
Surveillance for Metastasis in High-Risk Uveal Melanoma Patients: Standard versus Enhanced Protocols

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Patient Demographics and Ocular Tumor Parameters
2.4. Prognostication
2.5. Surveillance Protocols
2.6. Survival Data
2.7. Main Outcome Measures
2.8. Statistical Analysis
3. Results
3.1. Study Patients
3.2. Patient Demographics and Ocular Tumor Parameters
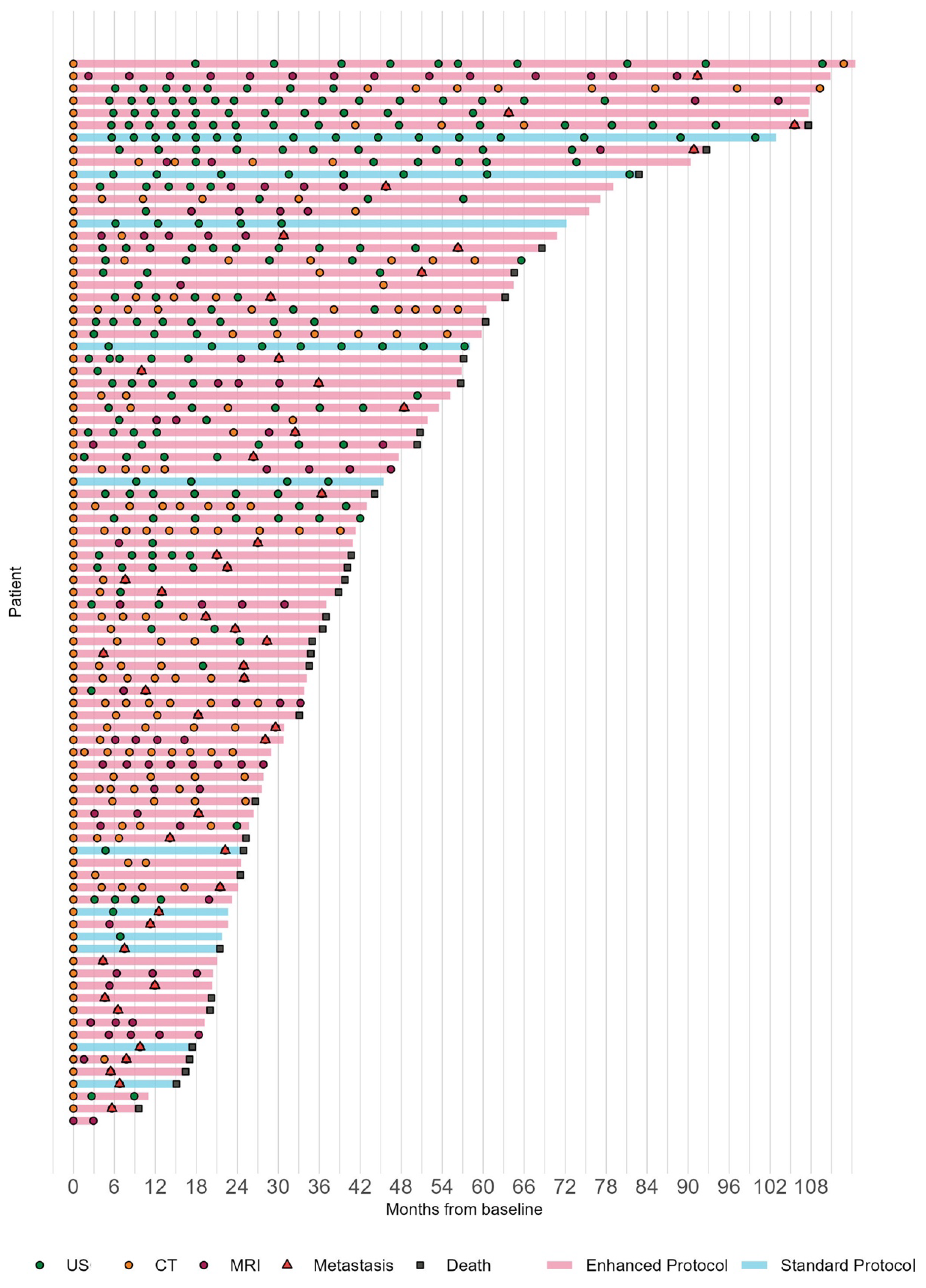
3.3. Surveillance Protocols
3.4. Characteristics of Metastatic Uveal Melanoma
3.5. Time to Prior Negative Scan and Survival since Detection of Metastasis
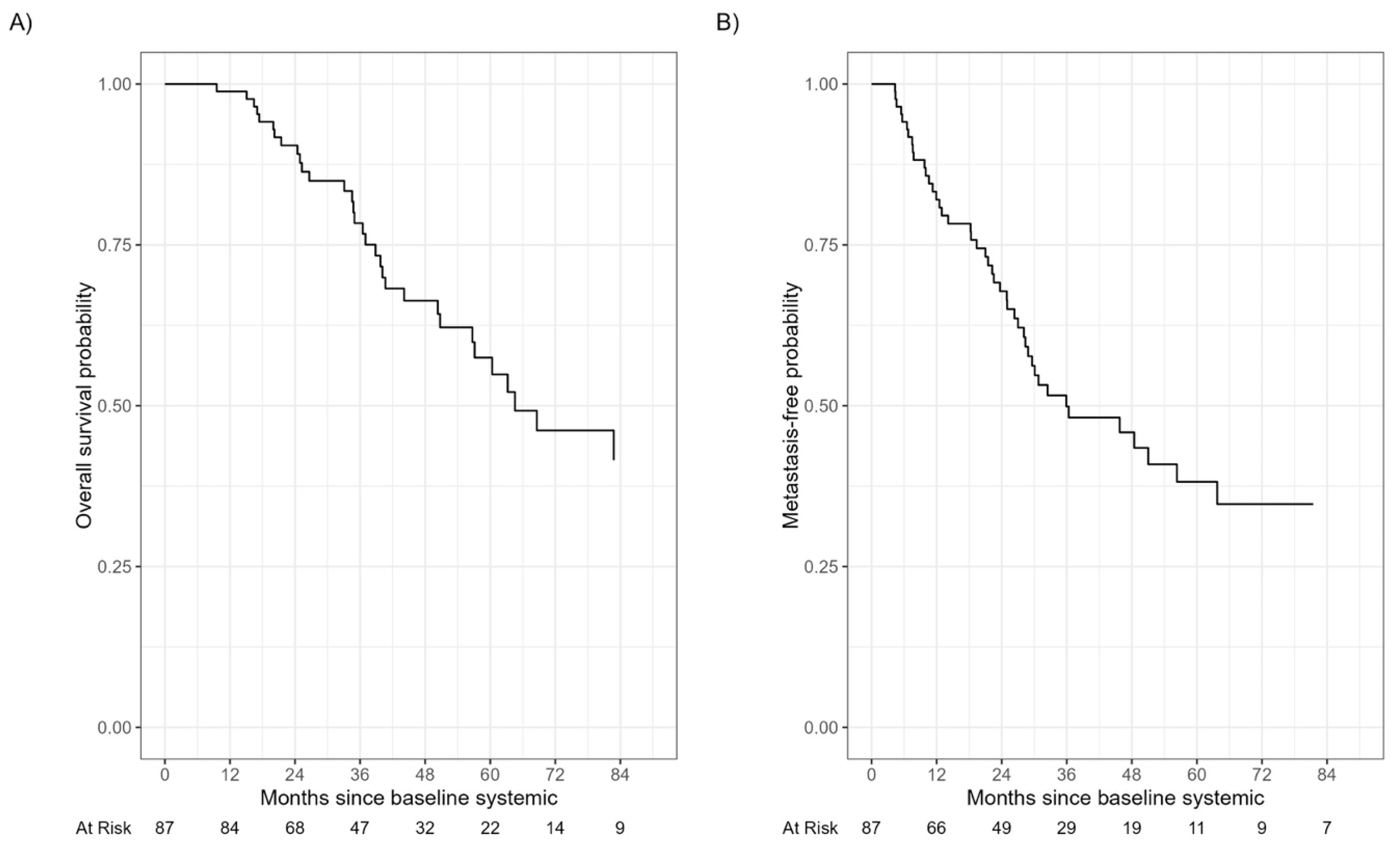
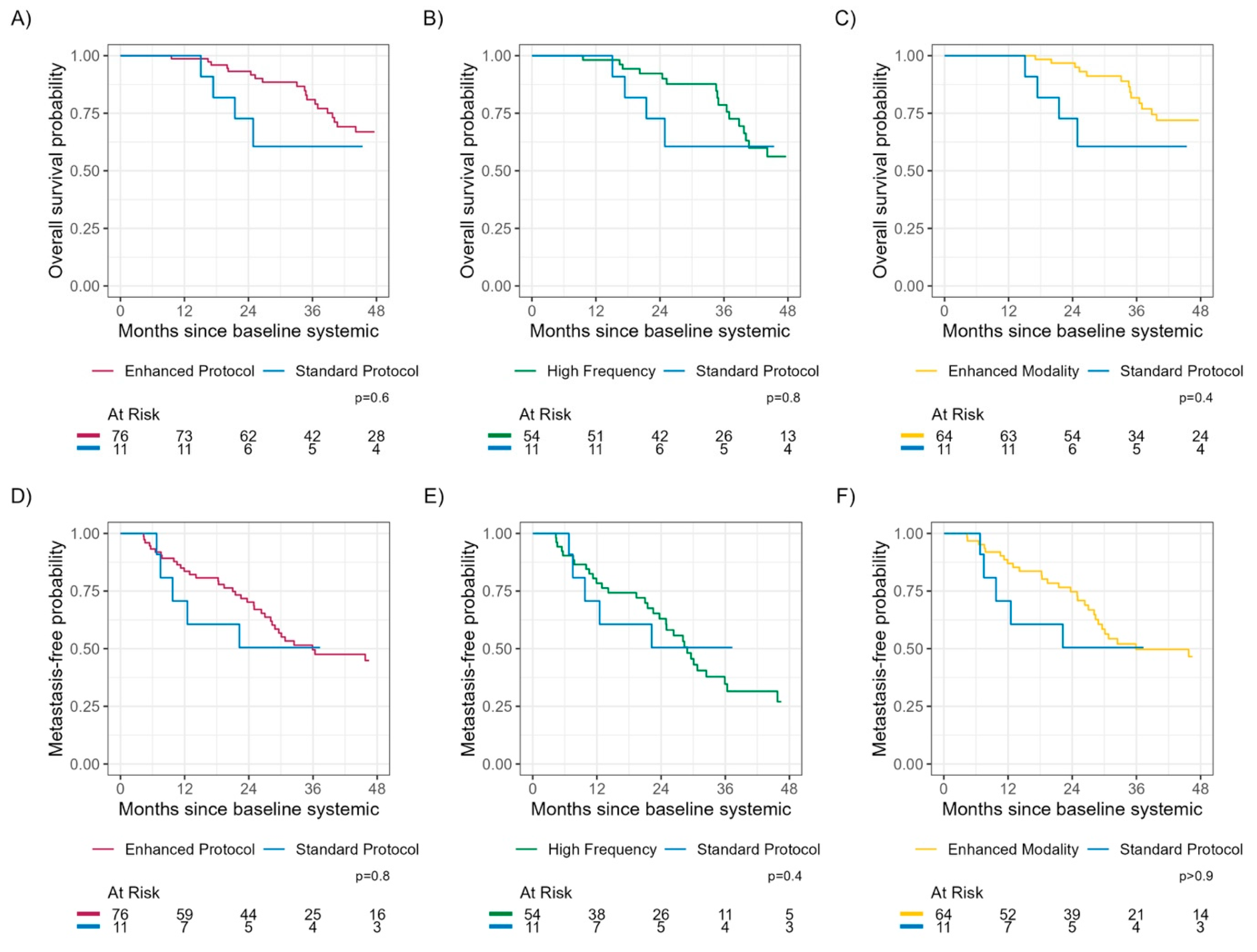
3.6. Time to Detection of Metastasis and Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eskelin, S.; Pyrhonen, S.; Summanen, P.; Prause, J.U.; Kivela, T. Screening for metastatic malignant melanoma of the uvea revisited. Cancer 1999, 85, 1151–1159. [Google Scholar] [CrossRef]
- Choudhary, M.M.; Gupta, A.; Bena, J.; Emch, T.; Singh, A.D. Hepatic Ultrasonography for Surveillance in Patients with Uveal Melanoma. JAMA Ophthalmol. 2016, 134, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Eskelin, S.; Pyrhonen, S.; Summanen, P.; Hahka-Kemppinen, M.; Kivela, T. Tumor doubling times in metastatic malignant melanoma of the uvea: Tumor progression before and after treatment. Ophthalmology 2000, 107, 1443–1449. [Google Scholar] [CrossRef] [PubMed]
- Harbour, J.W. A prognostic test to predict the risk of metastasis in uveal melanoma based on a 15-gene expression profile. Methods Mol Biol. 2014, 1102, 427–440. [Google Scholar] [PubMed]
- Field, M.G.; Harbour, J.W. Recent developments in prognostic and predictive testing in uveal melanoma. Curr. Opin. Ophthalmol. 2014, 25, 234–239. [Google Scholar] [CrossRef]
- Davanzo, J.M.; Binkley, E.M.; Bena, J.F.; Singh, A.D. Risk-stratified systemic surveillance in uveal melanoma. Br. J. Ophthalmol. 2019, 103, 1868–1871. [Google Scholar] [CrossRef]
- Rivoire, M.; Kodjikian, L.; Baldo, S.; Kaemmerlen, P.; Negrier, S.; Grange, J.D. Treatment of liver metastases from uveal melanoma. Ann Surg Oncol. 2005, 12, 422–428. [Google Scholar] [CrossRef]
- Barker, C.A.; Salama, A.K. New NCCN Guidelines for Uveal Melanoma and Treatment of Recurrent or Progressive Distant Metastatic Melanoma. J. Natl. Compr. Canc. Netw. 2018, 16, 646–650. [Google Scholar] [CrossRef]
- Marshall, E.; Romaniuk, C.; Ghaneh, P.; Wong, H.; McKay, M.; Chopra, M.; Coupland, S.E.; Damato, B.E. MRI in the detection of hepatic metastases from high-risk uveal melanoma: A prospective study in 188 patients. Br. J. Ophthalmol. 2013, 97, 159–163. [Google Scholar] [CrossRef]
- Aaberg, T.M., Jr.; Cook, R.W.; Oelschlager, K.; Maetzold, D.; Rao, P.K.; Mason, J.O., 3rd. Current clinical practice: Differential management of uveal melanoma in the era of molecular tumor analyses. Clin. Ophthalmol. 2014, 8, 2449–2460. [Google Scholar] [CrossRef]
- Nathan, P.; Cohen, V.; Coupland, S.; Curtis, K.; Damato, B.; Evans, J.; Fenwick, S.; Kirkpatrick, L.; Li, O.; Marshall, E.; et al. Uveal Melanoma UK National Guidelines. Eur. J. Cancer 2015, 51, 2404–2412. [Google Scholar] [CrossRef] [PubMed]
- Augsburger, J.J.; Correa, Z.M.; Trichopoulos, N. Surveillance testing for metastasis from primary uveal melanoma and effect on patient survival. Am. J. Ophthalmol. 2011, 152, 5–9 e1. [Google Scholar] [CrossRef] [PubMed]
- Gomez, D.; Wetherill, C.; Cheong, J.; Jones, L.; Marshall, E.; Damato, B.; Coupland, S.E.; Ghaneh, P.; Poston, G.J.; Malik, H.Z.; et al. The Liverpool uveal melanoma liver metastases pathway: Outcome following liver resection. J. Surg. Oncol. 2014, 109, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Mariani, P.; Piperno-Neumann, S.; Servois, V.; Berry, M.G.; Dorval, T.; Plancher, C.; Couturier, J.; Levy-Gabriel, C.; Lumbroso-Le Rouic, L.; Desjardins, L.; et al. Surgical management of liver metastases from uveal melanoma: 16 years’ experience at the Institut Curie. Eur. J. Surg. Oncol. 2009, 35, 1192–1197. [Google Scholar] [CrossRef]
- Frenkel, S.; Nir, I.; Hendler, K.; Lotem, M.; Eid, A.; Jurim, O.; Pe’er, J. Long-term survival of uveal melanoma patients after surgery for liver metastases. Br. J. Ophthalmol. 2009, 93, 1042–1046. [Google Scholar] [CrossRef]
- Trivedi, D.B.; Aldulaimi, N.; Karydis, I.; Wheater, M.; Modi, S.; Stedman, B.; Karavias, D.; Primrose, J.; Pearce, N.; Takhar, A.S. Liver resection for metastatic uveal melanoma: Experience from a supra-regional centre and review of literature. Melanoma Res. 2023, 33, 71–79. [Google Scholar] [CrossRef]
- Rantala, E.S.; Kivela, T.T.; Hernberg, M.M. Impact of staging on survival outcomes: A nationwide real-world cohort study of metastatic uveal melanoma. Melanoma Res. 2021, 31, 224–231. [Google Scholar] [CrossRef]
- Mariani, P.; Almubarak, M.M.; Kollen, M.; Wagner, M.; Plancher, C.; Audollent, R.; Piperno-Neumann, S.; Cassoux, N.; Servois, V. Radiofrequency ablation and surgical resection of liver metastases from uveal melanoma. Eur. J. Surg. Oncol. 2016, 42, 706–712. [Google Scholar] [CrossRef]
- Akyuz, M.; Yazici, P.; Dural, C.; Yigitbas, H.; Okoh, A.; Bucak, E.; McNamara, M.; Singh, A.; Berber, E. Laparoscopic management of liver metastases from uveal melanoma. Surg. Endosc. 2016, 30, 2567–2571. [Google Scholar] [CrossRef]
- Rantala, E.S.; Hernberg, M.; Kivela, T.T. Overall survival after treatment for metastatic uveal melanoma: A systematic review and meta-analysis. Melanoma Res. 2019, 29, 561–568. [Google Scholar] [CrossRef]
- Nathan, P.; Hassel, J.C.; Rutkowski, P.; Baurain, J.F.; Butler, M.O.; Schlaak, M.; Sullivan, R.J.; Ochsenreither, S.; Dummer, R.; Kirkwood, J.M.; et al. Overall Survival Benefit with Tebentafusp in Metastatic Uveal Melanoma. New Engl. J. Med. 2021, 385, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Kivela, T.; Simpson, E.; Grossniklaus, H.; Jager, M.; Singh, A.; Caminal, J. Uveal melanoma. In AJCC Cancer Staging Manual; Amin, M., Edge, S., Greene, F., Byrd, D., Brookland, R., Washington, M., Eds.; Springer: Chicago, IL, USA, 2017; pp. 813–826. [Google Scholar]
- Olofsson Bagge, R.; Nelson, A.; Shafazand, A.; All-Eriksson, C.; Cahlin, C.; Elander, N.; Helgadottir, H.; Kiilgaard, J.F.; Kinhult, S.; Ljuslinder, I.; et al. Isolated Hepatic Perfusion with Melphalan for Patients with Isolated Uveal Melanoma Liver Metastases: A Multicenter, Randomized, Open-Label, Phase III Trial (the SCANDIUM Trial). J. Clin. Oncol. 2023, 41, 3042–3050. [Google Scholar] [CrossRef] [PubMed]
- Olofsson Bagge, R.; Nelson, A.; Shafazand, A.; All-Eriksson, C.; Cahlin, C.; Elander, N.; Helgadottir, H.; Kiilgaard, J.F.; Kinhult, S.; Ljuslinder, I.; et al. Survival after isolated hepatic perfusion as a treatment for uveal melanoma liver metastases: Results from a randomized controlled trial (the SCANDIUM trial). J. Clin. Oncol. 2023, 41, LBA9512. [Google Scholar] [CrossRef]
- Cao, L.; Chen, S.; Sun, R.; Ashby, C.R., Jr.; Wei, L.; Huang, Z.; Chen, Z.S. Darovasertib, a novel treatment for metastatic uveal melanoma. Front. Pharmacol. 2023, 14, 1232787. [Google Scholar] [CrossRef]
- Piulats, J.M.; Espinosa, E.; de la Cruz Merino, L.; Varela, M.; Alonso Carrión, L.; Martín-Algarra, S.; López Castro, R.; Curiel, T.; Rodríguez-Abreu, D.; Redrado, M.; et al. Nivolumab Plus Ipilimumab for Treatment-Naive Metastatic Uveal Melanoma: An Open-Label, Multicenter, Phase II Trial by the Spanish Multidisciplinary Melanoma Group (GEM-1402). J. Clin. Oncol. 2021, 39, 586–598. [Google Scholar] [CrossRef]
- Zager, J.S.; Orloff, M.M.; Ferrucci, P.F.; Glazer, E.S.; Ejaz, A.; Richtig, E.; Ochsenreither, S.; Lowe, M.C.; Reddy, S.A.; Beasley, G.; et al. FOCUS phase 3 trial results: Percutaneous hepatic perfusion (PHP) with melphalan for patients with ocular melanoma liver metastases (PHP-OCM-301/301A). J. Clin. Oncol. 2022, 40 (Suppl. S16), 9510. [Google Scholar] [CrossRef]
- Rantala, E.S.; Peltola, E.; Helminen, H.; Hernberg, M.; Kivela, T.T. Hepatic Ultrasonography Compared with Computed Tomography and Magnetic Resonance Imaging at Diagnosis of Metastatic Uveal Melanoma. Am. J. Ophthalmol. 2020, 216, 156–164. [Google Scholar] [CrossRef]
- Maeda, T.; Tateishi, U.; Suzuki, S.; Arai, Y.; Kim, E.E.; Sugimura, K. Magnetic resonance screening trial for hepatic metastasis in patients with locally controlled choroidal melanoma. Jpn. J. Clin. Oncol. 2007, 37, 282–286. [Google Scholar] [CrossRef]
- Eberhardt, S.C.; Choi, P.H.; Bach, A.M.; Funt, S.A.; Felderman, H.E.; Hann, L.E. Utility of sonography for small hepatic lesions found on computed tomography in patients with cancer. J. Ultrasound Med. 2003, 22, 335–343. [Google Scholar] [CrossRef]
- Servois, V.; Mariani, P.; Malhaire, C.; Petras, S.; Piperno-Neumann, S.; Plancher, C.; Levy-Gabriel, C.; Lumbroso-le Rouic, L.; Desjardins, L.; Salmon, R.J. Preoperative staging of liver metastases from uveal melanoma by magnetic resonance imaging (MRI) and fluorodeoxyglucose-positron emission tomography (FDG-PET). Eur. J. Surg. Oncol. 2010, 36, 189–194. [Google Scholar] [CrossRef]
- Singh, A.D.; Binkley, E.M.; Wrenn, J.M.; Bena, J.F.; Hinz, C.; Boldt, H.C. Predicted vs Observed Metastasis-Free Survival in Individuals with Uveal Melanoma. JAMA Ophthalmol. 2022, 140, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Field, M.G.; Decatur, C.L.; Kurtenbach, S.; Gezgin, G.; van der Velden, P.A.; Jager, M.J.; Kozak, K.N.; Harbour, J.W. PRAME as an Independent Biomarker for Metastasis in Uveal Melanoma. Clin. Cancer Res. 2016, 22, 1234–1242. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Feature | Subtype | N = 87 1 | |
|---|---|---|---|
| Age (years) | 63 (57, 70) | ||
| Sex (Male/Female) | 44/43 | ||
| Tumor location | Choroid only | 63 (72%) | |
| Ciliary body +/− choroid | 24 (28%) | ||
| Tumor size (mm) | Largest basal diameter | 14.5 (11.0, 16.5) | |
| Tumor thickness | 6.1 (3.7, 9.1) | ||
| Uveal melanoma treatment | Plaque brachytherapy | 60 (69%) | |
| Enucleation | 27 (31%) | ||
| PRAME status | Positive | 24 (27%) | |
| Unknown | 38 (44%) | ||
| Surveillance protocol | Enhanced protocol | 76 (87%) | |
| Standard protocol | 11 (13%) | ||
| Months since prior negative scan | 6.0 (4.8, 7.0) | ||
| Number with hepatic metastasis | 47 (54%) 1 | ||
| Largest diameter of largest hepatic metastasis (cm) | 1.90 (1.20, 3.85) | ||
| Number of metastatic lesions | <5 | 20 (43%) | |
| ≥5 | 27 (57%) | ||
| Presence of extrahepatic metastasis | 7 (15%) | ||
| First-line metastasis treatment | Hepatic treatment | 20 (43%) | |
| Systemic +/− checkpoint inhibitors | 19 (40%) | ||
| No treatment | 6 (13%) | ||
| Unknown | 2 (4%) | ||
| Characteristics | Standard Protocol 1 (n = 11) | Enhanced Protocol 1 (n = 76) | p-Value 2 | High Frequency 1 (n = 54) | p-Value 2 | Enhanced Modality 1 (n = 64) | p-Value 2 |
|---|---|---|---|---|---|---|---|
| Largest diameter of largest hepatic metastasis | |||||||
| ≤3 cm | 10% (0.43%, 38%) | 24% (15%, 35%) | 0.050 | 31% (18%, 44%) | 0.017 | 22% (12%, 33%) | 0.063 |
| >3 cm | 39% (10%, 68%) | 5.7% (1.8%, 13%) | 0.043 | 6.2% (1.6%, 15%) | 0.064 | 3.5% (0.64%, 11%) | 0.021 |
| Number of hepatic metastatic lesions | |||||||
| <5 | 20% (2.5%, 50%) | 11% (5.2%, 20%) | 0.7 | 12% (4.9%, 23%) | 0.5 | 10% (4.1%, 20%) | 0.8 |
| ≥5 | 29% (5.9%, 59%) | 18% (10%, 28%) | >0.9 | 25% (14%, 38%) | 0.7 | 15% (7.3%, 25%) | >0.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yeşiltaş, Y.S.; Zabor, E.C.; Wrenn, J.; Oakey, Z.; Singh, A.D. Surveillance for Metastasis in High-Risk Uveal Melanoma Patients: Standard versus Enhanced Protocols. Cancers 2023, 15, 5025. https://doi.org/10.3390/cancers15205025
Yeşiltaş YS, Zabor EC, Wrenn J, Oakey Z, Singh AD. Surveillance for Metastasis in High-Risk Uveal Melanoma Patients: Standard versus Enhanced Protocols. Cancers. 2023; 15(20):5025. https://doi.org/10.3390/cancers15205025
Chicago/Turabian StyleYeşiltaş, Yağmur Seda, Emily C. Zabor, Jacquelyn Wrenn, Zackery Oakey, and Arun D. Singh. 2023. "Surveillance for Metastasis in High-Risk Uveal Melanoma Patients: Standard versus Enhanced Protocols" Cancers 15, no. 20: 5025. https://doi.org/10.3390/cancers15205025