
The Excretion of Cisplatin after Hyperthermic Intrathoracic Chemotherapy

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Surgery and Hyperthermic Intrathoracic Chemotherapy (HITOC)
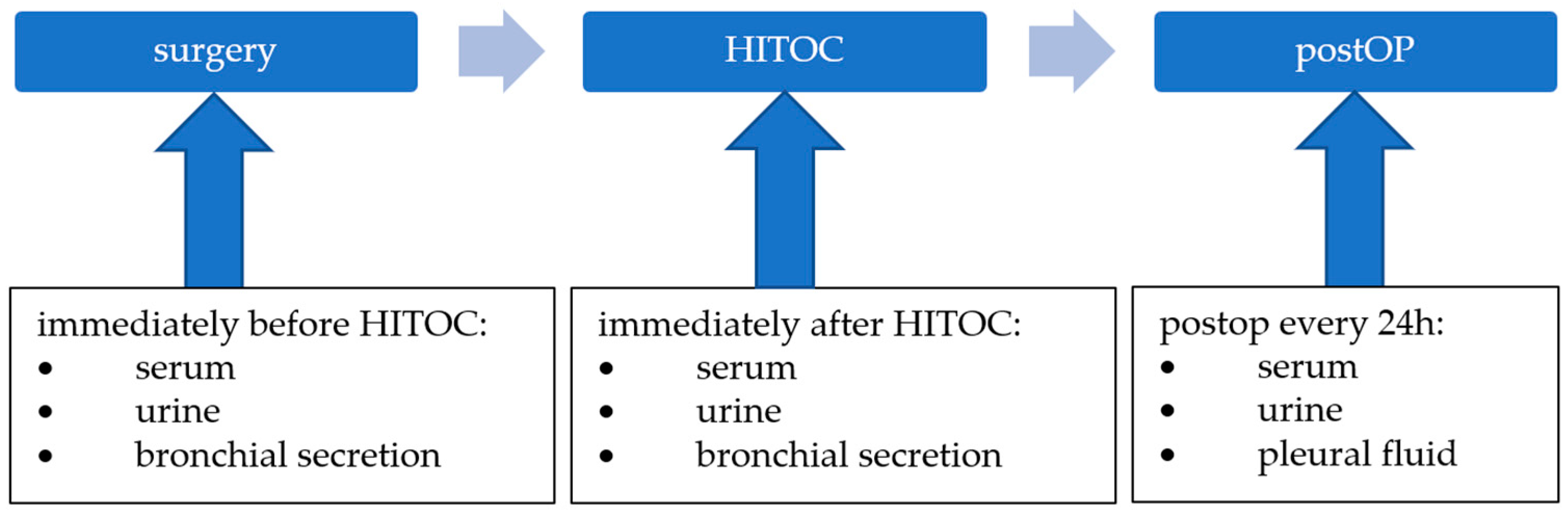
2.3. Sample Collection
2.4. Reagents and Chemicals
2.5. Instrumentation
2.6. Urine Analysis
2.7. Sample Preparation and Analysis
2.8. The Rational of the Measurement of Platinum and Cisplatin
2.9. Statistical Analysis
3. Results
3.1. General Patients’ Data and Overview
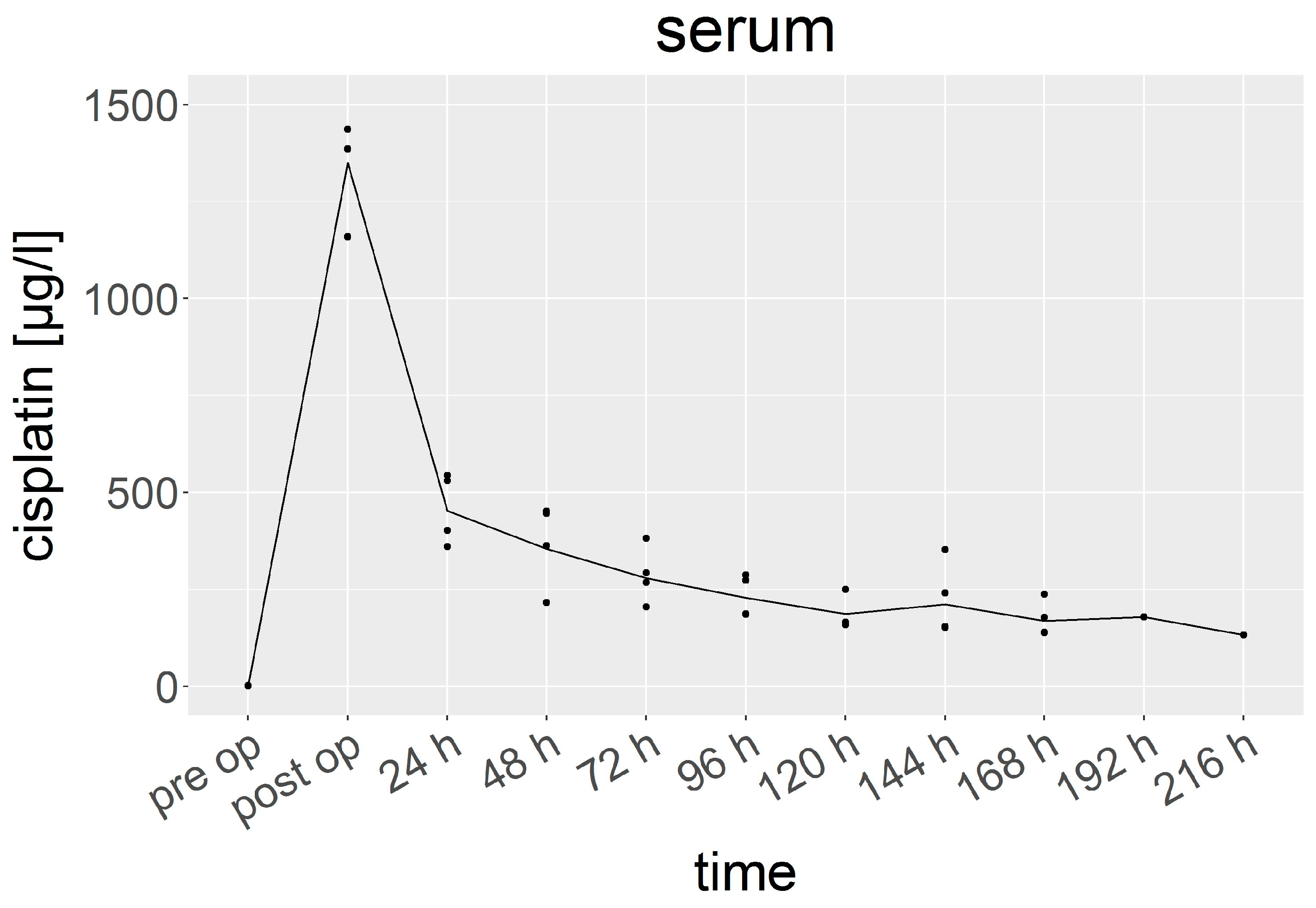
3.2. Cisplatin in Serum
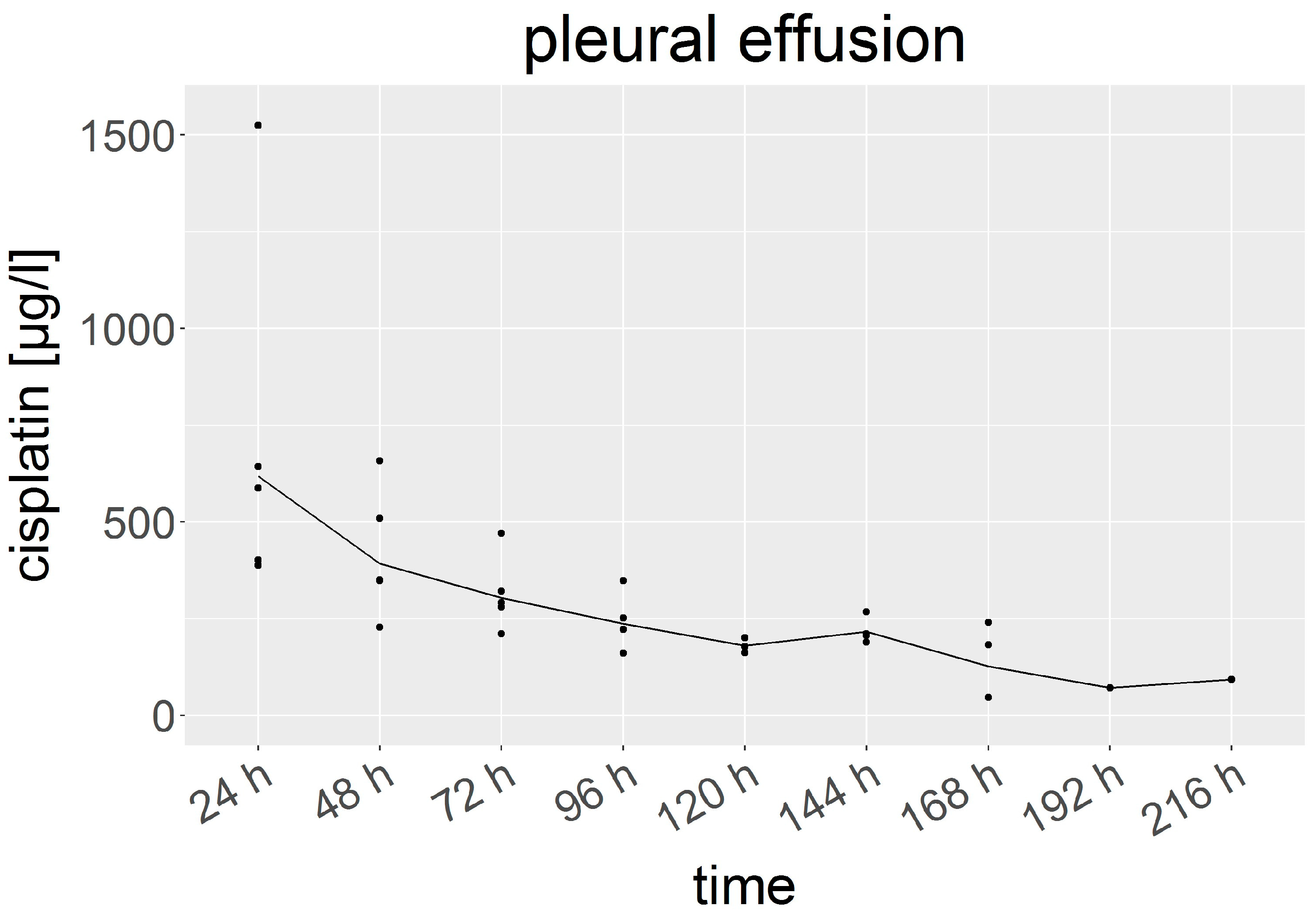
3.3. Cisplatin in Pleural Fluid
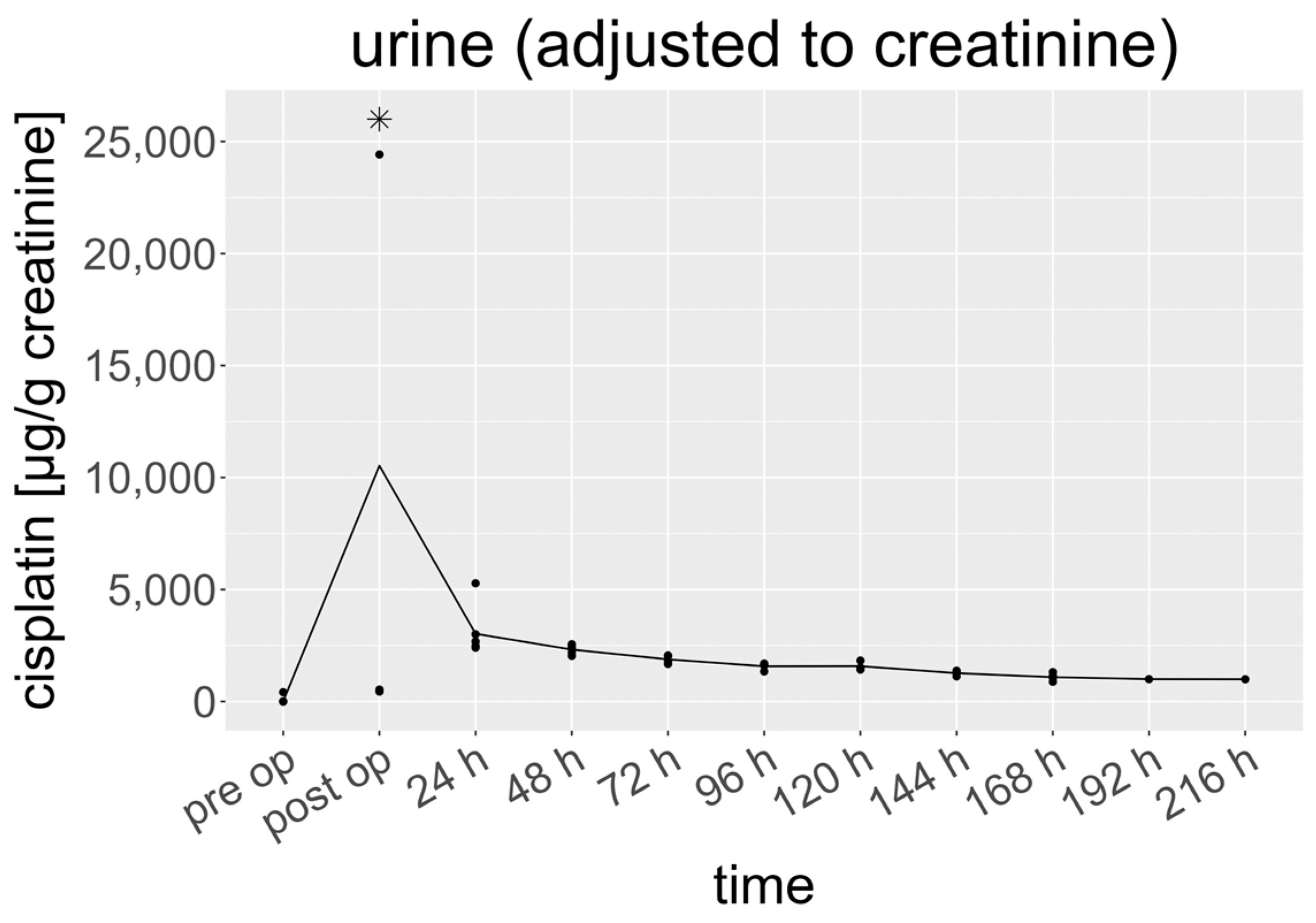
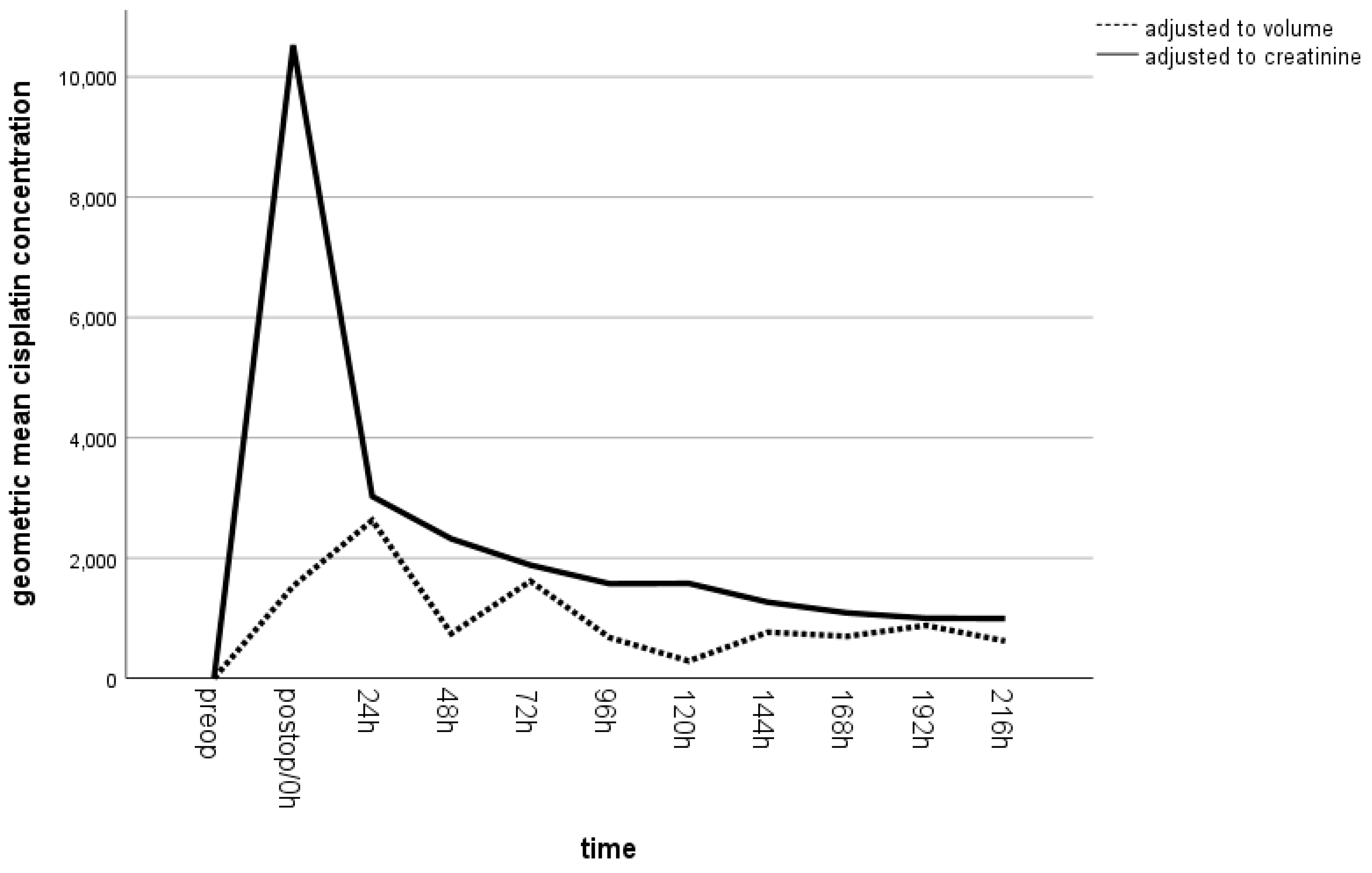
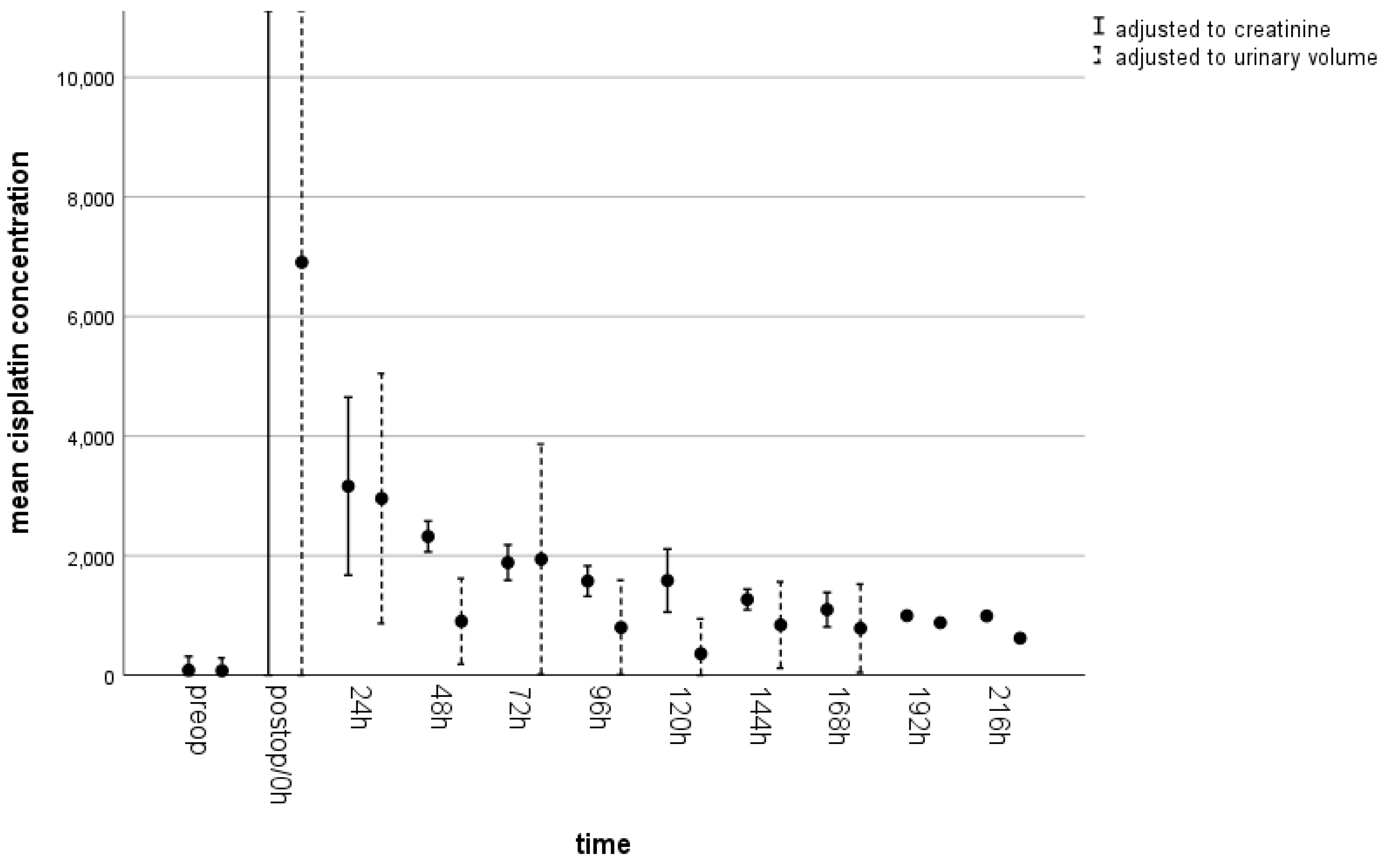
3.4. Cisplatin in Urine
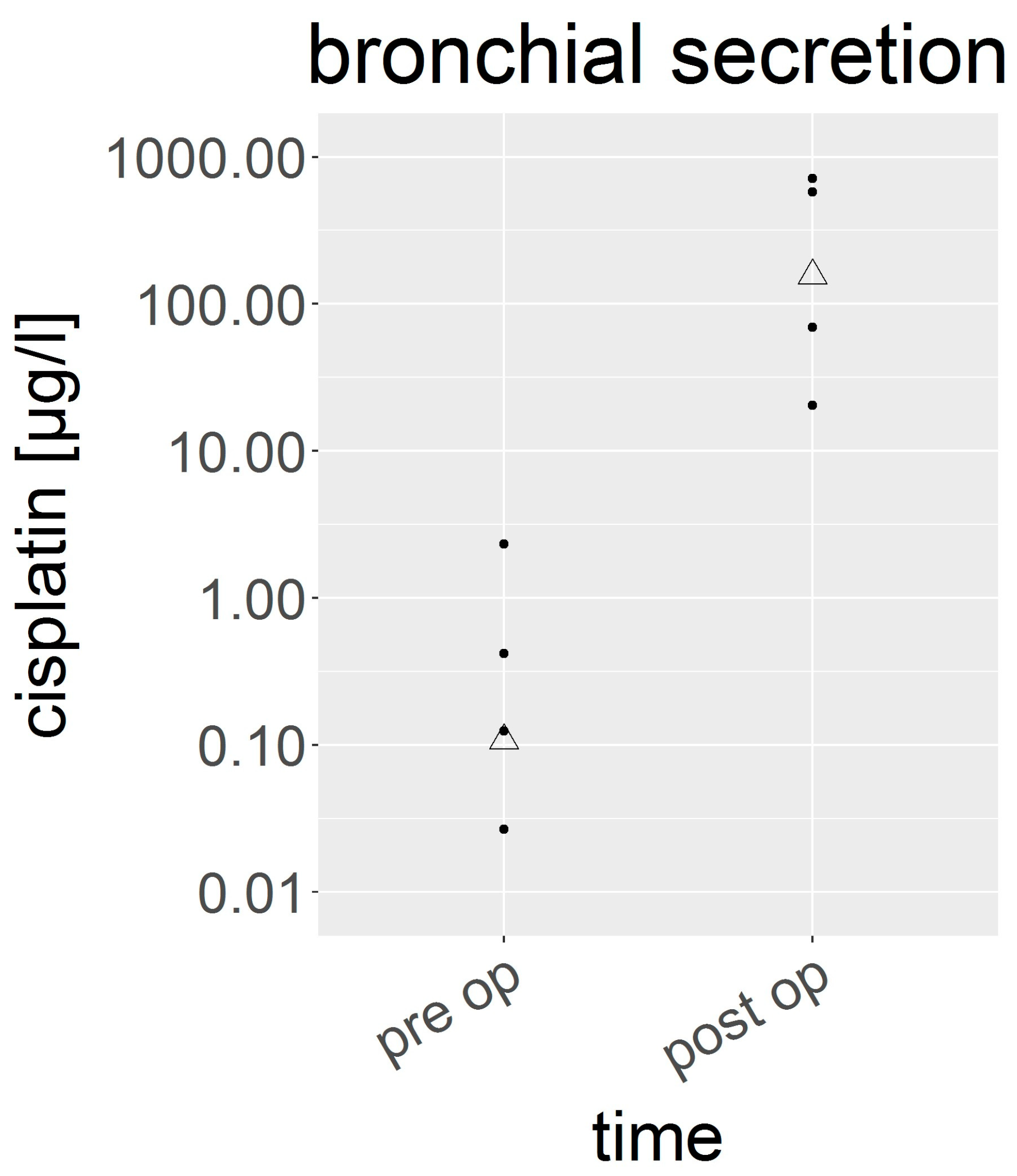
3.5. Cisplatin in Bronchial Secretion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


References
- Burt, B.M.; Richards, W.G.; Lee, H.-S.; Bartel, S.; DaSilva, M.C.; Gill, R.R.; Jaklitsch, M.T.; Johnson, B.E.; Swanson, S.J.; Bueno, R.; et al. A Phase I Trial of Surgical Resection and Intraoperative Hyperthermic Cisplatin and Gemcitabine for Pleural Mesothelioma. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2018, 13, 1400–1409. [Google Scholar] [CrossRef] [PubMed]
- Lapidot, M.; Gill, R.R.; Mazzola, E.; Freyaldenhoven, S.; Swanson, S.J.; Jaklitsch, M.T.; Sugarbaker, D.J.; Bueno, R. Pleurectomy Decortication in the Treatment of Malignant Pleural Mesothelioma: Encouraging Results and Novel Prognostic Implications Based on Experience in 355 Consecutive Patients. Ann. Surg. 2022, 275, 1212–1220. [Google Scholar] [CrossRef] [PubMed]
- Ried, M.; Kovacs, J.; Markowiak, T.; Muller, K.; Huppertz, G.; Koller, M.; Winter, H.; Klotz, L.V.; Hatz, R.; Zimmermann, J.; et al. Hyperthermic Intrathoracic Chemotherapy (HITOC) after Cytoreductive Surgery for Pleural Malignancies-A Retrospective, Multicentre Study. Cancers 2021, 13, 4580. [Google Scholar] [CrossRef] [PubMed]
- Hod, T.; Freedberg, K.J.; Motwani, S.S.; Chen, M.; Frendl, G.; Leaf, D.E.; Gupta, S.; Mothi, S.S.; Richards, W.G.; Bueno, R.; et al. Acute kidney injury after cytoreductive surgery and hyperthermic intraoperative cisplatin chemotherapy for malignant pleural mesothelioma. J. Thorac. Cardiovasc. Surg. 2021, 161, 1510–1518. [Google Scholar] [CrossRef]
- Ried, M.; Potzger, T.; Braune, N.; Diez, C.; Neu, R.; Sziklavari, Z.; Schalke, B.; Hofmann, H.S. Local and systemic exposure of cisplatin during hyperthermic intrathoracic chemotherapy perfusion after pleurectomy and decortication for treatment of pleural malignancies. J. Surg. Oncol. 2013, 107, 735–740. [Google Scholar] [CrossRef]
- Rusch, V.W.; Niedzwiecki, D.; Tao, Y.; Menendez-Botet, C.; Dnistrian, A.; Kelsen, D.; Saltz, L.; Markman, M. Intrapleural cisplatin and mitomycin for malignant mesothelioma following pleurectomy: Pharmacokinetic studies. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1992, 10, 1001–1006. [Google Scholar] [CrossRef]
- Sakaguchi, H.; Ishida, H.; Nitanda, H.; Yamazaki, N.; Kaneko, K.; Kobayashi, K. Pharmacokinetic evaluation of intrapleural perfusion with hyperthermic chemotherapy using cisplatin in patients with malignant pleural effusion. Lung Cancer 2017, 104, 70–74. [Google Scholar] [CrossRef]
- van Ruth, S.; van Tellingen, O.; Korse, C.M.; Verwaal, V.J.; Zoetmulder, F.A. Pharmacokinetics of doxorubicin and cisplatin used in intraoperative hyperthermic intrathoracic chemotherapy after cytoreductive surgery for malignant pleural mesothelioma and pleural thymoma. Anticancer Drugs 2003, 14, 57–65. [Google Scholar] [CrossRef]
- Ratto, G.B.; Civalleri, D.; Esposito, M.; Spessa, E.; Alloisio, A.; De Cian, F.; Vannozzi, M.O. Pleural space perfusion with cisplatin in the multimodality treatment of malignant mesothelioma: A feasibility and pharmacokinetic study. J. Thorac. Cardiovasc. Surg. 1999, 117, 759–765. [Google Scholar] [CrossRef]
- Schierl, R.; Novotna, J.; Piso, P.; Bohlandt, A.; Nowak, D. Low surface contamination by cis/oxaliplatin during hyperthermic intraperitoneal chemotherapy (HIPEC). Eur. J. Surg. Oncol. 2012, 38, 88–94. [Google Scholar] [CrossRef]
- Szikriszt, B.; Poti, A.; Nemeth, E.; Kanu, N.; Swanton, C.; Szuts, D. A comparative analysis of the mutagenicity of platinum-containing chemotherapeutic agents reveals direct and indirect mutagenic mechanisms. Mutagenesis 2021, 36, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Allgayer, N.; de Campos, R.A.; Gonzalez, L.P.F.; Flores, M.D.A.; Dihl, R.R.; Lehmann, M. Evaluation of mutagenic activity of platinum complexes in somatic cells of Drosophila melanogaster. Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2019, 133, 110782. [Google Scholar] [CrossRef] [PubMed]
- Ognio, E.; Lapide, M.; Ottone, M.; Mandys, V.; Peterka, M.; Parodi, B.; Viale, M. Embryo-lethal and teratogenic effect of the new platinum compound DPR in pregnant mice. Arch. Toxicol. 2003, 77, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.S.; Morgan, A.M.; Mekawy, M.M.; Zaki, A.R.; Ghazi, Z.M. Teratogenic effect of cisplatin in rats and the protective role of sodium selenate. Exp. Toxicol. Pathol. 2016, 68, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.S.; Morgan, A.M.; Mekawy, M.M.; Zeineb, M.A. Molecular mechanisms of Cisplatin- induced placental toxicity and teratogenicity in rats and the ameliorating role of N-acetyl-cysteine. Int. J. Biochem. Cell Biol. 2019, 115, 105579. [Google Scholar] [CrossRef] [PubMed]
- Kempf, S.R.; Ivankovic, S. Chemotherapy-induced malignancies in rats after treatment with cisplatin as single agent and in combination: Preliminary results. Oncology 1986, 43, 187–191. [Google Scholar] [CrossRef]
- Kempf, S.R.; Ivankovic, S. Carcinogenic effect of cisplatin (cis-diammine-dichloroplatinum (II), CDDP) in BD IX rats. J. Cancer Res. Clin. Oncol. 1986, 111, 133–136. [Google Scholar] [CrossRef]
- Fung, C.; Dinh, P., Jr.; Ardeshir-Rouhani-Fard, S.; Schaffer, K.; Fossa, S.D.; Travis, L.B. Toxicities Associated with Cisplatin-Based Chemotherapy and Radiotherapy in Long-Term Testicular Cancer Survivors. Adv. Urol. 2018, 2018, 8671832. [Google Scholar] [CrossRef]
- Markowiak, T.; Ried, M.; Larisch, C.; Nowak, D.; Hofmann, H.S.; Rakete, S. Exposure to cisplatin in the operating room during hyperthermic intrathoracic chemotherapy. Int. Arch. Occup. Environ. Health 2022, 95, 399–407. [Google Scholar] [CrossRef]
- Andersson, A.; Fagerberg, J.; Lewensohn, R.; Ehrsson, H. Pharmacokinetics of cisplatin and its monohydrated complex in humans. J. Pharm. Sci. 1996, 85, 824–827. [Google Scholar] [CrossRef]
- Kromhout, H.; Hoek, F.; Uitterhoeve, R.; Huijbers, R.; Overmars, R.F.; Anzion, R.; Vermeulen, R. Postulating a dermal pathway for exposure to anti-neoplastic drugs among hospital workers. Applying a conceptual model to the results of three workplace surveys. Ann. Occup. Hyg. 2000, 44, 551–560. [Google Scholar] [CrossRef]
- Sessink, P.J.; Van de Kerkhof, M.C.; Anzion, R.B.; Noordhoek, J.; Bos, R.P. Environmental contamination and assessment of exposure to antineoplastic agents by determination of cyclophosphamide in urine of exposed pharmacy technicians: Is skin absorption an important exposure route? Arch. Environ. Health 1994, 49, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Zhengzheng Xie, M.S.; Li, Y.; Yan, D.; Hu, X.; Liu Liu, M.S.; Lulu Sun, B.S.; Tao, X.; Yan, D.; Ping Yang, M.S.; Zhang, Z. Evaluation of exposure risk for healthcare personnel performing the open technique HIPEC procedure using cisplatin. Gynecol. Oncol. 2021, 161, 261–263. [Google Scholar] [CrossRef]
- Ametsbichler, P.; Bohlandt, A.; Nowak, D.; Schierl, R. Occupational exposure to cisplatin/oxaliplatin during Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC)? Eur. J. Surg. Oncol. 2018, 44, 1793–1799. [Google Scholar] [CrossRef] [PubMed]
- Villa, A.F.; El Balkhi, S.; Aboura, R.; Sageot, H.; Hasni-Pichard, H.; Pocard, M.; Elias, D.; Joly, N.; Payen, D.; Blot, F.; et al. Evaluation of oxaliplatin exposure of healthcare workers during heated intraperitoneal perioperative chemotherapy (HIPEC). Ind. Health 2015, 53, 28–37. [Google Scholar] [CrossRef]
- Ndaw, S.; Hanser, O.; Kenepekian, V.; Vidal, M.; Melczer, M.; Remy, A.; Robert, A.; Bakrin, N. Occupational exposure to platinum drugs during intraperitoneal chemotherapy. Biomonitoring and surface contamination. Toxicol. Lett. 2018, 298, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Saint-Lorant, G.; Rodier, S.; Guilloit, J.M.; Ndaw, S.; Melczer, M.; Lagadu, S.; Palix, A.; Delepee, R. Is the blood of a surgeon performing HIPEC contaminated by irinotecan, its major metabolites and platinum compounds? Pleura Peritoneum 2021, 6, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Dugheri, S.; Bonari, A.; Pompilio, I.; Boccalon, P.; Tognoni, D.; Cecchi, M.; Ughi, M.; Mucci, N.; Arcangeli, G. Analytical strategies for assessing occupational exposure to antineoplastic drugs in healthcare workplaces. Med. Pr. 2018, 69, 589–604. [Google Scholar] [CrossRef]
- Koller, M.; Bohlandt, A.; Haberl, C.; Nowak, D.; Schierl, R. Environmental and biological monitoring on an oncology ward during a complete working week. Toxicol. Lett. 2018, 298, 158–163. [Google Scholar] [CrossRef]
- Schenk, K.E.; Schierl, R.; Angele, M.; Burkhart-Reichl, A.; Glockzin, G.; Novotny, A.; Nowak, D. Cisplatin and oxaliplatin surface contamination in intensive care units (ICUs) and hospital wards during attendance of HIPEC patients. Int. Arch. Occup. Environ. Health 2016, 89, 991–996. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age (Years) | Sex | Tumour Stage | Surgery | Creatinine (mg/dL)/GFR Preop |
|---|---|---|---|---|---|
| 1 | 39 | male | MPM stage II | EPP | 0.64/125 |
| 2 | 57 | male | MPM stage II | eP/D | 0.65/110 |
| 3 | 75 | female | MPM stage IB | eP/D | 0.76/77 |
| 4 | 74 | male | MPM IIIA | eP/D | 0.85/86 |
| 5 | 64 | male | MPM stage IB | eP/D | 0.75/98 |
| Time | Serum (µg/L) | Pleural Effusion (µg/L) | Urine (µg/g Creatinine) | Urine (µg/L Urine) | Bronchial Secretion (µg/L) |
|---|---|---|---|---|---|
| preop | 0.79 (0.33–1.90) | --- | 3.5 (0.15–417) | 1.29 (0.07–384) | 0.11 (0.004–2.33) |
| postop/0 h | 1349 (1160–1437) | --- | 10,528 (442–197,421) | 1531 (143–27,873) | 156 (70–580) |
| 24 h | 452 (360–544) | 618 (388–1524) | 3025 (2404–5278) | 2627 (1490–5637) | --- |
| 48 h | 354 (216–452) | 392 (228–658) | 2319 (2040–2554) | 745 (305–1630) | --- |
| 72 h | 279 (204–381) | 304 (211–471) | 1882 (1677–2059) | 1615 (516–3159) | --- |
| 96 h | 229 (186–287) | 237 (161–348) | 1573 (1344–1696) | 676 (371–1329) | --- |
| 120 h | 187 (159–250) | 180 (162–201) | 1578 (1424–1828) | 288 (102–561) | --- |
| 144 h | 211 (152–353) | 216 (189–268) | 1266 (1122–1377) | 767 (513–1509) | --- |
| 168 h | 168 (138–237) | 127 (47–241) | 1088 (882–1314) | 698 (401–1456) | --- |
| 192 h | 178 * | 71 * | 999 * | 879 * | --- |
| 216 h | 133 * | 93 * | 994 * | 620 * | --- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larisch, C.; Markowiak, T.; Ried, M.; Nowak, D.; Hofmann, H.-S.; Rakete, S. The Excretion of Cisplatin after Hyperthermic Intrathoracic Chemotherapy. Cancers 2023, 15, 4872. https://doi.org/10.3390/cancers15194872
Larisch C, Markowiak T, Ried M, Nowak D, Hofmann H-S, Rakete S. The Excretion of Cisplatin after Hyperthermic Intrathoracic Chemotherapy. Cancers. 2023; 15(19):4872. https://doi.org/10.3390/cancers15194872
Chicago/Turabian StyleLarisch, Christopher, Till Markowiak, Michael Ried, Dennis Nowak, Hans-Stefan Hofmann, and Stefan Rakete. 2023. "The Excretion of Cisplatin after Hyperthermic Intrathoracic Chemotherapy" Cancers 15, no. 19: 4872. https://doi.org/10.3390/cancers15194872