
The Use of Artificial Intelligence (AI) in the Radiology Field: What Is the State of Doctor–Patient Communication in Cancer Diagnosis?

 , ,
, ,  ,
,  , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
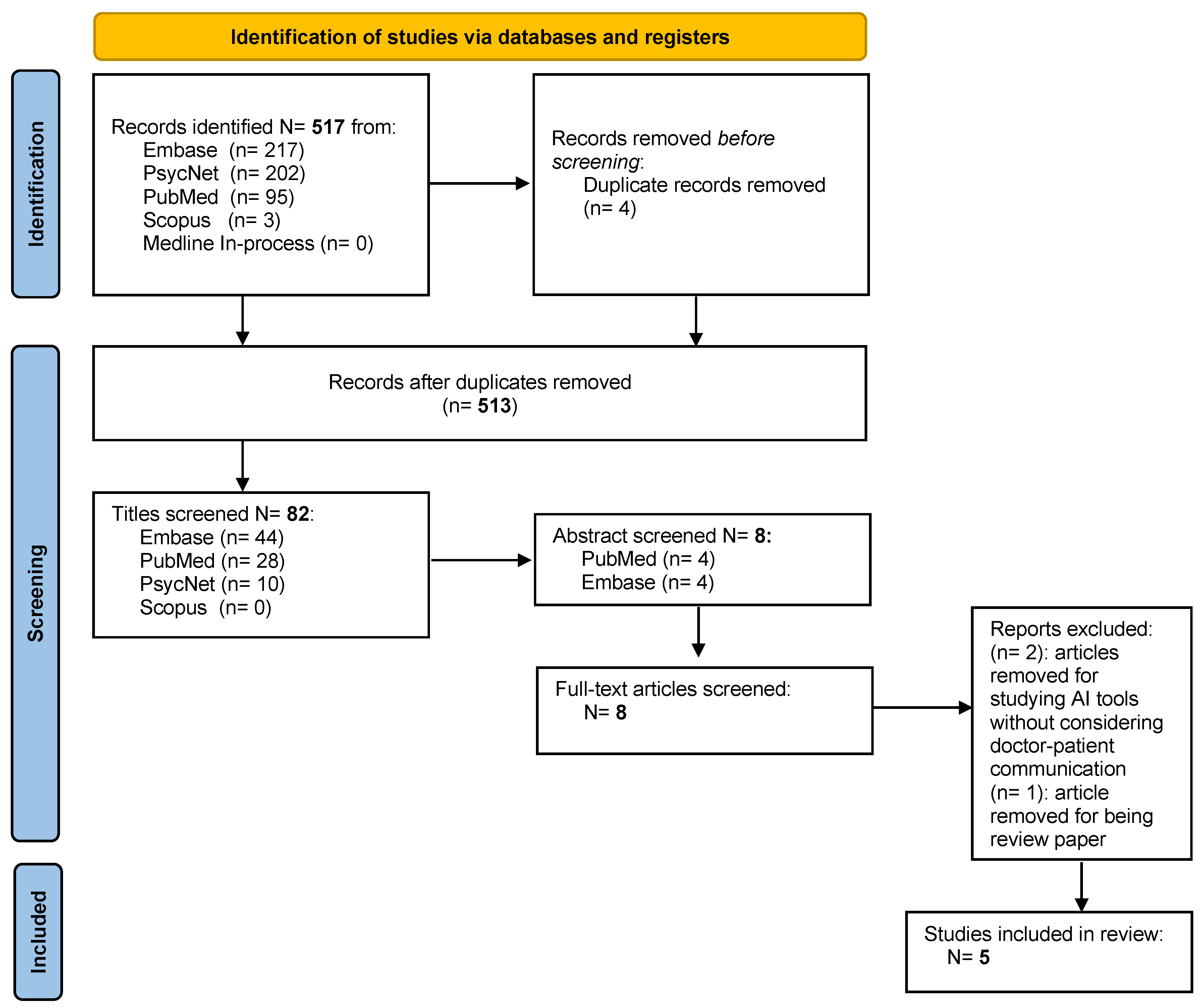
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Screening and Data Extraction
3. Results
3.1. Features of the Studies
3.2. Synthesis of the Results
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Title | URL | Resource | Type | Identifiers | Db |
|---|---|---|---|---|---|
| (1) Workflow Applications of Artificial Intelligence in Radiology and an Overview of Available Tools | doi.org/10.1016/j.jacr.2020.08.016 | PubMed | Narrative review | PMID: 33153540 | MeSH-PubMed |
| (2) Artificial Intelligence in Breast Imaging: Potentials and Limitations | doi.org/10.2214/AJR.18.20532 | PubMed | Narrative review | PMID: 30422715 | MeSH-PubMed |
| (3) Patient Perspectives and Priorities Regarding Artificial Intelligence in Radiology: Opportunities for Patient-Centered Radiology | doi.org/10.1016/j.jacr.2020.01.007 | PubMed | Qualitative | PMID: 32068006 | MeSH-PubMed |
| (4) The ethical, legal and social implications of using artificial intelligence systems in breast cancer care | doi.org/10.1016/j.breast.2019.10.001 | PubMed | Narrative review | PMID: 31677530 | MeSH-PubMed |
| (5) Artificial intelligence in screening mammography: A population Survey of Women’s Preferences | doi.org/10.1016/j.jacr.2020.09.042 | PubMed | Longitudinal study | PMID: 33058789 | MeSH-PubMed |
References
- Park, S.H.; Han, K. Methodologic Guide for Evaluating Clinical Performance and Effect of Artificial Intelligence Technology for Medical Diagnosis and Prediction. Radiology 2018, 286, 800–809. [Google Scholar] [CrossRef]
- Martín Noguerol, T.; Paulano-Godino, F.; Martín-Valdivia, M.T.; Menias, C.O.; Luna, A. Strengths, Weaknesses, Opportunities, and Threats Analysis of Artificial Intelligence and Machine Learning Applications in Radiology. J. Am. Coll. Radiol. 2019, 16, 1239–1247. [Google Scholar] [CrossRef]
- Lee, J.G.; Jun, S.; Cho, Y.W.; Lee, H.; Kim, G.B.; Seo, J.B.; Kim, N. Deep Learning in Medical Imaging: General Overview. Korean J. Radiol. 2017, 18, 570. [Google Scholar] [CrossRef] [Green Version]
- King, B.F. Guest Editorial: Discovery and Artificial Intelligence. Am. J. Roentgenol. 2017, 209, 1189–1190. [Google Scholar] [CrossRef]
- King, B.F. Artificial Intelligence and Radiology: What Will the Future Hold? J. Am. Coll. Radiol. 2018, 15, 501–503. [Google Scholar] [CrossRef]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J. Artificial Intelligence in Radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef]
- Google Says Its AI Can Spot Early-Stage Lung Cancer, in Some Cases Better Than Doctors Can—GeekWire. Available online: https://www.geekwire.com/2019/google-says-ai-can-spot-early-stage-lung-cancer-cases-better-doctors-can/ (accessed on 30 November 2022).
- AI Is Better at Diagnosing Skin Cancer Than Your Doctor, Study Finds. Available online: https://finance.yahoo.com/news/ai-better-diagnosing-skin-cancer-182057234.html?guccounter=1&guce_referrer=aHR0cHM6Ly93d3cuZ29vZ2xlLmNvbS8&guce_referrer_sig=AQAAANisvvSAdl5qYPcgGM6vghzJGoKDCILKb6ZGRYgyzSFEVWdkC4mwZBAxDq42fxoiV3IZEMfLzba8QgjRa2ifcPPF1ln8Lp2GKLxl-pW3muUc2iFRx4jHSPbe9_6AFiy16Ng_oRQlxR-gbT9ShXuKomPU5CN_DzKo7FscfW6YsGNv (accessed on 30 November 2022).
- Pesapane, F.; Codari, M.; Sardanelli, F. Artificial Intelligence in Medical Imaging: Threat or Opportunity? Radiologists Again at the Forefront of Innovation in Medicine. Eur. Radiol. Exp. 2018, 2, 35. [Google Scholar] [CrossRef] [Green Version]
- Neri, E.; de Souza, N.; Brady, A.; Bayarri, A.A.; Becker, C.D.; Coppola, F.; Visser, J. What the Radiologist Should Know about Artificial Intelligence—An ESR White Paper. Insights Imaging 2019, 10, 1–8. [Google Scholar] [CrossRef]
- Neisser, U.; Becklen, R. Selective Looking: Attending to Visually Specified Events. Cogn. Psychol. 1975, 7, 480–494. [Google Scholar] [CrossRef]
- Carrigan, A.J.; Wardle, S.G.; Rich, A.N. Finding Cancer in Mammograms: If You Know It’s There, Do You Know Where? Cogn. Res. Princ. Implic. 2018, 3, 1–14. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, J.W.; Muntinga, T.; Grigg, S.; Ioannidis, J.P.A. Prevalence and Outcomes of Incidental Imaging Findings: Umbrella Review. BMJ 2018, 361, k2387. [Google Scholar] [CrossRef] [Green Version]
- Sarwar, S.; Dent, A.; Faust, K.; Richer, M.; Djuric, U.; van Ommeren, R.; Diamandis, P. Physician Perspectives on Integration of Artificial Intelligence into Diagnostic Pathology. NPJ Digit. Med. 2019, 2, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haenssle, H.A.; Fink, C.; Schneiderbauer, R.; Toberer, F.; Buhl, T.; Blum, A.; Kalloo, A.; ben Hadj Hassen, A.; Thomas, L.; Enk, A.; et al. Man against Machine: Diagnostic Performance of a Deep Learning Convolutional Neural Network for Dermoscopic Melanoma Recognition in Comparison to 58 Dermatologists. Ann. Oncol. 2018, 29, 1836–1842. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.J.; Bang, C.S.; Park, S.W.; Yang, Y.J.; Seo, S.I.; Lim, H.; Shin, W.G.; Hong, J.T.; Yoo, Y.T.; Hong, S.H.; et al. Automated Classification of Gastric Neoplasms in Endoscopic Images Using a Convolutional Neural Network. Endoscopy 2019, 51, 1121–1129. [Google Scholar] [CrossRef]
- Astley, S.M.; Harkness, E.F.; Sergeant, J.C.; Warwick, J.; Stavrinos, P.; Warren, R.; Wilson, M.; Beetles, U.; Gadde, S.; Lim, Y.; et al. A Comparison of Five Methods of Measuring Mammographic Density: A Case-Control Study. Breast Cancer Res. 2018, 20, 10. [Google Scholar] [CrossRef]
- French, D.P.; Astley, S.; Astley, S.; Brentnall, A.R.; Cuzick, J.; Dobrashian, R.; Duffy, S.W.; Gorman, L.S.; Gorman, L.S.; Harkness, E.F.; et al. What Are the Benefits and Harms of Risk Stratified Screening as Part of the NHS Breast Screening Programme? Study Protocol for a Multi-Site Non-Randomised Comparison of BC-Predict versus Usual Screening (NCT04359420). BMC Cancer 2020, 20, 570. [Google Scholar] [CrossRef]
- Aerts, H.J.W.L. Data Science in Radiology: A Path Forward. Clin. Cancer Res. 2018, 24, 532. [Google Scholar] [CrossRef] [Green Version]
- Alshamrani, K.; Offiah, A.C. Applicability of Two Commonly Used Bone Age Assessment Methods to Twenty-First Century UK Children. Eur. Radiol. 2020, 30, 504. [Google Scholar] [CrossRef] [Green Version]
- Chilamkurthy, S.; Ghosh, R.; Tanamala, S.; Biviji, M.; Campeau, N.G.; Venugopal, V.K.; Mahajan, V.; Rao, P.; Warier, P. Deep Learning Algorithms for Detection of Critical Findings in Head CT Scans: A Retrospective Study. Lancet 2018, 392, 2388–2396. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Ruiz, A.; Lång, K.; Gubern-Merida, A.; Broeders, M.; Gennaro, G.; Clauser, P.; Helbich, T.H.; Chevalier, M.; Tan, T.; Mertelmeier, T.; et al. Stand-Alone Artificial Intelligence for Breast Cancer Detection in Mammography: Comparison With 101 Radiologists. J. Natl. Cancer Inst. 2019, 111, 916–922. [Google Scholar] [CrossRef]
- Codari, M.; Melazzini, L.; Morozov, S.P.; van Kuijk, C.C.; Sconfienza, L.M.; Sardanelli, F. Impact of Artificial Intelligence on Radiology: A EuroAIM Survey among Members of the European Society of Radiology. Insights Imaging 2019, 10, 105. [Google Scholar] [CrossRef] [Green Version]
- Hamon, R.; Junklewitz, H.; Sanchez, I.; European Commission. Joint Research Centre. Robustness and Explainability of Artificial Intelligence; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar] [CrossRef]
- Zanca, F.; Brusasco, C.; Pesapane, F.; Kwade, Z.; Beckers, R.; Avanzo, M. Regulatory Aspects of the Use of Artificial Intelligence Medical Software. Semin. Radiat. Oncol. 2022, 32, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, A.; Díaz-Rodríguez, N.; Del Ser, J.; Bennetot, A.; Tabik, S.; Barbado, A.; García, S.; Gil-López, S.; Molina, D.; Benjamins, R.; et al. Explainable Artificial Intelligence (XAI): Concepts, Taxonomies, Opportunities and Challenges toward Responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef] [Green Version]
- Cortes, C.; Vapnik, V.; Saitta, L. Support-Vector Networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Fan, W.; Liu, J.; Zhu, S.; Pardalos, P.M. Investigating the Impacting Factors for the Healthcare Professionals to Adopt Artificial Intelligence-Based Medical Diagnosis Support System (AIMDSS). Ann. Oper. Res. 2020, 294, 567–592. [Google Scholar] [CrossRef]
- Pesapane, F.; Rotili, A.; Valconi, E.; Agazzi, G.M.; Montesano, M.; Penco, S.; Nicosia, L.; Bozzini, A.; Meneghetti, L.; Latronico, A.; et al. Women’s Perceptions and Attitudes to the Use of AI in Breast Cancer Screening: A Survey in a Cancer Referral Centre. Br. J. Radiol. 2022, 95, 20220569. [Google Scholar] [CrossRef]
- Triberti, S.; Durosini, I.; Pravettoni, G. A “Third Wheel” Effect in Health Decision Making Involving Artificial Entities: A Psychological Perspective. Front. Public Health 2020, 8, 117. [Google Scholar] [CrossRef] [PubMed]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-Analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Ongena, Y.P.; Yakar, D.; Haan, M.; Kwee, T.C. Artificial Intelligence in Screening Mammography: A Population Survey of Women’s Preferences. J. Am. Coll. Radiol. 2021, 18, 79–86. [Google Scholar] [CrossRef]
- Adams, S.J.; Tang, R.; Babyn, P. Patient Perspectives and Priorities Regarding Artificial Intelligence in Radiology: Opportunities for Patient-Centered Radiology. J. Am. Coll. Radiol. 2020, 17, 1034–1036. [Google Scholar] [CrossRef] [PubMed]
- Carter, S.M.; Rogers, W.; Win, K.T.; Frazer, H.; Richards, B.; Houssami, N. The Ethical, Legal and Social Implications of Using Artificial Intelligence Systems in Breast Cancer Care. Breast 2020, 49, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Mendelson, E.B. Artificial Intelligence in Breast Imaging: Potentials and Limitations. Am. J. Roentgenol. 2019, 212, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, N.; Lacson, R.; Khorasani, R. Workflow Applications of Artificial Intelligence in Radiology and an Overview of Available Tools. J. Am. Coll. Radiol. 2020, 17, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, S.D.; Dalal, A.K.; Anik Sahni, V.; Lacson, R.; Khorasani, R. Does Integrating Nonurgent, Clinically Significant Radiology Alerts within the Electronic Health Record Impact Closed-Loop Communication and Follow-Up? J. Am. Med. Inform. Assoc. 2016, 23, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haan, M.; Ongena, Y.P.; Hommes, S.; Kwee, T.C.; Yakar, D. A Qualitative Study to Understand Patient Perspective on the Use of Artificial Intelligence in Radiology. J. Am. Coll. Radiol. 2019, 16, 1416–1419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coiera, E. The Fate of Medicine in the Time of AI. Lancet 2018, 392, 2331–2332. [Google Scholar] [CrossRef]
- McCabe, R.; Healey, P.G.T. Miscommunication in Doctor–Patient Communication. Top. Cogn. Sci. 2018, 10, 409–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahuja, A.S. The Impact of Artificial Intelligence in Medicine on the Future Role of the Physician. PeerJ 2019, 7, e7702. [Google Scholar] [CrossRef]

| References | Patient Characteristics | Attitude toward AI | Patient’s Knowledge and Point of View on AI | |||
|---|---|---|---|---|---|---|
| Populations | N | Average Age (SD) | Investigated | Language Population | ||
| Ongena et al., 2020 [32] | Breast cancer screening | 922 | ±45 | Trust Accountability Personal interaction Efficiency The general attitude toward AI | German | Those who have lower education are less supportive of AI Those who think AI is less efficient had a more negative attitude toward AI |
| Adams et al., 2020 [33] | / | 17 | / | Fear of the unknown Trust Human connection Improving communication | English | AI was shaped and viewed as “science fiction” |
| Carter et al., 2019 [34] | Breast cancer | / | / | Ethical Legal Social implications | English | No deep understanding of the way health technologies work |
| Mendelson, 2019 [35] | Breast cancer | / | / | Potentials Limitations | English | Education in AI for patients Empowerment skills in doctor–patient communication |
| Kapoor et al., 2020 [36] | / | / | / | Workflow applications of AI in radiology | English | Closed-loop communication of critical radiology results |
| References | Methods | Analysis | Main Variables |
|---|---|---|---|
| Ongena et al., 2020 [32] | Internet Survey with ad hoc 5-point Likert Scale | Quantitative analysis | Patients’ education levels shape trust and attitudes toward AI (low education is associated with low trust) |
| Adams et al., 2020 [33] | Patient engagement Workshop and interviews | Qualitative analysis (thematic analysis) | Trust is linked to the fear of the unknown uses of AI in radiology and the lack of human connections and empathy |
| Carter et al., 2019 [34] | Narrative review and perspective | Analysis of the ethical issues in doctor–patient communication | Knowledge and understanding of the way AI works are pivotal for the ethical use of AI |
| Mendelson, 2019 [35] | Narrative review and perspective | Analysis of the pros and cons of using AI in breast cancer imaging | Knowledge and education about AI for patients are as important as the empowerment of skills in communication for physicians |
| Kapoor et al., 2020 [36] | Overview of the applications of AI in radiology | Qualitative synthesis | Closed-loop communication to provide improved and personalized feedback for patients |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derevianko, A.; Pizzoli, S.F.M.; Pesapane, F.; Rotili, A.; Monzani, D.; Grasso, R.; Cassano, E.; Pravettoni, G. The Use of Artificial Intelligence (AI) in the Radiology Field: What Is the State of Doctor–Patient Communication in Cancer Diagnosis? Cancers 2023, 15, 470. https://doi.org/10.3390/cancers15020470
Derevianko A, Pizzoli SFM, Pesapane F, Rotili A, Monzani D, Grasso R, Cassano E, Pravettoni G. The Use of Artificial Intelligence (AI) in the Radiology Field: What Is the State of Doctor–Patient Communication in Cancer Diagnosis? Cancers. 2023; 15(2):470. https://doi.org/10.3390/cancers15020470
Chicago/Turabian StyleDerevianko, Alexandra, Silvia Francesca Maria Pizzoli, Filippo Pesapane, Anna Rotili, Dario Monzani, Roberto Grasso, Enrico Cassano, and Gabriella Pravettoni. 2023. "The Use of Artificial Intelligence (AI) in the Radiology Field: What Is the State of Doctor–Patient Communication in Cancer Diagnosis?" Cancers 15, no. 2: 470. https://doi.org/10.3390/cancers15020470