
A Comparative Multicenter Cohort Study Evaluating the Long-Term Influence of the Strict Lockdown during the First COVID-19 Wave on Lung Cancer Patients (ARTEMISIA Trial)
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Inclusion/Exclusion Criteria and Collected Criteria
2.3. Statistical Methods
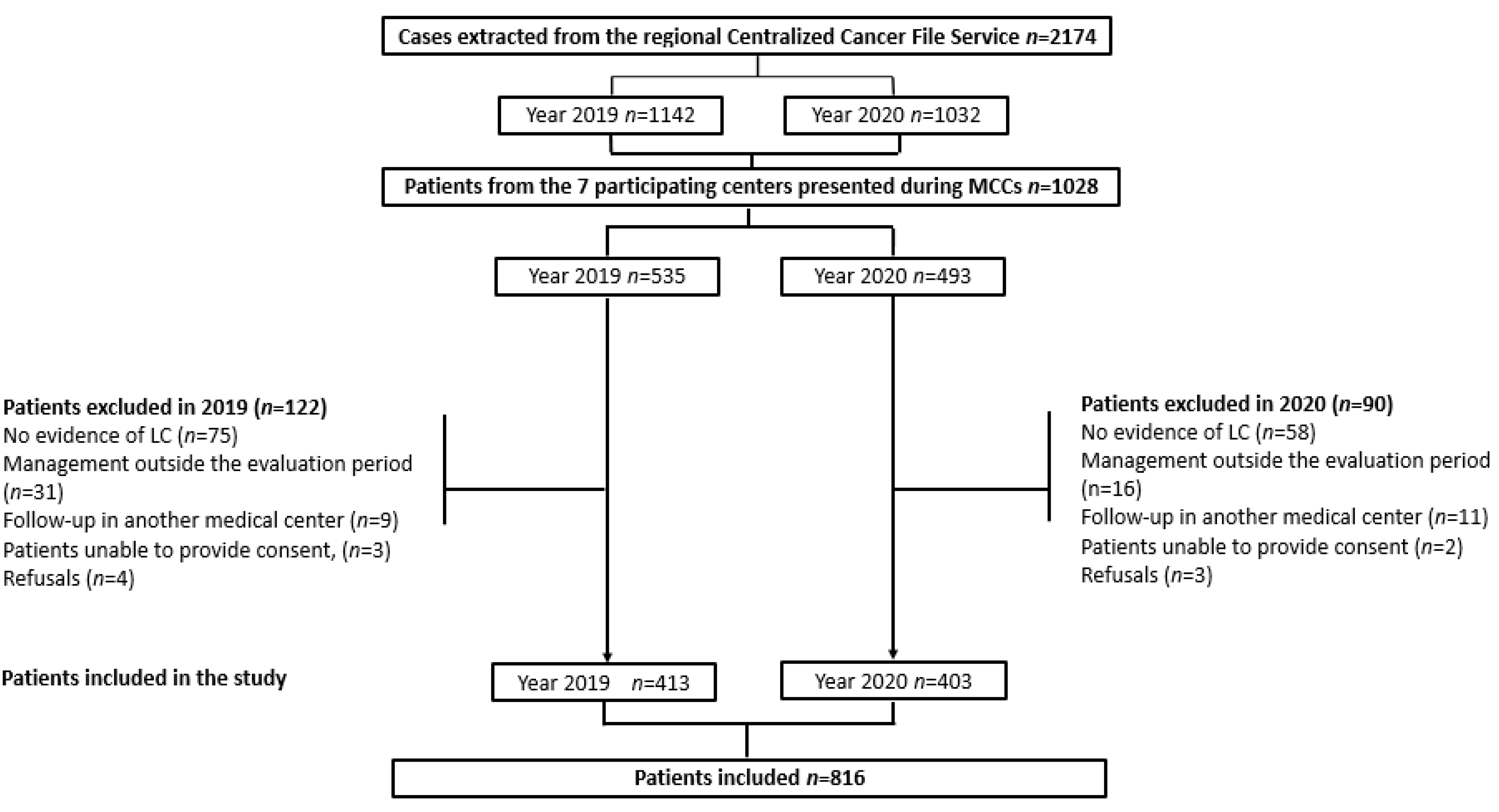
3. Results
3.1. Patient Characteristics
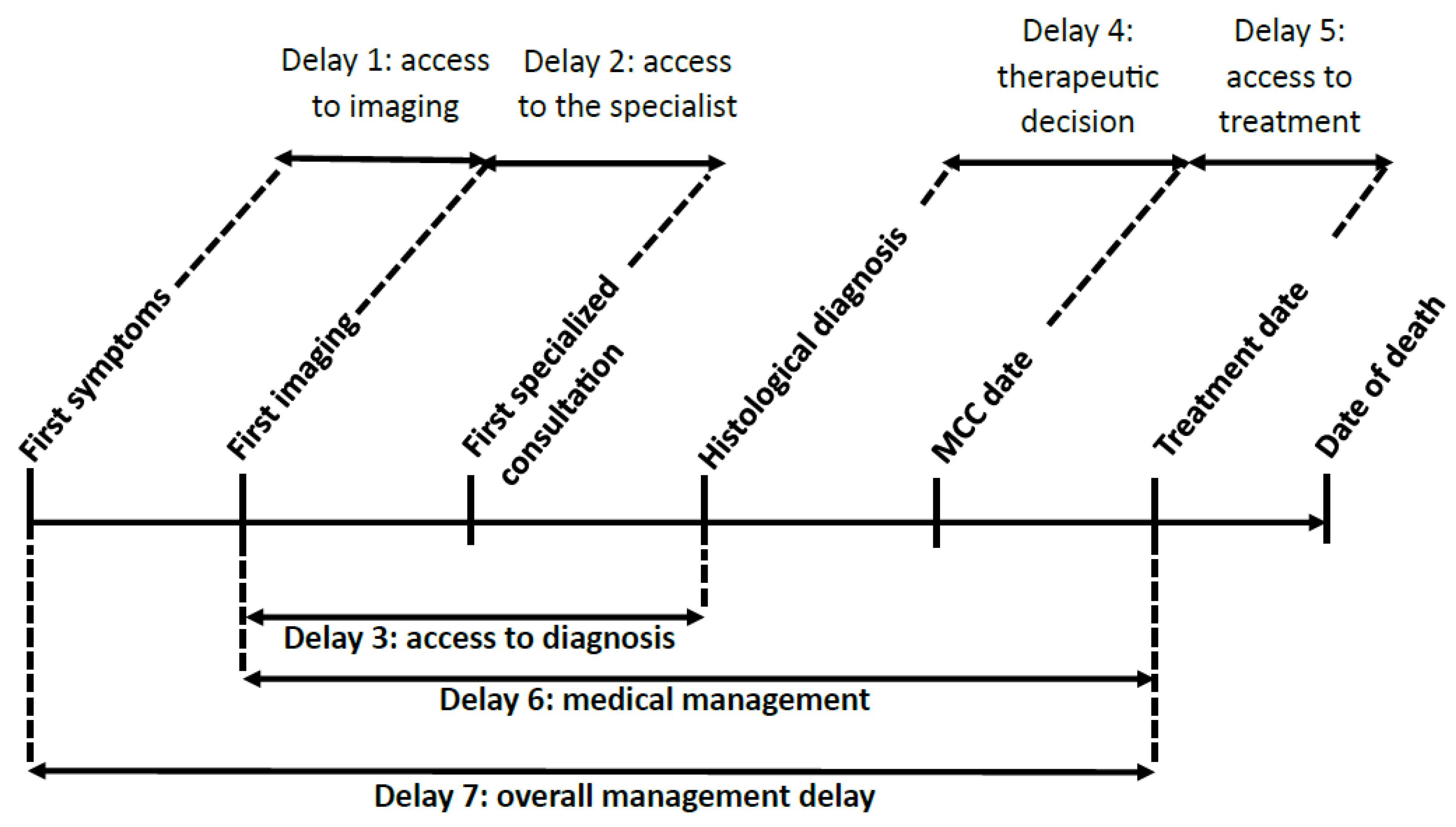
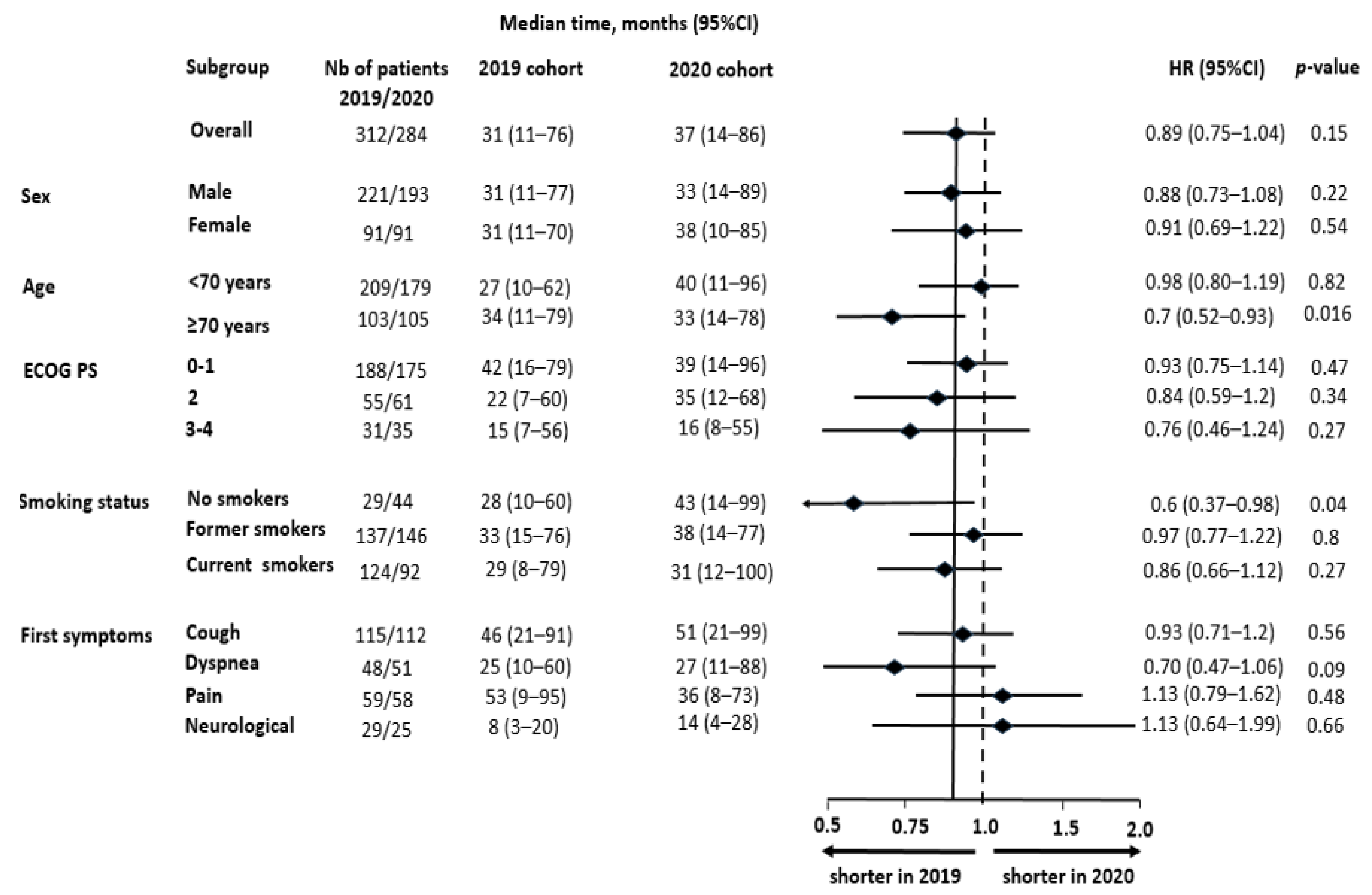
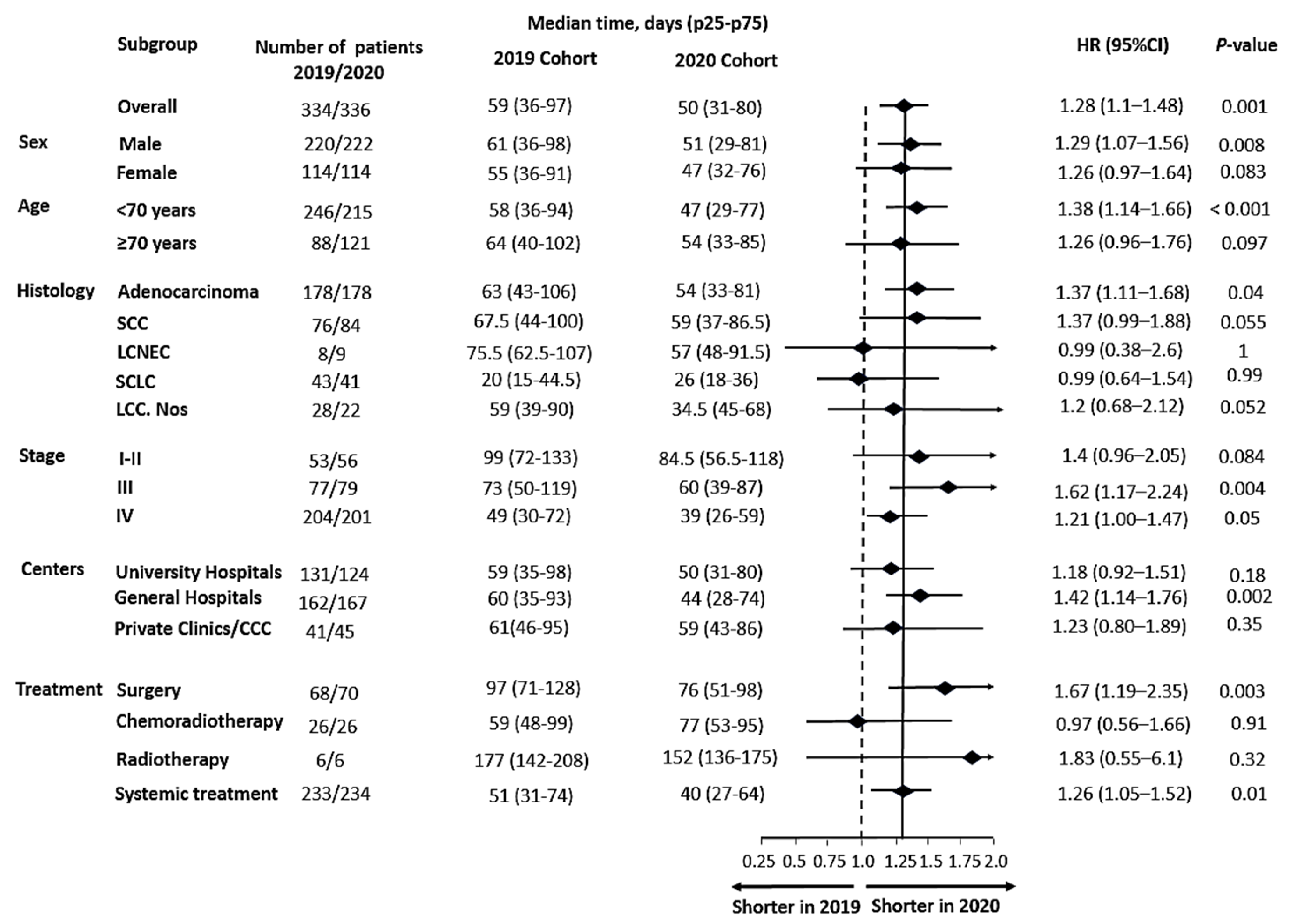
3.2. Delays for Patient Management
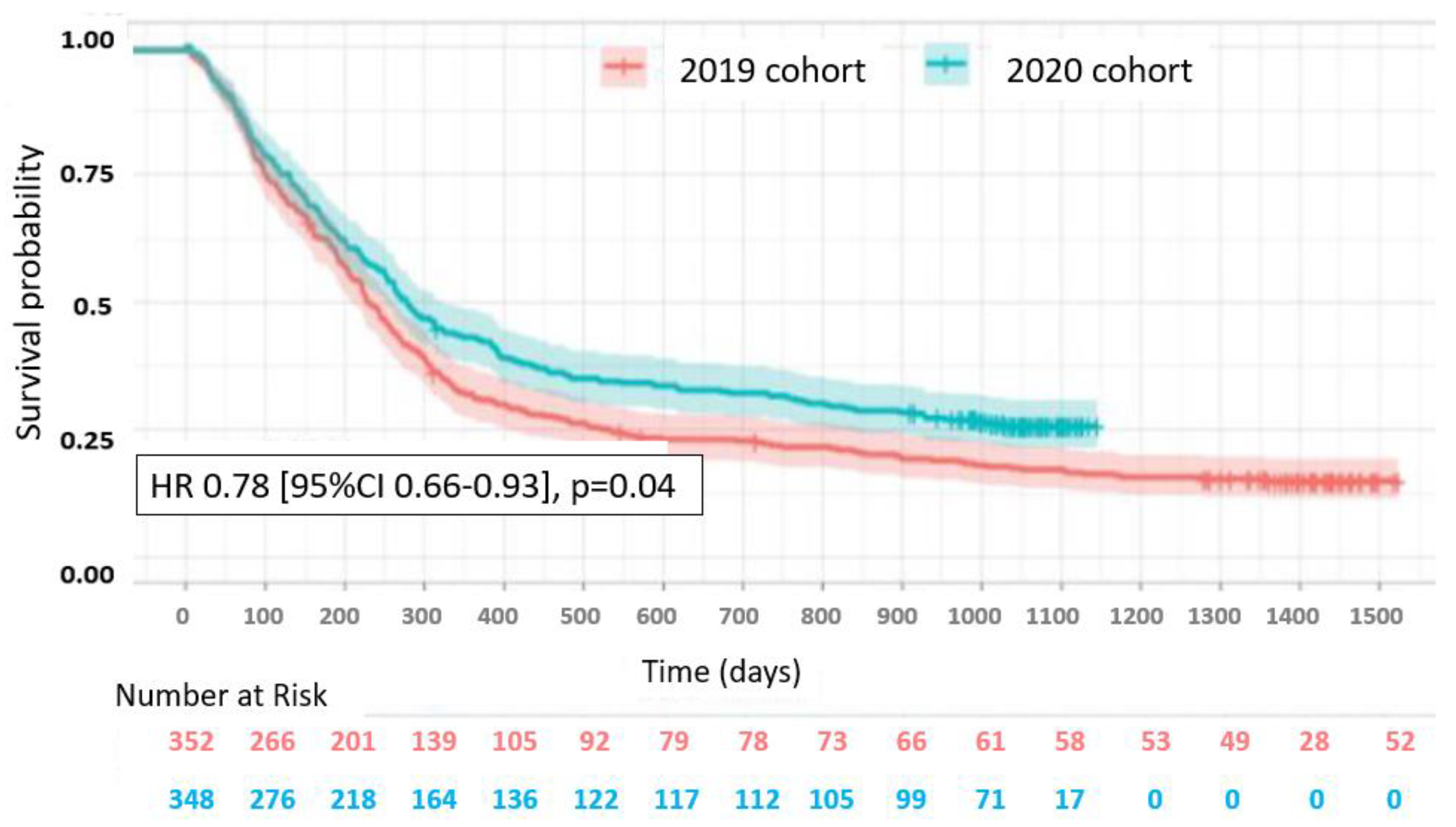
3.3. Survival Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dinmohamed, A.G.; Visser, O.; Verhoeven, R.H.A.; Louwman, M.W.J.; van Nederveen, F.H.; Willems, S.M.; Merkx, M.A.W.; Lemmens, V.E.P.P.; Nagtegaal, I.D.; Siesling, S. Fewer cancer diagnoses during the COVID-19 epidemic in the Netherlands. Lancet Oncol. 2020, 21, 750–751. [Google Scholar] [CrossRef]
- Kempf, E.; Lamé, G.; Layese, R.; Priou, S.; Chatellier, G.; Chaieb, H.; Benderra, M.A.; Bellamine, A.; Bey, R.; Bréant, S.; et al. New cancer cases at the time of SARS-CoV-2 pandemic and related public health policies: A persistent and concerning decrease long after the end of the national lockdown. Eur. J. Cancer. 2021, 150, 260–267. [Google Scholar] [CrossRef]
- Ward, Z.J.; Walbaum, M.; Walbaum, B.; Guzman, M.J.; Jimenez de la Jara, J.; Nervi, B.; Atun, R. Estimating the impact of the COVID-19 pandemic on diagnosis and survival of five cancers in Chile from 2020 to 2030: A simulation-based analysis. Lancet Oncol. 2021, 22, 1427–1437. [Google Scholar] [CrossRef] [PubMed]
- Blay, J.Y.; Boucher, S.; Le Vu, B.; Cropet, C.; Chabaud, S.; Perol, D.; Barranger, E.; Campone, M.; Conroy, T.; Coutant, C.; et al. Delayed care for patients with newly diagnosed cancer due to COVID-19 and estimated impact on cancer mortality in France. ESMO Open 2021, 6, 100134. [Google Scholar] [CrossRef] [PubMed]
- Cigarini, F.; Daolio, J.; Caviola, G.; Pellegri, C.; Cavuto, S.; Guberti, M.; Mazzini, E.; Cerullo, L. Impact of COVID-19 on cancer care pathways in a comprehensive cancer center in northern Italy. Front. Public. Health 2023, 11, 1187912. [Google Scholar] [CrossRef] [PubMed]
- Kuzuu, K.; Misawa, N.; Ashikari, K.; Tamura, S.; Kato, S.; Hosono, K.; Yoneda, M.; Nonaka, T.; Matsushima, S.; Komatsu, T.; et al. Changes in the Number of Gastrointestinal Cancers and Stage at Diagnosis with COVID-19 Pandemic in Japan: A Multicenter Cohort Study. Cancers 2023, 15, 4410. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.P.; Karlsson, U.L.; Lehrman, D.; Mazibuko, T.; Saghatelyan, T.; Thariat, J.; Baumert, B.G.; Vinh-Hung, V.; Gorobets, O.; Giap, H.; et al. Impact of COVID-19 444 pandemic on older cancer patients: Proposed solution by the International Geriatric Radiotherapy Group. Front. Oncol. 2023, 13, 1091329. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, E.; Swanton, C. Consequences of COVID-19 for cancer care—A CRUK perspective. Nat. Rev. Clin. Oncol. 2021, 18, 3–4. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Sud, A.; Jones, M.E.; Broggio, J.; Loveday, C.; Torr, B.; Garrett, A.; Nicol, D.L.; Jhanji, S.; Boyce, S.A.; Gronthoud, F.; et al. Collateral damage: The impact on outcomes from cancer surgery of the COVID-19 pandemic. Ann. Oncol. 2020, 31, 1065–1074. [Google Scholar] [CrossRef]
- Girard, N.; Greillier, L.; Zalcman, G.; Cadranel, J.; Moro-Sibilot, D.; Mazières, J.; Audigier-Valette, C.; Bennouna, J.; Besse, B.; Cortot, A.; et al. Proposals for managing patients with thoracic malignancies during COVID-19 pandemic. Respir. Med. Res. 2020, 78, 100769. [Google Scholar] [CrossRef]
- Basse, C.; Daniel, C.; Livartowski, A.; Beaucaire-Danel, S.; Girard, N. Impact of COVID-19 on the management of patients with thoracic cancers in a tertiary referral center. Lung Cancer 2021, 157, 79–84. [Google Scholar] [CrossRef]
- Singh, A.P.; Berman, A.T.; Marmarelis, M.E.; Haas, A.R.; Feigenberg, S.J.; Braun, J.; Ciunci, C.A.; Bauml, J.M.; Cohen, R.B.; Kucharczuk, J.C.; et al. Management of Lung Cancer During the COVID-19 Pandemic. JCO Oncol. Pract. 2020, 16, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Dingemans, A.C.; Soo, R.A.; Jazieh, A.R.; Rice, S.J.; Kim, Y.T.; Teo, L.L.S.; Warren, G.W.; Xiao, S.Y.; Smit, E.F.; Aerts, J.G.; et al. Treatment Guidance for Patients with Lung Cancer During the Coronavirus 2019 Pandemic. J. Thorac. Oncol. 2020, 15, 1119–1136. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Chmura, S.; Robinson, C.; Lin, S.H.; Gadgeel, S.M.; Donington, J.; Feliciano, J.; Stinchcombe, T.E.; Werner-Wasik, M.; Edelman, M.J.; et al. Alternative Multidisciplinary Management Options for Locally Advanced NSCLC During the Coronavirus Disease 2019 Global Pandemic. J. Thorac. Oncol. 2020, 15, 1137–1146. [Google Scholar] [CrossRef]
- Bakhribah, H.; Zeitouni, M.; Daghistani, R.A.; Almaghraby, H.Q.; Khankan, A.A.; Alkattan, K.M.; Alshehri, S.M.; Jazieh, A.R. Implications of COVID-19 pandemic on lung cancer management: A multidisciplinary perspective. Crit. Rev. Oncol. Hematol. 2020, 156, 103120. [Google Scholar] [CrossRef] [PubMed]
- Liao, Z.; Rivin Del Campo, E.; Salem, A.; Pang, Q.; Liu, H.; Lopez Guerra, J.L. Optimizing lung cancer radiation treatment worldwide in COVID-19 outbreak. Lung Cancer 2020, 146, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, L. The Untold Toll—The Pandemic’s Effects on Patients without COVID-19. N. Engl. J. Med. 2020, 382, 2368–2371. [Google Scholar] [CrossRef]
- Bhalla, S.; Bakouny, Z.; Schmidt, A.L.; Labaki, C.; Steinharter, J.A.; Tremblay, D.A.; Awad, M.M.; Kessler, A.J.; Haddad, R.I.; Evans, M.; et al. Care disruptions among 450 patients with lung cancer: A COVID-19 and cancer outcomes study. Lung Cancer 2021, 160, 78–83. [Google Scholar] [CrossRef]
- Cantini, L.; Mentrasti, G.; Russo, G.; Signorelli, D.; Pasello, G.; Rijavec, E.; Russano, M.; Antonuzzo, L.; Rocco, D.; Giusti, R.; et al. Evaluation of COVID-19 impact on DELAYing diagnostic-therapeutic pathways of lung cancer patients in Italy (COVID-DELAY study): Fewer cases and higher stages from a real-world scenario. ESMO Open 2022, 7, 100406. [Google Scholar] [CrossRef]
- Diaconescu, R.; Lafond, C.; Whittom, R. Treatment delays in non-small cell lung cancer and their prognostic implications. J. Thorac. Oncol. 2011, 6, 1254–1259. [Google Scholar] [CrossRef] [PubMed]
- Vinod, S.K.; Chandra, A.; Berthelsen, A.; Descallar, J. Does timeliness of care in Non-Small Cell Lung Cancer impact on survival? Lung Cancer 2017, 112, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Samson, P.; Patel, A.; Garrett, T.; Crabtree, T.; Kreisel, D.; Krupnick, A.S.; Patterson, G.A.; Broderick, S.; Meyers, B.F.; Puri, V. Effects of Delayed Surgical Resection on Short-Term and Long-Term Outcomes in Clinical Stage I Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2015, 99, 1906–1912. [Google Scholar] [CrossRef] [PubMed]
- Kanarek, N.F.; Hooker, C.M.; Mathieu, L.; Tsai, H.L.; Rudin, C.M.; Herman, J.G.; Brock, M.V. Survival after community diagnosis of early-stage non-small cell lung cancer. Am. J. Med. 2014, 127, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.; Plourde, M.; Guidolin, K.; Fortin, D.; Frechette, E.; Malthaner, R.; Inculet, R. Is it safe to wait? The effect of surgical wait time on survival in patients with non-small cell lung cancer. Can. J. Surg. 2015, 58, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Priou, S.; Lamé, G.; Zalcman, G.; Wislez, M.; Bey, R.; Chatellier, G.; Cadranel, J.; Tannier, X.; Zelek, L.; Daniel, C.; et al. Influence of the SARS-CoV-2 outbreak on management and prognosis of new lung cancer cases, 453 a retrospective multicentre real-life cohort study. Eur. J. Cancer 2022, 173, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Mayne, N.R.; Bajaj, S.S.; Powell, J.; Elser, H.C.; Civiello, B.S.; Fintelmann, F.J.; Li, X.; Yang, C.J. Extended Delay to Treatment for Stage III-IV Non-Small-Cell Lung Cancer and Survival: Balancing Risks During the COVID-19 Pandemic. Clin. Lung Cancer 2022, 23, e362–e376. [Google Scholar] [CrossRef]
- Kasymjanova, G.; Anwar, A.; Cohen, V.; Sultanem, K.; Pepe, C.; Sakr, L.; Friedmann, J.; Agulnik, J.S. The Impact of COVID-19 on the Diagnosis and Treatment of Lung Cancer at a Canadian Academic Center: A Retrospective Chart Review. Curr. Oncol. 2021, 28, 4247–4255. [Google Scholar] [CrossRef]
- Debieuvre, D.; Molinier, O.; Falchero, L.; Locher, C.; Templement-Grangerat, D.; Meyer, N. Lung cancer trends and tumor characteristic changes over 20 years (2000–2020): Results of three French consecutive nationwide prospective cohorts’ studies. Lancet Reg. Health Eur. 2022, 22, 100492. [Google Scholar] [CrossRef]
- Arrieta, O.; Lara-Mejía, L.; Bautista-GonzÁlez, E.; Heredia, D.; Turcott, J.G.; BarrÓn, F.; Ramos-Ramírez, M.; Cabrera-Miranda, L.; Salinas Padilla, M.Á.; Aguerrebere, M.; et al. Clinical Impact of the COVID-19 Pandemic in Mexican Patients with Thoracic Malignancies. Oncologist 2021, 26, 1035–1043. [Google Scholar] [CrossRef]
- Molinier, O.; Falchero, L.; Monnet, I.; Decroisette, C.; Neidhart, A.C.; Redureau, E.; Chiappa, A.M.; Bigot, F.; Bedossa, A.; Amrane, K.; et al. COVID-19 disease among lung cancer (LC) patients: Data from a real-life prospective multicentric study. Ann. Oncol. 2022, 33 (Suppl. 7), S775–S776. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population 2019 n = 413 | Population 2020 n = 403 | ||||||
|---|---|---|---|---|---|---|---|
| Sex | n | 413 | 403 | 0.697 | |||
| Male | n (%) | 285 | (69.0) | 273 | (67.7) | ||
| Female | n (%) | 128 | (31.0) | 130 | (32.3) | ||
| Age | n | 413 | 403 | 0.006 | |||
| Mean age | (sd) | 65.6 ans | (10.5) | 67.6 ans | (10.3) | ||
| Age ≥ or <70 years old | n | 413 | 403 | 0.002 | |||
| ≥70 years | n (%) | 122 | (29.5) | 160 | (39.7) | ||
| <70 years | n (%) | 291 | (70.5) | 243 | (60.3) | ||
| Smoking status | n | 408 | 401 | ||||
| Non-smoker | n (%) | 39 | (9.6) | 64 | (15.9) | 0.006 | |
| Former smoker | n (%) | 201 | (49.3) | 205 | (51.2) | ||
| Active smoker | n (%) | 168 | (41.1) | 132 | (32.9) | ||
| Disease discovery | n | 413 | 403 | ||||
| Symptomatic patients | n (%) | 329 | (79.7) | 328 | (81.4) | 0.533 | |
| Incidental finding | n (%) | 84 | (20.3) | 75 | (18.6) | ||
| Type of center | n | 413 | 403 | 0.923 | |||
| University Hospital | n (%) | 159 | (38.5) | 151 | (37.5) | ||
| General Hospitals | n (%) | 201 | (48.7) | 197 | (48.9) | ||
| Private Clinics or CCC | n (%) | 53 | (12.8) | 55 | (13.6) | ||
| Symptoms | n | 314 | 315 | 0.444 | |||
| Cough | n (%) | 135 | (43.0) | 128 | (40.6) | ||
| Dyspnea | n (%) | 52 | (16.6) | 61 | (19.4) | ||
| Pain | n (%) | 66 | (21.0) | 68 | (21.6) | ||
| Hemoptysis | n (%) | 18 | (5.7) | 10 | (3.2) | ||
| Neurological | n (%) | 30 | (9.6) | 28 | (8.9) | ||
| Others | n (%) | 13 | (4.1) | 20 | (6.3) | ||
| Histology | n | 413 | 403 | 0.688 | |||
| Adenocarcinoma | n (%) | 219 | (53.0) | 216 | (53.6) | ||
| SCC | n (%) | 98 | (23.7) | 99 | (24.6) | ||
| SCLC | n (%) | 50 | (12.1) | 48 | (11.9) | ||
| LCNEC | n (%) | 8 | (1.9) | 12 | (3.0) | ||
| LCC, Nos | n (%) | 38 | (9.2) | 28 | (6.9) | ||
| ECOG | n | 388 | 380 | 0.62 | |||
| 0–1 | n (%) | 275 | (70.8) | 257 | (67.6) | ||
| 2 | n (%) | 72 | (18.6) | 79 | (20.8) | ||
| 3–4 | n (%) | 41 | (10.6) | 44 | (11.6) | ||
| Stage | n | 413 | 403 | 0.782 | |||
| I–II | n (%) | 57 | (13.8) | 59 | (14.6) | ||
| III | n (%) | 86 | (20.8) | 90 | (22.3) | ||
| IV | n (%) | 270 | (65.4) | 254 | (63.0) | ||
| Specialist type | n | 412 | 403 | 0.005 | |||
| Pulmonologist | n (%) | 368 | (89.3) | 351 | (87.1) | ||
| Oncologist/radiotherapist | n (%) | 14 | (3.4) | 6 | (1.5) | ||
| Surgeon | n (%) | 17 | (4.1) | 38 | (10.8) | ||
| Others | n (%) | 13 | (3.5) | 8 | (2.3) | ||
| Diagnostic examination | n | 411 | 382 | 0.951 | |||
| Bronchoscopic Fibroscopy | n (%) | 174 | (42.3) | 157 | (41.1) | ||
| Image-guided biopsy | n (%) | 120 | (29.2) | 125 | (32.7) | ||
| Serous puncture | 23 | (5.6) | 23 | (6.0) | |||
| EBUS | 24 | (5.8) | 26 | (6.8) | |||
| Exploratory surgery | n (%) | 32 | (7.8) | 30 | (7.9) | ||
| Curative surgery | n (%) | 38 | (9.2) | 41 | (10.7) | ||
| Molecular Alterations | n | 413 | 403 | 0.003 | |||
| Absence | 327 | (74) | 328 | (70.3) | |||
| EGFR | n (%) | 32 | (9.8) | 23 | (7.8) | ||
| ALK/ROS1 | n (%) | 4 | (0.9) | 20 | (6.1) | ||
| Others | n (%) | 50 | (15.3) | 52 | (15.8) | ||
| PD-L1 TPS | n | 296 | 282 | 0.638 | |||
| <1% | n (%) | 121 | (40.9) | 122 | (43.3) | ||
| 49–50% | n (%) | 84 | (28.4) | 70 | (24.8) | ||
| ≥50% | n (%) | 91 | (30.7) | 90 | (31.9) | ||
| Treatments | n | 413 | 403 | 0.995 | |||
| Surgery | 71 | (17.2) | 71 | (17.6) | |||
| Curative radiotherapy | 8 | (1.9) | 9 | (2.2) | |||
| Radiochemotherapy | 27 | (6.5) | 27 | (6.7) | |||
| Systemic treatment | 247 | (59.8) | 245 | (60.8) | |||
| Upfront supportive care | 60 | (14.5) | 51 | (12.6) |
| Cohort | Mean Days ± Standard Deviation | Median Days (25th–75th Percentiles) | HR [CI 95%] | p | |
|---|---|---|---|---|---|
| Delay 1: access to imaging | 2019 | 53.8 ± 69.3 | 31 (11–76.2) | 0.89 [0.75–1.04] | 0.15 |
| 2020 | 61.7 ± 80.4 | 37 (14–85.8) | |||
| Delay 2: access to the specialist | 2019 | 16.9 ± 24.5 | 8 (2–21) | 1.18 [1.01–1.38] | 0.048 |
| 2020 | 14.2 ± 28.0 | 6 (1–16) | |||
| Delay 3: access to diagnosis | 2019 | 38.3 ± 37.5 | 25 (11–53) | 1.21 [1.03–1.41] | 0.022 |
| 2020 | 33.2 ± 40.4 | 20 (10–39) | |||
| Delay 4: therapeutic decision | 2019 | 8.7 ± 34.0 | 7 (2–15) | 1.02 [0.89–1.17] | 0.78 |
| 2020 | 7.7 ± 28.2 | 7 (2–14) | |||
| Delay 5: access to treatment | 2019 | 23.5 ± 35.6 | 17 (7–33) | 1.27 [1.09–1.47] | 0.002 |
| 2020 | 18.8 ± 18.1 | 14 (6–27) | |||
| Delay 6: medical management | 2019 | 72.0 ± 52.2 | 59.5 (36–97) | 1.28 [1.1–1.49] | 0.001 |
| 2020 | 60.3 ± 41 | 50 (30.8–80) | |||
| Delay 7: overall management delay | 2019 | 120 ± 84.3 | 100 (67.5–154) | 1.00 [0.84–119] | 0.97 |
| 2020 | 119 ± 96.5 | 97 (56.2–158) |
| Characteristics | HR | 95% CI | p-Value |
|---|---|---|---|
| Age ≥ 70 vs. <70 | 1.29 | 1.06–1.57 | 0.01 |
| Female vs. male | 0.64 | 0.52–0.78 | <0.001 |
| Smoking status | |||
| Non-smoker | - | ||
| Current smoker | 1.73 | 1.23–2.45 | 0.002 |
| Former smoker | 1.74 | 1.26–2.41 | 0.001 |
| Stage | |||
| I–II | - | ||
| III | 3.73 | 2.28–6.1 | <0.001 |
| IV | 7.75 | 4.85–12.39 | <0.001 |
| PS | |||
| 0–1 | - | ||
| 2 | 2.3 | 1.84–2.84 | <0.001 |
| 3–4 | 4.49 | 3.45–5.85 | <0.001 |
| 2020 vs. 2019 | 0.71 | 0.59–0.84 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molinier, O.; Guguen, C.; Marcq, M.; Chene, A.-L.; Masson, P.; Bigot, F.; Denis, F.; Empereur, F.; Saulnier, P.; Urban, T. A Comparative Multicenter Cohort Study Evaluating the Long-Term Influence of the Strict Lockdown during the First COVID-19 Wave on Lung Cancer Patients (ARTEMISIA Trial). Cancers 2023, 15, 5729. https://doi.org/10.3390/cancers15245729
Molinier O, Guguen C, Marcq M, Chene A-L, Masson P, Bigot F, Denis F, Empereur F, Saulnier P, Urban T. A Comparative Multicenter Cohort Study Evaluating the Long-Term Influence of the Strict Lockdown during the First COVID-19 Wave on Lung Cancer Patients (ARTEMISIA Trial). Cancers. 2023; 15(24):5729. https://doi.org/10.3390/cancers15245729
Chicago/Turabian StyleMolinier, Olivier, Camille Guguen, Marie Marcq, Anne-Laure Chene, Philippe Masson, Frédéric Bigot, Fabrice Denis, Fabienne Empereur, Philippe Saulnier, and Thierry Urban. 2023. "A Comparative Multicenter Cohort Study Evaluating the Long-Term Influence of the Strict Lockdown during the First COVID-19 Wave on Lung Cancer Patients (ARTEMISIA Trial)" Cancers 15, no. 24: 5729. https://doi.org/10.3390/cancers15245729