
Current Status and Future Prospects for Esophageal Cancer

Abstract
:Simple Summary
Abstract
1. Introduction
2. Epidemiology of Esophageal Cancer
3. Environmental Risk Factors for Esophageal Cancer
3.1. Habits
3.1.1. Tobacco
3.1.2. Alcohol
3.1.3. Opium
3.1.4. Hot Food and Drinks
3.2. Living Environment
3.2.1. Socioeconomic Status (SES)
3.2.2. Household Fuel
3.2.3. Water Source
3.2.4. Mycotoxin Contamination
3.2.5. Animal Contact
3.3. Individual Health
3.3.1. Gastroesophageal Reflux Disease (GERD)
3.3.2. Body Mass Index (BMI)
3.3.3. Gastric Atrophy
3.3.4. Poor oral Health and Hygiene
3.3.5. Microbiome
3.4. Dietary Factors
3.4.1. Whole Diet Quality
3.4.2. Intake of Specific Dietary Groups
3.4.3. Micronutrients
3.5. Infections
3.5.1. Viral Infections
3.5.2. Bacterial Infections
4. Prevention
5. Diagnosis
6. Treatment
6.1. Current Treatment Strategies
6.2. Future Perspectives for Treatment of Esophageal Cancer
Author Contributions
Funding
Conflicts of Interest
Disclaimer
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lagergren, J.; Smyth, E.; Cunningham, D.; Lagergren, P. Oesophageal Cancer. Lancet 2017, 390, 2383–2396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Intenational Agency for Research on Cancer (IARC). Global Cancer Observatory (Globocan). Available online: https://gco.iarc.fr/ (accessed on 23 October 2022).
- Uhlenhopp, D.J.; Then, E.O.; Sunkara, T.; Gaduputi, V. Epidemiology of Esophageal Cancer: Update in Global Trends, Etiology and Risk Factors. Clin. J. Gastroenterol. 2020, 13, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Park, J.Y.; Sheikh, M.; Kayamba, V.; Rumgay, H.; Jenab, M.; Narh, C.T.; Abedi-Ardekani, B.; Morgan, E.; de Martel, C.; et al. Population-Based Investigation of Common and Deviating Patterns of Gastric Cancer and Oesophageal Cancer Incidence across Populations and Time. Gut 2022, gutjnl-2022-328233. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, X.; Cao, S.; Dong, X.; Rao, S.; Cai, K. Understanding Esophageal Cancer: The Challenges and Opportunities for the Next Decade. Front. Oncol. 2020, 10, 1727. [Google Scholar] [CrossRef]
- Li, J.; Xu, J.; Zheng, Y.; Gao, Y.; He, S.; Li, H.; Zou, K.; Li, N.; Tian, J.; Chen, W.; et al. Esophageal Cancer: Epidemiology, Risk Factors and Screening. Chin. J. Cancer Res. 2021, 33, 535–547. [Google Scholar] [CrossRef]
- Mahboubi, E.; Kmet, J.; Cook, P.J.; Day, N.E.; Ghadirian, P.; Salmasizadeh, S. Oesophageal Cancer Studies in the Caspian Littoral of Iran: The Caspian Cancer Registry. Br. J. Cancer 1973, 28, 197–214. [Google Scholar] [CrossRef]
- GBD 2017 Oesophageal Cancer Collaborators. The Global, Regional, and National Burden of Oesophageal Cancer and Its Attributable Risk Factors in 195 Countries and Territories, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2020, 5, 582–597. [Google Scholar] [CrossRef]
- Yousefi, M.; Sharifi-Esfahani, M.; Pourgholam-Amiji, N.; Afshar, M.; Sadeghi-Gandomani, H.; Otroshi, O.; Salehiniya, H. Esophageal Cancer in the World: Incidence, Mortality and Risk Factors. Biomed. Res. Ther. 2018, 5, 2504–2517. [Google Scholar] [CrossRef]
- Wang, B.; He, F.; Hu, Y.; Wang, Q.; Wang, D.; Sha, Y.; Wu, J. Cancer Incidence and Mortality and Risk Factors in Member Countries of the “Belt and Road” Initiative. BMC Cancer 2022, 22, 582. [Google Scholar] [CrossRef]
- Ke, L. Mortality and Incidence Trends from Esophagus Cancer in Selected Geographic Areas of China circa 1970-90. Int. J. Cancer 2002, 102, 271–274. [Google Scholar] [CrossRef]
- Morgan, E.; Soerjomataram, I.; Rumgay, H.; Coleman, H.G.; Thrift, A.P.; Vignat, J.; Laversanne, M.; Ferlay, J.; Arnold, M. The Global Landscape of Esophageal Squamous Cell Carcinoma and Esophageal Adenocarcinoma Incidence and Mortality in 2020 and Projections to 2040: New Estimates From GLOBOCAN 2020. Gastroenterology 2022, 163, 649–658.e2. [Google Scholar] [CrossRef]
- Arnold, M.; Ferlay, J.; van Berge Henegouwen, M.I.; Soerjomataram, I. Global Burden of Oesophageal and Gastric Cancer by Histology and Subsite in 2018. Gut 2020, 69, 1564–1571. [Google Scholar] [CrossRef]
- Islami, F.; Kamangar, F.; Nasrollahzadeh, D.; Møller, H.; Boffetta, P.; Malekzadeh, R. Oesophageal Cancer in Golestan Province, a High-Incidence Area in Northern Iran —A Review. Eur. J. Cancer 2009, 45, 3156–3165. [Google Scholar] [CrossRef]
- Abnet, C.C.; Kamangar, F.; Islami, F.; Nasrollahzadeh, D.; Brennan, P.; Aghcheli, K.; Merat, S.; Pourshams, A.; Marjani, H.A.; Ebadati, A.; et al. Tooth Loss and Lack of Regular Oral Hygiene Are Associated with Higher Risk of Esophageal Squamous Cell Carcinoma. Cancer Epidemiol. Biomark. Prev. 2008, 17, 3062–3068. [Google Scholar] [CrossRef] [Green Version]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global Cancer Statistics. CA. Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [Green Version]
- Parkin, D.M.; Pisani, P.; Ferlay, J. Global Cancer Statistics. CA Cancer J. Clin. 1999, 49, 33–64. [Google Scholar] [CrossRef]
- Parkin, D.M. Global Cancer Statistics in the Year 2000. Lancet Oncol. 2001, 2, 533–543. [Google Scholar] [CrossRef]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global Cancer Statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [Green Version]
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [CrossRef] [Green Version]
- Global Burden of Disease 2019 Cancer Collaboration; Kocarnik, J.M.; Compton, K.; Dean, F.E.; Fu, W.; Gaw, B.L.; Harvey, J.D.; Henrikson, H.J.; Lu, D.; Pennini, A.; et al. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022, 8, 420–444. [Google Scholar] [CrossRef] [PubMed]
- Trivers, K.F.; Sabatino, S.A.; Stewart, S.L. Trends in Esophageal Cancer Incidence by Histology, United States, 1998–2003. Int. J. Cancer 2008, 123, 1422–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.; Zheng, R.; Zhang, S.; Chen, R.; Wang, S.; Sun, K.; Li, M.; Lei, S.; Zhuang, G.; Wei, W. Gastric and Esophageal Cancer in China 2000 to 2030: Recent Trends and Short-Term Predictions of the Future Burden. Cancer Med. 2022, 11, 1902–1912. [Google Scholar] [CrossRef]
- Roshandel, G.; Ferlay, J.; Ghanbari-Motlagh, A.; Partovipour, E.; Salavati, F.; Aryan, K.; Mohammadi, G.; Khoshaabi, M.; Sadjadi, A.; Davanlou, M.; et al. Cancer in Iran 2008 to 2025: Recent Incidence Trends and Short-Term Predictions of the Future Burden. Int. J. Cancer 2021, 149, 594–605. [Google Scholar] [CrossRef]
- Roshandel, G.; Ferlay, J.; Semnani, S.; Fazel, A.; Naeimi-Tabiei, M.; Ashaari, M.; Amiriani, T.; Honarvar, M.; Sedaghat, S.; Hasanpour-Heidari, S.; et al. Recent Cancer Incidence Trends and Short-Term Predictions in Golestan, Iran 2004–2025. Cancer Epidemiol. 2020, 67, 101728. [Google Scholar] [CrossRef]
- Li, B.; Liu, Y.; Peng, J.; Sun, C.; Rang, W. Trends of Esophageal Cancer Incidence and Mortality and Its Influencing Factors in China. Risk Manag. Healthc. Policy 2021, 14, 4809–4821. [Google Scholar] [CrossRef]
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology 2020, 159, 335–349.e15. [Google Scholar] [CrossRef]
- Bosetti, C.; Levi, F.; Ferlay, J.; Garavello, W.; Lucchini, F.; Bertuccio, P.; Negri, E.; La Vecchia, C. Trends in Oesophageal Cancer Incidence and Mortality in Europe. Int. J. Cancer 2008, 122, 1118–1129. [Google Scholar] [CrossRef]
- Castro, C.; Bosetti, C.; Malvezzi, M.; Bertuccio, P.; Levi, F.; Negri, E.; La Vecchia, C.; Lunet, N. Patterns and Trends in Esophageal Cancer Mortality and Incidence in Europe (1980–2011) and Predictions to 2015. Ann. Oncol. 2014, 25, 283–290. [Google Scholar] [CrossRef]
- Devesa, S.S.; Blot, W.J.; Fraumeni, J.F. Changing Patterns in the Incidence of Esophageal and Gastric Carcinoma in the United States. Cancer 1998, 83, 2049–2053. [Google Scholar] [CrossRef]
- Arnold, M.; Laversanne, M.; Brown, L.M.; Devesa, S.S.; Bray, F. Predicting the Future Burden of Esophageal Cancer by Histological Subtype: International Trends in Incidence up to 2030. Am. J. Gastroenterol. 2017, 112, 1247–1255. [Google Scholar] [CrossRef]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Personal Habits and Indoor Combustions; IARC: Lyon, France, 2012; Volume 100E, ISBN 978-92-832-1322-2. [Google Scholar]
- Tran, K.B.; Lang, J.J.; Compton, K.; Xu, R.; Acheson, A.R.; Henrikson, H.J.; Kocarnik, J.M.; Penberthy, L.; Aali, A.; Abbas, Q.; et al. The Global Burden of Cancer Attributable to Risk Factors, 2010–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 563–591. [Google Scholar] [CrossRef]
- Wang, Q.-L.; Xie, S.-H.; Li, W.-T.; Lagergren, J. Smoking Cessation and Risk of Esophageal Cancer by Histological Type: Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [Green Version]
- Freedman, N.D.; Abnet, C.C.; Leitzmann, M.F.; Mouw, T.; Subar, A.F.; Hollenbeck, A.R.; Schatzkin, A. A Prospective Study of Tobacco, Alcohol, and the Risk of Esophageal and Gastric Cancer Subtypes. Am. J. Epidemiol. 2007, 165, 1424–1433. [Google Scholar] [CrossRef]
- Zendehdel, K.; Nyrén, O.; Luo, J.; Dickman, P.W.; Boffetta, P.; Englund, A.; Ye, W. Risk of Gastroesophageal Cancer among Smokers and Users of Scandinavian Moist Snuff. Int. J. Cancer 2008, 122, 1095–1099. [Google Scholar] [CrossRef]
- Ishiguro, S.; Sasazuki, S.; Inoue, M.; Kurahashi, N.; Iwasaki, M.; Tsugane, S.; JPHC Study Group. Effect of Alcohol Consumption, Cigarette Smoking and Flushing Response on Esophageal Cancer Risk: A Population-Based Cohort Study (JPHC Study). Cancer Lett. 2009, 275, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Kaimila, B.; Mulima, G.; Kajombo, C.; Salima, A.; Nietschke, P.; Pritchett, N.; Chen, Y.; Murphy, G.; Dawsey, S.M.; Gopal, S.; et al. Tobacco and Other Risk Factors for Esophageal Squamous Cell Carcinoma in Lilongwe Malawi: Results from the Lilongwe Esophageal Cancer Case: Control Study. PLOS Glob. Public Health 2022, 2, e0000135. [Google Scholar] [CrossRef]
- Asombang, A.W.; Chishinga, N.; Nkhoma, A.; Chipaila, J.; Nsokolo, B.; Manda-Mapalo, M.; Montiero, J.F.G.; Banda, L.; Dua, K.S. Systematic Review and Meta-Analysis of Esophageal Cancer in Africa: Epidemiology, Risk Factors, Management and Outcomes. World J. Gastroenterol. 2019, 25, 4512–4533. [Google Scholar] [CrossRef] [PubMed]
- Tran, G.D.; Sun, X.-D.; Abnet, C.C.; Fan, J.-H.; Dawsey, S.M.; Dong, Z.-W.; Mark, S.D.; Qiao, Y.-L.; Taylor, P.R. Prospective Study of Risk Factors for Esophageal and Gastric Cancers in the Linxian General Population Trial Cohort in China. Int. J. Cancer 2005, 113, 456–463. [Google Scholar] [CrossRef]
- Sheikh, M.; Poustchi, H.; Pourshams, A.; Etemadi, A.; Islami, F.; Khoshnia, M.; Gharavi, A.; Hashemian, M.; Roshandel, G.; Khademi, H.; et al. Individual and Combined Effects of Environmental Risk Factors for Esophageal Cancer Based on Results From the Golestan Cohort Study. Gastroenterology 2019, 156, 1416–1427. [Google Scholar] [CrossRef] [Green Version]
- Shen, Y.; Xie, S.; Zhao, L.; Song, G.; Shao, Y.; Hao, C.; Niu, C.; Ruan, X.; Zang, Z.; Nakyeyune, R.; et al. Estimating Individualized Absolute Risk for Esophageal Squamous Cell Carcinoma: A Population-Based Study in High-Risk Areas of China. Front. Oncol. 2021, 10, 598603. [Google Scholar] [CrossRef]
- Yang, X.; Chen, X.; Zhuang, M.; Yuan, Z.; Nie, S.; Lu, M.; Jin, L.; Ye, W. Smoking and Alcohol Drinking in Relation to the Risk of Esophageal Squamous Cell Carcinoma: A Population-Based Case-Control Study in China. Sci. Rep. 2017, 7, 17249. [Google Scholar] [CrossRef] [Green Version]
- Nasrollahzadeh, D.; Kamangar, F.; Aghcheli, K.; Sotoudeh, M.; Islami, F.; Abnet, C.C.; Shakeri, R.; Pourshams, A.; Marjani, H.A.; Nouraie, M.; et al. Opium, Tobacco, and Alcohol Use in Relation to Oesophageal Squamous Cell Carcinoma in a High-Risk Area of Iran. Br. J. Cancer 2008, 98, 1857–1863. [Google Scholar] [CrossRef] [Green Version]
- Moody, S.; Senkin, S.; Islam, S.M.A.; Wang, J.; Nasrollahzadeh, D.; Cortez Cardoso Penha, R.; Fitzgerald, S.; Bergstrom, E.N.; Atkins, J.; He, Y.; et al. Mutational Signatures in Esophageal Squamous Cell Carcinoma from Eight Countries with Varying Incidence. Nat. Genet. 2021, 53, 1553–1563. [Google Scholar] [CrossRef]
- Kamangar, F.; Chow, W.-H.; Abnet, C.C.; Dawsey, S.M. Environmental Causes of Esophageal Cancer. Gastroenterol. Clin. N. Am. 2009, 38, 27–57, vii. [Google Scholar] [CrossRef] [Green Version]
- Mamtani, R.; Cheema, S.; Sheikh, J.; Al Mulla, A.; Lowenfels, A.; Maisonneuve, P. Cancer Risk in Waterpipe Smokers: A Meta-Analysis. Int. J. Public Health 2017, 62, 73–83. [Google Scholar] [CrossRef] [Green Version]
- Montazeri, Z.; Nyiraneza, C.; El-Katerji, H.; Little, J. Waterpipe Smoking and Cancer: Systematic Review and Meta-Analysis. Tob. Control 2017, 26, 92–97. [Google Scholar] [CrossRef]
- McCormack, V.A.; Menya, D.; Munishi, M.O.; Dzamalala, C.; Gasmelseed, N.; Leon Roux, M.; Assefa, M.; Osano, O.; Watts, M.; Mwasamwaja, A.O.; et al. Informing Etiologic Research Priorities for Squamous Cell Esophageal Cancer in Africa: A Review of Setting-Specific Exposures to Known and Putative Risk Factors. Int. J. Cancer 2017, 140, 259–271. [Google Scholar] [CrossRef] [Green Version]
- Akhtar, S. Areca Nut Chewing and Esophageal Squamous-Cell Carcinoma Risk in Asians: A Meta-Analysis of Case-Control Studies. Cancer Causes Control 2013, 24, 257–265. [Google Scholar] [CrossRef]
- Gupta, S.; Gupta, R.; Sinha, D.N.; Mehrotra, R. Relationship between Type of Smokeless Tobacco & Risk of Cancer: A Systematic Review. Indian J. Med. Res. 2018, 148, 56–76. [Google Scholar] [CrossRef] [PubMed]
- Sinha, D.N.; Abdulkader, R.S.; Gupta, P.C. Smokeless Tobacco-Associated Cancers: A Systematic Review and Meta-Analysis of Indian Studies. Int. J. Cancer 2016, 138, 1368–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.-M.; Katki, H.A.; Graubard, B.I.; Kahle, L.L.; Chaturvedi, A.; Matthews, C.E.; Freedman, N.D.; Abnet, C.C. Population Attributable Risks of Subtypes of Esophageal and Gastric Cancers in the United States. Am. J. Gastroenterol. 2021, 116, 1844–1852. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.B.; Kamangar, F.; Whiteman, D.C.; Freedman, N.D.; Gammon, M.D.; Bernstein, L.; Brown, L.M.; Risch, H.A.; Ye, W.; Sharp, L.; et al. Cigarette Smoking and Adenocarcinomas of the Esophagus and Esophagogastric Junction: A Pooled Analysis From the International BEACON Consortium. J. Natl. Cancer Inst. 2010, 102, 1344–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tramacere, I.; La Vecchia, C.; Negri, E. Tobacco Smoking and Esophageal and Gastric Cardia Adenocarcinoma: A Meta-Analysis. Epidemiology 2011, 22, 344–349. [Google Scholar] [CrossRef]
- IARC. Alcohol Consumption and Ethyl Carbamate; IARC: Lyon, France, 2022; ISBN 978-92-832-1296-6. [Google Scholar]
- Tramacere, I.; Pelucchi, C.; Bagnardi, V.; Rota, M.; Scotti, L.; Islami, F.; Corrao, G.; Boffetta, P.; Vecchia, C.L.; Negri, E. A Meta-Analysis on Alcohol Drinking and Esophageal and Gastric Cardia Adenocarcinoma Risk. Ann. Oncol. 2012, 23, 287–297. [Google Scholar] [CrossRef]
- Yu, X.; Chen, J.; Jiang, W.; Zhang, D. Alcohol, Alcoholic Beverages and Risk of Esophageal Cancer by Histological Type: A Dose-Response Meta-Analysis of Observational Studies. Alcohol. Alcohol. 2020, 55, 457–467. [Google Scholar] [CrossRef]
- Nucci, D.; Marino, A.; Realdon, S.; Nardi, M.; Fatigoni, C.; Gianfredi, V. Lifestyle, WCRF/AICR Recommendations, and Esophageal Adenocarcinoma Risk: A Systematic Review of the Literature. Nutrients 2021, 13, 3525. [Google Scholar] [CrossRef]
- Middleton, D.R.S.; Mmbaga, B.T.; Menya, D.; Dzamalala, C.; Nyakunga-Maro, G.; Finch, P.; Mlombe, Y.; Schüz, J.; McCormack, V.; Kigen, N.; et al. Alcohol Consumption and Oesophageal Squamous Cell Cancer Risk in East Africa: Findings from the Large Multicentre ESCCAPE Case-Control Study in Kenya, Tanzania, and Malawi. Lancet Glob. Health 2022, 10, e236–e245. [Google Scholar] [CrossRef]
- IARC Monographs on the Identification of Carcinogenic Hazards to Humans. Volume 126 Opium Consumption; IARC: Lyon, France, 2021; Volume 126, pp. 1–253. [Google Scholar]
- Shakeri, R.; Kamangar, F.; Mohamadnejad, M.; Tabrizi, R.; Zamani, F.; Mohamadkhani, A.; Nikfam, S.; Nikmanesh, A.; Sotoudeh, M.; Sotoudehmanesh, R.; et al. Opium Use, Cigarette Smoking, and Alcohol Consumption in Relation to Pancreatic Cancer. Medicine 2016, 95, e3922. [Google Scholar] [CrossRef]
- Pournaghi, S.-J.; Hojjat, S.K.; Noveyri, F.B.; Ghouchani, H.T.; Ahmadi, A.; Hamedi, A.; Rahimi, J.; Mohamaddoust, H.; Lashkardoost, H. Tobacco Consumption, Opium Use, Alcohol Drinking and the Risk of Esophageal Cancer in North Khorasan, Iran. J. Subst. Use 2019, 24, 105–109. [Google Scholar] [CrossRef]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Drinking Coffee, Mate, and Very Hot Beverages; IARC: Lyon, France, 2018; Volume 116, ISBN 978-92-832-0154-0. [Google Scholar]
- Luo, H.; Ge, H. Hot Tea Consumption and Esophageal Cancer Risk: A Meta-Analysis of Observational Studies. Front. Nutr. 2022, 9, 831567. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Tong, Y.; Yang, C.; Gan, Y.; Sun, H.; Bi, H.; Cao, S.; Yin, X.; Lu, Z. Consumption of Hot Beverages and Foods and the Risk of Esophageal Cancer: A Meta-Analysis of Observational Studies. BMC Cancer 2015, 15, 449. [Google Scholar] [CrossRef] [Green Version]
- Andrici, J.; Eslick, G.D. Hot Food and Beverage Consumption and the Risk of Esophageal Cancer: A Meta-Analysis. Am. J. Prev. Med. 2015, 49, 952–960. [Google Scholar] [CrossRef]
- Zhong, Y.; Yang, C.; Wang, N.; Pan, D.; Wang, S.; Sun, G. Hot Tea Drinking and the Risk of Esophageal Cancer: A Systematic Review and Meta-Analysis. Nutr. Cancer 2022, 74, 2384–2391. [Google Scholar] [CrossRef]
- Islami, F.; Poustchi, H.; Pourshams, A.; Khoshnia, M.; Gharavi, A.; Kamangar, F.; Dawsey, S.M.; Abnet, C.C.; Brennan, P.; Sheikh, M.; et al. A Prospective Study of Tea Drinking Temperature and Risk of Esophageal Squamous Cell Carcinoma. Int. J. Cancer 2020, 146, 18–25. [Google Scholar] [CrossRef]
- Masukume, G.; Mmbaga, B.T.; Dzamalala, C.P.; Mlombe, Y.B.; Finch, P.; Nyakunga-Maro, G.; Mremi, A.; Middleton, D.R.S.; Narh, C.T.; Chasimpha, S.J.D.; et al. A Very-Hot Food and Beverage Thermal Exposure Index and Esophageal Cancer Risk in Malawi and Tanzania: Findings from the ESCCAPE Case-Control Studies. Br. J. Cancer 2022, 127, 1106–1115. [Google Scholar] [CrossRef]
- Dar, N.A.; Bhat, G.A.; Shah, I.A.; Iqbal, B.; Rafiq, R.; Nabi, S.; Lone, M.M.; Islami, F.; Boffetta, P. Salt Tea Consumption and Esophageal Cancer: A Possible Role of Alkaline Beverages in Esophageal Carcinogenesis. Int. J. Cancer 2015, 136, E704–E710. [Google Scholar] [CrossRef]
- Deybasso, H.A.; Roba, K.T.; Nega, B.; Belachew, T. Dietary and Environmental Determinants of Oesophageal Cancer in Arsi Zone, Oromia, Central Ethiopia: A Case–Control Study. Cancer Manag. Res. 2021, 13, 2071–2082. [Google Scholar] [CrossRef]
- Lubin, J.H.; De Stefani, E.; Abnet, C.C.; Acosta, G.; Boffetta, P.; Victora, C.; Graubard, B.I.; Muñoz, N.; Deneo-Pellegrini, H.; Franceschi, S.; et al. Maté Drinking and Esophageal Squamous Cell Carcinoma in South America: Pooled Results from Two Large Multicenter Case–Control Studies. Cancer Epidemiol. Biomark. Prev. 2014, 23, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Cunha, L.; Fontes, F.; Come, J.; Lobo, V.; Santos, L.L.; Lunet, N.; Carrilho, C. Risk Factors for Oesophageal Squamous Cell Carcinoma in Mozambique. Available online: http://ecancer.org/en/journal/article/1437-risk-factors-for-oesophageal-squamous-cell-carcinoma-in-mozambique (accessed on 3 October 2022).
- Lin, S.; Xu, G.; Chen, Z.; Liu, X.; Li, J.; Ma, L.; Wang, X. Tea Drinking and the Risk of Esophageal Cancer: Focus on Tea Type and Drinking Temperature. Eur. J. Cancer Prev. 2020, 29, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Niu, C.; Liu, Y.; Wang, J.; Liu, Y.; Zhang, S.; Zhang, Y.; Zhang, L.; Zhao, D.; Liu, F.; Chao, L.; et al. Risk Factors for Esophageal Squamous Cell Carcinoma and Its Histological Precursor Lesions in China: A Multicenter Cross-Sectional Study. BMC Cancer 2021, 21, 1034. [Google Scholar] [CrossRef] [PubMed]
- Middleton, D.R.; Menya, D.; Kigen, N.; Oduor, M.; Maina, S.K.; Some, F.; Chumba, D.; Ayuo, P.; Osano, O.; Schüz, J.; et al. Hot Beverages and Oesophageal Cancer Risk in Western Kenya: Findings from the ESCCAPE Case–Control Study. Int. J. Cancer 2019, 144, 2669–2676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckle, G.C.; Mmbaga, E.J.; Paciorek, A.; Akoko, L.; Deardorff, K.; Mgisha, W.; Mushi, B.P.; Mwaiselage, J.; Hiatt, R.A.; Zhang, L.; et al. Risk Factors Associated With Early-Onset Esophageal Cancer in Tanzania. JCO Glob. Oncol. 2022, 8, e2100256. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Chen, Q.; Xia, H.; Lin, J. Green Tea Drinking Habits and Esophageal Cancer in Southern China: A Case-Control Study. Asian Pac. J. Cancer Prev. 2011, 12, 229–233. [Google Scholar]
- Tai, W.-P.; Nie, G.-J.; Chen, M.-J.; Yaz, T.Y.; Guli, A.; Wuxur, A.; Huang, Q.-Q.; Lin, Z.-G.; Wu, J. Hot Food and Beverage Consumption and the Risk of Esophageal Squamous Cell Carcinoma. Medicine 2017, 96, e9325. [Google Scholar] [CrossRef]
- De Jong, U.W.; Day, N.E.; Mounier-Kuhn, P.L.; Haguenauer, J.P. The Relationship between the Ingestion of Hot Coffee and Intraoesophageal Temperature. Gut 1972, 13, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Jansson, C.; Johansson, A.L.V.; Nyrén, O.; Lagergren, J. Socioeconomic Factors and Risk of Esophageal Adenocarcinoma: A Nationwide Swedish Case-Control Study. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1754–1761. [Google Scholar] [CrossRef] [Green Version]
- Islami, F.; Kamangar, F.; Nasrollahzadeh, D.; Aghcheli, K.; Sotoudeh, M.; Abedi-Ardekani, B.; Merat, S.; Nasseri-Moghaddam, S.; Semnani, S.; Sepehr, A.; et al. Socio-Economic Status and Oesophageal Cancer: Results from a Population-Based Case–Control Study in a High-Risk Area. Int. J. Epidemiol. 2009, 38, 978–988. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.-L.; Gao, J.-C.; Zhang, Y.-H. Association of Socioeconomic Status with Risk of Esophageal Cancer: A Meta-Analysis. In Proceedings of the 2021 11th International Conference on Information Technology in Medicine and Education (ITME), Fujian, China, 19–21 November 2021; pp. 324–329. [Google Scholar]
- Xie, S.-H.; Lagergren, J. Social Group Disparities in the Incidence and Prognosis of Oesophageal Cancer. United Eur. Gastroenterol. J. 2018, 6, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Mmbaga, E.J.; Mushi, B.P.; Deardorff, K.; Mgisha, W.; Akoko, L.O.; Paciorek, A.; Hiatt, R.A.; Buckle, G.C.; Mwaiselage, J.; Zhang, L.; et al. A Case-Control Study to Evaluate Environmental and Lifestyle Risk Factors for Esophageal Cancer in Tanzania. Cancer Epidemiol. Biomark. Prev. 2021, 30, 305–316. [Google Scholar] [CrossRef]
- Kou, K.; Baade, P.D.; Guo, X.; Gatton, M.; Cramb, S.; Lu, Z.; Fu, Z.; Chu, J.; Xu, A.; Sun, J. Area Socioeconomic Status Is Independently Associated with Esophageal Cancer Mortality in Shandong, China. Sci. Rep. 2019, 9, 6388. [Google Scholar] [CrossRef] [Green Version]
- Adler, N.E.; Newman, K. Socioeconomic Disparities in Health: Pathways and Policies. Health Aff. 2002, 21, 60–76. [Google Scholar] [CrossRef]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Household Use of Solid Fuels and High-Temperature Frying; IARC: Lyon, France, 2010; Volume 95, pp. 1–430. [Google Scholar]
- Sheikh, M.; Poustchi, H.; Pourshams, A.; Khoshnia, M.; Gharavi, A.; Zahedi, M.; Roshandel, G.; Sepanlou, S.G.; Fazel, A.; Hashemian, M.; et al. Household Fuel Use and the Risk of Gastrointestinal Cancers: The Golestan Cohort Study. Environ. Health Perspect. 2020, 128, 067002. [Google Scholar] [CrossRef]
- Kayamba, V.; Mulenga, C.; Mubbunu, M.; Kazhila, L.; Hodges, P.; Kelly, P. Association between Oesophageal Cancer and Biomass Smoke Exposure: A Case-Control Study. eCancer 2022, 16, 1422. [Google Scholar] [CrossRef]
- Mmbaga, E.; Deardorff, K.; Mushi, B.; Zhang, L.; Mgisha, W.; Parikh, A.; Hiatt, R.A.; Mwaiselage, J.; Van Loon, K. A Case-Control Study to Evaluate the Etiology of Esophageal Cancer in Tanzania. JGO 2016, 2, 5s. [Google Scholar] [CrossRef]
- Kayamba, V.; Bateman, A.C.; Asombang, A.W.; Shibemba, A.; Zyambo, K.; Banda, T.; Soko, R.; Kelly, P. HIV Infection and Domestic Smoke Exposure, but Not Human Papillomavirus, Are Risk Factors for Esophageal Squamous Cell Carcinoma in Zambia: A Case-Control Study. Cancer Med. 2015, 4, 588–595. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Zhang, T.; Wu, W.; Zhao, D.; Zhang, N.; Cui, Y.; Liu, Y.; Gu, J.; Lu, P.; Xue, F.; et al. Risk Factors Associated with Precancerous Lesions of Esophageal Squamous Cell Carcinoma: A Screening Study in a High Risk Chinese Population. J. Cancer 2019, 10, 3284–3290. [Google Scholar] [CrossRef] [Green Version]
- Golozar, A.; Etemadi, A.; Kamangar, F.; Fazeltabar Malekshah, A.; Islami, F.; Nasrollahzadeh, D.; Abedi-Ardekani, B.; Khoshnia, M.; Pourshams, A.; Semnani, S.; et al. Food Preparation Methods, Drinking Water Source, and Esophageal Squamous Cell Carcinoma in the High-Risk Area of Golestan, Northeast Iran. Eur. J. Cancer Prev. 2016, 25, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Menya, D.; Maina, S.K.; Kibosia, C.; Kigen, N.; Oduor, M.; Some, F.; Chumba, D.; Ayuo, P.; Middleton, D.R.S.; Osano, O.; et al. Dental Fluorosis and Oral Health in the African Esophageal Cancer Corridor: Findings from the Kenya ESCCAPE Case–Control Study and a Pan-African Perspective. Int. J. Cancer 2019, 145, 99–109. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.H.; deKok, T.M.; Levallois, P.; Brender, J.; Gulis, G.; Nolan, B.T.; VanDerslice, J. International Society for Environmental Epidemiology Workgroup Report: Drinking-Water Nitrate and Health--Recent Findings and Research Needs. Environ. Health Perspect. 2005, 113, 1607–1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keshavarzi, B.; Moore, F.; Najmeddin, A.; Rahmani, F.; Malekzadeh, A. Quality of Drinking Water and High Incidence Rate of Esophageal Cancer in Golestan Province of Iran: A Probable Link. Environ. Geochem. Health 2012, 34, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Yu, C.; Wen, D.; Chen, J.; Ling, Y.; Terajima, K.; Akazawa, K.; Shan, B.; Wang, S. Association of Nitrogen Compounds in Drinking Water with Incidence of Esophageal Squamous Cell Carcinoma in Shexian, China. Tohoku J. Exp. Med. 2012, 226, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Yokokawa, Y.; Ohta, S.; Hou, J.; Zhang, X.L.; Li, S.S.; Ping, Y.M.; Nakajima, T. Ecological Study on the Risks of Esophageal Cancer in Ci-Xian, China: The Importance of Nutritional Status and the Use of Well Water. Int. J. Cancer 1999, 83, 620–624. [Google Scholar] [CrossRef]
- Ostry, V.; Malir, F.; Toman, J.; Grosse, Y. Mycotoxins as Human Carcinogens-the IARC Monographs Classification. Mycotoxin Res. 2017, 33, 65–73. [Google Scholar] [CrossRef]
- Chu, F.S.; Li, G.Y. Simultaneous Occurrence of Fumonisin B1 and Other Mycotoxins in Moldy Corn Collected from the People’s Republic of China in Regions with High Incidences of Esophageal Cancer. Appl. Environ. Microbiol. 1994, 60, 847–852. [Google Scholar] [CrossRef] [Green Version]
- Yoshizawa, T.; Yamashita, A.; Luo, Y. Fumonisin Occurrence in Corn from High- and Low-Risk Areas for Human Esophageal Cancer in China. Appl. Environ. Microbiol. 1994, 60, 1626–1629. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Wei, H.; Ma, J.; Luo, X. The Fumonisin B1 Content in Corn from North China, a High-Risk Area of Esophageal Cancer. J. Environ. Pathol. Toxicol. Oncol. 2000, 19, 139–141. [Google Scholar]
- Shephard, G.S.; Marasas, W.F.O.; Leggott, N.L.; Yazdanpanah, H.; Rahimian, H.; Safavi, N. Natural Occurrence of Fumonisins in Corn from Iran. J. Agric. Food Chem. 2000, 48, 1860–1864. [Google Scholar] [CrossRef]
- Alizadeh, A.M.; Rohandel, G.; Roudbarmohammadi, S.; Roudbary, M.; Sohanaki, H.; Ghiasian, S.A.; Taherkhani, A.; Semnani, S.; Aghasi, M. Fumonisin B1 Contamination of Cereals and Risk of Esophageal Cancer in a High Risk Area in Northeastern Iran. Asian Pac. J. Cancer Prev. 2012, 13, 2625–2628. [Google Scholar] [CrossRef] [Green Version]
- Rheeder, J.P. Fusarium Moniliformeand Fumonisins in Corn in Relation to Human Esophageal Cancer in Transkei. Cytopathology 1992, 82, 353–357. [Google Scholar] [CrossRef]
- Sydenham, E.W.; Thiel, P.G.; Marasas, W.F.O.; Shephard, G.S.; Van Schalkwyk, D.J.; Koch, K.R. Natural Occurrence of Some Fusarium Mycotoxins in Corn from Low and High Esophageal Cancer Prevalence Areas of the Transkei, Southern Africa. J. Agric. Food Chem. 1990, 38, 1900–1903. [Google Scholar] [CrossRef]
- Ghasemi-Kebria, F.; Joshaghani, H.; Taheri, N.S.; Semnani, S.; Aarabi, M.; Salamat, F.; Roshandel, G. Aflatoxin Contamination of Wheat Flour and the Risk of Esophageal Cancer in a High Risk Area in Iran. Cancer Epidemiol. 2013, 37, 290–293. [Google Scholar] [CrossRef] [Green Version]
- Mwalwayo, D.S.; Thole, B. Prevalence of Aflatoxin and Fumonisins (B1+B2) in Maize Consumed in Rural Malawi. Toxicol. Rep. 2016, 3, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Abnet, C.C.; Borkowf, C.B.; Qiao, Y.L.; Albert, P.S.; Wang, E.; Merrill, A.H.; Mark, S.D.; Dong, Z.W.; Taylor, P.R.; Dawsey, S.M. Sphingolipids as Biomarkers of Fumonisin Exposure and Risk of Esophageal Squamous Cell Carcinoma in China. Cancer Causes Control 2001, 12, 821–828. [Google Scholar] [CrossRef]
- Xue, K.S.; Tang, L.; Sun, G.; Wang, S.; Hu, X.; Wang, J.-S. Mycotoxin Exposure Is Associated with Increased Risk of Esophageal Squamous Cell Carcinoma in Huaian Area, China. BMC Cancer 2019, 19, 1218. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Pan, D.; Zhang, T.; Su, M.; Sun, G.; Wei, J.; Guo, Z.; Wang, K.; Song, G.; Yan, Q. Corn Flour Intake, Aflatoxin B1 Exposure, and Risk of Esophageal Precancerous Lesions in a High-Risk Area of Huai’an, China: A Case-Control Study. Toxins 2020, 12, 299. [Google Scholar] [CrossRef]
- Nasrollahzadeh, D.; Ye, W.; Shakeri, R.; Sotoudeh, M.; Merat, S.; Kamangar, F.; Abnet, C.C.; Islami, F.; Boffetta, P.; Dawsey, S.M.; et al. Contact with Ruminants Is Associated with Esophageal Squamous Cell Carcinoma Risk. Int. J. Cancer 2015, 136, 1468–1474. [Google Scholar] [CrossRef]
- Dar, N.A.; Islami, F.; Bhat, G.A.; Shah, I.A.; Makhdoomi, M.A.; Iqbal, B.; Rafiq, R.; Lone, M.M.; Boffetta, P. Contact with Animals and Risk of Oesophageal Squamous Cell Carcinoma: Outcome of a Case-Control Study from Kashmir, a High-Risk Region. Occup. Environ. Med. 2014, 71, 208–214. [Google Scholar] [CrossRef]
- Miller, H.K.; Stoddard, R.A.; Dawsey, S.M.; Nasrollahzadeh, D.; Abnet, C.C.; Etemadi, A.; Kamangar, F.; Murphy, G.; Sotoudeh, M.; Kersh, G.J.; et al. Association Between Serological Responses to Two Zoonotic Ruminant Pathogens and Esophageal Squamous Cell Carcinoma. Vector-Borne Zoonotic Dis. 2021, 21, 125–127. [Google Scholar] [CrossRef]
- Cook, M.B.; Corley, D.A.; Murray, L.J.; Liao, L.M.; Kamangar, F.; Ye, W.; Gammon, M.D.; Risch, H.A.; Casson, A.G.; Freedman, N.D.; et al. Gastroesophageal Reflux in Relation to Adenocarcinomas of the Esophagus: A Pooled Analysis from the Barrett’s and Esophageal Adenocarcinoma Consortium (BEACON). PLoS ONE 2014, 9, e103508. [Google Scholar] [CrossRef] [PubMed]
- Eusebi, L.H.; Telese, A.; Cirota, G.G.; Haidry, R.; Zagari, R.M.; Bazzoli, F.; Ford, A.C. Effect of Gastro-Esophageal Reflux Symptoms on the Risk of Barrett’s Esophagus: A Systematic Review and Meta-Analysis. J. Gastroenterol. Hepatol. 2022, 37, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Li, L.; Huang, X.; Yang, C.; Liang, X.; Zhao, Y.; Xie, J.; Chen, R.; Wang, D.; Xie, S. Associations between Gastro-Oesophageal Reflux Disease and a Range of Diseases: An Umbrella Review of Systematic Reviews and Meta-Analyses. BMJ Open 2020, 10, e038450. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.M.; Freedman, N.D.; Katki, H.A.; Matthews, C.; Graubard, B.I.; Kahle, L.L.; Abnet, C.C. Gastroesophageal Reflux Disease: A Risk Factor for Laryngeal Squamous Cell Carcinoma and Esophageal Squamous Cell Carcinoma in the NIH-AARP Diet and Health Study Cohort. Cancer 2021, 127, 1871–1879. [Google Scholar] [CrossRef] [PubMed]
- Soroush, A.; Malekzadeh, R.; Roshandel, G.; Khoshnia, M.; Poustchi, H.; Kamangar, F.; Brennan, P.; Boffetta, P.; Dawsey, S.M.; Abnet, C.C.; et al. Sex and Smoking Differences in the Association between Gastroesophageal Reflux and Risk of Esophageal Squamous Cell Carcinoma in a High-Incidence Area: Golestan Cohort Study. Int. J. Cancer 2023, 152, 1137–1149. [Google Scholar] [CrossRef]
- Tian, J.; Zuo, C.; Liu, G.; Che, P.; Li, G.; Li, X.; Chen, H. Cumulative Evidence for the Relationship between Body Mass Index and the Risk of Esophageal Cancer: An Updated Meta-Analysis with Evidence from 25 Observational Studies. J. Gastroenterol. Hepatol. 2020, 35, 730–743. [Google Scholar] [CrossRef]
- Lahmann, P.H.; Pandeya, N.; Webb, P.M.; Green, A.C.; Whiteman, D.C. Australian Cancer Study Body Mass Index, Long-Term Weight Change, and Esophageal Squamous Cell Carcinoma: Is the Inverse Association Modified by Smoking Status? Cancer 2012, 118, 1901–1909. [Google Scholar] [CrossRef]
- Wang, S.-M.; Fan, J.-H.; Jia, M.-M.; Yang, Z.; Zhang, Y.-Q.; Qiao, Y.-L.; Taylor, P.R. Body Mass Index and Long-Term Risk of Death from Esophageal Squamous Cell Carcinoma in a Chinese Population. Thorac. Cancer 2016, 7, 387–392. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, T.; Yin, X.; Yuan, Z.; Chen, H.; Plymoth, A.; Jin, L.; Chen, X.; Lu, M.; Ye, W. Adult Height, Body Mass Index Change, and Body Shape Change in Relation to Esophageal Squamous Cell Carcinoma Risk: A Population-based Case-control Study in China. Cancer Med. 2019, 8, 5769–5778. [Google Scholar] [CrossRef] [Green Version]
- Islami, F.; Sheikhattari, P.; Ren, J.S.; Kamangar, F. Gastric Atrophy and Risk of Oesophageal Cancer and Gastric Cardia Adenocarcinoma—A Systematic Review and Meta-Analysis. Ann. Oncol. 2011, 22, 754–760. [Google Scholar] [CrossRef]
- Nasrollahzadeh, D.; Malekzadeh, R.; Aghcheli, K.; Sotoudeh, M.; Merat, S.; Islami, F.; Kamangar, F.; Abnet, C.C.; Shakeri, R.; Pourshams, A.; et al. Gastric Atrophy and Oesophageal Squamous Cell Carcinoma: Possible Interaction with Dental Health and Oral Hygiene Habit. Br. J. Cancer 2012, 107, 888–894. [Google Scholar] [CrossRef] [Green Version]
- Almodova Ede, C.; de Oliveira, W.K.; Machado, L.F.A.; Grejo, J.R.; da Cunha, T.R.; Colaiacovo, W.; Ortolan, E.V.P. Atrophic Gastritis: Risk Factor for Esophageal Squamous Cell Carcinoma in a Latin-American Population. World J. Gastroenterol. 2013, 19, 2060–2064. [Google Scholar] [CrossRef]
- Ekheden, I.; Yang, X.; Chen, H.; Chen, X.; Yuan, Z.; Jin, L.; Lu, M.; Ye, W. Associations Between Gastric Atrophy and Its Interaction With Poor Oral Health and the Risk for Esophageal Squamous Cell Carcinoma in a High-Risk Region of China: A Population-Based Case-Control Study. Am. J. Epidemiol. 2020, 189, 931–941. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.-X.; Yan, L.-B.; Xie, P.; Hu, P.; Zhao, W.; Lu, Y.; Xing, X.; Liu, X. Association of Serum Pepsinogens With Esophageal Squamous Cell Carcinoma Risk: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 928672. [Google Scholar] [CrossRef]
- Yano, Y.; Fan, J.-H.; Dawsey, S.M.; Qiao, Y.-L.; Abnet, C.C. A Long-Term Follow-up Analysis of Associations between Tooth Loss and Multiple Cancers in the Linxian General Population Cohort. J. Natl. Cancer Cent. 2021, 1, 39–43. [Google Scholar] [CrossRef]
- Chen, X.; Yuan, Z.; Lu, M.; Zhang, Y.; Jin, L.; Ye, W. Poor Oral Health Is Associated with an Increased Risk of Esophageal Squamous Cell Carcinoma—A Population-Based Case-Control Study in China. Int. J. Cancer 2017, 140, 626–635. [Google Scholar] [CrossRef]
- Abnet, C.C.; Qiao, Y.-L.; Mark, S.D.; Dong, Z.-W.; Taylor, P.R.; Dawsey, S.M. Prospective Study of Tooth Loss and Incident Esophageal and Gastric Cancers in China. Cancer Causes Control 2001, 12, 847–854. [Google Scholar] [CrossRef]
- Zhao, R.; Li, X.; Yang, X.; Zhang, T.; Lu, M.; Ye, W.; Jin, L.; Suo, C.; Chen, X. Association of Esophageal Squamous Cell Carcinoma With the Interaction Between Poor Oral Health and Single Nucleotide Polymorphisms in Regulating Cell Cycles and Angiogenesis: A Case-Control Study in High-Incidence Chinese. Cancer Control 2022, 29, 10732748221075812. [Google Scholar] [CrossRef]
- Sepehr, A.; Kamangar, F.; Fahimi, S.; Saidi, F.; Abnet, C.C.; Dawsey, S.M. Poor Oral Health as a Risk Factor for Esophageal Squamous Dysplasia in Northeastern Iran. Anticancer Res. 2005, 25, 543–546. [Google Scholar]
- Dar, N.A.; Islami, F.; Bhat, G.A.; Shah, I.A.; Makhdoomi, M.A.; Iqbal, B.; Rafiq, R.; Lone, M.M.; Abnet, C.C.; Boffetta, P. Poor Oral Hygiene and Risk of Esophageal Squamous Cell Carcinoma in Kashmir. Br. J. Cancer 2013, 109, 1367–1372. [Google Scholar] [CrossRef] [Green Version]
- Mmbaga, B.T.; Mwasamwaja, A.; Mushi, G.; Mremi, A.; Nyakunga, G.; Kiwelu, I.; Swai, R.; Kiwelu, G.; Mustapha, S.; Mghase, E.; et al. Missing and Decayed Teeth, Oral Hygiene and Dental Staining in Relation to Esophageal Cancer Risk: ESCCAPE Case-Control Study in Kilimanjaro, Tanzania. Int. J. Cancer 2021, 148, 2416–2428. [Google Scholar] [CrossRef]
- Guha, N.; Boffetta, P.; Wünsch Filho, V.; Eluf Neto, J.; Shangina, O.; Zaridze, D.; Curado, M.P.; Koifman, S.; Matos, E.; Menezes, A.; et al. Oral Health and Risk of Squamous Cell Carcinoma of the Head and Neck and Esophagus: Results of Two Multicentric Case-Control Studies. Am. J. Epidemiol. 2007, 166, 1159–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ljung, R.; Martin, L.; Lagergren, J. Oral Disease and Risk of Oesophageal and Gastric Cancer in a Nationwide Nested Case-Control Study in Sweden. Eur. J. Cancer 2011, 47, 2128–2132. [Google Scholar] [CrossRef]
- Jordão, H.W.; McKenna, G.; McMenamin, Ú.C.; Kunzmann, A.T.; Murray, L.J.; Coleman, H.G. The Association between Self-Reported Poor Oral Health and Gastrointestinal Cancer Risk in the UK Biobank: A Large Prospective Cohort Study. United Eur. Gastroenterol. J. 2019, 7, 1241–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abnet, C.C.; Kamangar, F.; Dawsey, S.M.; Stolzenberg-Solomon, R.Z.; Albanes, D.; Pietinen, P.; Virtamo, J.; Taylor, P.R. Tooth Loss Is Associated with Increased Risk of Gastric Non-Cardia Adenocarcinoma in a Cohort of Finnish Smokers. Scand. J. Gastroenterol. 2005, 40, 681–687. [Google Scholar] [CrossRef]
- Zhang, J.; Bellocco, R.; Sandborgh-Englund, G.; Yu, J.; Sällberg Chen, M.; Ye, W. Poor Oral Health and Esophageal Cancer Risk: A Nationwide Cohort Study. Cancer Epidemiol. Biomark. Prev. 2022, 31, 1418–1425. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Nie, S.; Zhu, Y.; Lu, M. Teeth Loss, Teeth Brushing and Esophageal Carcinoma: A Systematic Review and Meta-Analysis. Sci. Rep. 2015, 5, 15203. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.-L.; Zeng, X.-T.; Luo, Z.-X.; Duan, X.-L.; Qin, J.; Leng, W.-D. Tooth Loss Is Associated with Increased Risk of Esophageal Cancer: Evidence from a Meta-Analysis with Dose-Response Analysis. Sci. Rep. 2016, 6, 18900. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Peng, J.; Li, Y.; Luo, H.; Huang, G.; Luo, S.; Yin, X.; Song, J. Association between Tooth Loss and Risk of Oesophageal Cancer: A Dose–Response Meta-Analysis. SpringerPlus 2016, 5, 1020. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Wang, J.; Zhang, Q.; Xia, T.; Hu, S.; Yao, W.; Wei, L. Association between the Frequency of Tooth Brushing and Esophageal Carcinoma Risk: An Update Systematic Review and Meta-Analysis. J. Gastrointest. Oncol. 2022, 13, 499–509. [Google Scholar] [CrossRef]
- Yano, Y.; Etemadi, A.; Abnet, C.C. Microbiome and Cancers of the Esophagus: A Review. Microorganisms 2021, 9, 1764. [Google Scholar] [CrossRef]
- Chen, X.; Winckler, B.; Lu, M.; Cheng, H.; Yuan, Z.; Yang, Y.; Jin, L.; Ye, W. Oral Microbiota and Risk for Esophageal Squamous Cell Carcinoma in a High-Risk Area of China. PLoS ONE 2015, 10, e0143603. [Google Scholar] [CrossRef]
- Wang, Q.; Rao, Y.; Guo, X.; Liu, N.; Liu, S.; Wen, P.; Li, S.; Li, Y. Oral Microbiome in Patients with Oesophageal Squamous Cell Carcinoma. Sci. Rep. 2019, 9, 19055. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Q.; Yang, T.; Yan, Y.; Zhang, Y.; Li, Z.; Wang, Y.; Yang, J.; Xia, Y.; Xiao, H.; Han, H.; et al. Alterations of Oral Microbiota in Chinese Patients With Esophageal Cancer. Front. Cell. Infect. Microbiol. 2020, 10, 541144. [Google Scholar] [CrossRef]
- Liu, F.; Liu, M.; Liu, Y.; Guo, C.; Zhou, Y.; Li, F.; Xu, R.; Liu, Z.; Deng, Q.; Li, X.; et al. Oral Microbiome and Risk of Malignant Esophageal Lesions in a High-Risk Area of China: A Nested Case-Control Study. Chin. J. Cancer Res. 2020, 32, 742–754. [Google Scholar] [CrossRef]
- Shao, D.; Vogtmann, E.; Liu, A.; Qin, J.; Chen, W.; Abnet, C.C.; Wei, W. Microbial Characterization of Esophageal Squamous Cell Carcinoma and Gastric Cardia Adenocarcinoma from a High-Risk Region of China. Cancer 2019, 125, 3993–4002. [Google Scholar] [CrossRef]
- Li, D.; He, R.; Hou, G.; Ming, W.; Fan, T.; Chen, L.; Zhang, L.; Jiang, W.; Wang, W.; Lu, Z.; et al. Characterization of the Esophageal Microbiota and Prediction of the Metabolic Pathways Involved in Esophageal Cancer. Front. Cell Infect. Microbiol. 2020, 10, 268. [Google Scholar] [CrossRef]
- Nasrollahzadeh, D.; Malekzadeh, R.; Ploner, A.; Shakeri, R.; Sotoudeh, M.; Fahimi, S.; Nasseri-Moghaddam, S.; Kamangar, F.; Abnet, C.C.; Winckler, B.; et al. Variations of Gastric Corpus Microbiota Are Associated with Early Esophageal Squamous Cell Carcinoma and Squamous Dysplasia. Sci. Rep. 2015, 5, 8820. [Google Scholar] [CrossRef] [Green Version]
- Yu, G.; Gail, M.H.; Shi, J.; Klepac-Ceraj, V.; Paster, B.J.; Dye, B.A.; Wang, G.-Q.; Wei, W.-Q.; Fan, J.-H.; Qiao, Y.-L.; et al. Association between Upper Digestive Tract Microbiota and Cancer-Predisposing States in the Esophagus and Stomach. Cancer Epidemiol. Biomark. Prev. 2014, 23, 735–741. [Google Scholar] [CrossRef] [Green Version]
- Snider, E.J.; Compres, G.; Freedberg, D.E.; Giddins, M.J.; Khiabanian, H.; Lightdale, C.J.; Nobel, Y.R.; Toussaint, N.C.; Uhlemann, A.-C.; Abrams, J.A. Barrett’s Esophagus Is Associated with a Distinct Oral Microbiome. Clin. Transl. Gastroenterol. 2018, 9, 135. [Google Scholar] [CrossRef]
- Peters, B.A.; Wu, J.; Pei, Z.; Yang, L.; Purdue, M.P.; Freedman, N.D.; Jacobs, E.J.; Gapstur, S.M.; Hayes, R.B.; Ahn, J. Oral Microbiome Composition Reflects Prospective Risk for Esophageal Cancers. Cancer Res. 2017, 77, 6777–6787. [Google Scholar] [CrossRef] [Green Version]
- Elliott, D.R.F.; Walker, A.W.; O’Donovan, M.; Parkhill, J.; Fitzgerald, R.C. A Non-Endoscopic Device to Sample the Oesophageal Microbiota: A Case-Control Study. Lancet Gastroenterol. Hepatol. 2017, 2, 32–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackett, K.L.; Siddhi, S.S.; Cleary, S.; Steed, H.; Miller, M.H.; Macfarlane, S.; Macfarlane, G.T.; Dillon, J.F. Oesophageal Bacterial Biofilm Changes in Gastro-Oesophageal Reflux Disease, Barrett’s and Oesophageal Carcinoma: Association or Causality? Aliment. Pharmacol. Ther. 2013, 37, 1084–1092. [Google Scholar] [CrossRef] [PubMed]
- Lopetuso, L.R.; Severgnini, M.; Pecere, S.; Ponziani, F.R.; Boskoski, I.; Larghi, A.; Quaranta, G.; Masucci, L.; Ianiro, G.; Camboni, T.; et al. Esophageal Microbiome Signature in Patients with Barrett’s Esophagus and Esophageal Adenocarcinoma. PLoS ONE 2020, 15, e0231789. [Google Scholar] [CrossRef] [PubMed]
- Abnet, C.C.; Arnold, M.; Wei, W.-Q. Epidemiology of Esophageal Squamous Cell Carcinoma. Gastroenterology 2018, 154, 360–373. [Google Scholar] [CrossRef]
- Qin, X.; Jia, G.; Zhou, X.; Yang, Z. Diet and Esophageal Cancer Risk: An Umbrella Review of Systematic Reviews and Meta-Analyses of Observational Studies. Adv. Nutr. 2022, 13, 2207–2216. [Google Scholar] [CrossRef]
- World Cancer Research Fund International. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective: A Summary of the Third Expert Report; World Cancer Research Fund International: London, UK, 2018; ISBN 1-912259-46-X. [Google Scholar]
- Mozaffarian, D.; Rosenberg, I.; Uauy, R. History of Modern Nutrition Science—Implications for Current Research, Dietary Guidelines, and Food Policy. BMJ 2018, 361, k2392. [Google Scholar] [CrossRef] [Green Version]
- Li, W.Q.; Park, Y.; Wu, J.W.; Ren, J.S.; Goldstein, A.M.; Taylor, P.R.; Hollenbeck, A.R.; Freedman, N.D.; Abnet, C.C. Index-Based Dietary Patterns and Risk of Esophageal and Gastric Cancer in a Large Cohort Study. Clin. Gastroenterol. Hepatol. 2013, 11, 1130–1136.e2. [Google Scholar] [CrossRef] [Green Version]
- Schulpen, M.; Peeters, P.H.; van den Brandt, P.A. Mediterranean Diet Adherence and Risk of Esophageal and Gastric Cancer Subtypes in the Netherlands Cohort Study. Gastric Cancer 2019, 22, 663–674. [Google Scholar] [CrossRef] [Green Version]
- Shivappa, N.; Hébert, J.R.; Rashidkhani, B. Dietary Inflammatory Index and Risk of Esophageal Squamous Cell Cancer in a Case-Control Study from Iran. Nutr. Cancer 2015, 67, 1253–1259. [Google Scholar] [CrossRef] [Green Version]
- Shivappa, N.; Zucchetto, A.; Serraino, D.; Rossi, M.; La Vecchia, C.; Hébert, J.R. Dietary Inflammatory Index and Risk of Esophageal Squamous Cell Cancer in a Case-Control Study from Italy. Cancer Causes Control 2015, 26, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Realdon, S.; Antonello, A.; Arcidiacono, D.; Dassie, E.; Cavallin, F.; Fassan, M.; Nardi, M.T.; Alberti, A.; Rugge, M.; Battaglia, G. Adherence to WCRF/AICR Lifestyle Recommendations for Cancer Prevention and the Risk of Barrett’s Esophagus Onset and Evolution to Esophageal Adenocarcinoma: Results from a Pilot Study in a High-Risk Population. Eur. J. Nutr. 2016, 55, 1563–1571. [Google Scholar] [CrossRef] [PubMed]
- Romaguera, D.; Vergnaud, A.C.; Peeters, P.H.; van Gils, C.H.; Chan, D.S.; Ferrari, P.; Romieu, I.; Jenab, M.; Slimani, N.; Clavel-Chapelon, F.; et al. Is Concordance with World Cancer Research Fund/American Institute for Cancer Research Guidelines for Cancer Prevention Related to Subsequent Risk of Cancer? Results from the EPIC Study. Am. J. Clin. Nutr. 2012, 96, 150–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohse, T.; Faeh, D.; Bopp, M.; Rohrmann, S. Adherence to the Cancer Prevention Recommendations of the World Cancer Research Fund/American Institute for Cancer Research and Mortality: A Census-Linked Cohort. Am. J. Clin. Nutr. 2016, 104, 678–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IARC. Handbooks of Cancer Prevention Fruit and Vegetables; IARC: Lyon, France, 2023; Volume 8, ISBN 978-92-832-3008-3. [Google Scholar]
- Liu, J.; Wang, J.; Leng, Y.; Lv, C. Intake of Fruit and Vegetables and Risk of Esophageal Squamous Cell Carcinoma: A Meta-analysis of Observational Studies. Int. J. Cancer 2013, 133, 473–485. [Google Scholar] [CrossRef]
- Li, B.; Jiang, G.; Zhang, G.; Xue, Q.; Zhang, H.; Wang, C.; Zhao, T. Intake of Vegetables and Fruit and Risk of Esophageal Adenocarcinoma: A Meta-Analysis of Observational Studies. Eur. J. Nutr. 2014, 53, 1511–1521. [Google Scholar] [CrossRef]
- Ye, X.-Y.; Lai, Y.-T.; Song, W.-P.; Hu, Y. The Research Progress on the Association between Dietary Habits and Esophageal Cancer: A Narrative Review. Ann. Palliat. Med. 2021, 10, 6948–6956. [Google Scholar] [CrossRef]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Some Naturally Occurring Substances: Food Items and Constituents, Heterocyclic Aromatic Amines and Mycotoxins; IARC: Lyon, France, 1993; Volume 56, ISBN 978-92-832-1256-0. [Google Scholar]
- Islami, F.; Ren, J.-S.; Taylor, P.R.; Kamangar, F. Pickled Vegetables and the Risk of Oesophageal Cancer: A Meta-Analysis. Br. J. Cancer 2009, 101, 1641–1647. [Google Scholar] [CrossRef] [Green Version]
- Yan, B.; Zhang, L.; Shao, Z. Consumption of Processed and Pickled Food and Esophageal Cancer Risk: A Systematic Review and Meta-Analysis. Bull. Cancer 2018, 105, 992–1002. [Google Scholar] [CrossRef]
- Qu, X.; Ben, Q.; Jiang, Y. Consumption of Red and Processed Meat and Risk for Esophageal Squamous Cell Carcinoma Based on a Meta-Analysis. Ann. Epidemiol. 2013, 23, 762–770.e1. [Google Scholar] [CrossRef]
- Zhu, H.-C.; Yang, X.; Xu, L.-P.; Zhao, L.-J.; Tao, G.-Z.; Zhang, C.; Qin, Q.; Cai, J.; Ma, J.-X.; Mao, W.-D.; et al. Meat Consumption Is Associated with Esophageal Cancer Risk in a Meat- and Cancer-Histological-Type Dependent Manner. Dig. Dis. Sci. 2014, 59, 664–673. [Google Scholar] [CrossRef]
- Choi, Y.; Song, S.; Song, Y.; Lee, J.E. Consumption of Red and Processed Meat and Esophageal Cancer Risk: Meta-Analysis. World J. Gastroenterol. 2013, 19, 1020–1029. [Google Scholar] [CrossRef]
- Salehi, M.; Moradi-Lakeh, M.; Salehi, M.H.; Nojomi, M.; Kolahdooz, F. Meat, Fish, and Esophageal Cancer Risk: A Systematic Review and Dose-Response Meta-Analysis. Nutr. Rev. 2013, 71, 257–267. [Google Scholar] [CrossRef]
- Huang, W.; Han, Y.; Xu, J.; Zhu, W.; Li, Z. Red and Processed Meat Intake and Risk of Esophageal Adenocarcinoma: A Meta-Analysis of Observational Studies. Cancer Causes Control 2013, 24, 193–201. [Google Scholar] [CrossRef]
- Zhao, Z.; Wang, F.; Chen, D.; Zhang, C. Red and Processed Meat Consumption and Esophageal Cancer Risk: A Systematic Review and Meta-Analysis. Clin. Transl. Oncol. 2020, 22, 532–545. [Google Scholar] [CrossRef]
- Banda, K.-J.; Chiu, H.-Y.; Hu, S.H.; Yeh, H.-C.; Lin, K.-C.; Huang, H.-C. Associations of Dietary Carbohydrate and Salt Consumption with Esophageal Cancer Risk: A Systematic Review and Meta-Analysis of Observational Studies. Nutr. Rev. 2020, 78, 688–698. [Google Scholar] [CrossRef]
- Xuan, F.; Li, W.; Guo, X.; Liu, C. Dietary Carbohydrate Intake and the Risk of Esophageal Cancer: A Meta-Analysis. Biosci. Rep. 2020, 40, BSR20192576. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.J.; Li, J.; Huang, W.; Fang, Y.; Xiao, L.N.; Liao, Z.E. Fish Consumption and Risk of Esophageal Cancer and Its Subtypes: A Systematic Review and Meta-Analysis of Observational Studies. Eur. J. Clin. Nutr. 2013, 67, 147–154. [Google Scholar] [CrossRef] [Green Version]
- Jiang, G.; Li, B.; Liao, X.; Zhong, C. Poultry and Fish Intake and Risk of Esophageal Cancer: A Meta-Analysis of Observational Studies. Asia Pac. J. Clin. Oncol. 2016, 12, e82–e91. [Google Scholar] [CrossRef]
- Li, B.-L.; Jiang, G.-X.; Xue, Q.; Zhang, H.; Wang, C.; Zhang, G.-X.; Xu, Z.-Y. Dairy Consumption and Risk of Esophageal Squamous Cell Carcinoma: A Meta-Analysis of Observational Studies. Asia Pac. J. Clin. Oncol. 2016, 12, e269–e279. [Google Scholar] [CrossRef]
- He, D.; Huang, X.; Wang, Z.-P.; Chen, D.; Chen, J.; Duan, C.-Y. Dietary Fat Intake and Risk of Esophageal Carcinoma: A Meta-Analysis of Observational Studies. Oncotarget 2017, 8, 99049–99056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, Y.-X.; Zhao, W.; Li, J.; Xie, P.; Wang, S.; Yan, L.; Xing, X.; Lu, J.; Tse, L.-A.; Wang, H.H.-X.; et al. Dietary Intake of Monounsaturated and Polyunsaturated Fatty Acids Is Related to the Reduced Risk of Esophageal Squamous Cell Carcinoma. Lipids Health Dis. 2022, 21, 25. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.S.; Sun, Y.; Yang, Q.U.; Miller, K.W.; Li, G.Y.; Zheng, S.F.; Ershow, A.G.; Blot, W.J.; Li, J.Y. Vitamin A and Other Deficiencies in Linxian, a High Esophageal Cancer Incidence Area in Northern China. J. Natl. Cancer Inst. 1984, 73, 1449–1453. [Google Scholar] [PubMed]
- Li, J.Y.; Taylor, P.R.; Li, B.; Dawsey, S.; Wang, G.Q.; Ershow, A.G.; Guo, W.; Liu, S.F.; Yang, C.S.; Shen, Q. Nutrition Intervention Trials in Linxian, China: Multiple Vitamin/Mineral Supplementation, Cancer Incidence, and Disease-Specific Mortality among Adults with Esophageal Dysplasia. J. Natl. Cancer Inst. 1993, 85, 1492–1498. [Google Scholar] [CrossRef]
- Blot, W.J.; Li, J.Y.; Taylor, P.R.; Guo, W.; Dawsey, S.; Wang, G.Q.; Yang, C.S.; Zheng, S.F.; Gail, M.; Li, G.Y. Nutrition Intervention Trials in Linxian, China: Supplementation with Specific Vitamin/Mineral Combinations, Cancer Incidence, and Disease-Specific Mortality in the General Population. J. Natl. Cancer Inst. 1993, 85, 1483–1492. [Google Scholar] [CrossRef]
- Qiao, Y.-L.; Dawsey, S.M.; Kamangar, F.; Fan, J.-H.; Abnet, C.C.; Sun, X.-D.; Johnson, L.L.; Gail, M.H.; Dong, Z.-W.; Yu, B.; et al. Total and Cancer Mortality after Supplementation with Vitamins and Minerals: Follow-up of the Linxian General Population Nutrition Intervention Trial. J. Natl. Cancer Inst. 2009, 101, 507–518. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.-M.; Taylor, P.R.; Fan, J.-H.; Pfeiffer, R.M.; Gail, M.H.; Liang, H.; Murphy, G.A.; Dawsey, S.M.; Qiao, Y.-L.; Abnet, C.C. Effects of Nutrition Intervention on Total and Cancer Mortality: 25-Year Post-Trial Follow-up of the 5.25-Year Linxian Nutrition Intervention Trial. J. Natl. Cancer Inst. 2018, 110, 1229–1238. [Google Scholar] [CrossRef] [Green Version]
- Myung, S.-K.; Yang, H.J. Efficacy of Vitamin and Antioxidant Supplements in Prevention of Esophageal Cancer: Meta-Analysis of Randomized Controlled Trials. J. Cancer Prev. 2013, 18, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Ray, S.S.; Das, D.; Ghosh, T.; Ghosh, A.K. The Levels of Zinc and Molybdenum in Hair and Food Grain in Areas of High and Low Incidence of Esophageal Cancer: A Comparative Study. Glob. J. Health Sci. 2012, 4, 168–175. [Google Scholar] [CrossRef] [Green Version]
- Hurst, R.; Siyame, E.W.P.; Young, S.D.; Chilimba, A.D.C.; Joy, E.J.M.; Black, C.R.; Ander, E.L.; Watts, M.J.; Chilima, B.; Gondwe, J.; et al. Soil-Type Influences Human Selenium Status and Underlies Widespread Selenium Deficiency Risks in Malawi. Sci. Rep. 2013, 3, 1425. [Google Scholar] [CrossRef] [Green Version]
- Schaafsma, T.; Wakefield, J.; Hanisch, R.; Bray, F.; Schüz, J.; Joy, E.J.M.; Watts, M.J.; McCormack, V. Africa’s Oesophageal Cancer Corridor: Geographic Variations in Incidence Correlate with Certain Micronutrient Deficiencies. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [Green Version]
- Ahsan, A.; Liu, Z.; Su, R.; Liu, C.; Liao, X.; Su, M. Potential Chemotherapeutic Effect of Selenium for Improved Canceration of Esophageal Cancer. Int. J. Mol. Sci. 2022, 23, 5509. [Google Scholar] [CrossRef]
- Sun, Z.-G.; Song, G.-M.; Zhang, M.; Wang, Z. Clinical Study on Zinc, Copper and Manganese Levels in Patients with Esophageal Squamous Cell Cancer. Trace Elem. Electrolytes 2011, 28, 116–120. [Google Scholar] [CrossRef]
- Dar, N.A.; Mir, M.M.; Salam, I.; Malik, M.A.; Gulzar, G.M.; Yatoo, G.N.; Ahmad, A.; Shah, A. Association between Copper Excess, Zinc Deficiency, and TP53 Mutations in Esophageal Squamous Cell Carcinoma from Kashmir Valley, India—A High Risk Area. Nutr. Cancer 2008, 60, 585–591. [Google Scholar] [CrossRef]
- Abnet, C.C.; Lai, B.; Qiao, Y.-L.; Vogt, S.; Luo, X.-M.; Taylor, P.R.; Dong, Z.-W.; Mark, S.D.; Dawsey, S.M. Zinc Concentration in Esophageal Biopsy Specimens Measured by X-Ray Fluorescence and Esophageal Cancer Risk. J. Natl. Cancer Inst. 2005, 97, 301–306. [Google Scholar] [CrossRef]
- Hashemi, S.M.; Mashhadi, M.; Moghaddam, A.A.; Yousefi, J.; Mofrad, A.D.; Sadeghi, M.; Allahyari, A. The Relationship between Serum Selenium and Zinc with Gastroesophageal Cancers in the Southeast of Iran. Indian J. Med. Paediatr. Oncol. 2017, 38, 169–172. [Google Scholar] [CrossRef]
- Hashemian, M.; Murphy, G.; Etemadi, A.; Poustchi, H.; Brockman, J.D.; Kamangar, F.; Pourshams, A.; Khoshnia, M.; Gharavi, A.; Dawsey, S.M.; et al. Toenail Mineral Concentration and Risk of Esophageal Squamous Cell Carcinoma, Results from the Golestan Cohort Study. Cancer Med. 2017, 6, 3052–3059. [Google Scholar] [CrossRef] [Green Version]
- Semnani, S.; Roshandel, G.; Zendehbad, A.; Keshtkar, A.; Rahimzadeh, H.; Abdolahi, N.; Besharat, S.; Moradi, A.; Mirkarimi, H.; Hasheminasab, S. Soils Selenium Level and Esophageal Cancer: An Ecological Study in a High Risk Area for Esophageal Cancer. J. Trace Elem. Med. Biol. 2010, 24, 174–177. [Google Scholar] [CrossRef] [Green Version]
- Keshavarzi, B.; Moore, F.; Najmeddin, A.; Rahmani, F. The Role of Selenium and Selected Trace Elements in the Etiology of Esophageal Cancer in High Risk Golestan Province of Iran. Sci. Total Environ. 2012, 433, 89–97. [Google Scholar] [CrossRef]
- Nouraie, M.; Pourshams, A.; Kamangar, F.; Sotoudeh, M.; Derakhshan, M.H.; Akbari, M.R.; Fakheri, H.; Zahedi, M.J.; Caldwell, K.; Abnet, C.C.; et al. Ecologic Study of Serum Selenium and Upper Gastrointestinal Cancers in Iran. World J. Gastroenterol. 2004, 10, 2544–2546. [Google Scholar] [CrossRef]
- Pritchett, N.R.; Burgert, S.L.; Murphy, G.A.; Brockman, J.D.; White, R.E.; Lando, J.; Chepkwony, R.; Topazian, M.D.; Abnet, C.C.; Dawsey, S.M.; et al. Cross Sectional Study of Serum Selenium Concentration and Esophageal Squamous Dysplasia in Western Kenya. BMC Cancer 2017, 17, 835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, J.; Li, Q.; Fang, X.; Chen, L.; Qiang, Y.; Wang, J.; Wang, Q.; Min, J.; Zhang, S.; Wang, F. Increased Total Iron and Zinc Intake and Lower Heme Iron Intake Reduce the Risk of Esophageal Cancer: A Dose-Response Meta-Analysis. Nutr. Res. 2018, 59, 16–28. [Google Scholar] [CrossRef] [PubMed]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Human Papillomaviruses; IARC: Lyon, France, 2007; Volume 90, ISBN 978-92-832-1290-4. [Google Scholar]
- Rajendra, S.; Pavey, D.; McKay, O.; Merrett, N.; Gautam, S.D. Human Papillomavirus Infection in Esophageal Squamous Cell Carcinoma and Esophageal Adenocarcinoma: A Concise Review. Ann. N. Y. Acad. Sci. 2020, 1482, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Hošnjak, L.; Poljak, M. A Systematic Literature Review of Studies Reporting Human Papillomavirus (HPV) Prevalence in Esophageal Carcinoma over 36 Years (1982–2017). Acta Dermatovenerol. Alp. Pannonica Et Adriat. 2018, 27, 127–136. [Google Scholar] [CrossRef]
- Yao, P.-F.; Li, G.-C.; Li, J.; Xia, H.-S.; Yang, X.-L.; Huang, H.-Y.; Fu, Y.-G.; Wang, R.-Q.; Wang, X.-Y.; Sha, J.-W. Evidence of Human Papilloma Virus Infection and Its Epidemiology in Esophageal Squamous Cell Carcinoma. World J. Gastroenterol. 2006, 12, 1352–1355. [Google Scholar] [CrossRef]
- Zhang, S.-K.; Guo, L.-W.; Chen, Q.; Zhang, M.; Liu, S.-Z.; Quan, P.-L.; Lu, J.-B.; Sun, X.-B. Prevalence of Human Papillomavirus 16 in Esophageal Cancer among the Chinese Population: A Systematic Review and Meta-Analysis. Asian Pac. J. Cancer Prev. 2014, 15, 10143–10149. [Google Scholar] [CrossRef] [Green Version]
- Cheah, P.-L.; Koh, C.-C.; Khang, T.F.; Goh, K.-L.; Lau, P.-C.; Chin, K.-F.; Teoh, K.-H.; Toh, Y.-F.; Looi, L.-M. Esophageal Squamous Cell Carcinomas in a Malaysian Cohort Show a Lack of Association with Human Papillomavirus. J. Dig. Dis. 2018, 19, 272–278. [Google Scholar] [CrossRef]
- Wang, J.; Zhao, L.; Yan, H.; Che, J.; Huihui, L.; Jun, W.; Liu, B.; Cao, B. A Meta-Analysis and Systematic Review on the Association between Human Papillomavirus (Types 16 and 18) Infection and Esophageal Cancer Worldwide. PLoS ONE 2016, 11, e0159140. [Google Scholar] [CrossRef] [Green Version]
- Sitas, F.; Egger, S.; Urban, M.I.; Taylor, P.R.; Abnet, C.C.; Boffetta, P.; O’Connell, D.L.; Whiteman, D.C.; Brennan, P.; Malekzadeh, R.; et al. InterSCOPE Study: Associations between Esophageal Squamous Cell Carcinoma and Human Papillomavirus Serological Markers. J. Natl. Cancer Inst. 2012, 104, 147–158. [Google Scholar] [CrossRef] [Green Version]
- Liyanage, S.S.; Rahman, B.; Ridda, I.; Newall, A.T.; Tabrizi, S.N.; Garland, S.M.; Segelov, E.; Seale, H.; Crowe, P.J.; Moa, A.; et al. The Aetiological Role of Human Papillomavirus in Oesophageal Squamous Cell Carcinoma: A Meta-Analysis. PLoS ONE 2013, 8, e69238. [Google Scholar] [CrossRef] [Green Version]
- Liyanage, S.S.; Rahman, B.; Gao, Z.; Zheng, Y.; Ridda, I.; Moa, A.; Newall, A.T.; Seale, H.; Li, Q.; Liu, J.-F.; et al. Evidence for the Aetiology of Human Papillomavirus in Oesophageal Squamous Cell Carcinoma in the Chinese Population: A Meta-Analysis. BMJ Open 2013, 3, e003604. [Google Scholar] [CrossRef] [Green Version]
- Hussain, S.; Rani, J.; Tulsyan, S.; Sisodiya, S.; Chikara, A.; Nazir, S.; Srivastava, A.; Khan, A.; Dash, N.; Saraya, A.; et al. Influence of HPV Infection in Esophageal Cancer: A Systematic Review and Meta-Analysis. Gene Rep. 2022, 28, 101640. [Google Scholar] [CrossRef]
- Geng, H.; Xing, Y.; Zhang, J.; Cao, K.; Ye, M.; Wang, G.; Liu, C. Association between Viral Infection Other than Human Papillomavirus and Risk of Esophageal Carcinoma: A Comprehensive Meta-Analysis of Epidemiological Studies. Arch. Virol. 2022, 167, 1–20. [Google Scholar] [CrossRef]
- Ponvilawan, B.; Rittiphairoj, T.; Charoenngam, N.; Rujirachun, P.; Wattanachayakul, P.; Tornsatitkul, S.; Ungprasert, P. Association Between Chronic Hepatitis C Virus Infection and Esophageal Cancer: A Systematic Review and Meta-Analysis. J. Clin. Gastroenterol. 2022, 56, 55–63. [Google Scholar] [CrossRef]
- Yuan, T.; Hu, Y.; Zhou, X.; Yang, L.; Wang, H.; Li, L.; Wang, J.; Qian, H.-Z.; Clifford, G.M.; Zou, H. Incidence and Mortality of Non-AIDS-Defining Cancers among People Living with HIV: A Systematic Review and Meta-Analysis. eClinicalMedicine 2022, 52, 101613. [Google Scholar] [CrossRef]
- Thrift, A.P.; Kramer, J.R.; Hartman, C.M.; Royse, K.; Richardson, P.; Dong, Y.; Raychaudhury, S.; Desiderio, R.; Sanchez, D.; Anandasabapathy, S.; et al. Risk and Predictors of Esophageal and Stomach Cancers in HIV-Infected Veterans: A Matched Cohort Study. J. Acquir. Immune Defic. Syndr. 2019, 81, e65–e72. [Google Scholar] [CrossRef]
- Ebule, I.; Longdoh, A.; Paloheimo, I. Helicobacter Pylori Infection and Atrophic Gastritis. Afr. Health Sci. 2013, 13, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Rokkas, T.; Pistiolas, D.; Sechopoulos, P.; Robotis, I.; Margantinis, G. Relationship between Helicobacter Pylori Infection and Esophageal Neoplasia: A Meta-Analysis. Clin. Gastroenterol. Hepatol. 2007, 5, 1413–1417, 1417.e1-2. [Google Scholar] [CrossRef]
- Islami, F.; Kamangar, F. Helicobacter Pylori and Esophageal Cancer Risk—A Meta-Analysis. Cancer Prev. Res. 2008, 1, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Nie, S.; Chen, T.; Yang, X.; Huai, P.; Lu, M. Association of Helicobacter Pylori Infection with Esophageal Adenocarcinoma and Squamous Cell Carcinoma: A Meta-Analysis. Dis. Esophagus 2014, 27, 645–653. [Google Scholar] [CrossRef]
- Xie, F.-J.; Zhang, Y.-P.; Zheng, Q.-Q.; Jin, H.-C.; Wang, F.-L.; Chen, M.; Shao, L.; Zou, D.-H.; Yu, X.-M.; Mao, W.-M. Helicobacter Pylori Infection and Esophageal Cancer Risk: An Updated Meta-Analysis. World J. Gastroenterol. 2013, 19, 6098–6107. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Guo, X.; Wang, C.; Yin, Y.; Xu, G.; Chen, H.; Qi, X. Association of Barrett’s Esophagus with Helicobacter Pylori Infection: A Meta-Analysis. Ther. Adv. Chronic. Dis 2022, 13, 20406223221117972. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.-L.; Duan, R.-Q.; Duan, L.-P. Helicobacter Pylori Infection Is Associated with Reduced Risk of Barrett’s Esophagus: A Meta-Analysis and Systematic Review. BMC Gastroenterol. 2021, 21, 459. [Google Scholar] [CrossRef] [PubMed]
- Erőss, B.; Farkas, N.; Vincze, Á.; Tinusz, B.; Szapáry, L.; Garami, A.; Balaskó, M.; Sarlós, P.; Czopf, L.; Alizadeh, H.; et al. Helicobacter Pylori Infection Reduces the Risk of Barrett’s Esophagus: A Meta-Analysis and Systematic Review. Helicobacter 2018, 23, e12504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semnani, S.; Sadjadi, A.; Fahimi, S.; Nouraie, M.; Naeimi, M.; Kabir, J.; Fakheri, H.; Saadatnia, H.; Ghavamnasiri, M.R.; Malekzadeh, R. Declining Incidence of Esophageal Cancer in the Turkmen Plain, Eastern Part of the Caspian Littoral of Iran: A Retrospective Cancer Surveillance. Cancer Detect. Prev. 2006, 30, 14–19. [Google Scholar] [CrossRef]
- Fan, J.; Liu, Z.; Mao, X.; Tong, X.; Zhang, T.; Suo, C.; Chen, X. Global Trends in the Incidence and Mortality of Esophageal Cancer from 1990 to 2017. Cancer Med. 2020, 9, e03338. [Google Scholar] [CrossRef]
- Yang, S.; Lin, S.; Li, N.; Deng, Y.; Wang, M.; Xiang, D.; Xiang, G.; Wang, S.; Ye, X.; Zheng, Y.; et al. Burden, Trends, and Risk Factors of Esophageal Cancer in China from 1990 to 2017: An up-to-Date Overview and Comparison with Those in Japan and South Korea. J. Hematol. Oncol. 2020, 13, 146. [Google Scholar] [CrossRef]
- Edgren, G.; Adami, H.-O.; Weiderpass, E.; Weiderpass Vainio, E.; Nyrén, O. A Global Assessment of the Oesophageal Adenocarcinoma Epidemic. Gut 2013, 62, 1406–1414. [Google Scholar] [CrossRef]
- Ghasemi-Kebria, F.; Roshandel, G.; Semnani, S.; Shakeri, R.; Khoshnia, M.; Naeimi-Tabiei, M.; Merat, S.; Malekzadeh, R. Marked Increase in the Incidence Rate of Esophageal Adenocarcinoma in a High-Risk Area for Esophageal Cancer. Arch. Iran. Med. 2013, 16, 320–323. [Google Scholar]
- Etemadi, A.; Abnet, C.C.; Golozar, A.; Malekzadeh, R.; Dawsey, S.M. Modeling the Risk of Esophageal Squamous Cell Carcinoma and Squamous Dysplasia in a High Risk Area in Iran. Arch. Iran. Med. 2012, 15, 18–21. [Google Scholar]
- Thrift, A.P.; Kendall, B.J.; Pandeya, N.; Whiteman, D.C. A Model to Determine Absolute Risk for Esophageal Adenocarcinoma. Clin. Gastroenterol. Hepatol. 2013, 11, 138–144.e2. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Sun, D.; Cao, M.; He, S.; Zheng, Y.; Yu, X.; Wu, Z.; Lei, L.; Peng, J.; Li, J.; et al. Risk Prediction Models for Esophageal Cancer: A Systematic Review and Critical Appraisal. Cancer Med. 2021, 10, 7265–7276. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Zheng, R.; Zhou, J.; Li, M.; Shao, D.; Li, X.; Wang, S.; Wei, W. Risk Prediction Model for Esophageal Cancer Among General Population: A Systematic Review. Front. Public Health 2021, 9, 680967. [Google Scholar] [CrossRef] [PubMed]
- Noordzij, I.C.; Curvers, W.L.; Schoon, E.J. Endoscopic Resection for Early Esophageal Carcinoma. J. Thorac. Dis. 2019, 11, S713–S722. [Google Scholar] [CrossRef] [PubMed]
- Vantanasiri, K.; Iyer, P.G. State-of-the-Art Management of Dysplastic Barrett’s Esophagus. Gastroenterol. Rep. 2022, 10, goac068. [Google Scholar] [CrossRef]
- van Munster, S.; Nieuwenhuis, E.; Weusten, B.L.A.M.; Alvarez Herrero, L.; Bogte, A.; Alkhalaf, A.; Schenk, B.E.; Schoon, E.J.; Curvers, W.; Koch, A.D.; et al. Long-Term Outcomes after Endoscopic Treatment for Barrett’s Neoplasia with Radiofrequency Ablation ± Endoscopic Resection: Results from the National Dutch Database in a 10-Year Period. Gut 2022, 71, 265–276. [Google Scholar] [CrossRef]
- Weiss, S.; Pellat, A.; Corre, F.; Abou Ali, E.; Belle, A.; Terris, B.; Leconte, M.; Dohan, A.; Chaussade, S.; Coriat, R.; et al. Predictive Factors of Radiofrequency Ablation Failure in the Treatment of Dysplastic Barrett’s Esophagus. Clin. Res. Hepatol. Gastroenterol. 2022, 47, 102065. [Google Scholar] [CrossRef]
- Wolf, W.A.; Pasricha, S.; Cotton, C.; Li, N.; Triadafilopoulos, G.; Muthusamy, V.R.; Chmielewski, G.W.; Corbett, F.S.; Camara, D.S.; Lightdale, C.J.; et al. Incidence of Esophageal Adenocarcinoma and Causes of Mortality After Radiofrequency Ablation of Barrett’s Esophagus. Gastroenterology 2015, 149, 1752–1761.e1. [Google Scholar] [CrossRef] [Green Version]
- Bartusik-Aebisher, D.; Osuchowski, M.; Adamczyk, M.; Stopa, J.; Cieślar, G.; Kawczyk-Krupka, A.; Aebisher, D. Advancements in Photodynamic Therapy of Esophageal Cancer. Front. Oncol. 2022, 12, 1024576. [Google Scholar] [CrossRef]
- Qumseya, B.J.; David, W.; Wolfsen, H.C. Photodynamic Therapy for Barrett’s Esophagus and Esophageal Carcinoma. Clin. Endosc. 2013, 46, 30–37. [Google Scholar] [CrossRef] [Green Version]
- Ertan, A.; Zaheer, I.; Correa, A.M.; Thosani, N.; Blackmon, S.H. Photodynamic Therapy vs Radiofrequency Ablation for Barrett’s Dysplasia: Efficacy, Safety and Cost-Comparison. World J. Gastroenterol. 2013, 19, 7106–7113. [Google Scholar] [CrossRef]
- Chandan, S.; Bapaye, J.; Khan, S.R.; Deliwala, S.; Mohan, B.P.; Ramai, D.; Dhindsa, B.S.; Goyal, H.; Kassab, L.L.; Aziz, M.; et al. Safety and Efficacy of Liquid Nitrogen Spray Cryotherapy in Barrett’s Neoplasia—A Comprehensive Review and Meta-Analysis. Endosc. Int. Open 2022, 10, E1462–E1473. [Google Scholar] [CrossRef]
- Jankowski, J.A.Z.; de Caestecker, J.; Love, S.B.; Reilly, G.; Watson, P.; Sanders, S.; Ang, Y.; Morris, D.; Bhandari, P.; Brooks, C.; et al. Esomeprazole and Aspirin in Barrett’s Oesophagus (AspECT): A Randomised Factorial Trial. Lancet 2018, 392, 400–408. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, R.C.; Corley, D.A. Will a Proton Pump Inhibitor and an Aspirin Keep the Doctor Away for Patients With Barrett’s Esophagus? Gastroenterology 2019, 156, 1228–1231. [Google Scholar] [CrossRef] [Green Version]
- Tan, W.K.; Sharma, A.N.; Chak, A.; Fitzgerald, R.C. Progress in Screening for Barrett’s Esophagus: Beyond Standard Upper Endoscopy. Gastrointest. Endosc. Clin. N. Am. 2021, 31, 43–58. [Google Scholar] [CrossRef]
- Sawas, T.; Zamani, S.A.; Killcoyne, S.; Dullea, A.; Wang, K.K.; Iyer, P.G.; Fitzgerald, R.C.; Katzka, D.A. Limitations of Heartburn and Other Societies’ Criteria in Barrett’s Screening for Detecting De Novo Esophageal Adenocarcinoma. Clin. Gastroenterol. Hepatol. 2022, 20, 1709–1718. [Google Scholar] [CrossRef]
- Sawas, T.; Killcoyne, S.; Iyer, P.G.; Wang, K.K.; Smyrk, T.C.; Kisiel, J.B.; Qin, Y.; Ahlquist, D.A.; Rustgi, A.K.; Costa, R.J.; et al. Identification of Prognostic Phenotypes of Esophageal Adenocarcinoma in 2 Independent Cohorts. Gastroenterology 2018, 155, 1720–1728.e4. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, R.C.; di Pietro, M.; O’Donovan, M.; Maroni, R.; Muldrew, B.; Debiram-Beecham, I.; Gehrung, M.; Offman, J.; Tripathi, M.; Smith, S.G.; et al. Cytosponge-Trefoil Factor 3 versus Usual Care to Identify Barrett’s Oesophagus in a Primary Care Setting: A Multicentre, Pragmatic, Randomised Controlled Trial. Lancet 2020, 396, 333–344. [Google Scholar] [CrossRef]
- Roshandel, G.; Merat, S.; Sotoudeh, M.; Khoshnia, M.; Poustchi, H.; Lao-Sirieix, P.; Malhotra, S.; O’Donovan, M.; Etemadi, A.; Nickmanesh, A.; et al. Pilot Study of Cytological Testing for Oesophageal Squamous Cell Dysplasia in a High-Risk Area in Northern Iran. Br. J. Cancer 2014, 111, 2235–2241. [Google Scholar] [CrossRef] [Green Version]
- Middleton, D.R.S.; Mmbaga, B.T.; O’Donovan, M.; Abedi-Ardekani, B.; Debiram-Beecham, I.; Nyakunga-Maro, G.; Maro, V.; Bromwich, M.; Daudi, A.; Ngowi, T.; et al. Minimally Invasive Esophageal Sponge Cytology Sampling Is Feasible in a Tanzanian Community Setting. Int. J. Cancer 2021, 148, 1208–1218. [Google Scholar] [CrossRef]
- Mukkamalla, S.K.R.; Recio-Boiles, A.; Babiker, H.M. Esophageal Cancer. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Rubenstein, J.H.; Shaheen, N.J. Epidemiology, Diagnosis, and Management of Esophageal Adenocarcinoma. Gastroenterology 2015, 149, 302–317.e1. [Google Scholar] [CrossRef] [Green Version]
- Thakkar, S.; Kaul, V. Endoscopic Ultrasound Staging of Esophageal Cancer. Gastroenterol. Hepatol. 2020, 16, 14–20. [Google Scholar]
- Tan, C.; Qian, X.; Guan, Z.; Yang, B.; Ge, Y.; Wang, F.; Cai, J. Potential Biomarkers for Esophageal Cancer. Springerplus 2016, 5, 467. [Google Scholar] [CrossRef] [Green Version]
- Chu, L.-Y.; Peng, Y.-H.; Weng, X.-F.; Xie, J.-J.; Xu, Y.-W. Blood-Based Biomarkers for Early Detection of Esophageal Squamous Cell Carcinoma. World J. Gastroenterol. 2020, 26, 1708–1725. [Google Scholar] [CrossRef] [PubMed]
- Ju, C.; He, J.; Wang, C.; Sheng, J.; Jia, J.; Du, D.; Li, H.; Zhou, M.; He, F. Current Advances and Future Perspectives on the Functional Roles and Clinical Implications of Circular RNAs in Esophageal Squamous Cell Carcinoma: More Influential than Expected. Biomark. Res. 2022, 10, 41. [Google Scholar] [CrossRef] [PubMed]
- Nasrollahzadeh, D.; Roshandel, G.; Delhomme, T.M.; Avogbe, P.H.; Foll, M.; Saidi, F.; Poustchi, H.; Sotoudeh, M.; Malekzadeh, R.; Brennan, P.; et al. TP53 Targeted Deep Sequencing of Cell-Free DNA in Esophageal Squamous Cell Carcinoma Using Low-Quality Serum: Concordance with Tumor Mutation. Int. J. Mol. Sci. 2021, 22, 5627. [Google Scholar] [CrossRef]
- Ma, K.; Kalra, A.; Tsai, H.-L.; Okello, S.; Cheng, Y.; Meltzer, S.J.; Lumori, B.A.E.; Opio, C.K.; Jit, S.; Danilova, L.; et al. Accurate Nonendoscopic Detection of Esophageal Squamous Cell Carcinoma Using Methylated DNA Biomarkers. Gastroenterology 2022, 163, 507–509.e2. [Google Scholar] [CrossRef]
- Weidenbaum, C.; Gibson, M.K. Approach to Localized Squamous Cell Cancer of the Esophagus. Curr. Treat. Options Oncol. 2022, 23, 1370–1387. [Google Scholar] [CrossRef]
- Wani, S.; Drahos, J.; Cook, M.B.; Rastogi, A.; Bansal, A.; Yen, R.; Sharma, P.; Das, A. Comparison of Endoscopic Therapies and Surgical Resection in Patients with Early Esophageal Cancer: A Population-Based Study. Gastrointest. Endosc. 2014, 79, 224–232.e1. [Google Scholar] [CrossRef] [Green Version]
- Swanson, J.; Littau, M.; Tonelli, C.; Cohn, T.; Luchette, F.A.; Abdelsattar, Z.; Baker, M.S. A Matched Cohort Comparison of Endoscopic Resection, Chemoradiation and Esophagectomy in the Treatment of Early-Stage Esophageal Squamous Cell Carcinoma. Am. J. Surg. 2022, S0002-9610(22)00782-6. [Google Scholar] [CrossRef]
- Wang, H.; Zeng, X.; Bai, S.; Pu, K.; Zheng, Y.; Ji, R.; Guo, Q.; Guan, Q.; Wang, Y.; Zhou, Y. The safety and Efficacy of Endoscopic Submucosal Dissection for Treating Early Oesophageal Carcinoma: A Meta-Analysis. Annals 2020, 102, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Sun, Y. Efficacy and Safety of Endoscopic Submucosal Dissection versus Endoscopic Mucosal Resection for Superficial Esophageal Carcinoma: A Systematic Review and Meta-Analysis. Dis. Esophagus 2021, 34, doaa081. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, N.; Kelly, R.J. The Management of Localized Esophageal Squamous Cell Carcinoma: Western Approach. Chin. Clin. Oncol. 2017, 6, 46. [Google Scholar] [CrossRef]
- Vellayappan, B.A.; Soon, Y.Y.; Ku, G.Y.; Leong, C.N.; Lu, J.J.; Tey, J.C. Chemoradiotherapy versus Chemoradiotherapy plus Surgery for Esophageal Cancer. Cochrane Database Syst. Rev. 2017, 2017, CD010511. [Google Scholar] [CrossRef] [PubMed]
- Stahl, M.; Stuschke, M.; Lehmann, N.; Meyer, H.-J.; Walz, M.K.; Seeber, S.; Klump, B.; Budach, W.; Teichmann, R.; Schmitt, M.; et al. Chemoradiation with and without Surgery in Patients with Locally Advanced Squamous Cell Carcinoma of the Esophagus. J. Clin. Oncol. 2005, 23, 2310–2317. [Google Scholar] [CrossRef] [Green Version]
- Mann, C.; Berlth, F.; Hadzijusufovic, E.; Lang, H.; Grimminger, P.P. Minimally Invasive Esophagectomy: Clinical Evidence and Surgical Techniques. Langenbecks Arch. Surg. 2020, 405, 1061–1067. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Dinis-Ribeiro, M.; Ponchon, T.; Repici, A.; Vieth, M.; De Ceglie, A.; Amato, A.; Berr, F.; Bhandari, P.; Bialek, A.; et al. Endoscopic Submucosal Dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015, 47, 829–854. [Google Scholar] [CrossRef] [Green Version]
- Ishihara, R.; Goda, K.; Oyama, T. Endoscopic Diagnosis and Treatment of Esophageal Adenocarcinoma: Introduction of Japan Esophageal Society Classification of Barrett’s Esophagus. J. Gastroenterol. 2019, 54, 1–9. [Google Scholar] [CrossRef] [Green Version]
- di Pietro, M.; Canto, M.I.; Fitzgerald, R.C. Clinical Endoscopic Management of Early Adenocarcinoma and Squamous Cell Carcinoma of the Esophagus (Screening, Diagnosis and Therapy). Gastroenterology 2018, 154, 421–436. [Google Scholar] [CrossRef]
- Wang, A.Y.; Hwang, J.H.; Bhatt, A.; Draganov, P.V. AGA Clinical Practice Update on Surveillance After Pathologically Curative Endoscopic Submucosal Dissection of Early Gastrointestinal Neoplasia in the United States: Commentary. Gastroenterology 2021, 161, 2030–2040.e1. [Google Scholar] [CrossRef]
- Zhang, Z.; Ye, J.; Li, H.; Gu, D.; Du, M.; Ai, D.; Chen, W.; Fang, Y.; Xu, X.; Bai, C.; et al. Neoadjuvant Sintilimab and Chemotherapy in Patients with Resectable Esophageal Squamous Cell Carcinoma: A Prospective, Single-Arm, Phase 2 Trial. Front. Immunol. 2022, 13, 1031171. [Google Scholar] [CrossRef]
- Wang, R.; Liu, S.; Chen, B.; Xi, M. Recent Advances in Combination of Immunotherapy and Chemoradiotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma. Cancers 2022, 14, 5168. [Google Scholar] [CrossRef]
- Bolger, J.C.; Donohoe, C.L.; Lowery, M.; Reynolds, J.V. Advances in the Curative Management of Oesophageal Cancer. Br. J. Cancer 2022, 126, 706–717. [Google Scholar] [CrossRef]
- Yang, Y.-M.; Hong, P.; Xu, W.W.; He, Q.-Y.; Li, B. Advances in Targeted Therapy for Esophageal Cancer. Signal Transduct. Target. Ther. 2020, 5, 1–11. [Google Scholar] [CrossRef]
- Hoefnagel, S.J.M.; Boonstra, J.J.; Russchen, M.J.A.M.; Krishnadath, K.K. Towards Personalized Treatment Strategies for Esophageal Adenocarcinoma; A Review on the Molecular Characterization of Esophageal Adenocarcinoma and Current Research Efforts on Individualized Curative Treatment Regimens. Cancers 2021, 13, 4881. [Google Scholar] [CrossRef]
- Secrier, M.; Li, X.; de Silva, N.; Eldridge, M.D.; Contino, G.; Bornschein, J.; MacRae, S.; Grehan, N.; O’Donovan, M.; Miremadi, A.; et al. Mutational Signatures in Esophageal Adenocarcinoma Define Etiologically Distinct Subgroups with Therapeutic Relevance. Nat. Genet. 2016, 48, 1131–1141. [Google Scholar] [CrossRef] [Green Version]
- Harada, K.; Rogers, J.E.; Iwatsuki, M.; Yamashita, K.; Baba, H.; Ajani, J.A. Recent Advances in Treating Oesophageal Cancer. F1000Research 2020, 9, F1000 Faculty Rev-1189. [Google Scholar] [CrossRef]
- Pozzi, V.; Campagna, R.; Sartini, D.; Emanuelli, M. Nicotinamide N-Methyltransferase as Promising Tool for Management of Gastrointestinal Neoplasms. Biomolecules 2022, 12, 1173. [Google Scholar] [CrossRef]
- Xiao, Y.; Tang, J.; Yang, D.; Zhang, B.; Wu, J.; Wu, Z.; Liao, Q.; Wang, H.; Wang, W.; Su, M. Long Noncoding RNA LIPH-4 Promotes Esophageal Squamous Cell Carcinoma Progression by Regulating the MiR-216b/IGF2BP2 Axis. Biomark. Res. 2022, 10, 60. [Google Scholar] [CrossRef]
- van Haren, M.J.; Zhang, Y.; Thijssen, V.; Buijs, N.; Gao, Y.; Mateuszuk, L.; Fedak, F.A.; Kij, A.; Campagna, R.; Sartini, D.; et al. Macrocyclic Peptides as Allosteric Inhibitors of Nicotinamide N-Methyltransferase (NNMT). RSC Chem. Biol. 2021, 2, 1546–1555. [Google Scholar] [CrossRef]
- Gao, Y.; van Haren, M.J.; Buijs, N.; Innocenti, P.; Zhang, Y.; Sartini, D.; Campagna, R.; Emanuelli, M.; Parsons, R.B.; Jespers, W.; et al. Potent Inhibition of Nicotinamide N-Methyltransferase by Alkene-Linked Bisubstrate Mimics Bearing Electron Deficient Aromatics. J. Med. Chem. 2021, 64, 12938–12963. [Google Scholar] [CrossRef] [PubMed]
- Bennett, A.N.; Huang, R.X.; He, Q.; Lee, N.P.; Sung, W.-K.; Chan, K.H.K. Drug Repositioning for Esophageal Squamous Cell Carcinoma. Front. Genet. 2022, 13, 991842. [Google Scholar] [CrossRef] [PubMed]





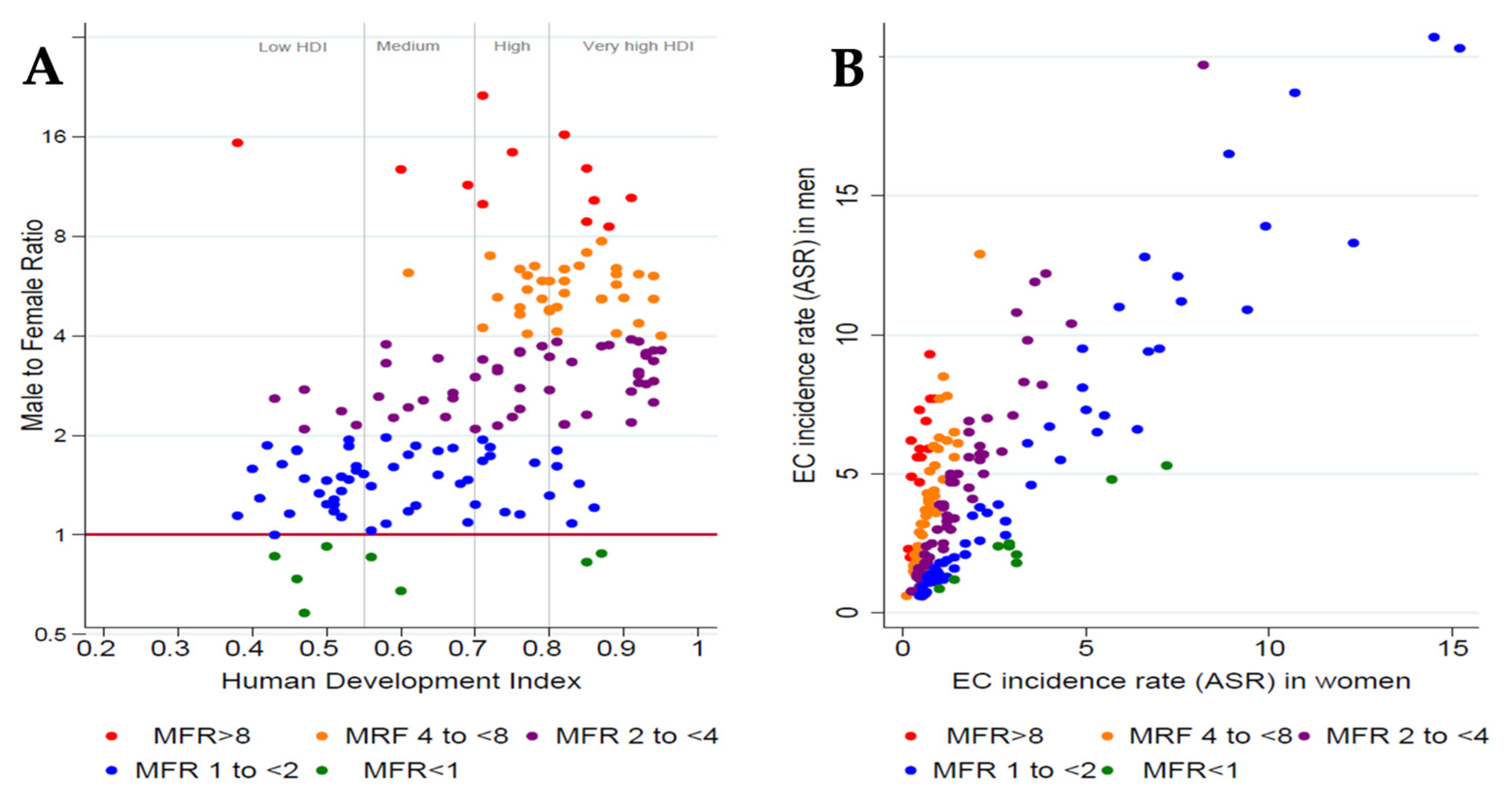{kind=link}
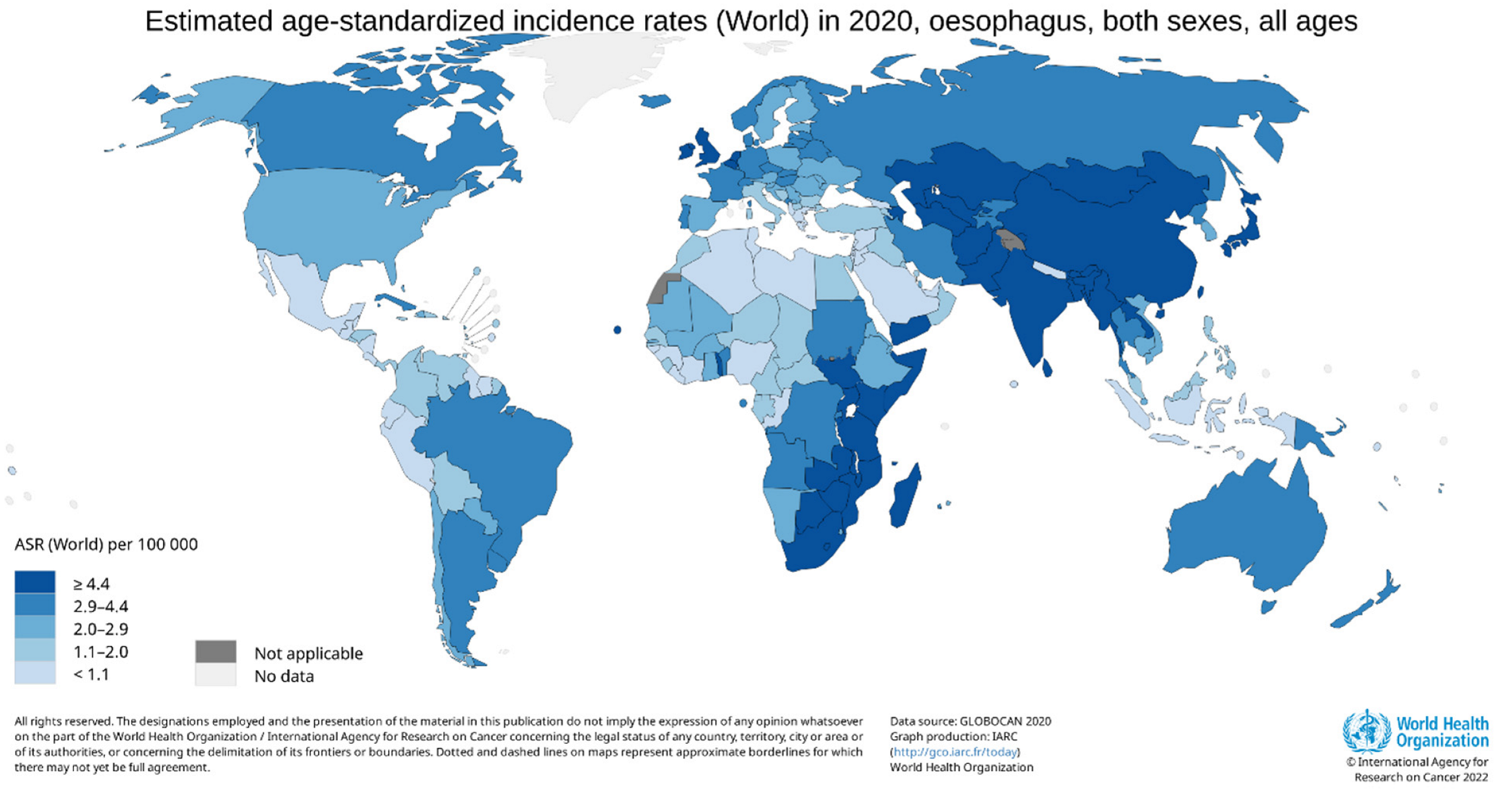{kind=link}
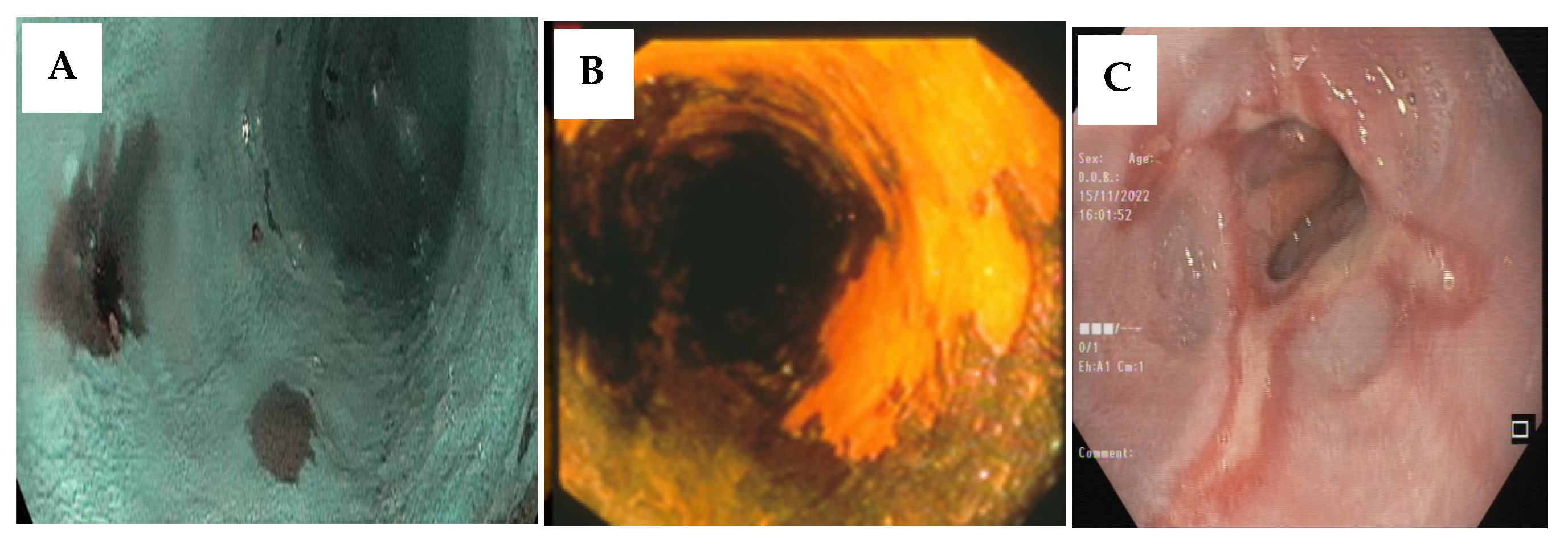{kind=link}
{kind=link}
| Habits | |
|---|---|
| Tobacco |
|
| Alcohol |
|
| Opium |
|
| Hot food and drinks |
|
| Living environment | |
| Socioeconomic status |
|
| Household fuel |
|
| Water source |
|
| Mycotoxin contamination |
|
| Animal contact |
|
| Individual health | |
| Gastroesophageal reflux disease (GERD) |
|
| Body mass index (BMI) |
|
| Gastric atrophy |
|
| Poor oral health and oral hygiene |
|
| Microbiome |
|
| Dietary factors | |
| Whole diet quality |
|
| Intake of specific dietary groups |
|
| Intake of micronutrients |
|
| Infections | |
| Viral infection |
|
| Bacterial infection |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheikh, M.; Roshandel, G.; McCormack, V.; Malekzadeh, R. Current Status and Future Prospects for Esophageal Cancer. Cancers 2023, 15, 765. https://doi.org/10.3390/cancers15030765
Sheikh M, Roshandel G, McCormack V, Malekzadeh R. Current Status and Future Prospects for Esophageal Cancer. Cancers. 2023; 15(3):765. https://doi.org/10.3390/cancers15030765
Chicago/Turabian StyleSheikh, Mahdi, Gholamreza Roshandel, Valerie McCormack, and Reza Malekzadeh. 2023. "Current Status and Future Prospects for Esophageal Cancer" Cancers 15, no. 3: 765. https://doi.org/10.3390/cancers15030765