

Systemic Oncological Treatments versus Supportive Care for Patients with Advanced Hepatobiliary Cancers: An Overview of Systematic Reviews
 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Criteria for Considering Reviews for Inclusion
2.1.1. Types of Studies
2.1.2. Types of Patients
2.1.3. Types of Interventions and Comparators
2.1.4. Type of Outcomes
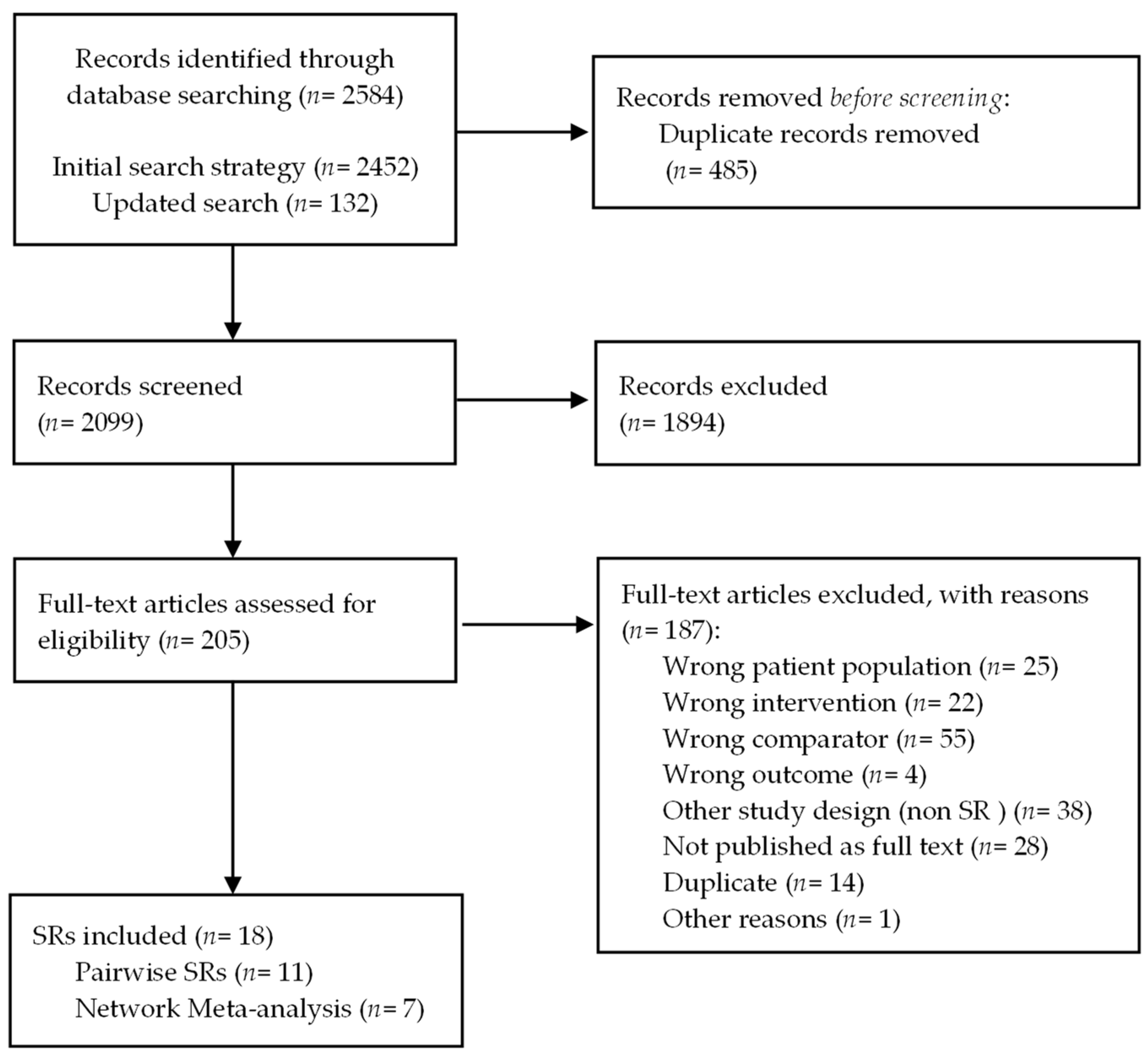
2.1.5. Search Methods and Selection of Studies
2.2. Data Extraction and Analysis
3. Results
3.1. Description of Included Reviews
3.2. Methodological Quality of the Included Reviews
3.3. Overlap Analysis
3.4. Effects of Interventions
3.4.1. Advanced Hepatocellular Carcinoma
SOTs as First-Line Therapy versus Placebo/UPSC
SOTs as Second-Line Therapy or More versus Placebo/UPSC
3.4.2. Advanced Gallbladder Cancer
SOTs versus Placebo/UPSC for Advanced Gallbladder Cancer
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benson, A.B.; D’Angelica, M.I.; Abbott, D.E.; Anaya, D.A.; Anders, R.; Are, C.; Bachini, M.; Borad, M.; Brown, D.; Burgoyne, A.; et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 541–565. [Google Scholar] [CrossRef]
- El-Serag, H.B. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 2012, 142, 1264–1273.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Pan, G.; Guan, L.; Liu, Z.; Wu, Y.; Liu, Z.; Lu, W.; Li, S.; Xu, H.; Ouyang, G. The burden of primary liver cancer caused by specific etiologies from 1990 to 2019 at the global, regional, and national levels. Cancer Med. 2022, 11, 1357–1370. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Yan, L.; Liu, Y.; Qu, C.; Ni, J.; Li, H. The burden and trends of primary liver cancer caused by specific etiologies from 1990 to 2017 at the global, regional, national, age, and sex level results from the global burden of disease study 2017. Liver Cancer 2020, 9, 563–582. [Google Scholar] [CrossRef] [PubMed]
- Janevska, D.; Chaloska-Ivanova, V.; Janevski, V. Hepatocellular carcinoma: Risk factors, diagnosis and treatment. Open Access Maced. J. Med. Sci. 2015, 3, 732–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020. Available online: https://gco.iarc.fr/today (accessed on 9 November 2022).
- Surveillance Research Program, National Cancer Institute. SEER*Explorer: An Interactive Website for SEER Cancer Statistics. Available online: https://seer.cancer.gov/statistics-network/explorer/ (accessed on 9 November 2022).
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M. SEER Cancer Statistics Review, 1975–2016. National Cancer Institute. Available online: https://seer.cancer.gov/archive/csr/1975_2016/ (accessed on 15 March 2022).
- Gordan, J.D.; Kennedy, E.B.; Abou-Alfa, G.K.; Beg, M.S.; Brower, S.T.; Gade, T.P.; Goff, L.; Gupta, S.; Guy, J.; Harris, W.P.; et al. Systemic therapy for advanced hepatocellular carcinoma: ASCO guideline. J. Clin. Oncol. 2020, 38, 4317–4345. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D.; ESMO Guidelines Committee. Biliary cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27 (Suppl. S5), v28–v37. [Google Scholar] [CrossRef]
- Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.M.; Meyer, T.; Nault, J.C.; Neumann, U.; Ricke, J.; Sangro, B.; et al. Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. S4), iv238–iv255. [Google Scholar] [CrossRef]
- Zerillo, J.A.; Schouwenburg, M.G.; van Bommel, A.C.M.; Stowell, C.; Lippa, J.; Bauer, D.; Berger, A.M.; Boland, G.; Borras, J.M.; Buss, M.K.; et al. An international collaborative standardizing a comprehensive patient-centered outcomes measurement set for colorectal cancer. JAMA Oncol. 2017, 3, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Nooruddin, Z.; Didwaniya, N.; Dev, R.; De La Cruz, M.; Kim, S.H.; Kwon, J.H.; Hutchins, R.; Liem, C.; Bruera, E. Concepts and definitions for “actively dying,” “end of life,” “terminally ill,” “terminal care,” and “transition of care”: A systematic review. J. Pain Symptom Manag. 2013, 47, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Dalal, S.; Bruera, E. End-of-life care matters: Palliative cancer care results in better care and lower costs. Oncologist 2017, 22, 361–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martín-Martín, J.; Pérez-Díez-Del-Corral, M.; Olano-Lizarraga, M.; Valencia-Gil, S.; Saracíbar-Razquin, M.I. Family narratives about providing end-of-life care at home. J. Fam. Nurs. 2022, 28, 17–30. [Google Scholar] [CrossRef]
- Mossman, B.; Perry, L.M.; Walsh, L.E.; Gerhart, J.; Malhotra, S.; Horswell, R.; Chu, S.; Raines, A.M.; Lefante, J.; Blais, C.M.; et al. Anxiety, depression, and end-of-life care utilization in adults with metastatic cancer. Psychooncology 2021, 30, 1876–1883. [Google Scholar] [CrossRef]
- PDQ Supportive and Palliative Care Editorial Board. Planning the transition to end-of-life care in advanced cancer (PDQ®): Health professional version. In PDQ Cancer Information Summaries; National Cancer Institute: Bethesda, MD, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/pubmed/26389513 (accessed on 9 November 2022).
- Colombet, I.; Bouleuc, C.; Piolot, A.; Vilfaillot, A.; Jaulmes, H.; Voisin-Saltiel, S.; Goldwasser, F.; Vinant, P.; EFIQUAVIE Study Group. Multicentre analysis of intensity of care at the end-of-life in patients with advanced cancer, combining health administrative data with hospital records: Variations in practice call for routine quality evaluation. BMC Palliat. Care 2019, 18, 35. [Google Scholar] [CrossRef]
- Earle, C.C.; Landrum, M.B.; Souza, J.M.; Neville, B.A.; Weeks, J.C.; Ayanian, J.Z. Aggressiveness of cancer care near the end of life: Is it a quality-of-care issue? J. Clin. Oncol. 2008, 26, 3860–3866. [Google Scholar] [CrossRef] [Green Version]
- Henson, L.A.; Gomes, B.; Koffman, J.; Daveson, B.A.; Higginson, I.J.; Gao, W.; BuildCARE. Factors associated with aggressive end of life cancer care. Support. Care Cancer 2015, 24, 1079–1089. [Google Scholar] [CrossRef] [Green Version]
- Khaki, A.R.; Chennupati, S.; Fedorenko, C.; Li, L.; Sun, Q.; Grivas, P.; Ramsey, S.D.; Schwartz, S.M.; Shankaran, V. Utilization of systemic therapy in patients with cancer near the end of life in the pre- versus postimmune checkpoint inhibitor eras. JCO Oncol. Pract. 2021, 17, e1728–e1737. [Google Scholar] [CrossRef]
- Nipp, R.D.; Currow, D.C.; Cherny, N.I.; Strasser, F.; Abernethy, A.P.; Zafar, S.Y. Best supportive care in clinical trials: Review of the inconsistency in control arm design. Br. J. Cancer 2015, 113, 6–11. [Google Scholar] [CrossRef]
- Mo, L.; Urbauer, D.L.; Bruera, E.; Hui, D. Recommendations for supportive care and best supportive care in NCCN clinical practice guidelines for treatment of cancer: Differences between solid tumor and hematologic malignancy guidelines. Support. Care Cancer 2021, 29, 7385–7392. [Google Scholar] [CrossRef] [PubMed]
- Sanz Rubiales, Á.; Sánchez-Gutiérrez, M.E.; Flores Pérez, L.A.; Del Valle Rivero, M.L. How is best supportive care provided in clinical trials for patients with advanced cancer? A review of registered protocols of clinical trials. Curr. Oncol. 2020, 27, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Bakitas, M.; Lyons, K.D.; Hegel, M.T.; Balan, S.; Brokaw, F.C.; Seville, J.; Hull, J.G.; Li, Z.; Tosteson, T.D.; Byock, I.R.; et al. Effects of a palliative care intervention on clinical outcomes in patients with advanced cancer: The project ENABLE II randomized controlled trial. JAMA 2009, 302, 741–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Jawahri, A.; Greer, J.A.; Pirl, W.F.; Park, E.R.; Jackson, V.A.; Back, A.L.; Kamdar, M.; Jacobsen, J.; Chittenden, E.H.; Rinaldi, S.P.; et al. Effects of early integrated palliative care on caregivers of patients with lung and gastrointestinal cancer: A randomized clinical trial. Oncologist 2017, 22, 1528–1534. [Google Scholar] [CrossRef] [Green Version]
- Temel, J.S.; Greer, J.A.; El-Jawahri, A.; Pirl, W.F.; Park, E.R.; Jackson, V.A.; Back, A.L.; Kamdar, M.; Jacobsen, J.; Chittenden, E.H.; et al. Effects of early integrated palliative care in patients with lung and GI cancer: A randomized clinical trial. J. Clin. Oncol. 2017, 35, 834–841. [Google Scholar] [CrossRef]
- De Schreye, R.; Smets, T.; Annemans, L.; Deliens, L.; Gielen, B.; De Gendt, C.; Cohen, J. Applying quality indicators for administrative databases to evaluate end-of-life care for cancer patients in Belgium. Health Aff. 2017, 36, 1234–1243. [Google Scholar] [CrossRef]
- Pérez-Bracchiglione, J.; Salazar, J.; Santero, M.; Requeijo, C.; Grijalva, G.R.; Acosta-Dighero, R.; Meza, N.; Salas-Gama, K.; Olid, A.S.; Meade, A.G.; et al. Efficacy of systemic oncological treatments in patients with advanced, non-intestinal digestive cancer at high risk of dying in the middle and short term: Evidence synthesis (astac-study). Open Sci. Framew. 2022. Available online: https://osf.io/7chx6/ (accessed on 9 November 2022).
- Salazar, J.; Pérez-Bracchiglione, J.; Salas-Gama, K.; Antequera, A.; Auladell-Rispau, A.; Dorantes-Romandía, R.; Meade, A.G.; Jesús Quintana, M.; Requeijo, C.; Rodríguez-Grijalva, G.; et al. Systemic treatments for advanced digestive cancer research. efficacy of systemic oncological treatments in patients with advanced pancreatic cancer at high risk of dying in the short or medium-term: Overview of systematic reviews. Eur. J. Cancer 2021, 154, 82–91. [Google Scholar] [CrossRef]
- Santero, M.; Pérez-Bracchiglione, J.; Acosta-Dighero, R.; Meade, A.G.; Antequera, A.; Auladell-Rispau, A.; Quintana, M.J.; Requeijo, C.; Rodríguez-Grijalva, G.; Salas-Gama, K.; et al. Efficacy of systemic oncological treatments in patients with advanced esophageal or gastric cancers at high risk of dying in the middle and short term: An overview of systematic reviews. BMC Cancer 2021, 21, 712. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Pollock, M.; Fernandes, R.M.; Becker, L.A.; Pieper, D.; Hartling, L. Chapter V: Overviews of Reviews; Higgins, J.P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 9 November 2022).
- Gates, M.; Gates, A.; Pieper, D.; Fernandes, R.M.; Tricco, A.C.; Moher, D.; Brennan, S.E.; Li, T.; Pollock, M.; Lunny, C.; et al. Reporting guideline for overviews of reviews of healthcare interventions: Development of the PRIOR statement. BMJ 2022, 378, e070849. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [Green Version]
- Zafar, S.Y.; Currow, D.C.; Cherny, N.; Strasser, F.; Fowler, R.; Abernethy, A.P. Consensus-based standards for best supportive care in clinical trials in advanced cancer. Lancet Oncol. 2012, 13, e77–e82. [Google Scholar] [CrossRef] [PubMed]
- De Kock, I.; Mirhosseini, M.; Lau, F.; Thai, V.; Downing, M.; Quan, H.; Lesperance, M.; Yang, J. Conversion of Karnofsky performance status (KPS) and eastern cooperative oncology group performance status (ECOG) to palliative performance scale (PPS), and the interchangeability of PPS and KPS in prognostic tools. J. Palliat. Care 2013, 29, 163–169. Available online: https://www.ncbi.nlm.nih.gov/pubmed/24380215 (accessed on 9 November 2022). [CrossRef]
- NIH National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 25 April 2022).
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pieper, D.; Antoine, S.L.; Mathes, T.; Neugebauer, E.A.M.; Eikermann, M. Systematic review finds overlapping reviews were not mentioned in every other overview. J. Clin. Epidemiol. 2014, 67, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Bracchiglione, J.; Meza, N.; Bangdiwala, S.I.; Niño de Guzmán, E.; Urrútia, G.; Bonfill, X.; Madrid, E. Graphical representation of overlap for OVErviews: GROOVE tool. Res. Synth. Methods 2022, 13, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2022; Available online: www.training.cochrane.org/handbook (accessed on 9 November 2022).
- Lin, L.; Chu, H.; Murad, M.H.; Hong, C.; Qu, Z.; Cole, S.R.; Chen, Y. Empirical comparison of publication bias tests in meta-analysis. J. Gen. Intern. Med. 2018, 33, 1260–1267. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Schünemann, H.; Brożek, J.; Guyatt, G.; Oxman, A. GRADE Handbook. October 2013. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 25 April 2022).
- Abdel-Rahman, O.; Elsayed, Z.; Elhalawani, H. Gemcitabine-based chemotherapy for advanced biliary tract carcinomas. Cochrane Database Syst. Rev. 2018, 4, CD011746. [Google Scholar] [CrossRef]
- Finn, R.S.; Zhu, A.X.; Farah, W.; Almasri, J.; Zaiem, F.; Prokop, L.J.; Murad, M.H.; Mohammed, K. Therapies for advanced stage hepatocellular carcinoma with macrovascular invasion or metastatic disease: A systematic review and meta-analysis. Hepatology 2018, 67, 422–435. Available online: http://doi.wiley.com/10.1002/hep.29486 (accessed on 9 November 2022). [CrossRef]
- Huang, Y.; Cheng, X.; Sun, P.; Li, T.; Song, Z.; Zheng, Q. Supplementary sorafenib therapies for hepatocellular carcinoma—A systematic review and meta-analysis. J. Clin. Gastroenterol. 2019, 53, 486–494. Available online: https://www.ingentaconnect.com/content/wk/jcga/2019/00000053/00000007/art00010 (accessed on 9 November 2022). [CrossRef] [PubMed]
- Guo, T.; Liu, P.; Yang, J.; Wu, P.; Chen, B.; Liu, Z.; Li, Z. Evaluation of targeted agents for advanced and unresectable hepatocellular carcinoma: A network meta-analysis. J. Cancer 2019, 10, 4671–4678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Yang, X.R.; Huang, X.W.; Wang, W.M.; Shi, R.Y.; Xu, Y.; Wang, Z.; Qiu, S.J.; Fan, J.; Zhou, J. Sorafenib in treatment of patients with advanced hepatocellular carcinoma: A systematic review. Hepatobiliary Pancreat. Dis. Int. 2012, 11, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Ling-lin, Z.; Li, M.; Jin-hui, T.; Ke-hu, Y. Sorafenib for advanced hepatocellular carcinoma: A systematic review. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2011, 33, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Meyers, B.M.; Knox, J.J.; Cosby, R.; Beecroft, J.R.; Chan, K.K.; Coburn, N.; Feld, J.J.; Jonker, D.; Mahmud, A.; Ringash, J. Non-surgical management of advanced hepatocellular carcinoma: A systematic review by cancer care Ontario. Can. Liver J. 2021, 4, 257–274. [Google Scholar] [CrossRef]
- Griffiths, C.D.; Zhang, B.; Tywonek, K.; Meyers, B.M.; Serrano, P.E. Toxicity profiles of systemic therapies for advanced hepatocellular carcinoma: A systematic review and meta-analysis. JAMA Netw. Open 2022, 5, e2222721. [Google Scholar] [CrossRef]
- Liu, W.; Quan, B.; Lu, S.; Tang, B.; Li, M.; Chen, R.; Ren, Z.; Yin, X. First-line systemic treatment strategies for unresectable hepatocellular carcinoma: A systematic review and network meta-analysis of randomized clinical trials. Front. Oncol. 2021, 11, 771045. [Google Scholar] [CrossRef]
- Jácome, A.A.; Castro, A.C.G.; Vasconcelos, J.P.S.; Silva, M.H.C.R.; Lessa, M.A.O.; Moraes, E.D.; Andrade, A.C.; Lima, F.M.T.; Farias, J.P.F.; Gil, R.A.; et al. Efficacy and safety associated with immune checkpoint inhibitors in unresectable hepatocellular carcinoma: A meta-analysis. JAMA Netw. Open 2021, 4, e2136128. [Google Scholar] [CrossRef]
- Jiang, Y.; Zeng, Z.; Zeng, J.; Liu, C.; Qiu, J.; Li, Y.; Tang, J.; Mo, N.; Du, L.; Ma, J. Efficacy and safety of first-line chemotherapies for patients with advanced biliary tract carcinoma: A systematic review and network meta-analysis. Front. Oncol. 2021, 11, 736113. [Google Scholar] [CrossRef]
- Chen, J.; Wang, J.; Xie, F. Comparative efficacy and safety for second-line treatment with ramucirumab, regorafenib, and cabozantinib in patients with advanced hepatocellular carcinoma progressed on sorafenib treatment: A network meta-analysis. Medicine 2021, 100, e27013. [Google Scholar] [CrossRef] [PubMed]
- Solimando, A.G.; Susca, N.; Argentiero, A.; Brunetti, O.; Leone, P.; De Re, V.; Fasano, R.; Krebs, M.; Petracci, E.; Azzali, I.; et al. Second-line treatments for advanced hepatocellular carcinoma: A systematic review and Bayesian network meta-analysis. Clin. Exp. Med. 2021, 22, 65–74. [Google Scholar] [CrossRef]
- Haber, P.K.; Puigvehí, M.; Castet, F.; Lourdusamy, V.; Montal, R.; Tabrizian, P.; Buckstein, M.; Kim, E.; Villanueva, A.; Schwartz, M.; et al. Evidence-based management of hepatocellular carcinoma: Systematic review and meta-analysis of randomized controlled trials (2002–2020). Gastroenterology 2021, 161, 879–898. [Google Scholar] [CrossRef]
- Park, R.; Lopes da Silva, L.; Nissaisorakarn, V.; Riano, I.; Williamson, S.; Sun, W.; Saeed, A. Comparison of efficacy of systemic therapies in advanced hepatocellular carcinoma: Updated systematic review and frequentist network meta-analysis of randomized controlled trials. J. Hepatocell. Carcinoma 2021, 8, 145–154. [Google Scholar] [CrossRef]
- Ziogas, I.A.; Evangeliou, A.P.; Giannis, D.; Hayat, M.H.; Mylonas, K.S.; Tohme, S.; Geller, D.A.; Elias, N.; Goyal, L.; Tsoulfas, G. The role of immunotherapy in hepatocellular carcinoma: A systematic review and pooled analysis of 2,402 Patients. Oncol. 2020, 26, e1036–e1049. [Google Scholar] [CrossRef] [PubMed]
- Sonbol, M.B.; Riaz, I.B.; Naqvi, S.A.A.; Almquist, D.R.; Mina, S.; Almasri, J.; Shah, S.; Almader-Douglas, D.; Uson Junior, P.L.S.; Mahipal, A.; et al. Systemic therapy and sequencing options in advanced hepatocellular carcinoma: A systematic review and network meta-analysis. JAMA Oncol. 2020, 6, e204930. [Google Scholar] [CrossRef] [PubMed]
- Faruque, L.I.; Lin, M.; Battistella, M.; Wiebe, N.; Reiman, T.; Hemmelgarn, B.; Thomas, C.; Tonelli, M. Systematic review of the risk of adverse outcomes associated with vascular endothelial growth factor inhibitors for the treatment of cancer. PLoS ONE 2014, 9, e101145. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2008, 10, 25–34. [Google Scholar] [CrossRef]
- Ji, Y.X.; Zhang, Z.F.; Lan, K.T.; Nie, K.K.; Geng, C.X.; Liu, S.C.; Zhang, L.; Zhuang, X.J.; Zou, X.; Sun, L.; et al. Sorafenib in liver function impaired advanced hepatocellular carcinoma. Chin. Med. Sci. J. 2014, 29, 7–14. [Google Scholar] [CrossRef]
- Hsu, C.; Yang, T.S.; Huo, T.I.; Hsieh, R.K.; Yu, C.W.; Hwang, W.S.; Hsieh, T.Y.; Huang, W.T.; Chao, Y.; Meng, R.; et al. Vandetanib in patients with inoperable hepatocellular carcinoma: A phase II, randomized, double-blind, placebo-controlled study. J. Hepatol. 2012, 56, 1097–1103. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Decaens, T.; Raoul, J.L.; Boucher, E.; Kudo, M.; Chang, C.; Kang, Y.K.; Assenat, E.; Lim, H.Y.; Boige, V.; et al. Brivanib in patients with advanced hepatocellular carcinoma who were intolerant to sorafenib or for whom sorafenib failed: Results from the randomized phase III BRISK-PS study. J. Clin. Oncol. 2013, 31, 3509–3516. [Google Scholar] [CrossRef]
- Santoro, A.; Rimassa, L.; Borbath, I.; Daniele, B.; Salvagni, S.; Van Laethem, J.L.; Van Vlierberghe, H.; Trojan, J.; Kolligs, F.T.; Weiss, A.; et al. Tivantinib for second-line treatment of advanced hepatocellular carcinoma: A randomised, placebo-controlled phase 2 study. Lancet Oncol. 2012, 14, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Rimassa, L.; Pressiani, T.; Boni, C.; Carnaghi, C.; Rota Caremoli, E.; Fagiuoli, S.; Foa, P.; Salvagni, S.; Cortesi, E.; Chiara Tronconi, M.; et al. A phase II randomized dose escalation trial of sorafenib in patients with advanced hepatocellular carcinoma. Oncologist 2013, 18, 379–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, C.J.; Daniele, B.; Kudo, M.; Merle, P.; Park, J.W.; Ross, P.J.; Peron, J.M.; Ebert, O.; Chan, S.L.; Poon, R.T.P.; et al. Randomized phase II trial of intravenous RO5137382/GC33 at 1600 mg every other week and placebo in previously treated patients with unresectable advanced hepatocellular carcinoma (HCC.; NCT01507168). J. Clin. Oncol. 2014, 32 (Suppl. S15), 4102. Available online: http://ascopubs.org/doi/10.1200/jco.2014.32.15_suppl.4102 (accessed on 9 November 2022). [CrossRef]
- Zhu, A.X.; Kudo, M.; Assenat, E.; Cattan, S.; Kang, Y.K.; Lim, H.Y.; Poon, R.T.P.; Blanc, J.F.; Vogel, A.; Chen, C.L.; et al. Effect of everolimus on survival in advanced hepatocellular carcinoma after failure of sorafenib: The EVOLVE-1 randomized clinical trial. JAMA 2014, 312, 57–67. [Google Scholar] [CrossRef]
- Zhu, A.X.; Park, J.O.; Ryoo, B.Y.; Yen, C.J.; Poon, R.; Pastorelli, D.; Blanc, J.F.; Chung, H.C.; Baron, A.D.; Pfiffer, T.E.F.; et al. Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015, 16, 859–870. [Google Scholar] [CrossRef]
- Kang, Y.K.; Yau, T.; Park, J.W.; Lim, H.Y.; Lee, T.Y.; Obi, S.; Chan, S.L.; Qin, S.; Kim, R.D.; Casey, M.; et al. Randomized phase II study of axitinib versus placebo plus best supportive care in second-line treatment of advanced hepatocellular carcinoma. Ann. Oncol. 2015, 26, 2457–2463. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Puig, O.; Daniele, B.; Kudo, M.; Merle, P.; Park, J.W.; Ross, P.; Peron, J.M.; Ebert, O.; Chan, S.; et al. Randomized phase II placebo controlled study of codrituzumab in previously treated patients with advanced hepatocellular carcinoma. J. Hepatol. 2016, 65, 289–295. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Moriguchi, M.; Numata, K.; Hidaka, H.; Tanaka, H.; Ikeda, M.; Kawazoe, S.; Ohkawa, S.; Sato, Y.; Kaneko, S.; et al. S-1 versus placebo in patients with sorafenib-refractory advanced hepatocellular carcinoma (S-CUBE): A randomised, double-blind, multicentre, phase 3 trial. Lancet Gastroenterol. Hepatol. 2017, 2, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Rimassa, L.; Assenat, E.; Peck-Radosavljevic, M.; Pracht, M.; Zagonel, V.; Mathurin, P.; Rota Caremoli, E.; Porta, C.; Daniele, B.; Bolondi, L.; et al. Tivantinib for second-line treatment of MET-high, advanced hepatocellular carcinoma (METIV-HCC): A final analysis of a phase 3, randomised, placebo-controlled study. Lancet Oncol. 2018, 19, 682–693. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Qin, S.; Ryoo, B.Y.; Lu, S.N.; Yen, C.J.; Feng, Y.H.; Lim, H.Y.; Izzo, F.; Colombo, M.; Sarker, D.; et al. Phase III randomized study of second line ADI-PEG 20 plus best supportive care versus placebo plus best supportive care in patients with advanced hepatocellular carcinoma. Ann. Oncol. 2018, 29, 1402–1408. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Ryoo, B.Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.Y.; Breder, V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: A randomized, double-blind, phase III trial. J. Clin. Oncol. 2020, 38, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Qin, S.; Gu, S.; Chen, X.; Lin, L.; Wang, Z.; Xu, A.; Chen, X.; Zhou, C.; Ren, Z.; et al. Apatinib as second-line therapy in Chinese patients with advanced hepatocellular carcinoma: A randomized, placebo-controlled, double-blind, phase III study. J. Clin. Oncol. 2020, 38, 4507. [Google Scholar] [CrossRef]
- Kudo, M.; Morimoto, M.; Moriguchi, M.; Izumi, N.; Takayama, T.; Yoshiji, H.; Hino, K.; Oikawa, T.; Chiba, T.; Motomura, K.; et al. A randomized, double-blind, placebo-controlled, phase 3 study of tivantinib in Japanese patients with MET-high hepatocellular carcinoma. Cancer Sci. 2020, 111, 3759–3769. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Dwary, A.D.; Mohanti, B.K.; Deo, S.V.; Pal, S.; Sreenivas, V.; Raina, V.; Shukla, N.K.; Thulkar, S.; Garg, P.; et al. Best supportive care compared with chemotherapy for unresectable gall bladder cancer: A randomized controlled study. J. Clin. Oncol. 2010, 28, 4581–4586. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Di Bisceglie, A.M.; Bruix, J.; Kramer, B.S.; Lencioni, R.; Zhu, A.X.; Sherman, M.; Schwartz, M.; Lotze, M.; Talwalkar, J.; et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Gynecol. Oncol. 2008, 100, 698–711. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Villanueva, A.; Marrero, J.A.; Schwartz, M.; Meyer, T.; Galle, P.R.; Lencioni, R.; Greten, T.F.; Kudo, M.; Mandrekar, S.J.; et al. Trial design and endpoints in hepatocellular carcinoma: AASLD consensus conference. Hepatology 2020, 73 (Suppl. S1), 158–191. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, I.; Corsini, N.; Hutchinson, A.D.; Marker, J.; Eckert, M. A core set of patient-reported outcomes for population-based cancer survivorship research: A consensus study. J. Cancer Surviv. 2020, 15, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Urquhart, R.; Murnaghan, S.; Kendell, C.; Sussman, J.; Porter, G.A.; Howell, D.; Grunfeld, E. What matters in cancer survivorship research? A suite of stakeholder-relevant outcomes. Curr. Oncol. 2021, 28, 3188–3200. [Google Scholar] [CrossRef] [PubMed]
- Di Maio, M.; Basch, E.; Denis, F.; Fallowfield, L.J.; Ganz, P.A.; Howell, D.; Kowalski, C.; Perrone, F.; Stover, A.M.; Sundaresan, P.; et al. The role of patient-reported outcome measures in the continuum of cancer clinical care: ESMO clinical practice guideline. Ann. Oncol. 2022, 33, 878–892. [Google Scholar] [CrossRef] [PubMed]
- COMET Initiative. Developing Core Outcomes for Prognostic Research in Palliative Care. Available online: https://www.comet-initiative.org/Studies/Details/2136 (accessed on 9 November 2022).
- European Oncology Nursing Society. PROMs Project-EONS-The European Oncology Nursing Society. Available online: https://cancernurse.eu/research/proms_project/ (accessed on 9 November 2022).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Country | Relevant Included Primary Studies 1/Total Included Studies | Type of Patients 1 | Type of SOT | Line of Treatment | Comparator | Outcomes Assessed | Type of Meta-Analysis | Funding | CoI of the Review | Databases Searched | Search Timeframe |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ling-lin 2011 [53] | China | 2/4 | Advanced HCC | BIO/TT (Sorafenib) | First | Placebo | OS | Pairwise | NS | NS | MEDLINE, EMBASE, Cochrane, other | Until November 2019 |
| Zhang 2012 [52] | China | 2/6 | Advanced HCC | BIO/TT (Sorafenib) | First | Placebo | OS, toxicity | Pairwise | Public | No CoI | MEDLINE, EMBASE, WoS | January 2005 to June 2011 |
| Faruque 2014 [65] | Canada | 2/72 | Advanced HCC | BIO/TT (Sorafenib) | First | NS | OS, toxicity | Pairwise | Public and private | With CoI | MEDLINE, EMBASE, Cochrane | Until April 2012 |
| Finn 2017 [49] | USA | 2/14 | Advanced HCC | BIO/TT (Sorafenib) | First | Placebo | OS | Pairwise | Private | With CoI | MEDLINE, EMBASE, CENTRAL, Scopus | Until February 2016 |
| Abdel-Rahman 2018 [48] | Canada | 1/7 | Advanced gallbladder cancer | CT (Fluorouracil/folinic acid, or gemcitabine/oxaliplatin) | NS | BSC | OS, PFS, toxicity | Pairwise | No funding | No CoI | MEDLINE, EMBASE, CENTRAL, WoS, LILACS, clinicaltrials.gov | Until June 2017 |
| Guo 2019 [51] | China | 12/31 | Advanced HCC | BIO/TT and IT (Sorafenib, vandetanib, brivanib, tivantinib, ramucirumab, axitinib, codrituzumab, cabozatinib) | First, second | Negative control (placebo or no treatment) | OS, PFS, toxicity | Network | NS | No CoI | MEDLINE, EMBASE, CENTRAL | Until March 2019 |
| Huang 2019 [50] | China | 5/11 | Advanced HCC | BIO/TT (Sorafenib) | First, second | Placebo/BSC | OS, toxicity | Pairwise | NS | No CoI | MEDLINE, EMBASE, CENTRAL, WoS, clinicaltrials.gov | Until April 2018 |
| Sonbol 2020 [64] | USA | 8/14 | Advanced HCC | BIO/TT and IT (Sorafenib, pembrolizumab, regorafenib, cabozantinib, ramucirumab, brivanib) | First, second | Placebo | OS, PFS | Network | NS | With CoI | MEDLINE, EMBASE, CENTRAL, WoS, Scopus | Until March 2020 |
| Ziogas 2021 [63] | Greece | 1/63 | Advanced HCC | IT (Pembrolizumab) | Second | Placebo | OS, PFS, toxicity | Pairwise | NS | With CoI | MEDLINE, Cochrane, clinicaltrials.gov | Until November 2020 |
| Park 2021 [62] | USA | 13/24 | Advanced HCC | BIO/TT and IT (Sorafenib, regorafenib, cabozitinib, ramucirumab, apatinib, pembrolizumab, brivanib, tivantinib, everolimus, axitinib) | First, second | Placebo | OS, PFS | Network | No funding | With CoI | MEDLINE, EMBASE, Cochrane | Until June 2020 |
| Chen 2021 [59] | China | 4/4 | Advanced HCC | BIO/TT (Regorafenib, cabozantinib, ramucirumab) | Second | Placebo | OS, PFS, toxicity | Network | No funding | No CoI | MEDLINE, EMBASE, Cochrane | Until April 2019 |
| Meyers 2021 [54] | Canada | 12/49 | Advanced HCC | BIO/TT and IT (Regorafenib, cabozantinib, brivanib, tivantinib, pembrolizumab, everolimus, ADI-peg 20, S-1, RO5137382/GC33) | Second or more | Placebo/BSC | OS, PFS, toxicity, QoL, symptoms | Pairwise | No funding | With CoI | MEDLINE, EMBASE, Cochrane | January 2000 to January 2020 |
| Haber 2021 [61] | USA | 13/49 | Advanced HCC | BIO/TT and IT (Sorafenib, tivantinib, S-1, regorafenib, ramucirumab, ADI-PEG20, everolimus, cabozantinib, brivanib, pembrolizumab) | First, second | Placebo | OS, PFS | Pairwise | Public | With CoI | MEDLINE, Cochrane, WoS | June 2002 to December 2020 |
| Jiang 2021 [58] | China | 1/24 | Advanced gallbladder cancer | CT (FUFA, or gemcitabine/oxaliplatin) | NS | BSC | OS, PFS, toxicity | Network | Public | NS | MEDLINE, EMBASE, Cochrane | Until August 2020 |
| Jácome 2021 [57] | Brazil | 1/3 | Advanced HCC | IT (Pembrolizumab) | Second | Standard care | OS, PFS, toxicity | Pairwise | NS | With CoI | MEDLINE, CENTRAL, WoS, LILACS | Until February 2020 |
| Liu 2021 [56] | China | 2/15 | Advanced HCC | BIO/TT (Sorafenib) | First | Placebo | OS, PFS, toxicity | Network | Public | No CoI | MEDLINE, EMBASE, CENTRAL, Cochrane, WoS, Scopus, other | Until August 2021 |
| Solimando 2022 [60] | Italy | 14/14 | Advanced HCC | BIO/TT and IT (Tivantinib, S-1, regorafenib, ramucirumab, ADI-PEG20, everolimus, cabozantinib, brivanib, pembrolizumab, axitinib, codrituzumab) | Second | Placebo | OS, PFS | Network | Public | No CoI | MEDLINE, WoS, Scopus, clinicaltrials.gov | Until December 2020 |
| Griffiths 2022 [55] | Canada | 13/30 | Advanced HCC | BIO/TT and IT (Sorafenib, tivantinib, regorafenib, ramucirumab, everolimus, cabozantinib, brivanib, pembrolizumab, axitinib) | First, second or more | Placebo | Toxicity | Pairwise | NS | With CoI | MEDLINE, EMBASE, CENTRAL | January 1990 to December 2021 |
| Study ID | Q1 | Q2 1 | Q3 | Q4 1 | Q5 | Q6 | Q7 1 | Q8 | Q9 1 | Q10 | Q11 1 | Q12 | Q13 1 | Q14 | Q15 1 | Q16 | Overall Quality of the Review |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ling-lin 2011 [53] | Y | N | Y | PY | Y | Y | N | PY | Y | N | Y | N | N | N | N | N | Critically low |
| Zhang 2012 [52] | Y | N | Y | PY | Y | N | N | Y | Y | N | Y | N | N | Y | Y | Y | Critically low |
| Faruque 2014 [65] | N | N | Y | PY | Y | Y | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | Critically low |
| Finn 2017 [49] | Y | PY | N | Y | Y | N | N | Y | Y | N | Y | N | N | Y | Y | Y | Critically low |
| Abdel- Rahman 2018 [48] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | High |
| Guo 2019 [51] | Y | Y | Y | Y | Y | Y | N | Y | Y | N | NA | Y | Y | Y | Y | Y | Low |
| Huang 2019 [50] | Y | PY | N | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | N | Moderate |
| Sonbol 2020 [64] | Y | N | N | PY | N | Y | N | PY | Y | N | Y | Y | Y | Y | N | Y | Critically low |
| Ziogas 2021 [63] | Y | N | N | Y | Y | Y | N | PY | N | N | NA | NA | N | Y | NA | Y | Critically low |
| Park 2021 [62] | Y | Y | Y | PY | PY | N | N | PY | Y | N | Y | Y | Y | N | Y | Y | Low |
| Chen 2021 [59] | Y | N | Y | PY | N | Y | N | PY | Y | N | Y | Y | Y | Y | Y | Y | Critically low |
| Meyers 2021 [54] | Y | N | Y | PY | N | N | N | PY | Y | N | NA | NA | N | N | NA | Y | Critically low |
| Haber 2021 [61] | Y | N | Y | PY | Y | Y | Y | PY | PY | N | NA | NA | Y | Y | NA | Y | Low |
| Jiang 2021 [58] | Y | N | Y | PY | N | Y | N | Y | Y | N | NA | NA | Y | Y | NA | Y | Critically low |
| Jácome 2021 [57] | Y | PY | Y | PY | Y | Y | N | N | Y | N | NA | NA | Y | Y | NA | N | Low |
| Liu 2021 [56] | Y | PY | Y | PY | Y | Y | N | PY | Y | N | Y | Y | Y | Y | Y | Y | Low |
| Solimando 2022 [60] | Y | N | Y | PY | N | Y | N | PY | Y | N | Y | Y | Y | Y | Y | N | Critically low |
| Griffiths 2022 [55] | Y | N | Y | Y | Y | Y | N | PY | Y | N | Y | Y | Y | N | N | Y | Critically low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bracchiglione, J.; Rodríguez-Grijalva, G.; Requeijo, C.; Santero, M.; Salazar, J.; Salas-Gama, K.; Meade, A.-G.; Antequera, A.; Auladell-Rispau, A.; Quintana, M.J.; et al. Systemic Oncological Treatments versus Supportive Care for Patients with Advanced Hepatobiliary Cancers: An Overview of Systematic Reviews. Cancers 2023, 15, 766. https://doi.org/10.3390/cancers15030766
Bracchiglione J, Rodríguez-Grijalva G, Requeijo C, Santero M, Salazar J, Salas-Gama K, Meade A-G, Antequera A, Auladell-Rispau A, Quintana MJ, et al. Systemic Oncological Treatments versus Supportive Care for Patients with Advanced Hepatobiliary Cancers: An Overview of Systematic Reviews. Cancers. 2023; 15(3):766. https://doi.org/10.3390/cancers15030766
Chicago/Turabian StyleBracchiglione, Javier, Gerardo Rodríguez-Grijalva, Carolina Requeijo, Marilina Santero, Josefina Salazar, Karla Salas-Gama, Adriana-Gabriela Meade, Alba Antequera, Ariadna Auladell-Rispau, María Jesús Quintana, and et al. 2023. "Systemic Oncological Treatments versus Supportive Care for Patients with Advanced Hepatobiliary Cancers: An Overview of Systematic Reviews" Cancers 15, no. 3: 766. https://doi.org/10.3390/cancers15030766