
Lung Carcinoids: A Comprehensive Review for Clinicians

Abstract
:Simple Summary
Abstract
1. Introduction
2. Epidemiology and Etiology
3. Clinical Presentation
4. Diagnosis
4.1. Macroscopic Pathology
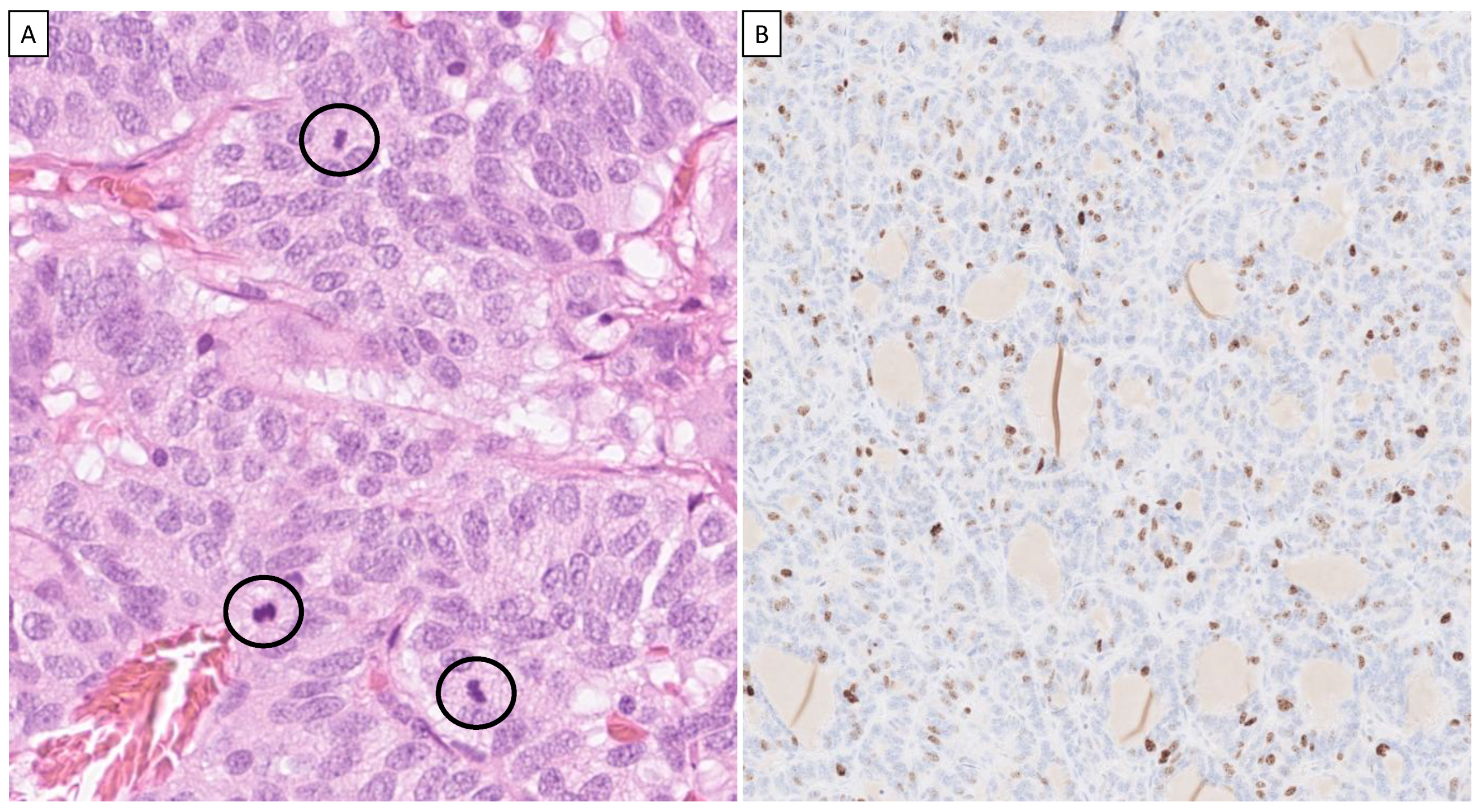
4.2. Histopathology
4.3. Diffuse Idiopathic Neuroendocrine Cell Hyperplasia (DIPNECH) and Carcinoid Tumorlets
4.4. Immunohistochemistry
4.5. Genetic Alterations
4.6. Radiology
4.7. Staging
4.8. Differential Diagnoses
5. Treatment
5.1. Surgery
5.2. Interventional Pulmonology
5.3. Radiotherapy
5.4. Somatostatin Analogues
5.5. Chemotherapy
5.6. Targeted Therapies
5.7. mTOR Inhibitors
5.8. Anti-Angiogenic Drugs
5.9. Immune Therapy
5.10. Local Treatment
5.11. Adjuvant Treatment
5.12. Symptomatic Treatment
5.13. Treatment of DIPNECH
6. Prognosis
7. Follow-Up
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Frölich, F. Die “Helle Zelle” der Bronchialschleimhaut und ihre Beziehungen zum Problem der Chemoreceptoren. Frankf. Z. Pathol. 1949, 60, 517–559. [Google Scholar]
- Feyrter, F. Über die Argyrophilie des Helle-Zelle-Systems in Bronchialbaum des Menschen. Z. Mikrosk. Anat. Forsch. 1954, 61, 73–81. [Google Scholar]
- Gould, V.E.; Linnoila, R.I.; Memoli, V.A.; Warren, W.H. Neuroendocrine Components of the Bronchopulmonary Tract: Hyperplasias, Dysplasias, and Neoplasms. Lab. Investig. 1983, 49, 519–537. [Google Scholar]
- Lauweryns, J.M.; Peuskens, J.C. Neuro-epithelial Bodies (Neuroreceptor or Secretory Organs?) in Human Infant Bronchial and Bronchiolar Epithelium. Anat. Rec. 1972, 172, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Bensch, K.G.; Corrin, B.; Pariente, R.; Spencer, H. Oat-Cell Carcinoma of the Lung. Its Origin and Relationship to Bronchial Carcinoid. Cancer 1968, 22, 1163–1172. [Google Scholar] [CrossRef] [PubMed]
- Bensch, K.G.; Gordon, G.B.; Miller, L.R. Electron Microscopic and Biochemical Studies on the Bronchial Carcinoid Tumor. Cancer 1965, 18, 592–602. [Google Scholar] [CrossRef]
- Gould, V.E.; Linnoila, R.I. Pulmonary neuroepithelial bodies, neuroendocrine cells, and pulmonary tumors. Hum. Pathol. 1982, 13, 1064–1066. [Google Scholar] [CrossRef] [PubMed]
- McDowell, E.M.; Barrett, L.A.; Trump, B.F. Observations on Small Granule Cells in Adult Human Bronchial Epithelium and in Carcinoid and Oat Cell Tumors. Lab. Investig. 1976, 34, 202–206. [Google Scholar]
- Arrigoni, M.G.; Woolner, L.B.; Bernatz, P.E. Atypical carcinoid tumors of the lung. J. Thorac. Cardiovasc. Surg. 1972, 64, 413–421. [Google Scholar] [CrossRef]
- Modlin, I.M.; Lye, K.D.; Kidd, M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer 2003, 97, 934–959. [Google Scholar] [CrossRef]
- Hallet, J.; Law CH, L.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the rising incidence of neuroendocrine tumors: A population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients with Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Fink, G.; Krelbaum, T.; Yellin, A.; Bendayan, D.; Saute, M.; Glazer, M.; Kramer, M.R. Pulmonary carcinoid: Presentation, diagnosis, and outcome in 142 cases in Israel and review of 640 cases from the literature. Chest 2001, 119, 1647–1651. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Christopher, D.J.; Balamugesh, T.; Shah, A. Clinico-pathologic study of pulmonary carcinoid tumours—A retrospective analysis and review of literature. Respir. Med. 2008, 102, 1611–1614. [Google Scholar] [CrossRef]
- Thompson, R.; Landry, C.S. Multiple endocrine neoplasia 1: A broad overview. Ther. Adv. Chronic. Dis. 2021, 12, 20406223211035288. [Google Scholar] [CrossRef] [PubMed]
- Wahbah, M.; Boroumand, N.; Castro, C.; El-Zeky, F.; Eltorky, M. Changing trends in the distribution of the histologic types of lung cancer: A review of 4439 cases. Ann. Diagn. Pathol. 2007, 11, 89–96. [Google Scholar] [CrossRef]
- Bertelsen, S.; Aasted, A.; Lund, C.; Badsberg, E.; Christoffersen, I.; Jacobsen, M.; Jensen, B.S.; Ludwigsen, E.; Paulsen, P.; Paulsen, M.; et al. Bronchial Carcinoid Tumors—A Clinicopathologic Study of 82 Cases. Scand. J. Thor. Cardiovasc. Surg. 1985, 19, 105–111. [Google Scholar]
- Harpole, D.H.; Feldman, J.M.; Buchanan, S.; Young, W.; Wolfe, W.G. Bronchial Carcinoid Tumors: A Retrospective Analysis of 126 Patients. Ann. Thorac. Surg. 1992, 54, 50–55. [Google Scholar] [CrossRef]
- McCaughan, B.C.; Martini, N.; Bains, M.S. Bronchial carcinoids—Review of 124 cases. J. Thorac. Cardiovasc. Surg. 1985, 89, 8–17. [Google Scholar] [CrossRef]
- Mårtensson, H.; Böttcher, G.; Hambraeus, G.; Sundler, F.; Willen, H.; Nobin, A. Bronchial Carcinoids: An Analysis of 91 Cases. World J. Surg. 1987, 11, 356–364. [Google Scholar] [CrossRef]
- Davila, D.G.; Dunn, W.F.; Tazelaar, H.D.; Pairolero, P.C. Bronchial Carcinoid Tumors. Mayo Clin. Proc. 1993, 68, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Dusmet, M.E.; McKneally, M.F. Pulmonary and Thymic Carcinoid Tumors. World J. Surg. 1996, 20, 189–195. [Google Scholar] [CrossRef]
- Ricci, C.; Patrassi, N.; Massa, R.; Mineo, C.; Benedetti-Valentini, F. Carcinoid Syndrome in Bronchial Adenoma. Am. J. Surg. 1973, 126, 671–677. [Google Scholar] [CrossRef]
- Soga, J.; Yakuwa, Y. Bronchopulmonary Carcinoids: An Analysis of 1,875 Reported Cases with Special Reference to a Comparison between Typical Carcinoids and Atypical Varieties. Ann. Thorac. Cardiovasc. Surg. 1999, 5, 211–219. [Google Scholar]
- Ezzat, S.; Asa, S.L.; Stefaneanu, L.; Whittom, R.; Smyth, H.S.; Horvath, E.; Kovacs, K.; A Frohman, L. Somatotroph Hyperplasia without Pituitary Adenoma Associated with a Long Standing Growth Hormone-Releasing Hormone-Producing Bronchial Carcinoid. J. Clin. Endocrinol. Metab. 1994, 78, 555–560. [Google Scholar] [PubMed]
- Huber, R.M.; Schopohl, J.; Losa, M.; Wolfram, G.; Thetter, O.; Permanetter, W.; Werder, K.V. Growth-Hormone Releasing Hormone in a Bronchial Carcinoid. Cancer 1991, 67, 2538–2542. [Google Scholar] [CrossRef] [PubMed]
- Colby, T.V. Carcinoid and Other Neuroendocrine Tumors. In Tumors of the Lower Respiratory Tract; Armed Forces Instute of Pathology: Bethesda, MD, USA, 1994; pp. 287–317. [Google Scholar]
- Okike, N.; Bernatz, P.E.; Woolner, L.B. Carcinoid Tumors of the Lung. Ann. Thorac. Surg. 1976, 22, 270–277. [Google Scholar] [CrossRef]
- Bełz, A.; Rosiek, V.; Szeląg, J.G.; Stęplewska, K.; Kos-Kudła, B. Lung Nodule 25 Years after Lobectomy—Recurrence of Bronchial Carcinoid. Wiad. Lek. 2020, 73, 2309–2312. [Google Scholar] [CrossRef]
- Granberg, D.; Öberg, K. Lung and Thymic Neuroendocrine Tumors. In Clinical Endocrine Oncology, 2nd ed.; Hay, I.D., Wass, J.A.H., Eds.; Blackwell Publishing Ltd.: Oxford, UK, 2008; pp. 452–487. [Google Scholar]
- Mortensen, R. Overview of gene targeting by homologous recombination. In Current Protocols in Molecular Biology; Wiley: New York, NY, USA, 1993; pp. 9.15.1–9.15.6. [Google Scholar]
- Travis, W.D.; Colby, T.V.; Corrin, B.; Shimosato, Y.; Brambilla, E. World Health Organization. Histological Typing of Lung and Pleural Tumours, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 1999. [Google Scholar]
- Travis, W.D.; Rush, W.; Flieder, D.B.; Falk, R.; Fleming, M.V.; Gal, A.A.; Koss, M.N. Survival Analysis of 200 Pulmonary Neuroendocrine Tumors with Clarification of Criteria for Atypical Carcinoid and Its Separation From Typical Carcinoid. Am. J. Surg. Pathol. 1998, 22, 934–944. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Müller-Hermelink, H.K.; Harris, C.C. (Eds.) World Health Organization Classification of Tumours. Pathology & Genetics. Tumours of the Lung, Pleura, Thymus and Heart; IARCPress: Lyon, Paris, 2004. [Google Scholar]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Warren, W.H.; Memoli, V.A.; Gould, V.E. Immunohistochemical and Ultrastructural Analysis of Bronchopulmonary Neuroendocrine Neoplasms. I. Carcinoids. Ultrastruct. Pathol. 1984, 6, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Barbareschi, M.; Frigo, B.; Mosca, L.; Carboni, N.; Arrigoni, G.; Leonardi, E.; Wilander, E.; Siegal, G.; Shiro, B. Bronchial Carcinoids with S-100 Positive Sustentacular Cells. A Comparative Study with Gastrointestinal Carcinoids, Pheochromocytomas and Paragangliomas. Path. Res. Pr. 1990, 186, 212–222. [Google Scholar] [CrossRef] [PubMed]
- El-Salhy, M.; Lundqvist, M.; Wilander, E. Bronchial Carcinoids and Pheochromocytomas—A Comparative Study with Special Emphasis on S-100 Protein, Serotonin and Neuron-Specific Enolase (NSE) Immunoreactivity. Acta Path. Microbiol. Immunol. Scand. Sect. A 1986, 94, 229–235. [Google Scholar]
- Granberg, D.; Wilander, E.; Öberg, K.; Skogseid, B. Decreased Survival in Patients with CD44-negative Typical Bronchial Carcinoid Tumors. Int. J. Cancer 1999, 84, 484–488. [Google Scholar] [CrossRef]
- Barbareschi, M.; Girlando, S.; Mauri, F.A.; Arrigoni, G.; Laurino, L.; Palma, P.D.; Doglioni, C. Tumour suppressor gene products, proliferation, and differentiation markers in lung neuroendocrine neoplasms. J. Pathol. 1992, 166, 343–350. [Google Scholar] [CrossRef]
- Gouyer, V.; Gazzéri, S.; Bolon, I.; Drevet, C.; Brambilla, C.; Brambilla, E. Mechanism of Retinoblastoma Gene Inactivation in the Spectrum of Neuroendocrine Lung Tumors. Am. J. Respir. Cell Mol. Biol. 1998, 18, 188–196. [Google Scholar] [CrossRef]
- Coppola, D.; Clarke, M.; Landreneau, R.; Weyant, R.; Cooper, D.; A Yousem, S. Bcl-2, p53, CD44, and CD44v6 isoform expression in neuroendocrine tumors of the lung. Mod. Pathol. 1996, 9, 484–490. [Google Scholar]
- Lohmann, D.; Pütz, B.; Reich, U.; Böhm, J.; Präuer, H.; Höfler, H. Mutational Spectrum of the p53 Gene in Human Small-Cell Lung Cancer and Relationship to Clinicopathological Data. Am. J. Pathol. 1993, 142, 907–915. [Google Scholar]
- Swarts, D.R.; Rudelius, M.; Claessen, S.M.H.; Cleutjens, J.P.; Seidl, S.; Volante, M.; Ramaekers, F.C.S.; Speel, E.J.M. Limited additive value of the Ki-67 proliferative index on patient survival in World Health Organization-classified pulmonary carcinoids. Histopathology 2017, 70, 412–422. [Google Scholar] [CrossRef]
- Cai, Y.-C.; Banner, B.; Glickman, J.; Odze, R.D. Cytokeratin 7 and 20 and thyroid transcription factor 1 can help distinguish pulmonary from gastrointestinal carcinoid and pancreatic endocrine tumors. Hum. Pathol. 2001, 32, 1087–1093. [Google Scholar] [CrossRef]
- Du, E.Z.; Goldstraw, P.; Zacharias, J.; Tiffet, O.; Craig, P.J.; Nicholson, A.G.; Weidner, N.; Yi, E.S. TTF-1 expression is specific for lung primary in typical and atypical carcinoids: TTF-1-positive carcinoids are predominantly in peripheral location. Hum. Pathol. 2004, 35, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Chejfec, G.; Lee, I.; Warren, W.H.; Gould, V.E. Bombesin in Human Neuroendocrine (NE) Neoplasms. Peptides 1985, 6, 107–112. [Google Scholar] [CrossRef]
- Walch, A.K.; Zitzelsberger, H.F.; Aubele, M.M.; Mattis, A.E.; Bauchinger, M.; Candidus, S.; Präuer, H.W.; Werner, M.; Höfler, H. Typical and Atypical Carcinoid Tumors of the Lung Are Characterized by 11q Deletions as Detected by Comparative Genomic Hybridization. Am. J. Pathol. 1998, 153, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Debelenko, L.V.; Brambilla, E.; Agarwal, S.K.; Swalwell, J.I.; Kester, M.B.; Lubensky, I.A.; Zhuang, Z.; Guru, S.C.; Manickam, P.; Olufemi, S.-E.; et al. Identification of MEN1 gene mutations in sporadic carcinoid tumors of the lung. Hum. Mol. Genet. 1997, 6, 2285–2290. [Google Scholar] [CrossRef] [PubMed]
- El-Naggar, A.K.; Ballance, W.; Karim, F.W.A.; Ordóñez, N.G.; McLemore, D.; Giacco, G.G.; Batsakis, J.G. Typical and Atypical Bronchopulmonary Carcinoids—A Clinicopathologic and Flow Cytometric Study. Am. J. Clin. Pathol. 1991, 95, 828–834. [Google Scholar] [CrossRef]
- Jones, D.J.; Hasleton, P.S.; Moore, N. DNA ploidy in bronchopulmonary carcinoid tumours. Thorax 1988, 43, 195–199. [Google Scholar] [CrossRef]
- Thunnissen, F.B.; Van Eijk, J.; Baak, J.P.; Schipper, N.W.; Uyterlinde, A.M.; Breederveld, R.S.; Meijer, S. Bronchopulmonary Carcinoids and Regional Lymph Node Metastases—A Quantitative Pathologic Investigation. Am. J. Pathol. 1988, 132, 119–122. [Google Scholar]
- Travis, W.D.; Linnoila, R.I.; Tsokos, M.G.; Hitchcock, C.L.; Cutler, G.B.; Nieman, L.; Chrousos, G.; Pass, H.; Doppman, J. Neuroendocrine Tumors of the Lung with Proposed Criteria for Large-Cell Neuroendocrine Carcinoma. An Ultrastructural, Immunohistochemical, and Flow Cytometric Study of 35 Cases. Am. J. Surg. Patol. 1991, 15, 529–553. [Google Scholar] [CrossRef]
- Metovic, J.; Barella, M.; Bianchi, F.; Hofman, P.; Hofman, V.; Remmelink, M.; Kern, I.; Carvalho, L.; Pattini, L.; Sonzogni, A.; et al. Morphologic and molecular classification of lung neuroendocrine neoplasms. Virchows Arch. 2021, 478, 5–19. [Google Scholar] [CrossRef]
- Stefani, A.; Morandi, U.; Urgese, A.L.; Rivasi, F.; Lodi, R. Carcinoid tumors of the lung. An analysis of 65 operated cases. J. Cardiovasc. Surg. 1999, 40, 607–612. [Google Scholar]
- Jeung, M.-Y.; Gasser, B.; Gangi, A.; Charneau, D.; Ducroq, X.; Kessler, R.; Quoix, E.; Roy, C. Bronchial carcinoid tumors of the thorax: Spectrum of radiologic findings. Radiographics 2002, 22, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Meisinger, Q.C.; Klein, J.S.; Butnor, K.J.; Gentchos, G.; Leavitt, B.J. CT features of peripheral pulmonary carcinoid tumors. AJR Am. J. Roentgenol. 2011, 197, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Schrevens, L.; Vansteenkiste, J.; Deneffe, G.; De Leyn, P.; Verbeken, E.; Vandenberghe, T.; Demedts, M. Clinical-radiological presentation and outcome of surgically treated pulmonary carcinoid tumours: A long-term single institution experience. Lung Cancer 2004, 43, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Granberg, D.; Sundin, A.; Janson, E.T.; Öberg, K.; Skogseid, B.; Westlin, J. Octreoscan in patients with bronchial carcinoid tumours. Clin. Endocrinol. 2003, 59, 793–799. [Google Scholar] [CrossRef]
- Gabriel, M.; Decristoforo, C.; Kendler, D.; Dobrozemsky, G.; Heute, D.; Uprimny, C.; Kovacs, P.; Von Guggenberg, E.; Bale, R.; Virgolini, I.J. 68Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: Comparison with somatostatin receptor scintigraphy and CT. J. Nucl. Med. 2007, 48, 508–518. [Google Scholar] [CrossRef]
- Caplin, M.E.; Baudin, E.; Ferolla, P.; Filosso, P.; Garcia-Yuste, M.; Lim, E.; Oberg, K.; Pelosi, G.; Perren, A.; Rossi, R.E.; et al. Pulmonary neuroendocrine (carcinoid) tumors: European Neuroendocrine Tumor Society expert consensus and recommendations for best practice for typical and atypical pulmonary carcinoids. Ann. Oncol. 2015, 26, 1604–1620. [Google Scholar] [CrossRef]
- Vaidya, B.; Richardson, D.; Hilton, C.J.; Kendall-Taylor, P. Adrenocorticotropin-secreting carcinoid tumour identified and treated 12 years after presentation with Cushing’s syndrome. Postgrad. Med. J. 1997, 73, 737–739. [Google Scholar] [CrossRef]
- Chong, S.; Lee, K.S.; Kim, B.-T.; Choi, J.Y.; A Yi, C.; Chung, M.J.; Oh, D.-K.; Lee, J.-Y. Integrated PET/CT of pulmonary neuroendocrine tumors: Diagnostic and prognostic implications. AJR Am. J. Roentgenol. 2007, 188, 1223–1231. [Google Scholar] [CrossRef]
- Erasmus, J.J.; McAdams, H.P.; Patz, E.F., Jr.; Coleman, R.E.; Ahuja, V.; Goodman, P.C. Evaluation of Primary Pulmonary Carcinoid Tumors Using FDG PET. AJR Am. J. Roentgenol. 1998, 170, 1369–1373. [Google Scholar] [CrossRef]
- Daniels, C.E.; Lowe, V.J.; Aubry, M.-C.; Allen, M.S.; Jett, J.R. The utility of fluorodeoxyglucose positron emission tomography in the evaluation of carcinoid tumors presenting as pulmonary nodules. Chest 2007, 131, 255–260. [Google Scholar] [CrossRef]
- Hurt, R.; Bates, M. Carcinoid tumours of the bronchus: A 33 year experience. Thorax 1984, 39, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Aslan, D.L.; Gulbahce, H.E.; Pambuccian, S.E.; Manivel, J.C.; Jessurun, J. Ki-67 immunoreactivity in the differential diagnosis of pulmonary neuroendocrine neoplasms in specimens with extensive crush artifact. Am. J. Clin. Pathol. 2005, 123, 874–878. [Google Scholar] [CrossRef]
- Pelosi, G.; Rodriguez, J.; Viale, G.; Rosai, J. Typical and atypical pulmonary carcinoid tumor overdiagnosed as small-cell carcinoma on biopsy specimens: A major pitfall in the management of lung cancer patients. Am. J. Surg. Pathol. 2005, 29, 179–187. [Google Scholar] [CrossRef]
- Detterbeck, F.C.; Boffa, D.J.; Kim, A.W.; Tanoue, L.T. The Eighth Edition Lung Cancer Stage Classification. Chest 2017, 151, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, I.; Le Teuff, G.; Guigay, J.; Caramella, C.; Berdelou, A.; Leboulleux, S.; Déandréis, D.; Hadoux, J.; Ducreux, M.; Duvillard, P.; et al. Antitumour activity of somatostatin analogues in sporadic, progressive, metastatic pulmonary carcinoids. Eur. J. Cancer 2017, 75, 259–267. [Google Scholar] [CrossRef]
- Lenotti, E.; Alberti, A.; Spada, F.; Amoroso, V.; Maisonneuve, P.; Grisanti, S.; Baggi, A.; Bianchi, S.; Fazio, N.; Berruti, A. Outcome of Patients with Metastatic Lung Neuroendocrine Tumors Submitted to First Line Monotherapy with Somatostatin Analogs. Front. Endocrinol. 2021, 12, 669484. [Google Scholar] [CrossRef] [PubMed]
- Crona, J.; Fanola, I.; Lindholm, D.P.; Antonodimitrakis, P.; Öberg, K.; Eriksson, B.; Granberg, D. Effect of Temozolomide in Patients with Metastatic Bronchial Carcinoids. Neuroendocrinology 2013, 98, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Ferolla, P.; Brizzi, M.P.; Meyer, T.; Mansoor, W.; Mazieres, J.; Cao, C.D.; Léna, H.; Berruti, A.; Damiano, V.; Buikhuisen, W.; et al. Efficacy and safety of long-acting pasireotide or everolimus alone or in combination in patients with advanced carcinoids of the lung and thymus (LUNA): An open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2017, 18, 1652–1664. [Google Scholar] [CrossRef] [PubMed]
- Papaxoinis, G.; Kordatou, Z.; McCallum, L.; Nasralla, M.; Lamarca, A.; Backen, A.; Nonaka, D.; Mansoor, W. Capecitabine and Temozolomide in Patients with Advanced Pulmonary Carcinoid Tumours. Neuroendocrinology 2020, 110, 413–421. [Google Scholar] [CrossRef]
- van Essen, M.; Krenning, E.P.; Bakker, W.H.; de Herder, W.W.; van Aken, M.O.; Kwekkeboom, D.J. Peptide receptor radionuclide therapy with (177)Lu-octreotate in patients with foregut carcinoid tumours of bronchial, gastric and thymic origin. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 1219–1227. [Google Scholar] [CrossRef]
- Imhof, A.; Brunner, P.; Marincek, N.; Briel, M.; Schindler, C.; Rasch, H.; Macke, H.R.; Rochlitz, C.; Muller-Brand, J.; Walter, M.A. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. J. Clin. Oncol. 2011, 29, 2416–2423. [Google Scholar] [CrossRef] [PubMed]
- Ianniello, A.; Sansovini, M.; Severi, S.; Nicolini, S.; Grana, C.M.; Massri, K.; Bongiovanni, A.; Antonuzzo, L.; Di Iorio, V.; Sarnelli, A.; et al. Peptide receptor radionuclide therapy with (177)Lu-DOTATATE in advanced bronchial carcinoids: Prognostic role of thyroid transcription factor 1 and (18)F-FDG PET. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Sabet, A.; Haug, A.R.; Eiden, C.; Auernhammer, C.J.; Simon, B.; Bartenstein, P.; Biersack, H.J.; Ezziddin, S. Efficacy of peptide receptor radionuclide therapy with (177)Lu-octreotate in metastatic pulmonary neuroendocrine tumors: A dual-centre analysis. Am. J. Nucl. Med. Mol. Imaging 2017, 7, 74–83. [Google Scholar] [PubMed]
- Mariniello, A.; Bodei, L.; Tinelli, C.; Baio, S.M.; Gilardi, L.; Colandrea, M.; Papi, S.; Valmadre, G.; Fazio, N.; Galetta, D.; et al. Long-term results of PRRT in advanced bronchopulmonary carcinoid. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 441–452. [Google Scholar] [CrossRef]
- Fazio, N.; Granberg, D.; Grossman, A.; Saletan, S.; Klimovsky, J.; Panneerselvam, A.; Wolin, E.M. Everolimus plus octreotide long-acting repeatable in patients with advanced lung neuroendocrine tumors: Analysis of the phase 3, randomized, placebo-controlled RADIANT-2 study. Chest 2013, 143, 955–962. [Google Scholar] [CrossRef]
- Fazio, N.; Buzzoni, R.; Delle Fave, G.; Tesselaar, M.E.; Wolin, E.; Van Cutsem, E.; Tomassetti, P.; Strosberg, J.; Voi, M.; Ridolfi, A.; et al. Everolimus in advanced, progressive, well-differentiated, non-functional neuroendocrine tumors: RADIANT-4 lung subgroup analysis. Cancer Sci. 2018, 109, 174–181. [Google Scholar] [CrossRef]
- Yao, J.C.; Strosberg, J.; Fazio, N.; Pavel, M.E.; Bergsland, E.; Ruszniewski, P.; Halperin, D.M.; Li, D.; Tafuto, S.; Raj, N.; et al. Spartalizumab in metastatic, well/poorly-differentiated neuroendocrine neoplasms. Endocr. Relat. Cancer 2021, 28, 161–172. [Google Scholar] [CrossRef]
- Mehnert, J.M.; Bergsland, E.; O’Neil, B.H.; Santoro, A.; Schellens, J.H.M.; Cohen, R.B.; Doi, T.; Ott, P.A.; Pishvaian, M.J.; Puzanov, I.; et al. Pembrolizumab for the treatment of programmed death-ligand 1-positive advanced carcinoid or pancreatic neuroendocrine tumors: Results from the KEYNOTE-028 study. Cancer 2020, 126, 3021–3030. [Google Scholar] [CrossRef]
- Dell’amore, A.; Chen, L.; Monaci, N.; Campisi, A.; Wang, Z.; Mammana, M.; Pangoni, A.; Zhao, H.; Schiavon, M.; Yao, F.; et al. Total Lung-sparing Surgery for Tracheobronchial Low-grade Malignancies. Ann. Thorac. Surg. 2021, 112, 450–458. [Google Scholar] [CrossRef]
- Kurul, I.C.; Topçu, S.; TaşTepe, I.; Yazici, A.T.; Cetinçetin, G. Surgery in bronchial carcinoids: Experience with 83 patients. Eur. J. Cardiothorac. Surg. 2002, 21, 883–887. [Google Scholar] [CrossRef]
- Reuling, E.; Dickhoff, C.; Plaisier, P.; Bonjer, H.; Daniels, J. Endobronchial and surgical treatment of pulmonary carcinoid tumors: A systematic literature review. Lung Cancer 2019, 134, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Fox, M.; Van Berkel, V.; Bousamra, M., II; Sloan, S.; Martin, R.C., II. Surgical management of pulmonary carcinoid tumors: Sublobar resection versus lobectomy. Am. J. Surg. 2013, 205, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Soldath, P.; Binderup, T.; Kjær, A.; Federspiel, B.; Langer, S.W.; Knigge, U.; Petersen, R.H. Long-term survival and recurrence after resection of bronchopulmonary carcinoids: A single-center cohort study of 236 patients. Lung Cancer 2021, 156, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Sihoe, A.D.L. Video-assisted thoracoscopic surgery as the gold standard for lung cancer surgery. Respirology 2020, 25 (Suppl. 2), 49–60. [Google Scholar] [CrossRef] [PubMed]
- Augustin, F.; Maier, H.T.; Weissenbacher, A.; Ng, C.; Lucciarini, P.; Öfner, D.; Ulmer, H.; Schmid, T. Causes, predictors and consequences of conversion from VATS to open lung lobectomy. Surg. Endosc. 2016, 30, 2415–2421. [Google Scholar] [CrossRef]
- Brokx, H.A.; Risse, E.K.; Paul, M.A.; Grünberg, K.; Golding, R.P.; Kunst, P.W.; Eerenberg, J.-P.; van Mourik, J.C.; Postmus, P.E.; Mooi, W.J.; et al. Initial bronchoscopic treatment for patients with intraluminal bronchial carcinoids. J. Thorac. Cardiovasc. Surg. 2007, 133, 973–978. [Google Scholar] [CrossRef]
- Neyman, K.; Sundset, A.; Naalsund, A.; Espinoza, A.; Solberg, S.; Kongerud, J.; Fosse, E. Endoscopic treatment of bronchial carcinoids in comparison to surgical resection: A retrospective study. J. Bronchol. Interv. Pulmonol. 2012, 19, 29–34. [Google Scholar] [CrossRef]
- Anderson, K.L.; Mulvihill, M.S.; Speicher, P.J.; Yerokun, B.A.; Gulack, B.C.; Nussbaum, D.P.; Harpole, D.H.; D’amico, T.A.; Berry, M.F.; Hartwig, M.G. Adjuvant Chemotherapy Does Not Confer Superior Survival in Patients with Atypical Carcinoid Tumors. Ann. Thorac. Surg. 2017, 104, 1221–1230. [Google Scholar] [CrossRef]
- Nussbaum, D.P.; Speicher, P.J.; Gulack, B.C.; Hartwig, M.G.; Onaitis, M.W.; D’amico, T.A.; Berry, M.F. Defining the role of adjuvant chemotherapy after lobectomy for typical bronchopulmonary carcinoid tumors. Ann. Thorac. Surg. 2015, 99, 428–434. [Google Scholar] [CrossRef]
- Rinke, A.; Müller, H.H.; Schade-Brittinger, C.; Klose, K.-J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.-F.; Bläker, M.; et al. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors: A Report From the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef]
- Baudin, E.; Horsch, D.; Singh, S.; Caplin, M.; Ferone, D.; Wolin, E.; Capdevila, J.; Buikhuisen, W.; Raderer, M.; Dansin, E.; et al. Lanreotide autogel/depot (LAN) in patients with advanced bronchopulmonary (BP) neuroendocrine tumors (NETs): Results from the phase III SPINET study. Ann. Oncol. 2021, 32 (Suppl. 5), S906–S920. [Google Scholar] [CrossRef]
- De Dosso, S.; Bajetta, E.; Procopio, G.; Cortinovis, D.; Buzzoni, R.; Catena, L.; Platania, M.; Verzoni, E. Pulmonary carcinoid tumours: Indolent but not benign. Oncology 2007, 73, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Granberg, D.; Eriksson, B.; Wilander, E.; Grimfjärd, P.; Fjällskog, M.-L.; Öberg, K.; Skogseid, B. Experience in treatment of metastatic pulmonary carcinoid tumors. Ann. Oncol. 2001, 12, 1383–1391. [Google Scholar] [CrossRef]
- Turner, N.C.; Strauss, S.J.; Sarker, D.; Gillmore, R.; Kirkwood, A.; Hackshaw, A.; Papadopoulou, A.; Bell, J.; Kayani, I.; Toumpanakis, C.; et al. Chemotherapy with 5-fluorouracil, cisplatin and streptozocin for neuroendocrine tumours. Br. J. Cancer 2010, 102, 1106–1112. [Google Scholar] [CrossRef] [PubMed]
- Wirth, L.J.; Carter, M.R.; Jänne, P.A.; Johnson, B.E. Outcome of patients with pulmonary carcinoid tumors receiving chemotherapy or chemoradiotherapy. Lung Cancer 2004, 44, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Chong, C.R.; Wirth, L.J.; Nishino, M.; Chen, A.B.; Sholl, L.M.; Kulke, M.H.; McNamee, C.J.; Jänne, P.A.; Johnson, B.E. Chemotherapy for locally advanced and metastatic pulmonary carcinoid tumors. Lung Cancer 2014, 86, 241–246. [Google Scholar] [CrossRef]
- Faure, M.; Niccoli, P.; Autret, A.; Cavaglione, G.; Mineur, L.; Raoul, J.L. Systemic chemotherapy with FOLFOX in metastatic grade 1/2 neuroendocrine cancer. Mol. Clin. Oncol. 2017, 6, 44–48. [Google Scholar] [CrossRef]
- Spada, F.; Antonuzzo, L.; Marconcini, R.; Radice, D.; Antonuzzo, A.; Ricci, S.; Di Costanzo, F.; Fontana, A.; Gelsomino, F.; Luppi, G.; et al. Oxaliplatin-Based Chemotherapy in Advanced Neuroendocrine Tumors: Clinical Outcomes and Preliminary Correlation with Biological Factors. Neuroendocrinology 2016, 103, 806–814. [Google Scholar] [CrossRef]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; Van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; de Vries, E.G.; et al. Everolimus for advanced pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.L.; Bang, Y.-J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A.; et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Bergsland, E.K.; Card, C.M.; Hope, T.A.; Kunz, P.L.; Laidley, D.T.; Lawrence, B.; Leyden, S.; Metz, D.C.; Michael, M.; et al. Commonwealth Neuroendocrine Tumour Research Collaboration and the North American Neuroendocrine Tumor Society Guidelines for the Diagnosis and Management of Patients with Lung Neuroendocrine Tumors: An International Collaborative Endorsement and Update of the 2015 European Neuroendocrine Tumor Society Expert Consensus Guidelines. J. Thorac. Oncol. 2020, 15, 1577–1598. [Google Scholar]
- Granberg, D.; Wilander, E.; Öberg, K. Expression of tyrosine kinase receptors in lung carcinoids. Tumor Biol. 2006, 27, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Grande, E.; Capdevila, J.; Castellano, D.; Teulé, A.; Durán, I.; Fuster, J.; Sevilla, I.; Escudero, P.; Sastre, J.; García-Donas, J.; et al. Pazopanib in pretreated advanced neuroendocrine tumors: A phase II, open-label trial of the Spanish Task Force Group for Neuroendocrine Tumors (GETNE). Ann. Oncol. 2015, 26, 1987–1993. [Google Scholar] [CrossRef]
- Kulke, M.H.; Lenz, H.J.; Meropol, N.J.; Posey, J.; Ryan, D.P.; Picus, J.; Bergsland, E.; Stuart, K.; Tye, L.; Huang, X.; et al. Activity of sunitinib in patients with advanced neuroendocrine tumors. J. Clin. Oncol. 2008, 26, 3403–3410. [Google Scholar] [CrossRef] [PubMed]
- Tsuruoka, K.; Horinouchi, H.; Goto, Y.; Kanda, S.; Fujiwara, Y.; Nokihara, H.; Yamamoto, N.; Asakura, K.; Nakagawa, K.; Sakurai, H.; et al. PD-L1 expression in neuroendocrine tumors of the lung. Lung Cancer 2017, 108, 115–120. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Norlen, O.; Stalberg, P.; Zedenius, J.; Hellman, P. Outcome after resection and radiofrequency ablation of liver metastases from small intestinal neuroendocrine tumours. Br. J. Surg. 2013, 100, 1505–1514. [Google Scholar] [CrossRef]
- Sobash, P.T.; Ullah, A.; Karim, N.A. Survival Benefit of Adjuvant Chemotherapy in Pulmonary Carcinoid Tumors. Cancers 2022, 14, 4730. [Google Scholar] [CrossRef]
- Daddi, N.; Schiavon, M.; Filosso, P.L.; Cardillo, G.; Ambrogi, M.C.; De Palma, A.; Luzzi, L.; Bandiera, A.; Casali, C.; Ruffato, A.; et al. Prognostic factors in a multicentre study of 247 atypical pulmonary carcinoids. Eur. J. Cardiothorac. Surg. 2014, 45, 677–686. [Google Scholar] [CrossRef]
- Baudin, E.; Caplin, M.; Garcia-Carbonero, R.; Fazio, N.; Ferolla, P.; Filosso, P.; Frilling, A.; de Herder, W.; Hörsch, D.; Knigge, U.; et al. Lung and thymic carcinoids: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 32, 439–451. [Google Scholar] [CrossRef]
- Lamarca, A.; Barriuso, J.; McNamara, M.G.; A Hubner, R.; Valle, J.W. Telotristat ethyl: A new option for the management of carcinoid syndrome. Expert. Opin. Pharmacother. 2016, 17, 2487–2498. [Google Scholar] [CrossRef]
- Lyseng-Williamson, K.A. Telotristat Ethyl: A Review in Carcinoid Syndrome Diarrhoea. Drugs 2018, 78, 941–950. [Google Scholar] [CrossRef]
- Young, J.; Haissaguerre, M.; Viera-Pinto, O.; Chabre, O.; Baudin, E.; Tabarin, A. Management of endocrine disease: Cushing’s syndrome due to ectopic ACTH secretion: An expert operational opinion. Eur. J. Endocrinol. 2020, 182, R29–R58. [Google Scholar] [CrossRef]
- Falhammar, H. Cyclic ectopic Cushing’s syndrome and somatostatin analogue treatment. N. Z. Med. J. 2009, 122, 92–95. [Google Scholar]
- Al-Toubah, T.; Strosberg, J.; Halfdanarson, T.R.; Oleinikov, K.; Gross, D.J.; Haider, M.; Sonbol, M.B.; Almquist, D.; Grozinsky-Glasberg, S. Somatostatin Analogs Improve Respiratory Symptoms in Patients with Diffuse Idiopathic Neuroendocrine Cell Hyperplasia. Chest 2020, 158, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Gorshtein, A.; Gross, D.J.; Barak, D.; Strenov, Y.; Refaeli, Y.; Shimon, I.; Grozinsky-Glasberg, S. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia and the associated lung neuroendocrine tumors: Clinical experience with a rare entity. Cancer 2012, 118, 612–619. [Google Scholar] [CrossRef]
- Nassar, A.A.; Jaroszewski, D.E.; Helmers, R.A.; Colby, T.V.; Patel, B.M.; Mookadam, F. Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia: A systematic overview. Am. J. Respir. Crit. Care Med. 2011, 184, 8–16. [Google Scholar] [CrossRef]
- Chughtai, T.S.; Morin, J.E.; Sheiner, N.M.; A Wilson, J.; Mulder, D.S. Bronchial carcinoid—Twenty years’ experience defines a selective surgical approach. Surgery 1997, 122, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.F., Jr.; Tazelaar, H.D.; Jett, J.R. Typical and atypical pulmonary carcinoids: Outcome in patients presenting with regional lymph node involvement. Chest 2001, 119, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Gal, A.A.; Colby, T.V.; Klimstra, D.S.; Falk, R.; Koss, M.N. Reproducibility of Neuroendocrine Lung Tumor Classification. Hum. Pathol. 1998, 29, 272–279. [Google Scholar] [CrossRef]
- Daskalakis, K.; Kaltsas, G.; Oberg, K.; Tsolakis, A.V. Lung Carcinoids: Long-Term Surgical Results and the Lack of Prognostic Value of Somatostatin Receptors and Other Novel Immunohistochemical Markers. Neuroendocrinology 2018, 107, 355–365. [Google Scholar] [CrossRef]
- Filosso, P.L.; Oliaro, A.; Ruffini, E.; Bora, G.; Lyberis, P.; Asioli, S.; Delsedime, L.; Sandri, A.; Guerrera, F. Outcome and Prognostic Factors in Bronchial Carcinoids: A Single-Center Experience. J. Thorac. Oncol. 2013, 8, 1282–1288. [Google Scholar] [CrossRef]
- Osakwe, N.C.; Narula, N.; Port, J.L.; Paul, S.; Stiles, B.M.; Andrews, W.G.; Nasar, A.; Altorki, N.K.; Lee, P.C. Predictors of Disease-free Survival and Recurrence in Patients with Resected Bronchial Carcinoid Tumors. Thorac. Cardiovasc. Surg. 2016, 64, 159–165. [Google Scholar] [CrossRef]
- Garcia-Yuste, M.; Matilla, J.M.; Cueto, A.; Paniagua, J.M.R.; Ramos, G.; Cañizares, M.A.; Muguruza, I. Typical and atypical carcinoid tumours: Analysis of the experience of the Spanish Multi-centric Study of Neuroendocrine Tumours of the Lung. Eur. J. Cardiothorac. Surg. 2007, 31, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Margaritora, S.; Cardillo, G.; Filosso, P.; Novellis, P.; Rapicetta, C.; Carleo, F.; Bora, G.; Cesario, A.; Stefani, A.; Rossi, G.; et al. Bronchopulmonary Carcinoids causing Cushing Syndrome: Results from a Multicentric Study Suggesting a More Aggressive Behavior. Thorac. Cardiovasc. Surg. 2016, 64, 172–181. [Google Scholar] [CrossRef]
- Granberg, D.; Wilander, E.; Öberg, K.; Skogseid, B. Prognostic Markers in Patients with Typical Bronchial Carcinoid Tumors. J. Clin. Endocrinol. Metab. 2000, 85, 3425–3430. [Google Scholar]
- Canizares, M.A.; Matilla, J.M.; Cueto, A.; Algar, J.; Muguruza, I.; Moreno-Mata, N.; Moreno-Balsalobre, R.; Guijarro, R.; Arrabal, R.; Garcia-Fontan, E.; et al. Atypical carcinoid tumours of the lung: Prognostic factors and patterns of recurrence. Thorax 2014, 69, 648–653. [Google Scholar] [CrossRef]
- Ciment, A.; Gil, J.; Teirstein, A. Late recurrent pulmonary typical carcinoid tumor: Case report and review of the literature. Mt. Sinai J. Med. 2006, 73, 884–886. [Google Scholar] [PubMed]
- Lou, F.; Sarkaria, I.; Pietanza, C.; Travis, W.; Roh, M.S.; Sica, G.; Healy, D.; Rusch, V.; Huang, J. Recurrence of pulmonary carcinoid tumors after resection: Implications for postoperative surveillance. Ann. Thorac. Surg. 2013, 96, 1156–1162. [Google Scholar] [CrossRef] [PubMed]
- Marciello, F.; Mercier, O.; Ferolla, P.; Scoazec, J.-Y.; Filosso, P.L.; Chapelier, A.; Guggino, G.; Monaco, R.; Grimaldi, F.; Pizzolitto, S.; et al. Natural History of Localized and Locally Advanced Atypical Lung Carcinoids after Complete Resection: A Joined French-Italian Retrospective Multicenter Study. Neuroendocrinology 2018, 106, 264–273. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | CR + PR | SD | PFS (mo) | OS (mo) | Reference | |
|---|---|---|---|---|---|---|
| Octr, Lan | 61 | 0 | 47 (77%) | 17.4 | 58.4 | [70] |
| Octr, Lan | 31 | 2 (6.5%) | 24 (77.4%) | 28.6 | NR | [71] |
| Tem | 31 | 3 (14%) | 11 (52%) | 5.3 | 23.2 | [72] |
| Pas | 41 | 1 (2.4%) | 14 (34.1%) | 8.5 | - | [73] |
| Cap + Tem | 33 | 6 (18%) | 19 (58%) | 9.0 | 30.4 | [74] |
| 177Lu | 9 | 5 (56%) | - | - | - | [75] |
| 90Y | 84 | 24 (29%) | - | - | 40 | [76] |
| 177Lu | 34 | 5 (15%) | 16 (47%) | 18.5 | 48.6 | [77] |
| 177Lu | 22 | 6 (27.3%) | 9 (40.9%) | 27 | 42 | [78] |
| 90Y, 177Lu, 90Y + 177Lu | 114 | 15 (13.3%) | 61 (53.5%) | 28.0 | 58.8 | [79] |
| Everolimus + Octr | 33 | 20 (66.7%) * | - | 13.6 | - | [80] |
| Everolimus | 63 | 1 (1.6%) | 50 (79.4%) | 9.2 | - | [81] |
| Everolimus | 42 | 1 (2.4%) | 13 (31.0%) | 12.5 | - | [73] |
| Everolimus + Pas | 41 | 1 (2.4%) | 20 (48.8%) | 11.8 | - | [73] |
| Spartalizumab | 30 | 5 (16.7%) | 17 (56.7%) | - | - | [82] |
| Pembrolizumab | 9 | 1 (11.1%) | - | - | - | [83] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granberg, D.; Juhlin, C.C.; Falhammar, H.; Hedayati, E. Lung Carcinoids: A Comprehensive Review for Clinicians. Cancers 2023, 15, 5440. https://doi.org/10.3390/cancers15225440
Granberg D, Juhlin CC, Falhammar H, Hedayati E. Lung Carcinoids: A Comprehensive Review for Clinicians. Cancers. 2023; 15(22):5440. https://doi.org/10.3390/cancers15225440
Chicago/Turabian StyleGranberg, Dan, Carl Christofer Juhlin, Henrik Falhammar, and Elham Hedayati. 2023. "Lung Carcinoids: A Comprehensive Review for Clinicians" Cancers 15, no. 22: 5440. https://doi.org/10.3390/cancers15225440