kim, H. Histopathologic Basis for a Chest CT Deep Learning Survival Prediction Model in Patients with Lung Adenocarcinoma. Radiology 2022, 305, 441–451. [Google Scholar] [CrossRef]
- Ibragimov, B.; Toesca, D.; Chang, D.; Yuan, Y.; Koong, A.; Xing, L. Development of deep neural network for individualized hepa-to-biliary toxicity prediction after liver SBRT. Med. Phys. 2018, 45, 4763–4774. [Google Scholar] [CrossRef]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Kornblith, S.; Shlens, J.; Le, Q.V. Do Better ImageNet Models Transfer Better? arXiv 2019, arXiv:1805.08974. [Google Scholar]
- Raghu, M.; Zhang, C.; Kleinberg, J.; Bengio, S. Transfusion: Understanding Transfer Learning for Medical Imaging. arXiv 2018, arXiv:1902.07208v2. [Google Scholar]
- Romero, M.; Interian, Y.; Solberg, T.; Valdes, G. Targeted transfer learning to improve performance in small medical physics da-tasets. Med. Phys. 2020, 47, 6246–6256. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.; Lee, H.; Hwang, S.J.; Shin, J. Learning What and Where to Transfer. In International Conference on Machine Learning; PMLR: London, UK, 2019. [Google Scholar]
- Liu, Y.; Wang, H.; Li, Q.; McGettigan, M.J.; Balagurunathan, Y.; Garcia, A.L.; Thompson, Z.J.; Heine, J.J.; Ye, Z.; Gillies, R.J.; et al. Radiologic Features of Small Pulmonary Nodules and Lung Cancer Risk in the National Lung Screening Trial: A Nested Case-Control Study. Radiology 2018, 286, 298–306. [Google Scholar] [CrossRef] [Green Version]
- Van Riel, S.J.; Jacobs, C.; Scholten, E.T.; Wittenberg, R.; Winkler Wille, M.M.; de Hoop, B.; Sprengers, R.; Mets, O.M.; Geurts, B.; Prokop, M.; et al. Observer variability for lung-RADS categorisation of lung cancer screening CTs: Impact on patient management. Eur Radiol. 2019, 29, 924–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of Terms for Thoracic Imaging. Radiology 2008, 246, 697–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, T.; Yu, Z.; Gu, Z.; Li, Y. Grouped Automatic Relevance Determination and Its Application in Channel Selection for P300 BCIs. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 1068–1077. [Google Scholar] [CrossRef] [PubMed]
- Panaretos, V.M.; Zemel, Y. Statistical Aspects of Wasserstein Distances. Annu. Rev. Stat. Its Appl. 2019, 6, 405–431. [Google Scholar] [CrossRef] [Green Version]
- Lang, S.; Sun, J.; Wang, X.; Xiao, Y.; Wang, J.; Zhang, M.; Ao, T.; Wang, J. Asymptomatic pulmonary tuberculosis mimicking lung cancer on imaging: A retrospective study. Exp. Ther. Med. 2017, 14, 2180–2188. [Google Scholar] [CrossRef] [Green Version]
- Beig, N.; Khorrami, M.; Alilou, M.; Prasanna, P.; Braman, N.; Orooji, M.; Rakshit, S.; Bera, K.; Rajiah, P.; Ginsberg, J.; et al. Perinodular and Intranodular Radiomic Features on Lung CT Images Distinguish Adenocarcinomas from Granulomas. Radiology 2019, 290, 783–792. [Google Scholar] [CrossRef]
- Yanagawa, M.; Johkoh, T.; Noguchi, M.; Morii, E.; Shintani, Y.; Okumura, M.; Hata, A.; Fujiwara, M.; Honda, O.; Tomiyama, N. Radio-logical prediction of tumor invasiveness of lung adenocarcinoma on thin-section CT. Medicine 2017, 96, e6331. [Google Scholar] [CrossRef] [Green Version]
- Hawkins, S.; Wang, H.; Liu, Y.; Garcia, A.; Stringfield, O.; Krewer, H.; Li, Q.; Cherezov, D.; Gatenby, R.A.; Balagurunathan, Y.; et al. Predicting Malignant Nodules from Screening CT Scans. J. Thorac. Oncol. 2016, 11, 2120–2128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azour, L.; Ko, J.P.; Washer, S.L.; Lanier, A.; Brusca-Augello, G.; Alpert, J.B.; Moore, W.H. Incidental Lung Nodules on Cross-sectional Imaging Current Reporting and Management. Radiol. Clin. North Am. 2021, 59, 535–549. [Google Scholar] [CrossRef]
- He, K.; Girshick, R.; Dollar, P. Rethinking ImageNet Pre-Training. In Proceedings of the 2019 IEEE/CVF International Conference on Computer Vision (ICCV), Seoul, Republic of Korea, 27 October–2 November 2019; IEEE: Manhattan, NY, USA, 2019; pp. 4917–4926. [Google Scholar]
- Hashimoto, K.; Nishimura, S.; Akagi, M. Lung Adenocarcinoma Presenting as a Soft Tissue Metastasis to the Shoulder: A Case Report. Medicina 2021, 57, 181. [Google Scholar] [CrossRef] [PubMed]
- McKee, B.J.; Regis, S.M.; McKee, A.B.; Flacke, S.; Wald, C. Performance of ACR LungRADS in a Clinical CT Lung Screening Program. J. Am. Coll. Radiol. 2015, 12, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambillam, E.; Burke, A.P.; Marx, A.; Nicholson, A.G. Who Classification of Tumours of the Lung, Pleura, Thymus and Heart; IARC Press: Lyon, France, 2015; pp. 26–48. ISBN 9283224361. [Google Scholar]
- Romero, A.; Ballas, N.; Kahou, S.E.; Chassang, A.; Gatta, C.; Bengio, Y. FitNets: Hints for Thin Deep Nets. arXiv 2015, arXiv:1412.6550. [Google Scholar]
- Krizhevsky, A.; Hinton, G. Convolutional Deep Belief Networks on cifar-10. 2010. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwj35Y2Y5NL8AhVQDewKHesdBV4QFnoECAsQAQ&url=https%3A%2F%2Fwww.cs.toronto.edu%2F~kriz%2Fconv-cifar10-aug2010.pdf&usg=AOvVaw36AzS-_kdTFXs9D5M5k87C (accessed on 1 November 2022).
- Kingma, D.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Kotikalapudi, R. keras-vis. GitHub. 2017. Available online: https://github.com/raghakot/keras-vis (accessed on 1 November 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Cohort (n = 268) | Internal Validation Cohort (n = 214) | External Validation Cohort 1 (n = 187) | External Validation Cohort 2 (n = 57) | External Validation Cohort 3 (n = 115) | Whole Validation Data (n = 573) | |
|---|---|---|---|---|---|---|
| CT scan time | January 2014 to May 2018 | June 2018 to September 2020 | January 2015 to December 2018 | May 2018 to December 2020 | March 2013 to August 2019 | March 2013 to December 2020 |
| Pathological type | ||||||
| LGN | 114 | 65 | 44 | 30 | 23 | 162 |
| LAC | 154 | 149 | 143 | 27 | 92 | 411 |
| Gender | ||||||
| Men | 129 | 122 | 90 | 29 | 62 | 303 |
| Women | 139 | 92 | 97 | 28 | 53 | 270 |
| Age (mean ± SD, years) | 55.75 ± 12.49 | 58.54 ± 11.72 | 58.38 ± 10.78 | 56.37 ± 11.57 | 58.34 ± 9.98 | 58.23 ± 11.06 |
| Age range (years) | 20–81 | 16–79 | 28–80 | 31–79 | 27–75 | 16–80 |
| Training Cohort (n = 268) | Internal Validation Cohort (n = 214) | External Validation Cohort 1 (n = 187) | |||||||
| LGN (114) | LAC (154) | p Value | LGN (65) | LAC (149) | p Value | LGN (44) | LAC (143) | p Value | |
| Gender | |||||||||
| Men | 64 | 65 | 0.0240 * | 48 | 74 | 0.0010 * | 28 | 62 | 0.0186 * |
| Women | 50 | 89 | 17 | 75 | 16 | 81 | |||
| Age (mean ± SD, years) | |||||||||
| 50.96 ± 13.16 | 59.29 ± 10.70 | <0.0001 # | 51.66 ± 12.65 | 61.54 ± 9.94 | <0.0001 # | 56.20 ± 11.73 | 59.05 ± 10.31 | 0.1176 # | |
| Nodule size (mean ± SD, mm) | |||||||||
| 13.07 ± 8.00 | 17.31 ± 8.40 | <0.0001 # | 12.05 ± 5.30 | 17.79 ± 8.57 | <0.0001 # | 13.56 ± 8.11 | 21.74 ± 8.57 | <0.0001 # | |
| Location | |||||||||
| LUL | 27 | 44 | 0.0811 * | 21 | 38 | 0.2682 * | 10 | 35 | 0.6573 & |
| LLL | 14 | 33 | 5 | 28 | 8 | 22 | |||
| RUL | 35 | 45 | 21 | 48 | 12 | 52 | |||
| RML | 11 | 12 | 5 | 13 | 4 | 13 | |||
| RLL | 27 | 20 | 13 | 22 | 10 | 21 | |||
| Margin | |||||||||
| Irregular | 64 | 133 | <0.0001 * | 33 | 129 | <0.0001 * | 25 | 135 | <0.0001 * |
| Regular | 50 | 21 | 32 | 20 | 19 | 8 | |||
| Lobulated shape | |||||||||
| Absence | 67 | 23 | <0.0001 * | 38 | 27 | <0.0001 * | 32 | 18 | <0.0001* |
| Presence | 47 | 131 | 27 | 122 | 12 | 125 | |||
| Spiculated sign | |||||||||
| Absence | 100 | 74 | <0.0001 * | 53 | 83 | 0.0003 * | 40 | 73 | 0.0005 * |
| Presence | 14 | 80 | 12 | 66 | 4 | 70 | |||
| External Validation Cohort 2 (n = 57) | External Validation Cohort 3 (n = 115) | Whole Validation Data (n = 573) | |||||||
| LGN (30) | LAC (27) | p Value | LGN (23) | LAC (92) | p Value | LGN (162) | LAC (411) | p Value | |
| Gender | |||||||||
| Men | 14 | 15 | 0.5027 * | 12 | 50 | 0.8516 * | 102 | 201 | 0.0024 * |
| Women | 16 | 12 | 11 | 42 | 60 | 210 | |||
| Age (mean ± SD, years) | |||||||||
| 51.53 ± 10.54 | 61.74 ± 10.37 | <0.0001 # | 55.52 ± 10.99 | 59.04 ± 9.65 | 0.1436 # | 53.42 ± 11.99 | 60.13 ± 10.08 | <0.0001 # | |
| Nodule size (mean ± SD, mm) | |||||||||
| 8.54 ± 4.07 | 18.14 ± 6.80 | <0.0001 # | 16.52 ± 6.61 | 17.33 ± 5.56 | 0.3311 # | 12.45 ± 6.66 | 18.91 ± 7.65 | <0.0001 # | |
| Location | |||||||||
| LUL | 6 | 5 | 0.3856 & | 6 | 25 | 0.9844 & | 43 | 103 | 0.3856 * |
| LLL | 5 | 5 | 4 | 12 | 22 | 67 | |||
| RUL | 6 | 9 | 6 | 24 | 45 | 133 | |||
| RML | 5 | 6 | 2 | 11 | 16 | 43 | |||
| RLL | 8 | 2 | 5 | 20 | 36 | 65 | |||
| Margin | |||||||||
| Irregular | 16 | 26 | 0.0002 * | 19 | 82 | 0.4747 & | 93 | 372 | <0.0001 * |
| Regular | 14 | 1 | 4 | 10 | 69 | 39 | |||
| Lobulated shape | |||||||||
| Absence | 20 | 8 | 0.0052 * | 9 | 7 | 0.0005 & | 99 | 60 | <0.0001 * |
| Presence | 10 | 19 | 14 | 85 | 63 | 351 | |||
| Spiculated sign | |||||||||
| Absence | 21 | 15 | 0.2590 * | 19 | 28 | <0.0001 * | 133 | 199 | <0.0001 * |
| Presence | 9 | 12 | 4 | 64 | 29 | 212 | |||
| Clinical Validation Cohort (n = 99) | |||||||||
| LGN (37) | LAC (62) | p Value | |||||||
| Gender | |||||||||
| Men | 25 | 29 | 0.0444 * | ||||||
| Women | 12 | 33 | |||||||
| Age (mean ± SD, years) | |||||||||
| 55.03 ± 10.32 | 60.76 ± 10.90 | 0.0103 # | |||||||
| Nodule size (mean ± SD, mm) | |||||||||
| 12.73 ± 5.72 | 16.11 ± 6.16 | 0.0048 # | |||||||
| Location | |||||||||
| LUL | 6 | 13 | 0.9734 * | ||||||
| LLL | 5 | 7 | |||||||
| RUL | 13 | 20 | |||||||
| RML | 3 | 6 | |||||||
| RLL | 10 | 16 | |||||||
| Margin | |||||||||
| Irregular | 21 | 52 | 0.0030 * | ||||||
| Regular | 16 | 10 | |||||||
| Lobulated shape | |||||||||
| Absence | 20 | 18 | 0.0133 * | ||||||
| Presence | 17 | 44 | |||||||
| Spiculated sign | |||||||||
| Absence | 30 | 6 | <0.0001 * | ||||||
| Presence | 7 | 56 | |||||||
| Dataset | Models | AUC (95% CI) | Sensitivity | Specificity | Accuracy | PPV | NPV |
|---|---|---|---|---|---|---|---|
| Training cohort (n = 268) | Non-TLS | 0.9216 (0.8906–0.9526) | 0.7597 (117/154) | 0.9386 (107/114) | 0.8358 (224/268) | 0.9435 (117/124) | 0.7431 (107/144) |
| TLS-LIDC | 0.9245 (0.8941–0.9549) | 0.9026 (139/154) | 0.8070 (92/114) | 0.8619 (231/268) | 0.8634 (139/161) | 0.8598 (92/107) | |
| TLS-ImageNet | 0.9136 (0.8814–0.9458) | 0.8701 (134/154) | 0.7807 (89/114) | 0.8321 (223/268) | 0.8428 (134/159) | 0.8165 (89/109) | |
| TLS-LW | 0.9260 (0.8964–0.9556) | 0.8571 (132/154) | 0.8509 (97/114) | 0.8545 (229/268) | 0.8859 (132/149) | 0.8151 (97/119) | |
| Internal validation cohort (n = 214) | Non-TLS | 0.7949 (0.7295–0.8604) | 0.7315 (109/149) | 0.7846 (51/65) | 0.7477 (160/214) | 0.8862 (109/123) | 0.5604 (51/91) |
| TLS-LIDC | 0.7740 (0.7048–0.8431) | 0.6980 (104/149) | 0.7385 (48/65) | 0.7130 (152/214) | 0.8595 (108/121) | 0.5161 (48/93) | |
| TLS-ImageNet | 0.8050 (0.7440–0.8659) | 0.7450 (111/149) | 0.7385 (48/65) | 0.7430 (159/214) | 0.8672 (111/128) | 0.5581 (48/86) | |
| TLS-LW | 0.8769 (0.8308–0.9231) | 0.6846 (102/149) | 0.8769 (57/65) | 0.7430 (159/214) | 0.9273 (102/110) | 0.5481 (57/104) | |
| External validation cohort 1 (n = 187) | Non-TLS | 0.6465 (0.5458–0.7472) | 0.9021 (129/143) | 0.4091 (18/44) | 0.7861 (147/187) | 0.8323 (129/155) | 0.5625 (18/32) |
| TLS-LIDC | 0.7972 (0.7195–0.8749) | 0.8182 (117/143) | 0.7045 (31/44) | 0.7914 (148/187) | 0.9000 (117/130) | 0.5439 (31/57) | |
| TLS-ImageNet | 0.7600 (0.6756–0.8445) | 0.6084 (87/143) | 0.8409 (37/44) | 0.6631 (124/187) | 0.9255 (87/94) | 0.3987 (37/93) | |
| TLS-LW | 0.8984 (0.8519–0.9450) | 0.8392 (120/143) | 0.8409 (37/44) | 0.8396 (157/187) | 0.9449 (120/127) | 0.6167 (37/60) | |
| External validation cohort 2 (n = 57) | Non-TLS | 0.8123 (0.7029–0.9218) | 0.7778 (21/27) | 0.7667 (23/30) | 0.7719 (44/57) | 0.7500 (21/28) | 0.7931 (23/29) |
| TLS-LIDC | 0.6778 (0.5390–0.8166) | 0.6667 (18/27) | 0.6333 (19/30) | 0.6491 (37/57) | 0.6207 (18/29) | 0.6786 (19/28) | |
| TLS-ImageNet | 0.7519 (0.6236–0.8801) | 0.5556 (15/27) | 0.8667 (26/30) | 0.7193 (41/57) | 0.7895 (15/19) | 0.6842 (26/38) | |
| TLS-LW | 0.8951 (0.8085–0.9816) | 0.8519 (23/27) | 0.9000 (27/30) | 0.8772 (50/57) | 0.8846 (23/26) | 0.8710 (27/31) | |
| External validation cohort 3 (n = 115) | Non-TLS | 0.6541 (0.5276–0.7805) | 0.8804 (81/92) | 0.3913 (9/23) | 0.7826 (90/115) | 0.8526 (81/95) | 0.4500 (9/20) |
| TLS-LIDC | 0.5416 (0.4257–0.6574) | 0.2609 (24/92) | 0.9565 (22/23) | 0.4000 (46/115) | 0.9600 (24/25) | 0.2444 (22/90) | |
| TLS-ImageNet | 0.7902 (0.6942–0.8862) | 0.6196 (57/92) | 0.8696 (20/23) | 0.6696 (77/115) | 0.9500 (57/60) | 0.3636 (20/55) | |
| TLS-LW | 0.8228 (0.7150–0.9306) | 0.9348 (86/92) | 0.6522 (15/23) | 0.8783 (101/115) | 0.9149 (86/94) | 0.7143 (15/21) | |
| Whole validation data (n = 573) | Non-TLS | 0.7156 (0.6687–0.7625) | 0.8273 (340/411) | 0.6235 (101/162) | 0.7696 (441/573) | 0.8479 (340/401) | 0.5872 (101/172) |
| TLS-LIDC | 0.7030 (0.6569–0.7491) | 0.6399 (263/411) | 0.7407 (120/162) | 0.6684 (383/573) | 0.8623 (263/305) | 0.4478 (120/268) | |
| TLS-ImageNet | 0.7755 (0.7374–0.8167) | 0.6569 (270/411) | 0.8086 (131/162) | 0.6998 (401/573) | 0.8970 (270/301) | 0.4816 (131/272) | |
| TLS-LW | 0.8395 (0.8058–0.8732) | 0.8054 (331/411) | 0.8395 (136/162) | 0.8168 (468/573) | 0.9272 (331/357) | 0.6296 (136/216) | |
| Clinical validation cohort (n = 99) | Non-TLS | 0.6866 (0.5770–0.7961) | 0.8871 (55/62) | 0.4324 (16/37) | 0.7172 (71/99) | 0.7237 (55/76) | 0.6957 (16/23) |
| TLS-LIDC | 0.6844 (0.5662–0.8026) | 0.7742 (48/62) | 0.5946 (22/37) | 0.7071 (70/99) | 0.7619 (48/63) | 0.6111 (22/36) | |
| TLS-ImageNet | 0.7162 (0.6118–0.8207) | 0.4516 (28/62) | 0.8919 (33/37) | 0.6162 (61/99) | 0.8750 (28/32) | 0.4925 (33/67) | |
| TLS-LW | 0.9076 (0.8503–0.9649) | 1 (62/62) | 0.6486 (24/37) | 0.8687 (86/99) | 0.8267 (62/75) | 1 (24/24) |
| Dataset | Models | AUC (95% CI) | Sensitivity | Specificity | Accuracy | PPV | NPV |
|---|---|---|---|---|---|---|---|
| Training cohort (n = 268) | Clinical model | 0.8535 (0.8066–0.9004) | 0.8247 (127/154) | 0.7719 (88/114) | 0.8022 (215/268) | 0.8301 (127/153) | 0.7652 (88/115) |
| TLS-LW | 0.9260 (0.8964–0.9556) | 0.8571 (132/154) | 0.8509 (97/114) | 0.8545 (229/268) | 0.8859 (132/149) | 0.8151 (97/119) | |
| TLRM | 0.9502 (0.9274–0.9731) | 0.9091 (140/154) | 0.8684 (99/114) | 0.8918 (239/268) | 0.9032 (140/155) | 0.8761 (99/113) | |
| Internal validation cohort (n = 214) | Clinical model | 0.7531 (0.6798–0.8263) | 0.8926 (133/149) | 0.5692 (37/65) | 0.7944 (170/214) | 0.8261 (133/161) | 0.6981 (37/53) |
| TLS-LW | 0.8769 (0.8308–0.9231) | 0.6846 (102/149) | 0.8769 (57/65) | 0.7430 (159/214) | 0.9273 (102/110) | 0.5481 (57/104) | |
| TLRM | 0.9268 (0.8923–0.9613) | 0.9195 (137/149) | 0.7846 (51/65) | 0.8785 (188/214) | 0.9073 (137/151) | 0.8095 (51/63) | |
| External validation cohort 1 (n = 187) | Clinical model | 0.8543 (0.7926–0.9160) | 0.8392 (120/143) | 0.7045 (31/44) | 0.8075 (151/187) | 0.9023 (120/133) | 0.5741 (31/54) |
| TLS-LW | 0.8984 (0.8519–0.9450) | 0.8392 (120/143) | 0.8409 (37/44) | 0.8396 (157/187) | 0.9449 (120/127) | 0.6167 (37/60) | |
| TLRM | 0.9442 (0.9067–0.9817) | 0.9930 (142/143) | 0.7500 (33/44) | 0.9358 (175/187) | 0.9281 (142/153) | 0.9706 (33/34) | |
| External validation cohort 2 (n = 57) | Clinical model | 0.7111 (0.5755–0.8467) | 0.4815 (13/27) | 0.9000 (27/30) | 0.7018 (40/57) | 0.8125 (13/16) | 0.6585 (27/41) |
| TLS-LW | 0.8951 (0.8085–0.9816) | 0.8519 (23/27) | 0.9000 (27/30) | 0.8772 (50/57) | 0.8846 (23/26) | 0.8710 (27/31) | |
| TLRM | 0.9074 (0.8314–0.9834) | 0.7407 (20/27) | 0.9333 (28/30) | 0.8421 (48/57) | 0.9091 (20/22) | 0.8000 (28/35) | |
| External validation cohort 3 (n = 115) | Clinical model | 0.7966 (0.6962–0.8969) | 0.6957 (64/92) | 0.9130 (21/23) | 0.7391 (85/115) | 0.9697 (64/66) | 0.4286 (21/49) |
| TLS-LW | 0.8228 (0.7150–0.9306) | 0.9348 (86/92) | 0.6522 (15/23) | 0.8783 (101/115) | 0.9149 (86/94) | 0.7143 (15/21) | |
| TLRM | 0.9324 (0.8839–0.9809) | 0.8152 (75/92) | 0.9130 (21/23) | 0.8348 (96/115) | 0.9740 (75/77) | 0.5526 (21/38) | |
| Whole validation data (n = 573) | Clinical model | 0.7930 (0.7529–0.8332) | 0.8029 (330/411) | 0.7160 (116/162) | 0.7784 (446/573) | 0.8777 (330/376) | 0.5888 (116/197) |
| TLS-LW | 0.8395 (0.8058–0.8732) | 0.8054 (331/411) | 0.8395 (136/162) | 0.8168 (468/573) | 0.9272 (331/357) | 0.6296 (136/216) | |
| TLRM | 0.9074 (0.8825–0.9324) | 0.9100 (374/411) | 0.8210 (133/162) | 0.8848 (507/573) | 0.9280 (374/403) | 0.7824 (133/170) | |
| Clinical validation cohort (n = 99) | Clinical model | 0.8745 (0.8079–0.9410) | 0.7903 (49/62) | 0.8378 (31/37) | 0.8081 (80/99) | 0.8909 (49/55) | 0.7045 (31/44) |
| TLS-LW | 0.9076 (0.8503–0.9649) | 1 (62/62) | 0.6486 (24/37) | 0.8687 (86/99) | 0.8267 (62/75) | 1 (24/24) | |
| TLRM | 0.9429 (0.9016–0.9842) | 0.8065 (50/62) | 1 (37/37) | 0.8788 (87/99) | 1 (50/50) | 0.4551 (37/49) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, B.; Chen, X.; Chen, Y.; Yu, T.; Duan, X.; Liu, K.; Li, K.; Liu, Z.; Lin, H.; Li, S.; et al. Identifying Solitary Granulomatous Nodules from Solid Lung Adenocarcinoma: Exploring Robust Image Features with Cross-Domain Transfer Learning. Cancers 2023, 15, 892. https://doi.org/10.3390/cancers15030892
Feng B, Chen X, Chen Y, Yu T, Duan X, Liu K, Li K, Liu Z, Lin H, Li S, et al. Identifying Solitary Granulomatous Nodules from Solid Lung Adenocarcinoma: Exploring Robust Image Features with Cross-Domain Transfer Learning. Cancers. 2023; 15(3):892. https://doi.org/10.3390/cancers15030892
Chicago/Turabian StyleFeng, Bao, Xiangmeng Chen, Yehang Chen, Tianyou Yu, Xiaobei Duan, Kunfeng Liu, Kunwei Li, Zaiyi Liu, Huan Lin, Sheng Li, and et al. 2023. "Identifying Solitary Granulomatous Nodules from Solid Lung Adenocarcinoma: Exploring Robust Image Features with Cross-Domain Transfer Learning" Cancers 15, no. 3: 892. https://doi.org/10.3390/cancers15030892