

Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management

Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
3. Definition and Measurement of Obesity
4. Epidemiology
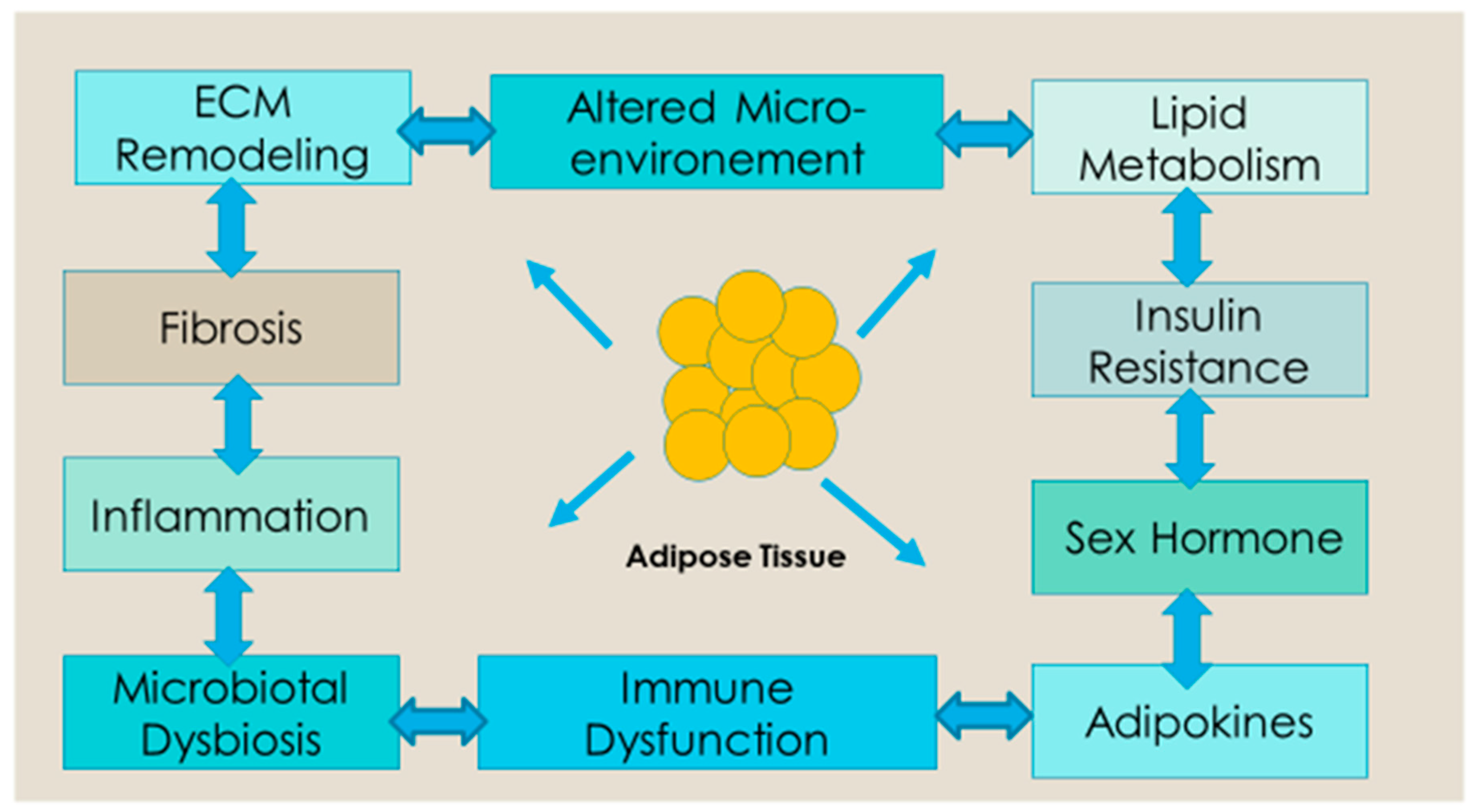
5. Biological Relationship between Obesity and Cancer
Obesity, Body Fat Distribution and Metabolic Syndrome
6. Obesity and Cancer Risk
7. Obesity and Cancer Outcomes
7.1. Breast Cancer
7.2. Colorectal Cancer
7.3. Pancreatic Cancer
7.4. Endometrial Cancer
7.5. Prostate Cancer
8. Obesity and Treatment-Related Adverse Effects
Treatment Selection
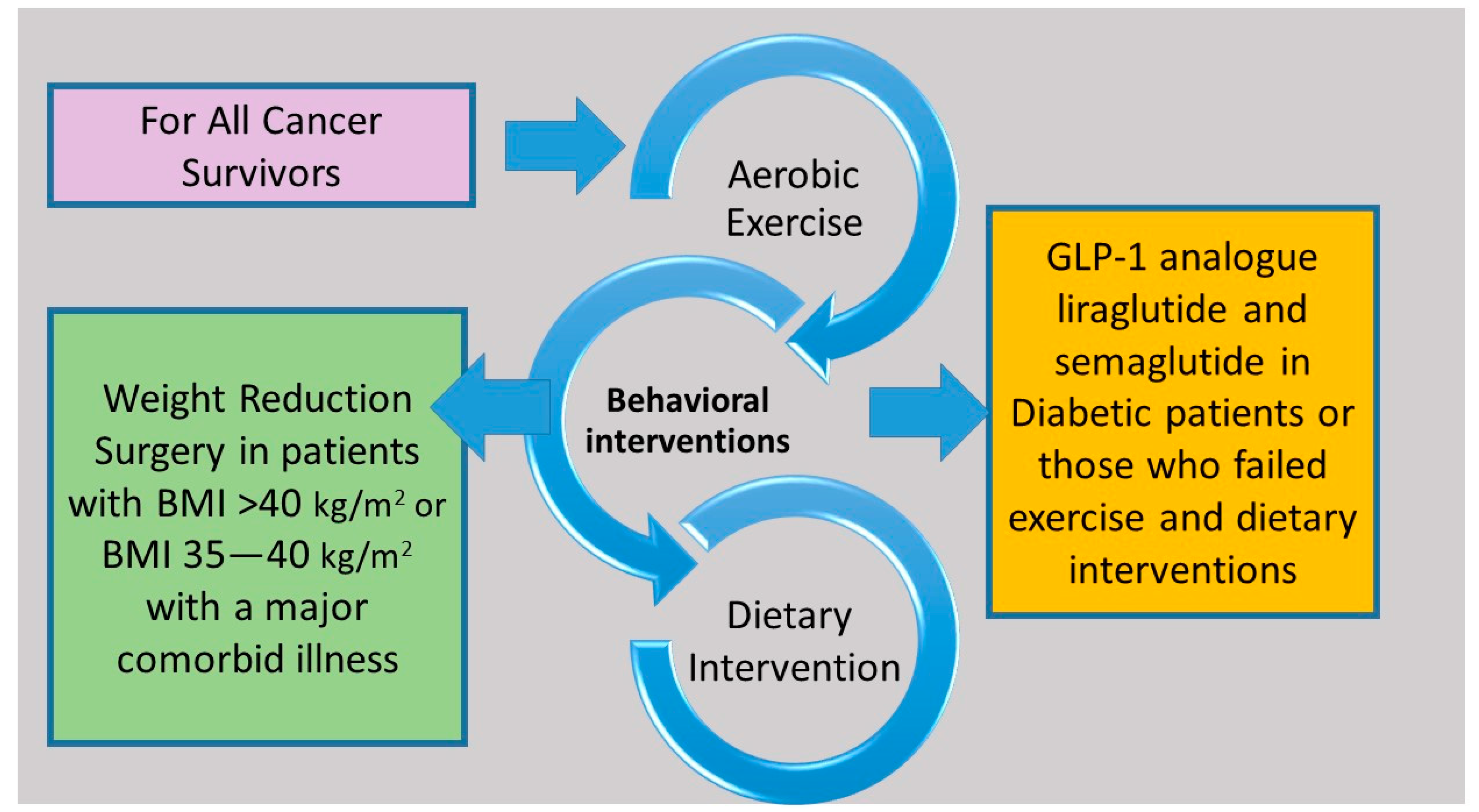
9. Management of Obesity in Cancer Survivors
9.1. Diet
9.2. Exercise
9.3. Behavior Therapy
9.4. Drug Therapy

{kind=link}
{kind=link}
| Drug [28,156] | Mechanism of Action | Dose | Weight Change Relative to Placebo | Side Effects |
|---|---|---|---|---|
| Semaglutide | glucagon-like peptide 1 receptor (GLP1R) agonists, decreases appetite and delays gastric emptying and gut motility | 2.4 mg once per week subcutaneous injection | 2.4% to 14.9% | abdominal pain, constipation, diarrhea, nausea, vomiting, and pancreatitis (rare) |
| Liraglutide | GLP1R agonists, decreases appetite and delays gastric emptying and gut motility | 3.0 mg per day subcutaneous injection | 2.6% to 8% | diarrhea, nausea, vomiting, constipation, dyspepsia, abdominal pain, pancreatitis, and gallstones |
| Naltrexone SR/bupropion SR | Opioid receptor antagonist/dopamine and noradrenaline reuptake inhibitor causing appetite suppression | 32 mg/360 mg oral twice daily | dose dependent 1.3% to 6.1% | headaches, hypertension, sleep disorders, nausea, constipation, vomiting, diarrhea, palpitation, dizziness, tremor, and others |
| Orlistat | Pancreatic lipase inhibitor causing excretion of 30% of ingested trigylcerides in stool | 120 mg 3 times daily | 6.1% to 10.2% | nausea, diarrhea, steatorrhea, abdominal bloating, and hepatitis |
| Phentermine/ topiramate | Sympathomimetics/anticonvulsant causing appetite suppression | 15 mg/92 mg once daily oral | dose depending 1.2% to 7.8% | tachycardia, xerostomia, constipation, headache, sleep disorder, anxiety, depression, suicidal ideation, and cardiovascular event |
| Phendimetrazine | Sympathomimetics causing appetite suppression | Short-term (≤12 weeks) 17.5 to 35 mg 2 or 3 times daily | Not available | hypertension, ischemic events, palpitations, tachycardia, headache, insomnia, overstimulation, psychosis, and others |
9.5. Weight Reduction Surgery
10. Future Directions
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Obesity and Overweight. World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 1 September 2022).
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [PubMed]
- Kivimäki, M.; Strandberg, T.; Pentti, J.; Nyberg, S.T.; Frank, P.; Jokela, M.; Ervasti, J.; Suominen, S.B.; Vahtera, J.; Sipilä, P.N.; et al. Body-mass index and risk of obesity-related complex multimorbidity: An observational multicohort study. Lancet Diabetes Endocrinol. 2022, 10, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Renehan, A.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Pandeya, N.; Byrnes, G.; Renehan, P.A.G.; Stevens, G.A.; Ezzati, P.M.; Ferlay, J.; Miranda, J.J.; Romieu, I.; Dikshit, R.; et al. Global burden of cancer attributable to high body-mass index in 2012: A population-based study. Lancet Oncol. 2015, 16, 36–46. [Google Scholar] [CrossRef]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K.; International Agency for Research on Cancer Handbook Working Group. Body Fatness and Cancer--Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Siegel, R.L.; Torre, L.A.; Pearson-Stuttard, J.; Islami, F.; Fedewa, S.A.; Goding Sauer, A.; Shuval, K.; Gapstur, S.M.; Jacobs, E.J.; et al. Global patterns in excess body weight and the associated cancer burden. CA Cancer J. Clin. 2019, 69, 88–112. [Google Scholar] [CrossRef]
- Islami, F.; Goding Sauer, A.; Gapstur, S.M.; Jemal, A. Proportion of cancer cases attributable to excess body weight by US state, 2011–2015. JAMA Oncol. 2019, 5, 384–392. [Google Scholar] [CrossRef]
- Jenabi, E.; Poorolajal, J. The effect of body mass index on endometrial cancer: A meta-analysis. Public Health 2015, 129, 872–880. [Google Scholar] [CrossRef]
- Hoyo, C.; Cook, M.B.; Kamangar, F.; Freedman, N.D.; Whiteman, D.C.; Bernstein, L.; Brown, L.M.; Risch, H.A.; Ye, W.; Sharp, L.; et al. Body mass index in relation to oesophageal and oesophagogastric junction adenocarcinomas: A pooled analysis from the International BEACON Consortium. Int. J. Epidemiol. 2012, 41, 1706–1718. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, L.; Wang, X.; Wang, J.; Yan, Z.; Cheng, J.; Gong, G.; Li, G. Body mass index and risk of gastric cancer: A meta-analysis of a population with more than ten million from 24 prospective studies. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 1395–1408. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, X.; Wang, J.; Yan, Z.; Luo, J. Excess body weight and the risk of primary liver cancer: An updated meta-analysis of prospective studies. Eur. J. Cancer 2012, 48, 2137–2145. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Xu, Y. Body mass index and risk of renal cell cancer: A dose-response meta-analysis of published cohort studies. Int. J. Cancer 2014, 135, 1673–1686. [Google Scholar] [CrossRef]
- Wallin, A.; Larsson, S.C. Body mass index and risk of multiple myeloma: A meta-analysis of prospective studies. Eur. J. Cancer 2011, 47, 1606–1615. [Google Scholar] [CrossRef]
- Niedermaier, T.; Behrens, G.; Schmid, D.; Schlecht, I.; Fischer, B.; Leitzmann, M.F. Body mass index, physical activity, and risk of adult meningioma and glioma: A meta-analysis. Neurology 2015, 85, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Genkinger, J.M.; Spiegelman, D.; Anderson, K.E.; Bernstein, L.; van den Brandt, P.A.; Calle, E.E.; English, D.R.; Folsom, A.R.; Freudenheim, J.L.; Fuchs, C.S.; et al. A pooled analysis of 14 cohort studies of anthropometric factors and pancreatic cancer risk. Int. J. Cancer 2011, 129, 1708–1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Yang, Y.; Wang, F.; Zhang, P.; Shi, C.; Zou, Y.; Qin, H. Obesity and risk of colorectal cancer: A systematic review of prospective studies. PLoS ONE 2013, 8, e53916. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Gan, Y.; Li, W.; Wu, C.; Lu, Z. Overweight, obesity and the risk of gallbladder and extrahepatic bile duct cancers: A meta-analysis of observational studies. Obesity 2016, 24, 1786–1802. [Google Scholar] [CrossRef] [Green Version]
- Coe, P.O.; O’Reilly, D.A.; Renehan, A.G. Excess adiposity and gastrointestinal cancer. Br. J. Surg. 2014, 101, 1518–1531. [Google Scholar] [CrossRef] [PubMed]
- Munsell, M.F.; Sprague, B.L.; Berry, D.A.; Chisholm, G.; Trentham-Dietz, A. Body mass index and breast cancer risk according to postmenopausal estrogen-progestin use and hormone receptor status. Epidemiol. Rev. 2014, 36, 114–136. [Google Scholar] [CrossRef] [PubMed]
- Chan, D.S.M.; Abar, L.; Cariolou, M.; Nanu, N.; Greenwood, D.C.; Bandera, E.V.; McTiernan, A.; Norat, T. World Cancer Research Fund International: Continuous Update Project-systematic literature review and meta-analysis of observational cohort studies on physical activity, sedentary behavior, adiposity, and weight change and breast cancer risk. Cancer Causes Control. 2019, 30, 1183–1200. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Group on Epidemiological Studies of Ovarian Cancer. Ovarian cancer and body size: Individual participant meta-analysis including 25,157 women with ovarian cancer from 47 epidemiological studies. PLoS Med. 2012, 9, e1001200. [Google Scholar]
- Aune, D.; Greenwood, D.C.; Chan, D.S.; Vieira, R.; Vieira, A.R.; Navarro Rosenblatt, D.A.; Cade, J.E.; Burley, V.J.; Norat, T. Body mass index, abdominal fatness and pancreatic cancer risk: A systematic review and non-linear dose-response meta-analysis of prospective studies. Ann. Oncol. 2012, 23, 843–852. [Google Scholar] [CrossRef]
- Schmid, D.; Ricci, C.; Behrens, G.; Leitzmann, M.F. Adiposity and risk of thyroid cancer: A systematic review and meta-analysis. Obes. Rev. 2015, 16, 1042–1054. [Google Scholar] [CrossRef]
- Barrington, W.E.; Schenk, J.M.; Etzioni, R.; Arnold, K.B.; Neuhouser, M.L.; Thompson, I.M., Jr.; Lucia, M.S.; Kristal, A.R. Difference in Association of Obesity With Prostate Cancer Risk Between US African American and Non-Hispanic White Men in the Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA Oncol. 2015, 1, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Sen, A.; Prasad, M.; Norat, T.; Janszky, I.; Tonstad, S.; Romundstad, P.; Vatten, L.J. BMI and all cause mortality: Systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants. BMJ 2016, 353, i2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrelli, F.; Cortellini, A.; Indini, A.; Tomasello, G.; Ghidini, M.; Nigro, O.; Salati, M.; Dottorini, L.; Iaculli, A.; Varricchio, A.; et al. Association of Obesity With Survival Outcomes in Patients With Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e213520. [Google Scholar] [CrossRef]
- Müller, T.D.; Blüher, M.; Tschöp, M.H.; DiMarchi, R.D. Anti-obesity drug discovery: Advances and challenges. Nat. Rev. Drug Discov. 2022, 21, 201–223. [Google Scholar] [PubMed]
- Pi-Sunyer, X.; Astrup, A.; Fujioka, K.; Greenway, F.; Halpern, A.; Krempf, M.; Lau, D.C.; le Roux, C.W.; Violante Ortiz, R.; Jensen, C.B.; et al. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management. N. Engl. J. Med. 2015, 373, 11–22. [Google Scholar] [CrossRef]
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.D.; Wadden, T.A.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med. 2021, 384, 989–1002. [Google Scholar] [CrossRef]
- James, W.P. WHO recognition of the global obesity epidemic. Int. J. Obes. 2008, 32 (Suppl. S7), S120–S126. [Google Scholar] [CrossRef] [Green Version]
- Jukaku, S.A.; Williams, S.R.P. The cause of obesity is multifactorial but GPs can do more. BMJ 2021, 373, n956. [Google Scholar] [CrossRef] [PubMed]
- Darsini, D.; Hamidah, H.; Notobroto, H.B.; Cahyono, E.A. Health risks associated with high waist circumference: A systematic review. J. Public Health Res. 2020, 9, 1811. [Google Scholar] [CrossRef] [PubMed]
- Ashwell, M.; Gunn, P.; Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes. Rev. 2012, 13, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Waist Circumference and Waist-Hip Ratio Report of a WHO Expert Consultation. GENEVA, 8–11 DECEMBER 2008. Available online: https://www.who.int/publications/i/item/9789241501491 (accessed on 1 September 2022).
- Harding, J.L.; Shaw, J.E.; Anstey, K.J.; Adams, R.; Balkau, B.; Brennan-Olsen, S.L.; Briffa, T.; Davis, T.M.; Davis, W.A.; Dobson, A.; et al. Comparison of anthropometric measures as predictors of cancer incidence: A pooled collaborative analysis of 11 Australian cohorts. Int. J. Cancer 2015, 137, 1699–1708. [Google Scholar] [CrossRef]
- Barberio, A.M.; Alareeki, A.; Viner, B.; Pader, J.; Vena, J.E.; Arora, P.; Friedenreich, C.M.; Brenner, D.R. Central body fatness is a stronger predictor of cancer risk than overall body size. Nat. Commun. 2019, 10, 383. [Google Scholar] [CrossRef] [Green Version]
- Recalde, M.; Davila-Batista, V.; Díaz, Y.; Leitzmann, M.; Romieu, I.; Freisling, H.; Duarte-Salles, T. Body mass index and waist circumference in relation to the risk of 26 types of cancer: A prospective cohort study of 3.5 million adults in Spain. BMC Med. 2021, 19, 10. [Google Scholar] [CrossRef]
- Staunstrup, L.M.; Nielsen, H.B.; Pedersen, B.K.; Karsdal, M.; Blair, J.P.M.; Christensen, J.F.; Bager, C.L. Cancer risk in relation to body fat distribution, evaluated by DXA-scans, in postmenopausal women—The Prospective Epidemiological Risk Factor (PERF) study. Sci. Rep. 2019, 9, 5379. [Google Scholar] [CrossRef] [Green Version]
- Wagner, D.R. Ultrasound as a tool to assess body fat. J. Obes. 2013, 2013, 280713. [Google Scholar] [CrossRef]
- Kim, Y.J.; Lee, S.H.; Kim, T.Y.; Park, J.Y.; Choi, S.H.; Kim, K.G. Body fat assessment method using CT images with separation mask algorithm. J. Digit. Imaging 2013, 26, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Borga, M. MRI adipose tissue and muscle composition analysis-a review of automation techniques. Br. J. Radiol. 2018, 91, 20180252. [Google Scholar] [CrossRef]
- Neeland, I.J.; Yokoo, T.; Leinhard, O.D.; Lavie, C.J. 21st Century Advances in Multimodality Imaging of Obesity for Care of the Cardiovascular Patient. JACC Cardiovasc. Imaging. 2021, 14, 482–494. [Google Scholar] [CrossRef]
- Li, Y.C.; Li, C.I.; Lin, W.Y.; Liu, C.S.; Hsu, H.S.; Lee, C.C.; Chen, F.N.; Li, T.C.; Lin, C.C. Percentage of body fat assessment using bioelectrical impedance analysis and dual-energy X-ray absorptiometry in a weight loss program for obese or overweight Chinese adults. PLoS ONE 2013, 8, e58272. [Google Scholar] [CrossRef] [Green Version]
- Kelly, T.; Yang, W.; Chen, C.S.; Reynolds, K.; He, J. Global burden of obesity in 2005 and projections to 2030. Int. J. Obes. 2008, 32, 1431–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund. Diet, Nutrition, Physical Activity and Cancer. A Global Perspective. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/Summary-of-Third-Expert-Report-2018.pdf (accessed on 1 September 2022).
- National Cancer Institute. Cancer Survivors and Weight. Available online: https://progressreport.cancer.gov/after/weight (accessed on 1 September 2022).
- Lengyel, E.; Makowski, L.; DiGiovanni, J.; Kolonin, M.G. Cancer as a Matter of Fat: The Crosstalk between adipose Tissue and Tumors. Trends Cancer 2018, 4, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.Z.; Pedersen, L.; Halberg, N. Cellular mechanisms linking cancers to obesity. Cell Stress 2021, 5, 55–72. [Google Scholar] [CrossRef] [PubMed]
- Annett, S.; Moore, G.; Robson, T. Obesity and Cancer Metastasis: Molecular and Translational Perspectives. Cancers 2020, 12, 3798. [Google Scholar] [CrossRef]
- Rogers, C.J.; Prabhu, K.S.; Vijay-Kumar, M. The microbiome and obesity-an established risk for certain types of cancer. Cancer J. 2014, 20, 176–180. [Google Scholar] [CrossRef]
- Renehan, A.; Zwahlen, M.; Egger, M. Adiposity and cancer risk: New mechanistic insights from epidemiology. Nat. Rev. Cancer 2015, 15, 484–498. [Google Scholar] [CrossRef]
- Bhardwaj, P.; Au, C.C.; Benito-Martin, A.; Ladumor, H.; Oshchepkova, S.; Moges, R.; Brown, K.A. Estrogens and breast cancer: Mechanisms involved in obesity-related development, growth and progression. J. Steroid. Biochem. Mol. Biol. 2019, 189, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Morley, T.; Kim, M.; Clegg, D.; Scherer, P. Obesity and cancer—Mechanisms underlying tumour progression and recurrence. Nat. Rev. Endocrinol. 2014, 10, 455–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedenreich, C.M.; Ryder-Burbidge, C.; McNeil, J. Physical activity, obesity and sedentary behavior in cancer etiology: Epidemiologic evidence and biologic mechanisms. Mol. Oncol. 2021, 15, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Shahid, R.K.; Ahmed, S.; Le, D.; Yadav, S. Diabetes and Cancer: Risk, Challenges, Management and Outcomes. Cancers 2021, 13, 5735. [Google Scholar] [CrossRef]
- Iyengar, N.; Gucalp, A.; Dannenberg, A.; Hudis, C. Obesity and Cancer Mechanisms: Tumor Microenvironment and Inflammation. J. Clin. Oncol. 2016, 34, 4270–4276. [Google Scholar] [CrossRef] [PubMed]
- Afify, S.M.; Hassan, G.; Seno, A.; Seno, M. Cancer-inducing niche: The force of chronic inflammation. Br. J. Cancer 2022, 127, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.A.; Diehl, A.M. Fat and the liver--a molecular overview. Semin. Gastrointest Dis. 2002, 13, 3–16. [Google Scholar]
- Seo, B.R.; Bhardwaj, P.; Choi, S.; Gonzalez, J.; Andresen Eguiluz, R.C.; Wang, K.; Mohanan, S.; Morris, P.G.; Du, B.; Zhou, X.K.; et al. Obesity-dependent changes in interstitial ECM mechanics promote breast tumorigenesis. Sci. Transl. Med. 2015, 7, 301ra130. [Google Scholar] [CrossRef] [Green Version]
- Cornier, M.A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The metabolic syndrome. Endocr. Rev. 2008, 29, 777–822. [Google Scholar]
- Varbo, A.; Benn, M.; Smith, G.D.; Timpson, N.J.; Tybjaerg-Hansen, A.; Nordestgaard, B.G. Remnant cholesterol, low-density lipoprotein cholesterol, and blood pressure as mediators from obesity to ischemic heart disease. Circ. Res. 2015, 116, 665–673. [Google Scholar] [CrossRef] [Green Version]
- Würtz, P.; Wang, Q.; Kangas, A.J.; Richmond, R.C.; Skarp, J.; Tiainen, M.; Tynkkynen, T.; Soininen, P.; Havulinna, A.S.; Kaakinen, M.; et al. Metabolic signatures of adiposity in young adults: Mendelian randomization analysis and effects of weight change. PLoS Med. 2014, 11, e1001765. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.A.; Carslake, D.; O’Keeffe, L.M.; Frysz, M.; Howe, L.D.; Hamer, M.; Wade, K.H.; Timpson, N.J.; Davey Smith, G. Associations of Body Mass and Fat Indexes With Cardiometabolic Traits. J. Am. Coll. Cardiol. 2018, 72, 3142–3154. [Google Scholar] [CrossRef]
- Lim, S.; Meigs, J.B. Ectopic fat and cardiometabolic and vascular risk. Int. J. Cardiol. 2013, 169, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D. Role of body fat distribution and the metabolic complications of obesity. J. Clin. Endocrinol. Metab. 2008, 93, S57–S63. [Google Scholar] [CrossRef] [PubMed]
- Karpe, F.; Pinnick, K.E. Biology of upper-body and lower-body adipose tissue--link to whole-body phenotypes. Nat. Rev. Endocrinol. 2015, 11, 90–100. [Google Scholar] [CrossRef]
- Grundy, S.M.; Williams, C.; Vega, G.L. Upper body fat predicts metabolic syndrome similarly in men and women. Eur. J. Clin. Investig. 2018, 48, e12941. [Google Scholar] [CrossRef] [Green Version]
- Nead, K.T.; Sharp, S.J.; Thompson, D.J.; Painter, J.N.; Savage, D.B.; Semple, R.K.; Barker, A.; Australian National Endometrial Cancer Study Group (ANECS). Evidence of a Causal Association Between Insulinemia and Endometrial Cancer: A Mendelian Randomization Analysis. J. Natl. Cancer Inst. 2015, 107, djv178. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Douglas, I.; Forbes, H.; dos-Santos-Silva, I.; Leon, D.A.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 524 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thrift, A.P.; Shaheen, N.J.; Gammon, M.D.; Bernstein, L.; Reid, B.J.; Onstad, L.; Risch, H.A.; Liu, G.; Bird, N.C.; Wu, A.H.; et al. Obesity and risk of esophageal adenocarcinoma and Barrett’s esophagus: A Mendelian randomization study. J. Natl. Cancer Inst. 2014, 106, dju252. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Yan, C.; Lu, Q.; Zhu, M.; Yu, F.; Wang, C.; Dai, J.; Ma, H.; Hu, Z.; Shen, H.; et al. Genetically predicted high body mass index is associated with increased gastric cancer risk. Eur. J. Hum. Genet. 2017, 25, 1061–1066. [Google Scholar] [CrossRef] [Green Version]
- Johansson, M.; Carreras-Torres, R.; Scelo, G.; Purdue, M.P.; Mariosa, D.; Muller, D.C.; Timpson, N.J.; Haycock, P.C.; Brown, K.M.; Wang, Z.; et al. The influence of obesity-related factors in the etiology of renal cell carcinoma-A mendelian randomization study. PLoS Med. 2019, 16, e1002724. [Google Scholar] [CrossRef] [Green Version]
- Gao, C.; Patel, C.J.; Michailidou, K.; Peters, U.; Gong, J.; Schildkraut, J.; Schumacher, F.R.; Zheng, W.; Boffetta, P.; Stucker, I.; et al. The Colorectal Transdisciplinary Study (CORECT); Discovery, Biology and Risk of Inherited Variants in Breast Cancer (DRIVE); Elucidating Loci Involved in Prostate Cancer Susceptibility (ELLIPSE); Follow-up of Ovarian Cancer Genetic Association and Interaction Studies (FOCI); and Transdisciplinary Research in Cancer of the Lung (TRICL). Mendelian randomization study of adiposity-related traits and risk of breast, ovarian, prostate, lung and colorectal cancer. Int. J. Epidemiol. 2016, 45, 896–908. [Google Scholar] [PubMed]
- Wild, C.P.; Weiderpass, E.; Stewart, B.W.; World Cancer Report. Cancer Research for Cancer Prevention. International Agency for Research on Cancer (IARC). Available online: https://www.iarc.who.int/cards_page/world-cancer-report/ (accessed on 1 September 2022).
- World Cancer Research Fund and American Institute for Cancer Research. Continuous Update Project Report. Food, Nutrition, Physical Activity, and the Prevention of Ovarian Cancer. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/ovarian-cancer-report.pdf (accessed on 18 September 2022).
- World Cancer Research Fund and American Institute for Cancer Research. Continuous Update Project Report: Diet, Nutrition, Physical Activity, and Prostate Cancer. Available online: https://www.wcrf.org/wp-content/uploads/2021/02/prostate-cancer-report.pdf (accessed on 18 September 2022).
- Kyrgiou, M.; Kalliala, I.; Markozannes, G.; Gunter, M.J.; Paraskevaidis, E.; Gabra, H.; Martin-Hirsch, P.; Tsilidis, K.K. Adiposity and cancer at major anatomical sites: Umbrella review of the literature. BMJ 2017, 356, 477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Premenopausal Breast Cancer Collaborative Group; Schoemaker, M.J.; Nichols, H.B.; Wright, L.B.; Brook, M.N.; Jones, M.E.; O’Brien, K.M.; Adami, H.O.; Baglietto, L.; Bernstein, L.; et al. Association of Body Mass Index and Age With Subsequent Breast Cancer Risk in Premenopausal Women. JAMA Oncol. 2018, 4, e181771. [Google Scholar] [PubMed]
- Iyengar, N.M.; Arthur, R.; Manson, J.E.; Chlebowski, R.T.; Kroenke, C.H.; Peterson, L.; Cheng, T.D.; Feliciano, E.C.; Lane, D.; Luo, J.; et al. Association of Body Fat and Risk of Breast Cancer in Postmenopausal Women With Normal Body Mass Index: A Secondary Analysis of a Randomized Clinical Trial and Observational Study. JAMA Oncol. 2019, 5, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, P.G.; Hudis, C.A.; Giri, D.; Morrow, M.; Falcone, D.J.; Zhou, X.K.; Du, B.; Brogi, E.; Crawford, C.B.; Kopelovich, L.; et al. Inflammation and increased aromatase expression occur in the breast tissue of obese women with breast cancer. Cancer Prev. Res. 2011, 4, 1021–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazzeroni, M.; Bellerba, F.; Calvello, M.; Macrae, F.; Win, A.K.; Jenkins, M.; Serrano, D.; Marabelli, M.; Cagnacci, S.; Tolva, G.; et al. A Meta-Analysis of Obesity and Risk of Colorectal Cancer in Patients with Lynch Syndrome: The Impact of Sex and Genetics. Nutrients 2021, 13, 1736. [Google Scholar] [CrossRef] [PubMed]
- Ligibel, J.A.; Alfano, C.M.; Hershman, D.; Ballard, R.M.; Bruinooge, S.S.; Courneya, K.S.; Daniels Elvan, C.; Demark-Wahnefried, W.; Frank Elizabeth, S.; Goodwin Pamela, J.; et al. Recommendations for Obesity Clinical Trials in Cancer Survivors: American Society of Clinical Oncology Statement. J. Clin. Oncol. 2015, 33, 3961–3967. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, E.; Bays, H.E. Cancer and Obesity: An Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022. Obes. Pillars 2022, 3, 100026. [Google Scholar] [CrossRef]
- Slawinski, C.; Barriuso, J.; Guo, H.; Renehan, A. Obesity and Cancer Treatment Outcomes: Interpreting the Complex Evidence. Clin. Oncol. 2020, 32, 591–608. [Google Scholar] [CrossRef]
- Parekh, N.; Chandran, U.; Bandera, E. Obesity in Cancer Survival. Annu. Rev. Nutr. 2012, 32, 311–342. [Google Scholar] [CrossRef] [Green Version]
- Ri, M.; Aikou, S.; Seto, Y. Obesity as a surgical risk factor. Ann. Gastroenterol. Surg. 2017, 2, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Fukagawa, T.; Haga, Y.; Oba, K. Does postoperative morbidity worsen the oncological outcome after radical surgery for gastrointestinal cancers? A systematic review of the literature. Ann. Gastroenterol. Surg. 2017, 1, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Ross, K.; Gogineni, K.; Subhedar, P.; Lin, J.; McCullough, L. Obesity and cancer treatment efficacy: Existing challenges and opportunities. Cancer 2019, 125, 1588–1592. [Google Scholar] [CrossRef]
- Kang, C.; LeRoith, D.; Gallagher, E.J. Diabetes, Obesity, and Breast Cancer. Endocrinology 2018, 159, 3801–3812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, L.S.; Watson, K.E.; Barac, A.; Beckie, T.M.; Bittner, V.; Cruz-Flores, S.; Dent, S.; Kondapalli, L.; Ky, B.; Okwuosa, T.; et al. American Heart Association Cardiovascular Disease in Women and Special Populations Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; and Council on Quality of Care and Outcomes Research. Cardiovascular Disease and Breast Cancer: Where These Entities Intersect: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e30–e66. [Google Scholar]
- Connor, A.E.; Baumgartner, R.N.; Pinkston, C.M.; Boone, S.D.; Baumgartner, K.B. Obesity, ethnicity, and quality of life among breast cancer survivors and women without breast cancer: The long-term quality of life follow-up study. Cancer Causes Control. 2016, 27, 115–124. [Google Scholar] [CrossRef] [Green Version]
- Chan, D.S.M.; Vieira, A.R.; Aune, D.; Bandera, E.V.; Greenwood, D.C.; McTiernan, A.; Navarro Rosenblatt, D.; Thune, I.; Vieira, R.; Norat, T. Body mass index and survival in women with breast cancer-systematic literature review and meta-analysis of 82 follow-up studies. Ann. Oncol. 2014, 25, 1901–1914. [Google Scholar] [CrossRef]
- Harborg, S.; Zachariae, R.; Olsen, J.; Johannsen, M.; Cronin-Fenton, D.; Bøggild, H.; Borgquist, S. Overweight and prognosis in triple-negative breast cancer patients: A systematic review and meta-analysis. NPJ Breast Cancer. 2021, 7, 119. [Google Scholar] [CrossRef]
- Renehan, A.G.; Harvie, M.; Cutress, R.I.; Leitzmann, M.; Pischon, T.; Howell, S.; Howell, A. How to Manage the Obese Patient With Cancer. J. Clin. Oncol. 2016, 34, 4284–4294. [Google Scholar] [CrossRef] [Green Version]
- Jiralerspong, S.; Goodwin, P.J. Obesity and Breast Cancer Prognosis: Evidence, Challenges, and Opportunities. J. Clin. Oncol. 2016, 34, 4203–4216. [Google Scholar] [CrossRef]
- Playdon, M.C.; Bracken, M.B.; Sanft, T.B.; Ligibel, J.A.; Harrigan, M.; Irwin, M.L. Weight Gain After Breast Cancer Diagnosis and All-Cause Mortality: Systematic Review and Meta-Analysis. J. Natl. Cancer Inst. 2015, 107, djv275. [Google Scholar] [CrossRef] [Green Version]
- Ioannides, S.J.; Barlow, P.L.; Elwood, J.M.; Porter, D. Effect of obesity on aromatase inhibitor efficacy in postmenopausal, hormone receptor-positive breast cancer: A systematic review. Breast. Cancer Res. Treat. 2014, 147, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Sinicrope, F.; Foster, N.; Yothers, G.; Benson, A.; Seitz, J.; Labianca, R.; Goldberg, R.; DeGramont, A.; O’Connell, M.; Sargent, D. Body mass index at diagnosis and survival among colon cancer patients enrolled in clinical trials of adjuvant chemotherapy. Cancer 2013, 119, 1528–1536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkin, E.; O’Reilly, D.; Sherlock, D.; Manoharan, P.; Renehan, A. Excess adiposity and survival in patients with colorectal cancer: A systematic review. Obes. Rev. 2014, 15, 434–451. [Google Scholar] [CrossRef] [PubMed]
- Doleman, B.; Mills, K.T.; Lim, S.; Zelhart, M.D.; Gagliardi, G. Body mass index and colorectal cancer prognosis: A systematic review and meta-analysis. Tech. Coloproctol. 2016, 20, 517–535. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Meyerhardt, J.A.; Giovannucci, E.; Jeon, J.Y. Association between body mass index and prognosis of colorectal cancer: A meta-analysis of prospective cohort studies. PLoS ONE 2015, 10, e0120706. [Google Scholar] [CrossRef] [Green Version]
- Mintziras, I.; Miligkos, M.; Wächter, S.; Manoharan, J.; Maurer, E.; Bartsch, D.K. Sarcopenia and sarcopenic obesity are significantly associated with poorer overall survival in patients with pancreatic cancer: Systematic review and meta-analysis. Int. J. Surg. 2018, 59, 19–26. [Google Scholar] [CrossRef]
- Majumder, K.; Gupta, A.; Arora, N.; Singh, P.P.; Singh, S. Premorbid Obesity and Mortality in Patients With Pancreatic Cancer: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2016, 14, 355–368.e2. [Google Scholar] [CrossRef] [Green Version]
- Kokts-Porietis, R.L.; Elmrayed, S.; Brenner, D.R.; Friedenreich, C.M. Obesity and mortality among endometrial cancer survivors: A systematic review and meta-analysis. Obes. Rev. 2021, 22, e13337. [Google Scholar] [CrossRef]
- Kokts-Porietis, R.L.; McNeil, J.; Morielli, A.R.; Cook, L.S.; Courneya, K.S.; Friedenreich, C.M. Prospective Cohort Study of Pre- and Postdiagnosis Obesity and Endometrial Cancer Survival. J. Natl. Cancer Inst. 2022, 114, 409–418. [Google Scholar] [CrossRef]
- Cao, Y.; Ma, J. Body mass index, prostate cancer-specific mortality, and biochemical recurrence: A systematic review and meta-analysis. Cancer Prev. Res. 2011, 4, 486–501. [Google Scholar] [CrossRef] [Green Version]
- Rivera-Izquierdo, M.; Pérez de Rojas, J.; Martínez-Ruiz, V.; Pérez-Gómez, B.; Sánchez, M.J.; Khan, K.S.; Jiménez-Moleón, J.J. Obesity as a Risk Factor for Prostate Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of 280,199 Patients. Cancers 2021, 13, 4169. [Google Scholar] [CrossRef] [PubMed]
- Vidal, A.C.; Howard, L.E.; Sun, S.X.; Cooperberg, M.R.; Kane, C.J.; Aronson, W.J.; Terris, M.K.; Amling, C.L.; Freedland, S.J. Obesity and prostate cancer-specific mortality after radical prostatectomy: Results from the Shared Equal Access Regional Cancer Hospital (SEARCH) database. Prostate Cancer Prostatic. Dis. 2017, 20, 72–78. [Google Scholar] [CrossRef] [Green Version]
- Meeske, K.A.; Sullivan-Halley, J.; Smith, A.W.; McTiernan, A.; Baumgartner, K.B.; Harlan, L.C.; Bernstein, L. Risk factors for arm lymphedema following breast cancer diagnosis in Black women and White women. Breast Cancer Res. Treat. 2009, 113, 383–391. [Google Scholar] [CrossRef]
- Helyer, L.K.; Varnic, M.; Le, L.W.; Leong, W.; McCready, D. Obesity is a risk factor for developing postoperative lymphedema in breast cancer patients. Breast J. 2010, 16, 48–54. [Google Scholar] [CrossRef]
- Mizrahi, D.; Park, S.B.; Li, T.; Timmins, H.C.; Trinh, T.; Au, K.; Battaglini, E.; Wyld, D.; Henderson, R.D.; Grimison, P.; et al. Hemoglobin, Body Mass Index, and Age as Risk Factors for Paclitaxel- and Oxaliplatin-Induced Peripheral Neuropathy. JAMA Netw. Open. 2021, 4, e2036695. [Google Scholar] [CrossRef]
- Ottaiano, A.; Nappi, A.; Tafuto, S.; Nasti, G.; De Divitiis, C.; Romano, C.; Cassata, A.; Casaretti, R.; Silvestro, L.; Avallone, A.; et al. Diabetes and body mass index are associated with neuropathy and prognosis in colon cancer patients treated with capecitabine and oxaliplatin adjuvant chemotherapy. Oncology 2016, 90, 36–42. [Google Scholar] [CrossRef]
- Guenancia, C.; Lefebvre, A.; Cardinale, D.; Yu, A.F.; Ladoire, S.; Ghiringhelli, F.; Zeller, M.; Rochette, L.; Cottin, Y.; Vergely, C. Obesity As a Risk Factor for Anthracyclines and Trastuzumab Cardiotoxicity in Breast Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2016, 34, 3157–3165. [Google Scholar] [CrossRef] [Green Version]
- Kaboré, E.G.; Guenancia, C.; Vaz-Luis, I.; Di Meglio, A.; Pistilli, B.; Coutant, C.; Cottu, P.; Lesur, A.; Petit, T.; Dalenc, F.; et al. Association of body mass index and cardiotoxicity related to anthracyclines and trastuzumab in early breast cancer: French CANTO cohort study. PLoS Med. 2019, 16, e1002989. [Google Scholar] [CrossRef]
- Xie, Y.; Wang, Q.; Hu, T.; Chen, R.; Wang, J.; Chang, H.; Cheng, J. Risk Factors Related to Acute Radiation Dermatitis in Breast Cancer Patients After Radiotherapy: A Systematic Review and Meta-Analysis. Front Oncol. 2021, 11, 738851. [Google Scholar] [CrossRef]
- Bouwman, F.; Smits, A.; Lopes, A.; Das, N.; Pollard, A.; Massuger, L.; Bekkers, R.; Galaal, K. The impact of BMI on surgical complications and outcomes in endometrial cancer surgery--an institutional study and systematic review of the literature. Gynecol. Oncol. 2015, 139, 369–376. [Google Scholar] [CrossRef]
- Wu, X.S.; Wu, W.G.; Li, M.L.; Yang, J.H.; Ding, Q.C.; Zhang, L.; Mu, J.S.; Gu, J.; Dong, P.; Lu, J.H.; et al. Impact of being overweight on the surgical outcomes of patients with gastric cancer: A meta-analysis. World J. Gastroenterol. 2013, 19, 4596–4606. [Google Scholar] [CrossRef]
- Brewster, A.M.; Etzel, C.; Zhou, R.; Wong, Y.; Edge, S.; Blayney, D.W.; Wilson, J.; Hudis, C.; Ottesen, R.; Hughes, M.E.; et al. The impact of obesity on receipt of adjuvant chemotherapy for breast cancer in the National Comprehensive Cancer Network (NCCN) centers. Breast Cancer Res. Treat. 2011, 130, 897–904. [Google Scholar] [CrossRef] [Green Version]
- Brennan, M.E.; Spillane, A.J. Uptake and predictors of post-mastectomy reconstruction in women with breast malignancy—Systematic review. Eur. J. Surg. Oncol. 2013, 39, 527–541. [Google Scholar] [CrossRef]
- Au-Yeung, G.; Webb, P.M.; DeFazio, A.; Fereday, S.; Bressel, M.; Mileshkin, L. Impact of obesity on chemotherapy dosing for women with advanced stage serous ovarian cancer in the Australian Ovarian Cancer Study (AOCS). Gynecol. Oncol. 2014, 133, 16–22. [Google Scholar] [CrossRef]
- Chambers, P.; Daniels, S.H.; Thompson, L.C.; Stephens, R.J. Chemotherapy dose reductions in obese patients with colorectal cancer. Ann. Oncol. 2012, 23, 748–753. [Google Scholar] [CrossRef]
- Gennari, A.; Amadori, D.; Scarpi, E.; Farolfi, A.; Paradiso, A.; Mangia, A.; Biglia, N.; Gianni, L.; Tienghi, A.; Rocca, A.; et al. Impact of body mass index (BMI) on the prognosis of high-risk early breast cancer (EBC) patients treated with adjuvant chemotherapy. Breast Cancer Res. Treat. 2016, 159, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Budman, D.R.; Berry, D.A.; Cirrincione, C.T.; Henderson, I.C.; Wood, W.C.; Weiss, R.B.; Ferree, C.R.; Muss, H.B.; Green, M.R.; Norton, L.; et al. Dose and dose intensity as determinants of outcome in the adjuvant treatment of breast cancer. The Cancer and Leukemia Group B. J. Natl. Cancer Inst. 1998, 90, 1205–1211. [Google Scholar] [CrossRef] [Green Version]
- Wildiers, H.; Reiser, M. Relative dose intensity of chemotherapy and its impact on outcomes in patients with early breast cancer or aggressive lymphoma. Crit. Rev. Oncol. Hematol. 2011, 77, 221–240. [Google Scholar] [CrossRef]
- Griggs, J.J.; Mangu, P.B.; Temin, S.; Lyman, G.H. Appropriate Chemotherapy Dosing for Obese Adult Patients With Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Oncol. Pract. 2012, 8, e59–e61. [Google Scholar] [CrossRef]
- Reddy, S.M.; Sadim, M.; Li, J.; Yi, N.; Agarwal, S.; Mantzoros, C.S.; Kaklamani, V.G. Clinical and genetic predictors of weight gain in patients diagnosed with breast cancer. Br. J. Cancer 2013, 109, 872–881. [Google Scholar] [CrossRef] [Green Version]
- Caan, B.J.; Kwan, M.L.; Shu, X.O.; Pierce, J.P.; Patterson, R.E.; Nechuta, S.J.; Poole, E.M.; Kroenke, C.H.; Weltzien, E.K.; Flatt, S.W.; et al. Weight change and survival after breast cancer in the after breast cancer pooling project. Cancer Epidemiol. Biomarkers Prev. 2012, 21, 1260–1271. [Google Scholar] [CrossRef] [Green Version]
- Alamuddin, N.; Bakizada, Z.; Wadden, T.A. Management of Obesity. J. Clin. Oncol. 2016, 34, 4295–4305. [Google Scholar] [CrossRef]
- Moore, S.C.; Lee, I.M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; Berrington de Gonzalez, A.; Hartge, P.; et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef]
- McTiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Med. Sci. Sport. Exerc. 2019, 51, 1252–1261. [Google Scholar] [CrossRef]
- Lee, I.M.; Djoussé, L.; Sesso, H.D.; Wang, L.; Buring, J.E. Physical activity and weight gain prevention. JAMA 2010, 303, 1173–1179. [Google Scholar] [CrossRef] [Green Version]
- van Gemert, W.A.; Schuit, A.J.; van der Palen, J.; May, A.M.; Iestra, J.A.; Wittink, H.; Peeters, P.H.; Monninkhof, E.M. Effect of weight loss, with or without exercise, on body composition and sex hormones in postmenopausal women: The SHAPE-2 trial. Breast Cancer Res. 2015, 17, 120. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.L.; Foster-Schubert, K.E.; Alfano, C.M.; Wang, C.C.; Wang, C.Y.; Duggan, C.R.; Mason, C.; Imayama, I.; Kong, A.; Xiao, L.; et al. Reduced-calorie dietary weight loss, exercise, and sex hormones in postmenopausal women: Randomized controlled trial. J. Clin. Oncol. 2012, 30, 2314–2326. [Google Scholar] [CrossRef]
- Foster-Schubert, K.E.; Alfano, C.M.; Duggan, C.R.; Xiao, L.; Campbell, K.L.; Kong, A.; Bain, C.E.; Wang, C.Y.; Blackburn, G.L.; McTiernan, A. Effect of diet and exercise, alone or combined, on weight and body composition in overweight-to-obese postmenopausal women. Obesity 2012, 20, 1628–1638. [Google Scholar] [CrossRef] [Green Version]
- Imayama, I.; Ulrich, C.M.; Alfano, C.M.; Wang, C.; Xiao, L.; Wener, M.H.; Campbell, K.L.; Duggan, C.; Foster-Schubert, K.E.; Kong, A.; et al. Effects of a caloric restriction weight loss diet and exercise on inflammatory biomarkers in overweight/obese postmenopausal women: A randomized controlled trial. Cancer Res. 2012, 72, 2314–2326. [Google Scholar] [CrossRef] [Green Version]
- Mason, C.; Foster-Schubert, K.E.; Imayama, I.; Kong, A.; Xiao, L.; Bain, C.; Campbell, K.L.; Wang, C.Y.; Duggan, C.R.; Ulrich, C.M.; et al. Dietary weight loss and exercise effects on insulin resistance in postmenopausal women. Am. J. Prev. Med. 2011, 41, 366–375. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Bohlke, K.; May, A.M.; Clinton, S.K.; Demark-Wahnefried, W.; Gilchrist, S.C.; Irwin, M.L.; Late, M.; Mansfield, S.; Marshall, T.F.; et al. Exercise, Diet, and Weight Management During Cancer Treatment: ASCO Guideline. J. Clin. Oncol. 2022, 40, 2491–2507. [Google Scholar] [CrossRef]
- Denlinger, C.S.; Ligibel, J.A.; Are, M.; Baker, K.S.; Demark-Wahnefried, W.; Dizon, D.; Friedman, D.L.; Goldman, M.; Jones, L.; National Comprehensive Cancer Network; et al. Survivorship: Nutrition and weight management, Version 2.2014. Clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2014, 12, 1396–1406. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, H.; Bradhurst, P.; Ma, L.X.; Tan, S.Y.C.; Egger, S.J.; Vardy, J.L. Body weight management in overweight and obese breast cancer survivors. Cochrane Database Syst. Rev. 2020, 12, CD012110. [Google Scholar]
- Sacks, F.M.; Bray, G.A.; Carey, V.J.; Smith, S.R.; Ryan, D.H.; Anton, S.D.; McManus, K.; Champagne, C.M.; Bishop, L.M.; Laranjo, N.; et al. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. N. Engl. J. Med. 2009, 360, 859–873. [Google Scholar] [CrossRef]
- Foster, G.D.; Wyatt, H.R.; Hill, J.O.; Makris, A.P.; Rosenbaum, D.L.; Brill, C.; Stein, R.I.; Mohammed, B.S.; Miller, B.; Rader, D.J.; et al. Weight and metabolic outcomes after 2 years on a low-carbohydrate versus low-fat diet: A randomized trial. Ann. Intern. Med. 2010, 153, 147–157. [Google Scholar] [CrossRef]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Bruno, E.; Krogh, V.; Gargano, G.; Grioni, S.; Bellegotti, M.; Venturelli, E.; Panico, S.; Santucci de Magistris, M.; Bonanni, B.; Zagallo, E.; et al. Adherence to Dietary Recommendations after One Year of Intervention in Breast Cancer Women: The DIANA-5 Trial. Nutrients 2021, 13, 2990. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Obesity Society. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129 (Suppl. S25), S102–S138. [Google Scholar]
- Barry, V.W.; Baruth, M.; Beets, M.W.; Durstine, J.L.; Liu, J.; Blair, S.N. Fitness vs. fatness on all-cause mortality: A meta-analysis. Prog. Cardiovasc. Dis. 2014, 56, 382–390. [Google Scholar] [CrossRef]
- Gaesser, G.A.; Angadi, S.S.; Sawyer, B.J. Exercise and diet, independent of weight loss, improve cardiometabolic risk profile in overweight and obese individuals. Phys. Sportsmed. 2011, 39, 87–97. [Google Scholar] [CrossRef]
- Rack, B.; Andergassen, U.; Neugebauer, J.; Salmen, J.; Hepp, P.; Sommer, H.; Lichtenegger, W.; Friese, K.; Beckmann, M.W.; Hauner, D.; et al. The German SUCCESS C Study—The First European Lifestyle Study on Breast Cancer. Breast Care 2010, 5, 395–400. [Google Scholar] [CrossRef] [Green Version]
- Janni, W.; Rack, B.; Friedl, T.; Müller, V.; Lorenz, R.; Rezai, M.; Tesch, H.; Heinrich, G.; Andergassen, U.; Harbeck, N. Abstract GS5-03. lifestyle intervention and effect on disease-free survival in early breast cancer pts: Interim analysis from the randomized SUCCESS C study. Cancer Res. 2019, 79, GS5-03. [Google Scholar] [CrossRef]
- Egan, A.G.; Blind, E.; Dunder, K.; de Graeff, P.A.; Hummer, B.T.; Bourcier, T.; Rosebraugh, C. Pancreatic safety of incretin-based drugs--FDA and EMA assessment. N. Engl. J. Med. 2014, 370, 794–797. [Google Scholar] [CrossRef] [Green Version]
- Bjerre Knudsen, L.; Madsen, L.W.; Andersen, S.; Almholt, K.; de Boer, A.S.; Drucker, D.J.; Gotfredsen, C.; Egerod, F.L.; Hegelund, A.C.; Jacobsen, H.; et al. Glucagon-like Peptide-1 receptor agonists activate rodent thyroid C-cells causing calcitonin release and C-cell proliferation. Endocrinology 2010, 151, 1473–1486. [Google Scholar] [CrossRef] [Green Version]
- Nomiyama, T.; Kawanami, T.; Irie, S.; Hamaguchi, Y.; Terawaki, Y.; Murase, K.; Tsutsumi, Y.; Nagaishi, R.; Tanabe, M.; Morinaga, H.; et al. Exendin-4, a GLP-1 receptor agonist, attenuates prostate cancer growth. Diabetes 2014, 63, 3891–3905. [Google Scholar] [CrossRef]
- Iwaya, C.; Nomiyama, T.; Komatsu, S.; Kawanami, T.; Tsutsumi, Y.; Hamaguchi, Y.; Horikawa, T.; Yoshinaga, Y.; Yamashita, S.; Tanaka, T.; et al. Exendin-4, a glucagonlike peptide-1 receptor agonist, attenuates breast cancer growth by inhibiting NF-κB activation. Endocrinology 2017, 158, 4218–4232. [Google Scholar] [CrossRef] [Green Version]
- Ligumsky, H.; Wolf, I.; Israeli, S.; Haimsohn, M.; Ferber, S.; Karasik, A.; Kaufman, B.; Rubinek, T. The peptide-hormone glucagon-like peptide-1 activates cAMP and inhibits growth of breast cancer cells. Breast Cancer Res. Treat. 2012, 132, 449–461. [Google Scholar] [CrossRef]
- Yanovski, S.Z.; Yanovski, J.A. Long-term drug treatment for obesity: A systematic and clinical review. JAMA 2014, 311, 74–86. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, B.M.; Kvach, E.; Eckel, R.H. Treatment of Obesity: Weight Loss and Bariatric Surgery. Circ. Res. 2016, 118, 1844–1855. [Google Scholar] [CrossRef]
- Albaugh, V.L.; Abumrad, N.N. Surgical treatment of obesity. Eur. J. Endocrinol. 2018, 158, 135–145. [Google Scholar] [CrossRef] [Green Version]
- Nudel, J.; Sanchez, V.M. Surgical management of obesity. Metab. Clin. Exp. 2019, 92, 206–216. [Google Scholar] [CrossRef]
- Philip, E.J.; Torghabeh, M.H.; Strain, G.W. Bariatric surgery in cancer survivorship: Does a history of cancer affect weight loss outcomes? Surg. Obes. Relat. Dis. 2015, 11, 1105–1108. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, L.M.S.; Sjöholm, K.; Jacobson, P.; Andersson-Assarsson, J.C.; Svensson, P.A.; Taube, M.; Carlsson, B.; Peltonen, M. Life Expectancy after Bariatric Surgery in the Swedish Obese Subjects Study. N. Engl. J. Med. 2020, 383, 1535–1543. [Google Scholar] [CrossRef]
- Tee, M.C.; Cao, Y.; Warnock, G.L.; Hu, F.B.; Chavarro, J.E. Effect of bariatric surgery on oncologic outcomes: A systematic review and meta-analysis. Surg. Endosc. 2013, 27, 4449–4456. [Google Scholar] [CrossRef] [Green Version]
- Adams, T.D.; Hunt, S.C. Cancer and obesity: Effect of bariatric surgery. World J. Surg. 2009, 33, 2028–2033. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Barry, W.T.; Alfano, C.; Hershman, D.L.; Irwin, M.; Neuhouser, M.; Thomson, C.A.; Delahanty, L.; Frank, E.; Spears, P.; et al. Randomized phase III trial evaluating the role of weight loss in adjuvant treatment of overweight and obese women with early breast cancer (Alliance A011401): Study design. NPJ Breast Cancer 2017, 3, 37. [Google Scholar] [CrossRef] [Green Version]
- Thomson, C.A.; Crane, T.E.; Miller, A.; Garcia, D.O.; Basen-Engquist, K.; Alberts, D.S. A randomized trial of diet and physical activity in women treated for stage II-IV ovarian cancer: Rationale and design of the Lifestyle Intervention for Ovarian Cancer Enhanced Survival (LIVES): An NRG Oncology/Gynecologic Oncology Group (GOG-225) Study. Contemp. Clin. Trials 2016, 49, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Courneya, K.S.; Vardy, J.L.; O’Callaghan, C.J.; Friedenreich, C.M.; Campbell, K.L.; Prapavessis, H.; Crawford, J.J.; O’Brien, P.; Dhillon, H.M.; Jonker, D.J.; et al. Effects of a Structured Exercise Program on Physical Activity and Fitness in Colon Cancer Survivors: One Year Feasibility Results from the CHALLENGE Trial. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Newton, R.U.; Galvão, D.A. Accumulating Evidence for Physical Activity and Prostate Cancer Survival: Time for a Definitive Trial of Exercise Medicine? Eur. Urol. 2016, 70, 586–587. [Google Scholar] [CrossRef]


| Methods | Technical Principles | Potential Benefit and Drawbacks |
|---|---|---|
| Anthropometric measurement | Manual measurement of weight to height ratio (Body mass index), waist–hip ratio, waist circumference, arm circumference, skinfold thickness, etc. | Low cost and easy to measure but are not fully accurate or validated in different ethnicities |
| Dual energy X-ray absorptiometry (DEXA) | Generates X-rays at two different energies and uses differential attenuation of the X-ray beam at two energies to measure body composition including fat, fat free mass, and bone mineral density | Highly accurate, relatively low cost, and able to assess whole body but associated with low radiation exposure |
| Ultrasound | Reflection of ultrasound waves from tissue in the path of the beam | Highly accurate, no radiation exposure, but user-dependent and lack of standardization |
| Computed tomography (CT) scan | Uses X-ray beam and special digital X-ray detectors for generation of cross-sectional imaging with volumetric reconstruction of body adipose tissue and other tissues | Highly accurate and able to assess whole body but with greater radiation exposure and higher cost |
| Magnetic resonance imaging (MRI) | Employ powerful magnets, which produce a strong magnetic field that forces protons in the body to align with that field and generate cross-sectional imaging with volumetric reconstruction on the basis of different magnetic properties of water and fat | Provides better soft tissue contrast than other imaging studies and differentiates between fat, water, and muscle better; is able to assess the whole body but has a higher cost, limited access and longer scan times compared with CT and ultrasound |
| Bioelectrical impedance | Based on the principle that electric current flows at different rates through the body depending upon its composition | Low cost but limited accuracy |
| Type of Cancer | Number of Cohorts | Relative Risk (95% Confidence Interval) | |
|---|---|---|---|
| Women | Men | ||
| Endometrial cancer [4] | 19 | 1.59 (1.50–1.68) | NA |
| Gallbladder cancer [4] | 4 | 1.59 (1.02–2.47) | 1.09 (0.99–1.21) |
| Esophageal adenocarcinoma [4] | 5 | 1.51 (1.31–1.74) | 1.52 (1.33–1.74) |
| Kidney cancer [4] | 12 | 1.34 (1.25–1.43) | 1.24 (1.15–1.34) |
| Postmenopausal breast cancer [4] | 34 | 1.12 (1.08–1.16) | NA |
| Hpatocellular cancer [19] | 9 | 1.12 (1.03–1.22) | 1.19 (1.09–1.29) |
| Pancreatic adenocarcinoma [23] | 23 | 1.10 (1.04–1.16) | 1.13 (1.04–1.22) |
| Colon cancer [4] | 29 | 1.09 (1.05–1.13) | 1.24 (1.20–1.28) |
| Ovarian cancer [77] | 34 | 1.06 (1.00–1.12) | NA |
| Stomach cancer [4] | 8 | 1.04 (0.90–1.20) | 0.97 (0.88–1.06) |
| Rectal cancer [4] | 29 | 1.02 (1.00–1.05) | 1.09 (1.06–1.12) |
| Later stage prostate cancer [73] | 23 | NA | 1.08 (1.04–1.12) |
| Type of Cancer [27] | Number of Cohorts | Overall Survival (HR, 95%CI) | Number of Cohorts | Cancer-Specific Survival (HR, 95%CI) |
|---|---|---|---|---|
| Breast | 59 | 1.26 (1.20–1.33) | 36 | 1.23 (1.15–1.32) |
| Colorectal cancer | 30 | 1.22 (1.14–1.31) | 13 | 1.24 (1.16–1.33) |
| Pancreas | 6 | 1.36 (0.95–1.93) | 3 | 1.28 (1.05–1.57) |
| Endometrial cancer | 12 | 1.20 (1.04–1.38) | 6 | 1.02 (0.75–1.39) |
| Prostate cancer | 12 | 1.07 (0.91–1.25) | 15 | 1.26 (1.08–1.47) |
| Gastroesophageal cancer | 7 | 1.08 (0.77–1.52) | 2 | 0.83 (0.58–1.16) |
| Bladder cancer | 3 | 1.08 (0.98–1.20) | 3 | 1.36 (0.96–1.93) |
| Hepatobiliary cancer | 5 | 1.06 (0.89–1.25) | 1 | 0.79 (0.50–1.24) |
| Ovarian cancer | 4 | 1.03 (0.75–1.41) | 4 | 1.06 (0.82–1.37) |
| Registration Number | Phase | Title of the Study |
|---|---|---|
| NCT02750826 | Phase III | Breast Cancer Weight Loss Study (BWEL Study) |
| NCT00719303 | Phase III | Diet and Physical Activity Change or Usual Care in Improving Progression-Free Survival in Patients With Previously Treated Stage II, III, or IV Ovarian, Fallopian Tube, or Primary Peritoneal Cancer |
| NCT04447313 | Phase III | Telephone Delivered Weight Loss, Nutrition, Exercise WeLNES Study |
| NCT05316467 | Phase II/III | Weight Management Plus Megestrol Acetate in Early-stage Endometrioid Carcinoma |
| NCT00819208 | Phase III | A Phase III Study of the Impact of a Physical Activity Program on Disease-Free Survival in Patients with High Risk Stage II or Stage III Colon Cancer: A Randomized Controlled Trial (CHALLENGE) |
| NCT04861220 | Phase II/III | Surgical Pre-habilitation in Breast Cancer |
| NCT02730338 | Phase III | INTense ExeRcise for surviVAL Among Men With Metastatic Prostate Cancer (INTERVAL-GAP4) (INTERVAL) |
| NCT04298086 | Phase II | A Study of the Body’s Response to Exercise and a Plant-Based Diet in Overweight Postmenopausal Women With Breast Cancer |
| NCT04499950 | Phase II | Adaptive Nutrition and Exercise Weight Loss (A-NEW) Study |
| NCT04931017 | Phase II | Metformin for Chemoprevention of Lung Cancer in Overweight or Obese Individuals at High Risk for Lung Cancer |
| NCT05082519 | Phase II | Caloric Restriction and Activity to Reduce Chemoresistance in B-ALL |
| NCT04717050 | Phase II | Reducing Metabolic Dysregulation in Obese Latina Breast Cancer Survivors Using Physical Activity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pati, S.; Irfan, W.; Jameel, A.; Ahmed, S.; Shahid, R.K. Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management. Cancers 2023, 15, 485. https://doi.org/10.3390/cancers15020485
Pati S, Irfan W, Jameel A, Ahmed S, Shahid RK. Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management. Cancers. 2023; 15(2):485. https://doi.org/10.3390/cancers15020485
Chicago/Turabian StylePati, Sukanya, Wadeed Irfan, Ahmad Jameel, Shahid Ahmed, and Rabia K. Shahid. 2023. "Obesity and Cancer: A Current Overview of Epidemiology, Pathogenesis, Outcomes, and Management" Cancers 15, no. 2: 485. https://doi.org/10.3390/cancers15020485