
Development of a Treatment Planning Framework for Laser Interstitial Thermal Therapy (LITT)

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
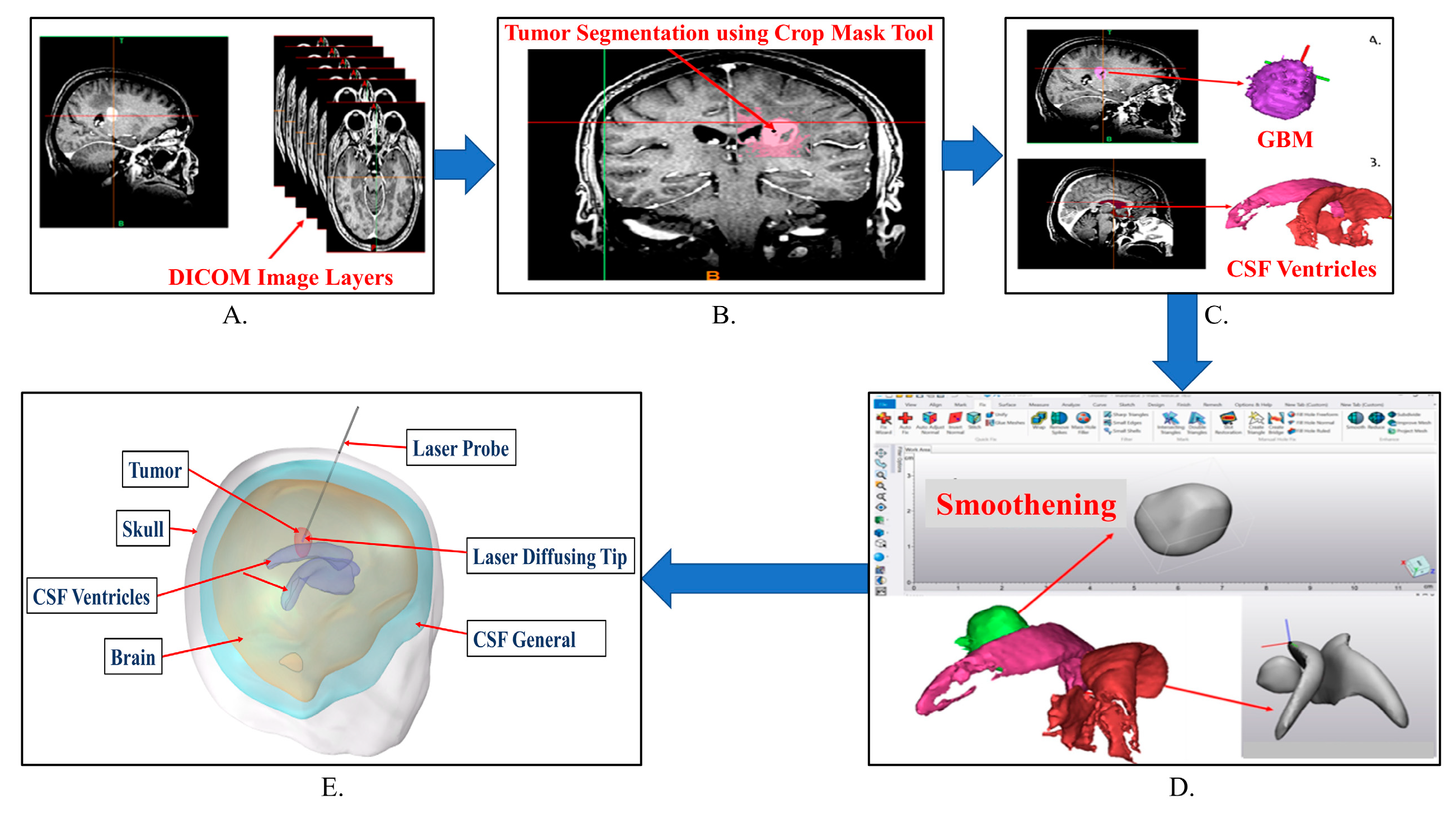
2.1. Medical Image Segmentation
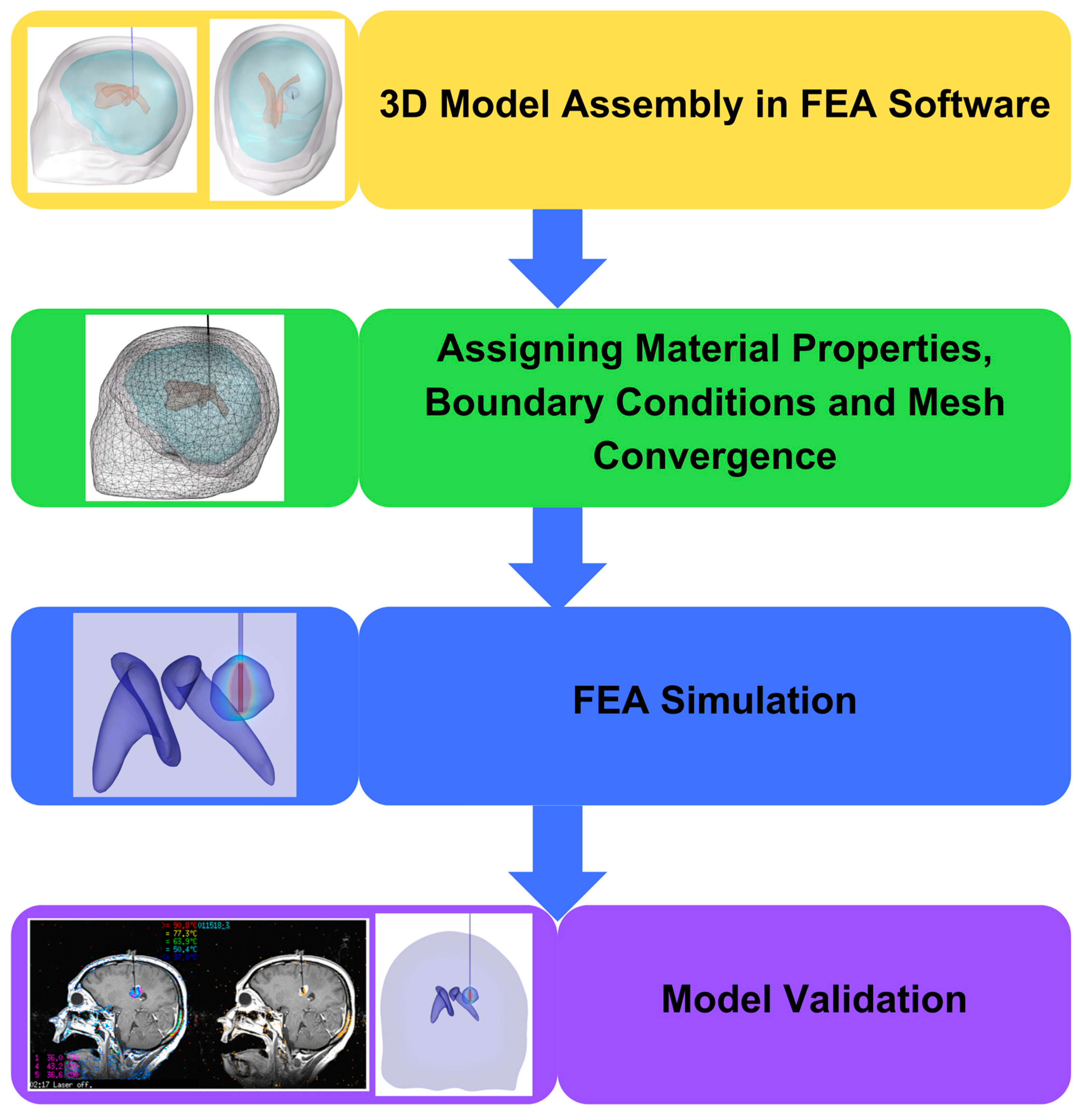
2.2. Importing the 3D Model into FEA Software
2.3. Assigning Material Properties
2.4. Modeling the Bioheat Transfer Equation with Time Dependent Study
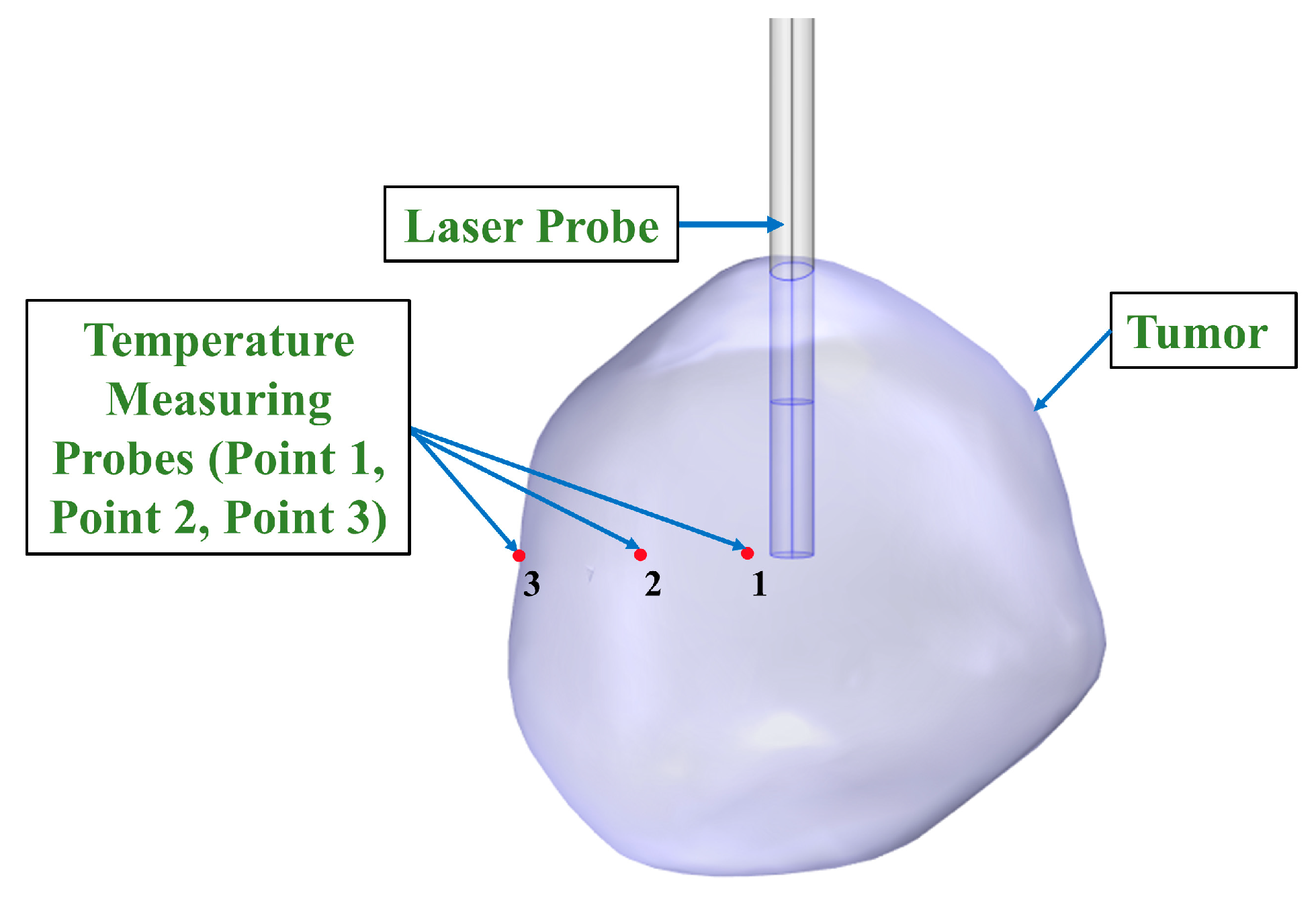
2.5. Modeling Temperature Distribution
2.6. Modeling Thermal Damage Dependent Blood Perfusion
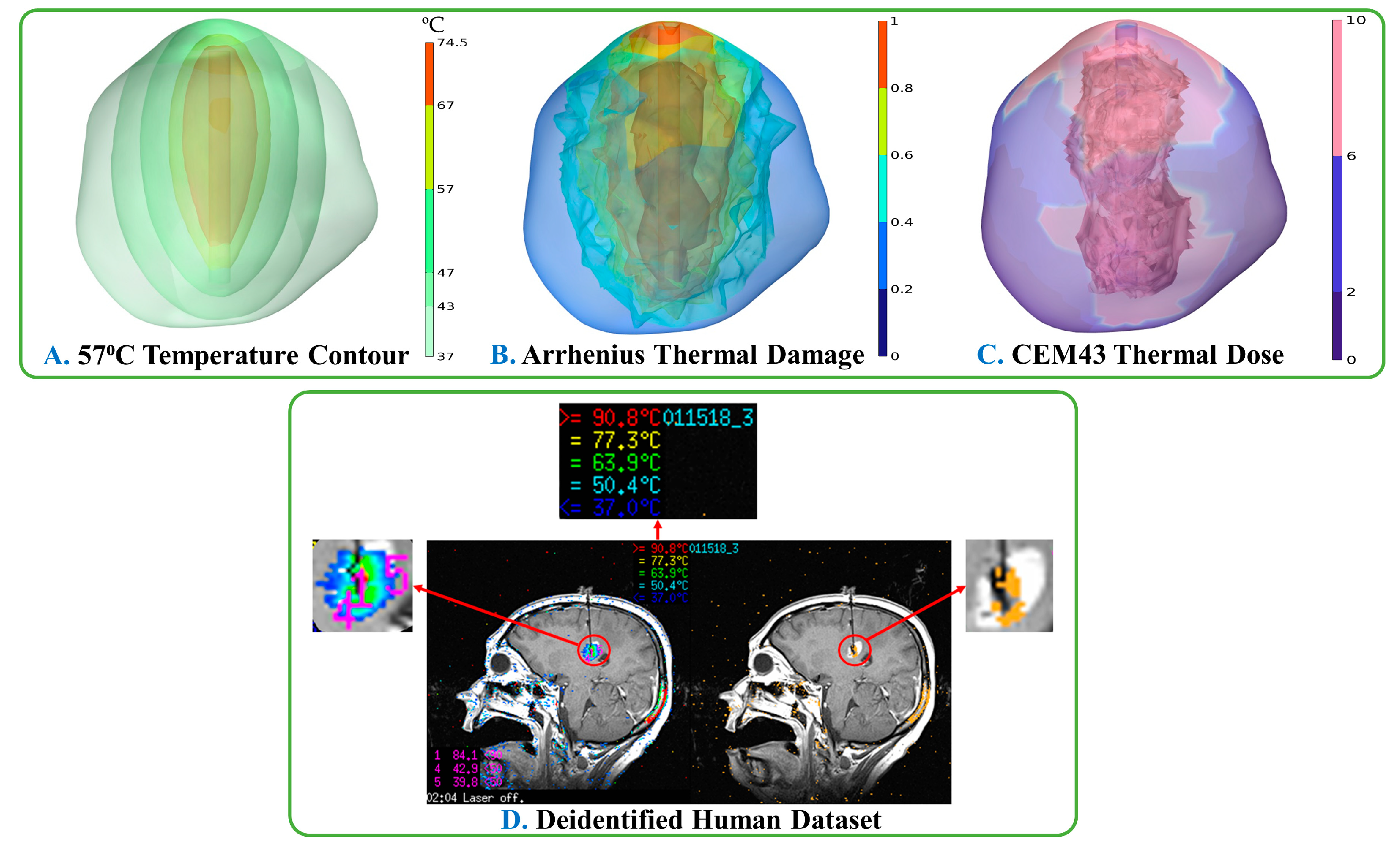
2.7. Calculating CEM43 Thermal Dose Volume
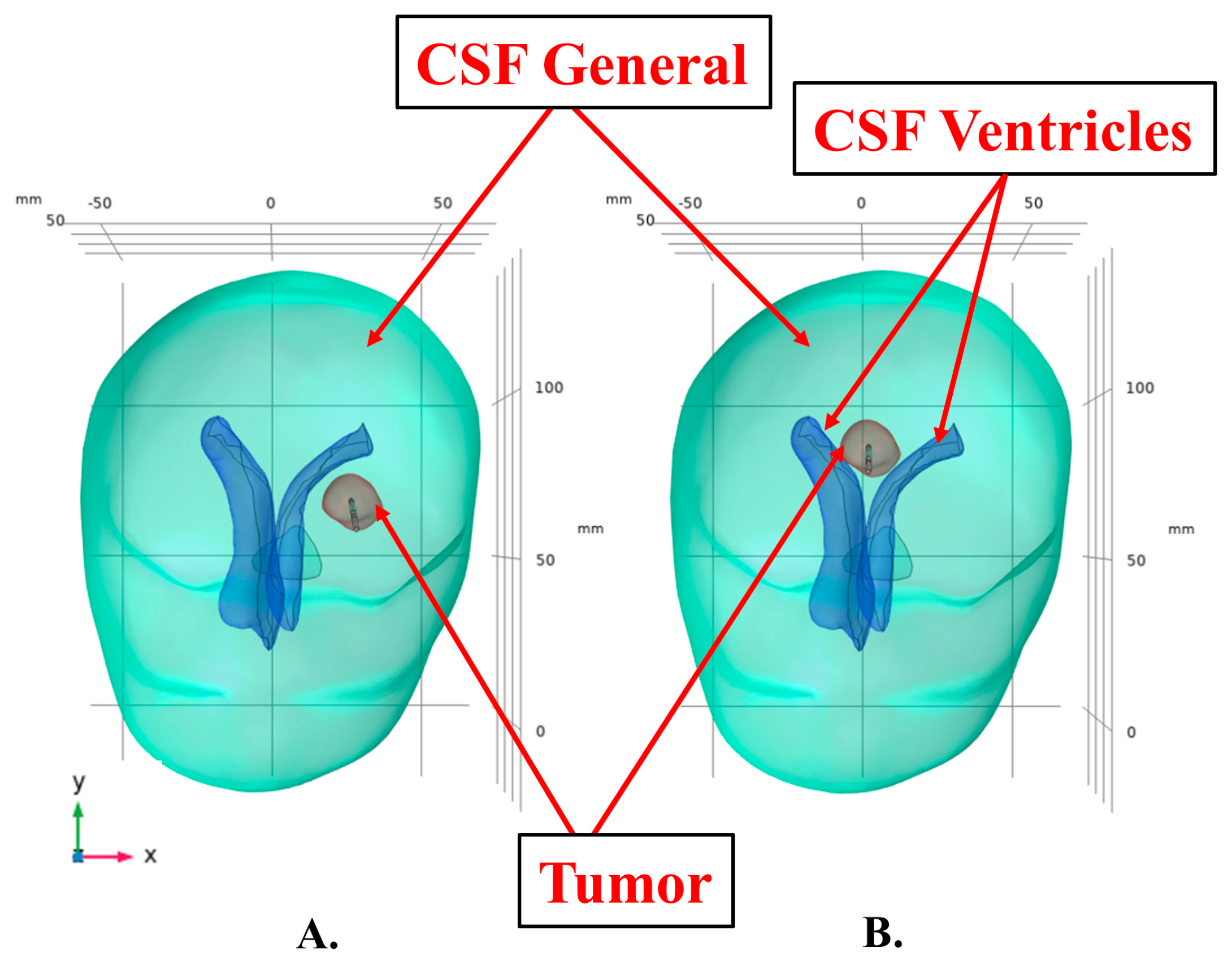
2.8. Modeling CSF and CSF Ventricles
- CSF and CSF ventricles modeled as solids with high thermal conductivity, 6.2 [W/m·K] and
- CSF and CSF ventricles modeled as fluids with convectively enhanced conductivity.
2.9. Laser-Tissue Interaction
2.10. Defining Idealized Computational Model
2.11. Modeling Convective Cooling Induced by the CSF Based on Tumor Location
2.12. Modeling Stationary Heat Source with Pulsed Laser Power
2.13. Modeling Pullback Laser Probe with Pulsed Laser Power
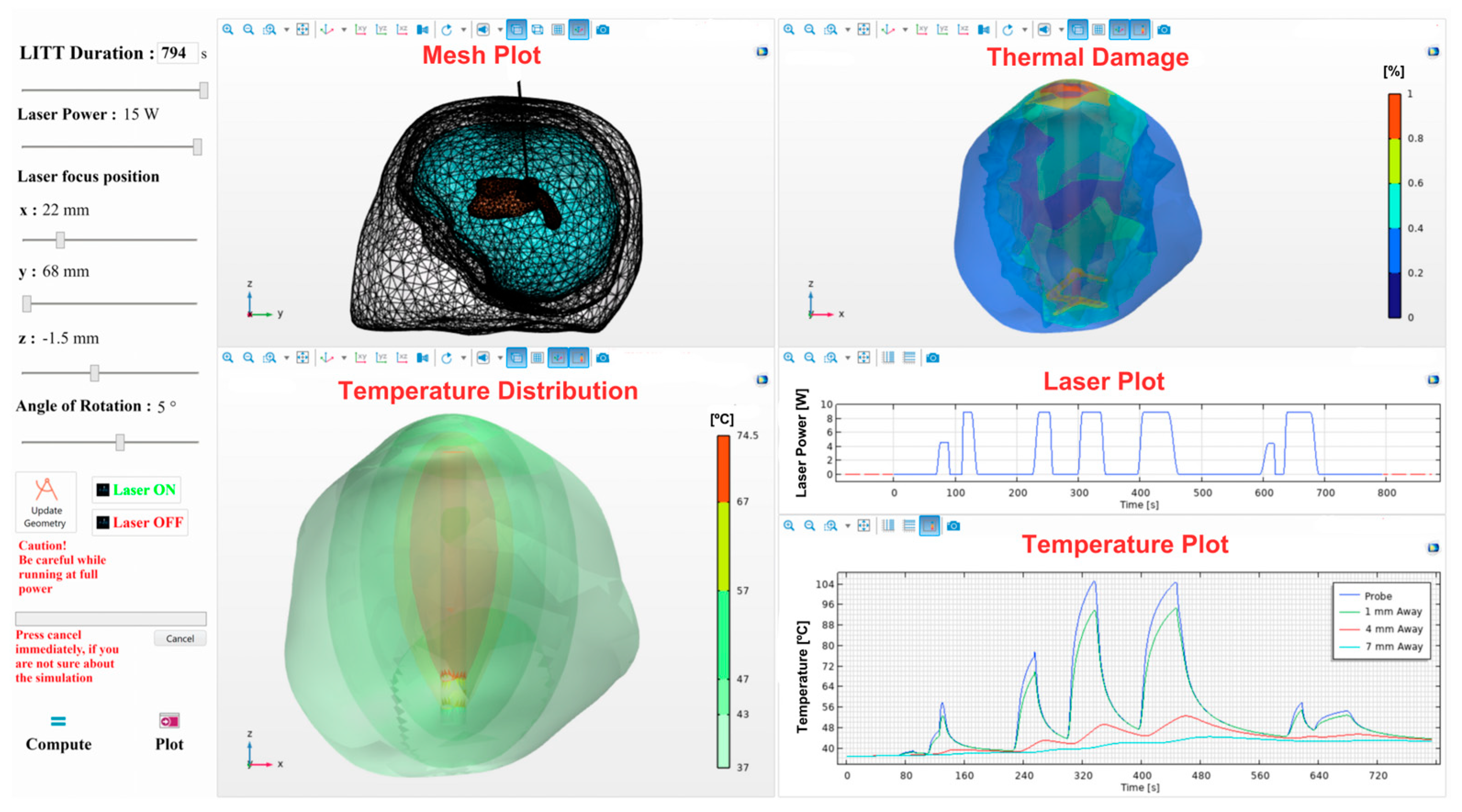
2.14. Creating a Graphical User Interface (GUI)
3. Results
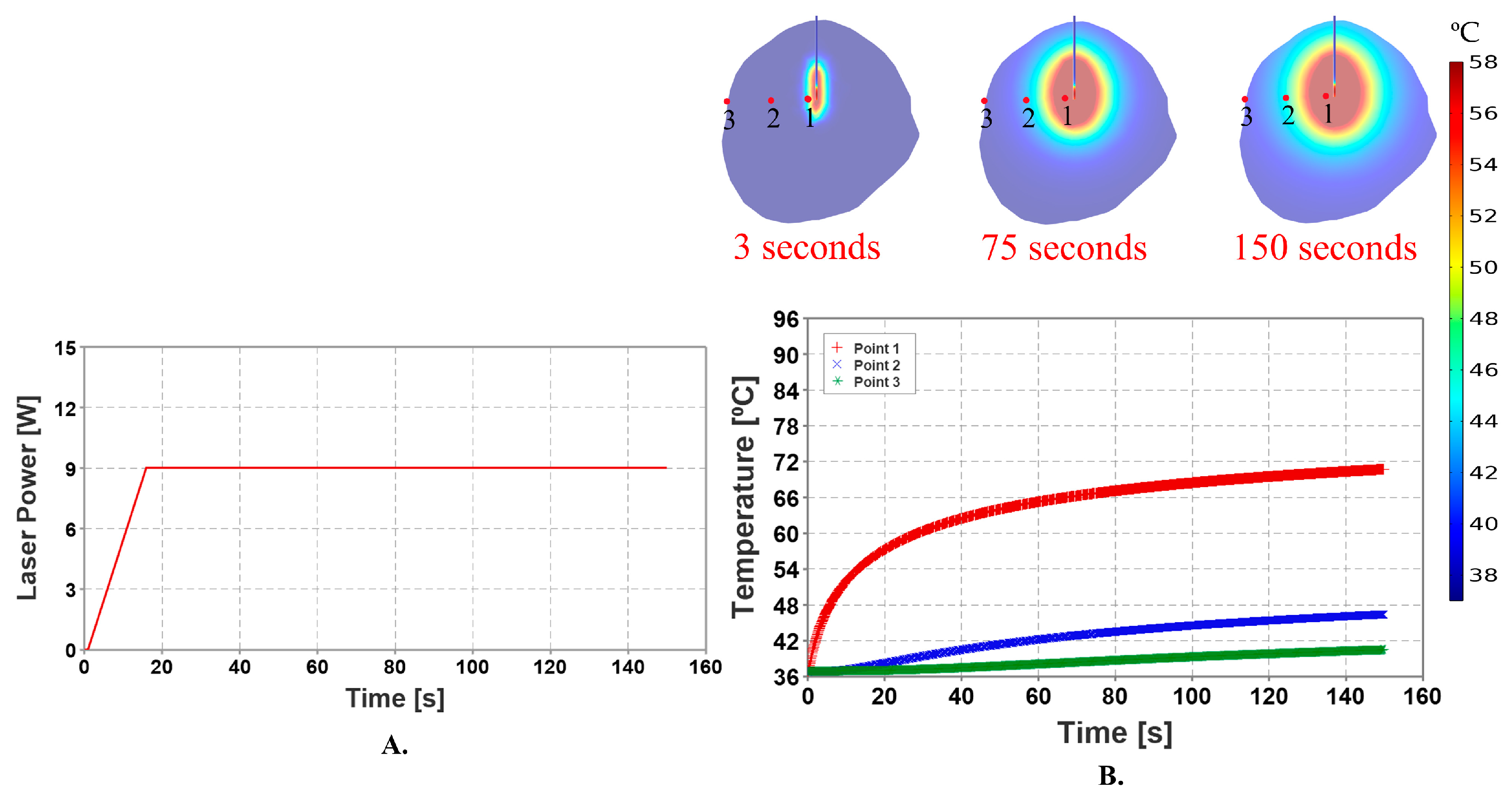
3.1. Stationary Heat Source with Constant Laser Power
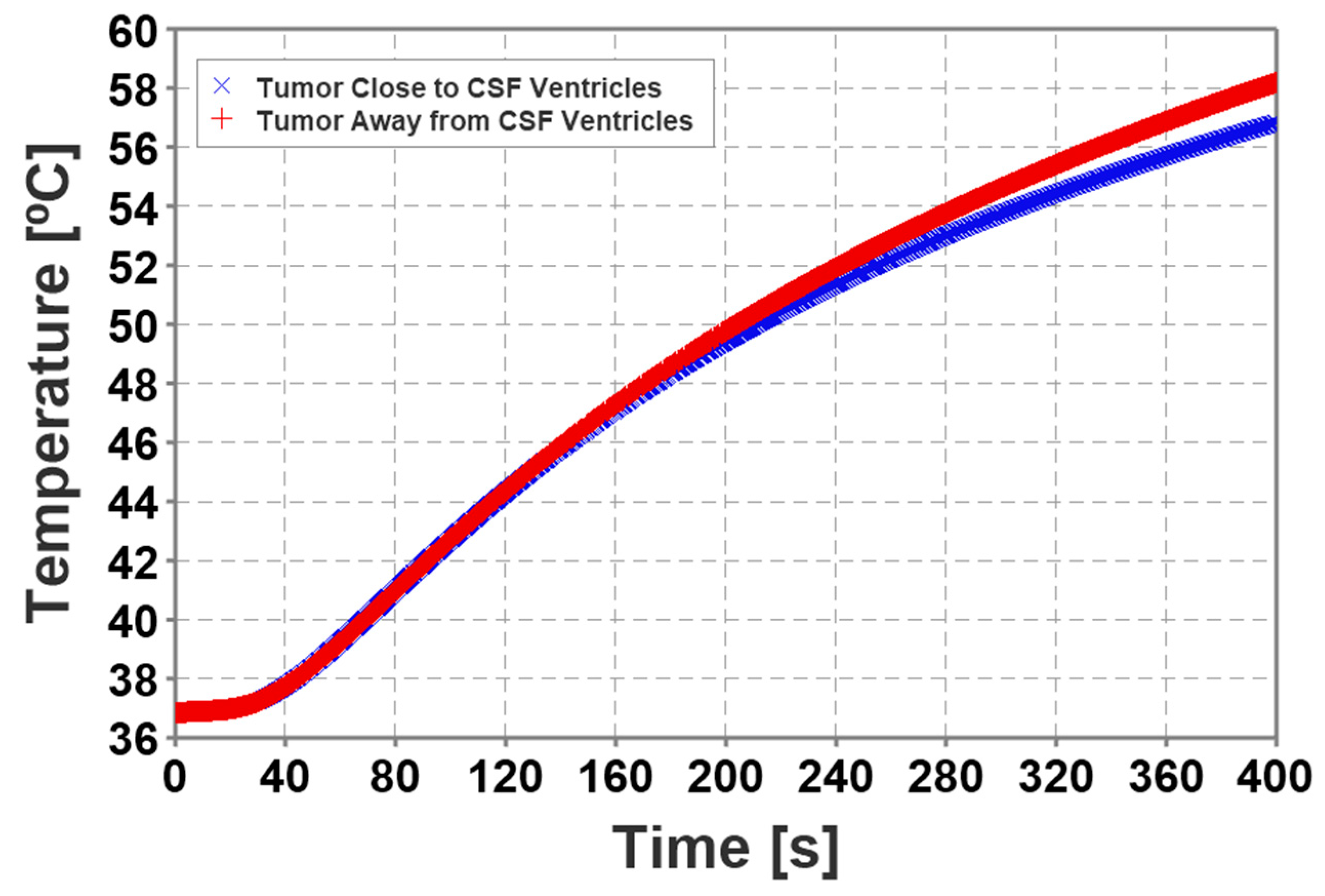
3.2. Convective Cooling Induced by CSF and CSF Ventricles
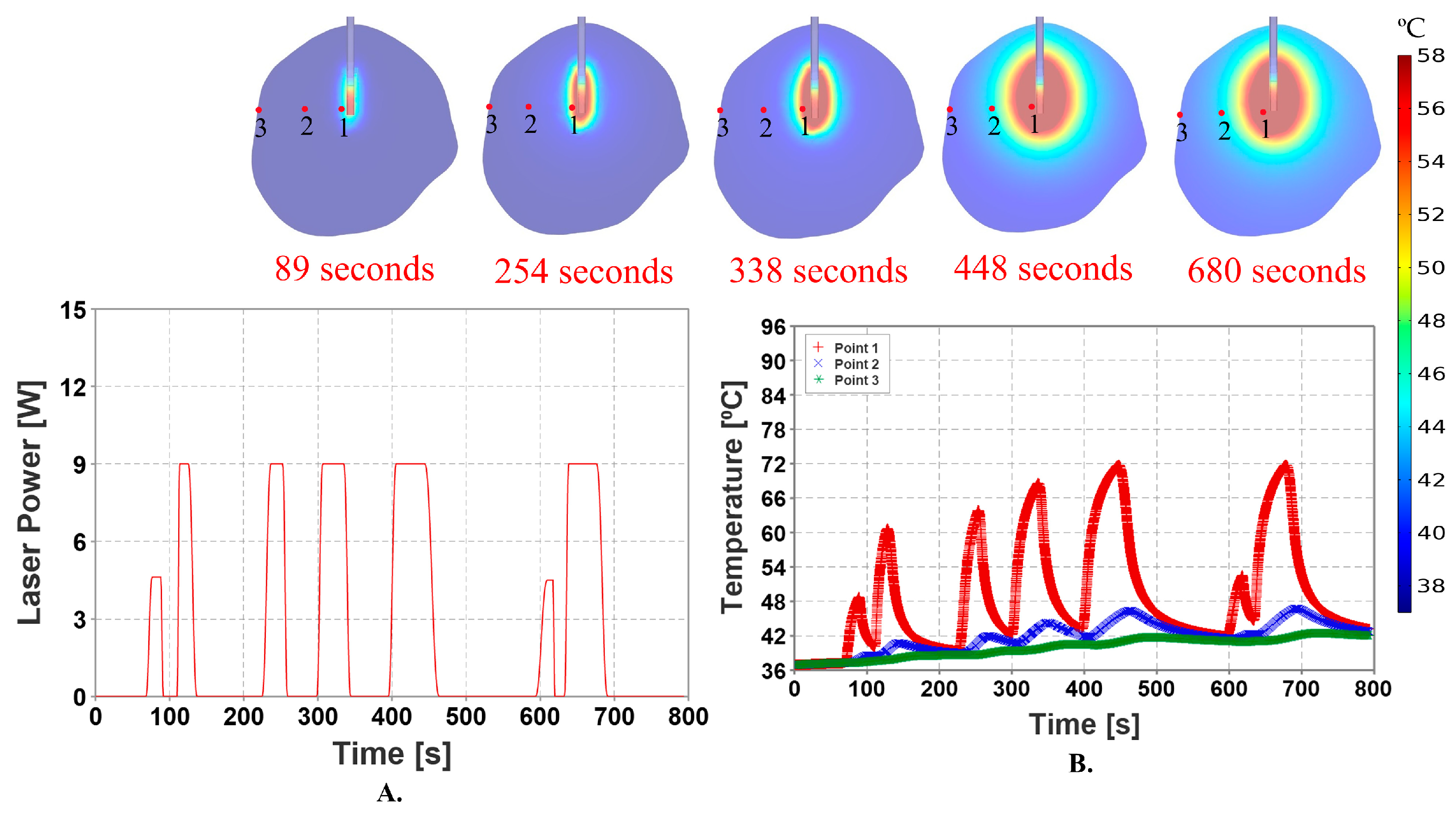
3.3. Stationary Heat Source with Pulsed Laser Power
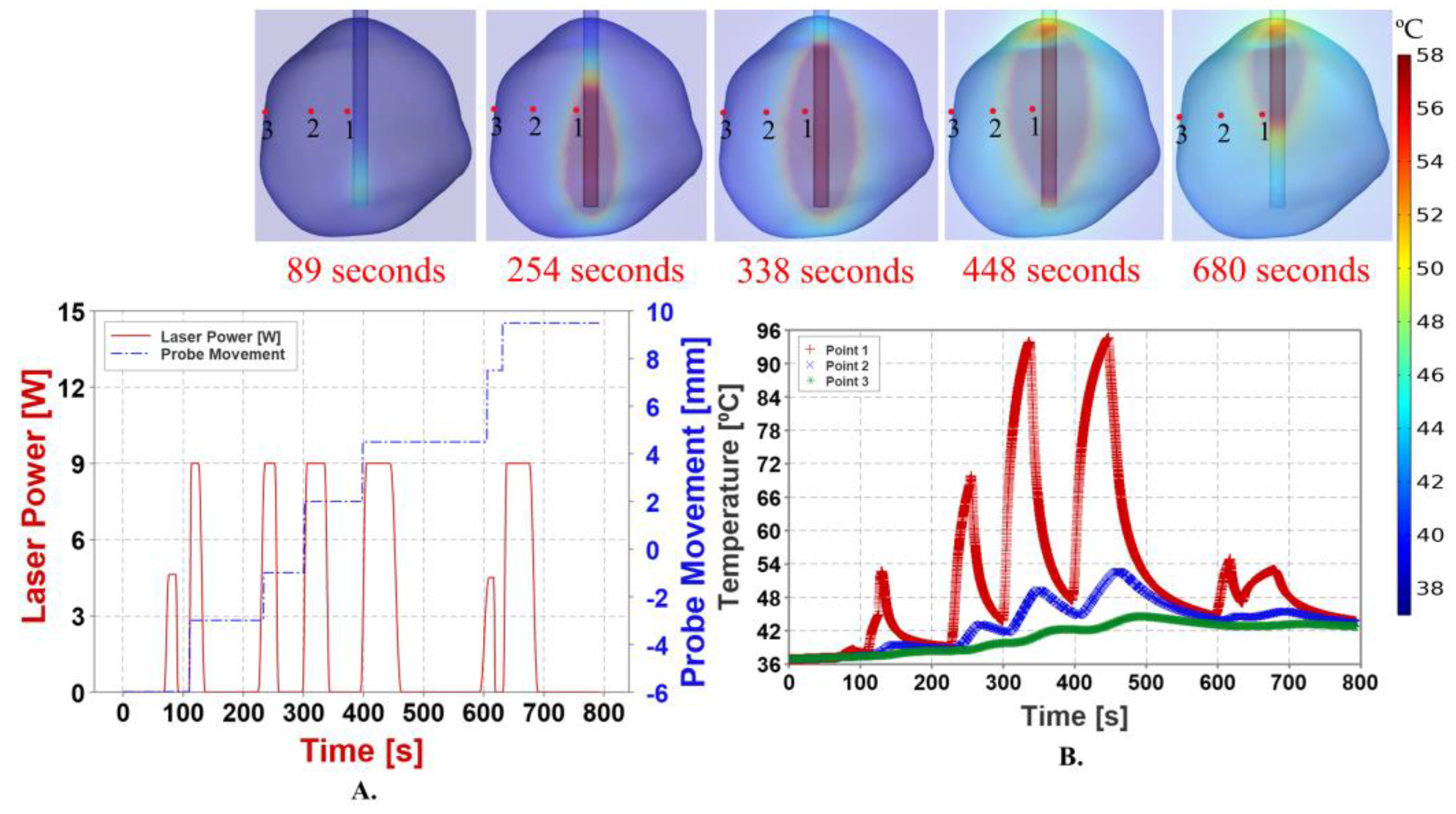
3.4. Pullback Heat Source with Pulsed Laser Power
4. Discussion
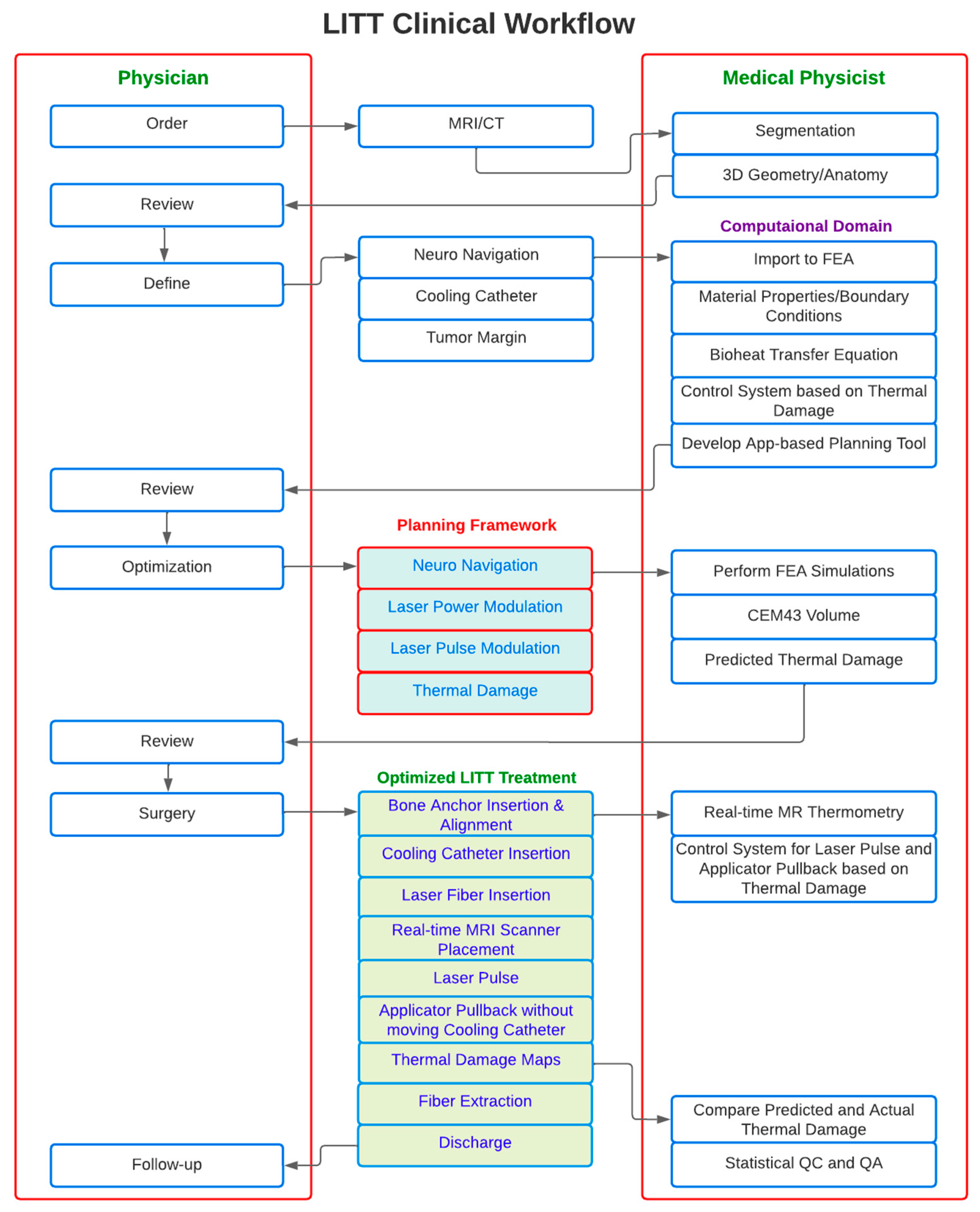
Proposed Workflow for LITT Treatment Framework
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Brain Tumor Association. Glioblastoma. Available online: https://www.abta.org/types-of-tumors/glioblastoma/ (accessed on 16 March 2023).
- Lee, E.J.; Kalia, S.K.; Hong, S.H. A Primer on Magnetic Resonance-Guided Laser Interstitial Thermal Therapy for Medically Refractory Epilepsy. J. Korean Neurosurg. Soc. 2019, 62, 353–360. [Google Scholar] [CrossRef]
- Chen, C.; Lee, I.; Tatsui, C.; Elder, T.; Sloan, A.E. Laser interstitial thermotherapy (LITT) for the treatment of tumors of the brain and spine: A brief review. J. Neuro-Oncol. 2021, 151, 429–442. [Google Scholar] [CrossRef]
- Thomas, J.G.; Rao, G.; Kew, Y.; Prabhu, S.S. Laser interstitial thermal therapy for newly diagnosed and recurrent glioblastoma. Neurosurg. Focus 2016, 41, E12. [Google Scholar] [CrossRef]
- Repasky, E.A.; Evans, S.S.; Dewhirst, M.W. Temperature Matters! And Why It Should Matter to Tumor Immunologists. Cancer Immunol. Res. 2013, 1, 210–216. [Google Scholar] [CrossRef]
- Jensdottir, M.; Sandvik, U.; Jakola, A.S.; Fagerlund, M.; Kits, A.; Gudhmundsdottir, K.; Tabari, S.; Majing, T.; Fletch-er-Sandersjoo, A.; Chen, C.C.; et al. Learning Curve Analysis and Adverse Events After Implementation of Neurosurgical Laser Ablation Treatment: A Population-Based Single-Institution Consecutive Series. Neurosurg. Clin. 2023, 34, 259–267. [Google Scholar] [CrossRef]
- Patel, P.; Patel, N.V.; Danish, S.F. Intracranial MR-guided laser-induced thermal therapy: Single-center experience with the Visualase thermal therapy system. J. Neurosurg. 2016, 125, 853–860. [Google Scholar] [CrossRef]
- Torres-Reveron, J.; Tomasiewicz, H.C.; Shetty, A.; Amankulor, N.M.; Chiang, V.L. Stereotactic laser induced thermotherapy (LITT): A novel treatment for brain lesions regrowing after radiosurgery. J. Neuro-Oncol. 2013, 113, 495–503. [Google Scholar] [CrossRef]
- Surgical Planning Brain Lab. Available online: https://www.brainlab.com/digital-o-r/surgical-planning/ (accessed on 15 August 2023).
- End-to-End Orthopedic Templating, Brain Lab TraumaCad. Available online: https://www.brainlab.com/surgery-products/orthopedic-surgery-products/orthopedic-templating-software/#tcmobile (accessed on 15 August 2023).
- EmprintTM Ablation System. Available online: https://play.google.com/store/apps/details?id=com.covidienlp.emprint&pcampaignid=web_share (accessed on 17 August 2023).
- Fahrenholtz, S.J.; Moon, T.Y.; Franco, M.; Medina, D.; Danish, S.; Gowda, A.; Shetty, A.; Maier, F.; Hazle, J.D.; Stafford, R.J.; et al. A model evaluation study for treatment planning of laser-induced thermal therapy. Int. J. Hyperth. 2015, 31, 705–714. [Google Scholar] [CrossRef]
- Yeniaras, E.; Fuentes, D.T.; Fahrenholtz, S.J.; Weinberg, J.S.; Maier, F.; Hazle, J.D.; Stafford, R.J. Design and initial evaluation of a treatment planning software system for MRI-guided laser ablation in the brain. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 659–667. [Google Scholar] [CrossRef]
- Shang, M. A Novel Laser Interstitial Thermal Therapy Treatment Planning System to Optimize Laser Ablation Delivery to Brain Targets. Ph.D. Thesis, University of Florida, Gainesville, FL, USA, 2019. [Google Scholar]
- Bi, S.; Liu, H.; Nan, Q.; Mai, X. Study on the Effect of Micro-Vessels on Ablation Effect in Laser Interstitial Brain Tissue Thermal Therapy Based on PID Temperature Control. Appl. Sci. 2023, 13, 3751. [Google Scholar] [CrossRef]
- Mitchell, D.; Fahrenholtz, S.; MacLellan, C.; Bastos, D.; Rao, G.; Prabhu, S.; Weinberg, J.; Hazle, J.; Stafford, J.; Fuentes, D. A heterogeneous tissue model for treatment planning for magnetic resonance-guided laser interstitial thermal therapy. Int. J. Hyperth. 2018, 34, 943–952. [Google Scholar] [CrossRef]
- Bergeron, D.; Iorio-Morin, C.; Bigder, M.; Dakson, A.; Eagles, M.E.; Elliott, C.A.; Honey, C.M.; Kameda-Smith, M.M.; Persad, A.R.L.; Touchette, C.J.; et al. Mobile applications in neurosurgery: A systematic review, quality audit, and survey of Canadian neurosurgery residents. World Neurosurg. 2019, 127, e1026–e1038. [Google Scholar] [CrossRef]
- Butson, C.R.; Tamm, G.; Jain, S.; Fogal, T.; Krüger, J. Evaluation of Interactive Visualization on Mobile Computing Platforms for Selection of Deep Brain Stimulation Parameters. IEEE Trans. Vis. Comput. Graph. 2012, 19, 108–117. [Google Scholar] [CrossRef]
- Jamal, A.; Yuan, T.; Galvan, S.; Castellano, A.; Riva, M.; Secoli, R.; Falini, A.; Bello, L.; Rodriguez y Baena, F.; Dini, D.; et al. Insights into infusion-based targeted drug delivery in the brain: Perspectives, challenges and opportunities. Int. J. Mol. Sci. 2022, 23, 3139. [Google Scholar] [CrossRef] [PubMed]
- Saha, N.; Kuehne, A.; Millward, J.M.; Eigentler, T.W.; Starke, L.; Waiczies, S.; Niendorf, T. Advanced Radio Frequency Applicators for Thermal Magnetic Resonance Theranostics of Brain Tumors. Cancers 2023, 15, 2303. [Google Scholar] [CrossRef] [PubMed]
- Ademaj, A.; Veltsista, D.P.; Ghadjar, P.; Marder, D.; Oberacker, E.; Ott, O.J.; Wust, P.; Puric, E.; Hälg, R.A.; Rogers, S.; et al. Clinical Evidence for Thermometric Parameters to Guide Hyperthermia Treatment. Cancers 2022, 14, 625. [Google Scholar] [CrossRef]
- Ginalis, E.E.; Danish, S.F. Magnetic resonance–guided laser interstitial thermal therapy for brain tumors in geriatric patients. Neurosurg. Focus 2020, 49, E12. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.; Kim, A.H. Laser Interstitial Thermal Therapy. Mo. Med. 2020, 117, 50. [Google Scholar] [PubMed]
- Pruitt, R.; Gamble, A.; Black, K.; Schulder, M.; Mehta, A.D. Complication avoidance in laser interstitial thermal therapy: Lessons learned. J. Neurosurg. 2017, 126, 1238–1245. [Google Scholar] [CrossRef]
- Sun, X.R.; Nitesh, V.P.; Shabbar, F.D. Tissue ablation dynamics during magnetic resonance–guided, laser-induced thermal therapy. Neurosurgery 2015, 77, 51–58. [Google Scholar] [CrossRef]
- Sloan, A.E.; Ahluwalia, M.S.; Valerio-Pascua, J.; Manjila, S.; Torchia, M.G.; Jones, S.E.; Sunshine, J.L.; Phillips, M.; Griswold, M.A.; Clampitt, M.; et al. Results of the NeuroBlate System first-in-humans Phase I clinical trial for recurrent glioblastoma. J. Neurosurg. 2013, 118, 1202–1219. [Google Scholar] [CrossRef]
- FDA Alert on MR-Guided Laser Interstitial Thermal Therapy Devices. Available online: https://www.medscape.com/viewarticle/895688 (accessed on 16 March 2023).
- Tyc, R.; Torchia, M.G.; Beccaria, K.; Canney, M.; Carpentier, A. Magnetic Resonance-Guided Laser Interstitial Thermal Therapy: Historical Perspectives and Overview of the Principles of LITT. In Laser Interstitial Thermal Therapy in Neurosurgery; Springer: Cham, Switzerland, 2020; pp. 1–17. [Google Scholar] [CrossRef]
- Donos, C.; Breier, J.; Friedman, E.; Rollo, P.; Johnson, J.; Moss, L.; Thompson, S.; Thomas, M.; Hope, O.; Slater, J.; et al. Laser ablation for mesial temporal lobe epilepsy: Surgical and cognitive outcomes with and without mesial temporal sclerosis. Epilepsia 2018, 59, 1421–1432. [Google Scholar] [CrossRef]
- Schooneveldt, G.; Trefná, H.D.; Persson, M.; de Reijke, T.M.; Blomgren, K.; Kok, H.P.; Crezee, H. Hyperthermia Treatment Planning Including Convective Flow in Cerebrospinal Fluid for Brain Tumour Hyperthermia Treatment using a Novel Dedicated Paediatric Brain Applicator. Cancers 2019, 11, 1183. [Google Scholar] [CrossRef]
- Maureen, S. Mimics Innovation Suite Training; Johns Hopkins School of Medicine: Baltimore, MD, USA, 2021. Available online: www.materialise.com (accessed on 7 December 2022).
- ITIS Foundation. Tissue Properties. Available online: https://itis.swiss/virtual-population/tissue-properties/database/database-summary/ (accessed on 7 December 2022).
- ITIS Foundation. Heat Capacity. Available online: https://itis.swiss/virtual-population/tissue-properties/database/heat-capacity/ (accessed on 7 December 2022).
- ITIS Foundation. Thermal Conductivity. Available online: https://itis.swiss/virtual-population/tissue-properties/database/thermal-conductivity/ (accessed on 7 December 2022).
- Final Advanced Materials. Pure Silica Fibre. Available online: https://www.final-materials.com/gb/24-pure-silica-fibre (accessed on 7 December 2022).
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. J. Appl. Physiol. 1948, 1, 93–122. [Google Scholar] [CrossRef]
- Feng, Y.; Fuentes, D. Model-based planning and real-time predictive control for laser-induced thermal therapy. Int. J. Hyperth. 2011, 27, 751–761. [Google Scholar] [CrossRef] [PubMed]
- He, X.; McGee, S.; Coad, J.E.; Schmidlin, F.; Iaizzo, P.A.; Swanlund, D.J.; Kluge, S.; Rudie, E.; Bischof, J.C. Investigation of the thermal and tissue injury behaviour in microwave thermal therapy using a porcine kidney model. Int. J. Hyperth. 2004, 20, 567–593. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.V.; Frenchu, K.; Danish, S.F. Does the Thermal Damage Estimate Correlate with the Magnetic Resonance Imaging Predicted Ablation Size after Laser Interstitial Thermal Therapy? Neurosurgery 2018, 15, 179–183. [Google Scholar] [CrossRef]
- Schutt, D.J.; Haemmerich, D. Effects of variation in perfusion rates and of perfusion models in computational models of radio frequency tumor ablation. Med. Phys. 2008, 35, 3462–3470. [Google Scholar] [CrossRef] [PubMed]
- Kandala, S.K.; Liapi, E.; Whitcomb, L.L.; Attaluri, A.; Ivkov, R. Temperature-controlled power modulation compensates for heterogeneous nanoparticle distribu-tions: A computational optimization analysis for magnetic hyperthermia. Int. J. Hyperth. 2019, 36, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Schwarzmaier, H.-J.; Yaroslavsky, I.V.; Yaroslavsky, A.N.; Fiedler, V.; Ulrich, F.; Kahn, T. Treatment planning for MRI-guided laser-induced interstitial thermotherapy of brain tumors—The role of blood perfusion. J. Magn. Reson. Imaging 1998, 8, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, A.M.; Schroeder, J.L. Laser interstitial thermal therapy in treatment of brain tumors—The NeuroBlate System. Expert Rev. Med. Devices 2014, 11, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.V.; Mian, M.; Stafford, R.J.; Nahed, B.V.; Willie, J.T.; Gross, R.E.; Danish, S.F. Laser interstitial thermal therapy tech-nology, physics of magnetic resonance imaging thermometry, and technical considerations for proper catheter placement during magnetic resonance imaging–guided laser interstitial thermal therapy. Neurosurgery 2016, 79, S8–S16. [Google Scholar] [CrossRef] [PubMed]
- Scutigliani, E.M.; Liang, Y.; Crezee, H.; Kanaar, R.; Krawczyk, P.M. Modulating the Heat Stress Response to Improve Hy-perthermia-Based Anticancer Treatments. Cancers 2021, 13, 1243. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.-K.; Chung, B.-J. Natural convection experiments on the upward and downward faces of inclined plates using an electroplating system. Heat Mass Transf. 2015, 51, 713–722. [Google Scholar] [CrossRef]
- Nellis, G.F.; Klein, S.A. Introduction to Engineering Heat Transfer; Cambridge University Press: Cambridge, MA, USA, 2020. [Google Scholar] [CrossRef]
- Balasundaram, H.; Sathiamoorthy, S.; Santra, S.S.; Ali, R.; Govindan, V.; Dreglea, A.; Noeiaghdam, S. Effect of Ventricular Elasticity Due to Congenital Hydrocephalus. Symmetry 2021, 13, 2087. [Google Scholar] [CrossRef]
- Casali, C.; Del Bene, M.; Messina, G.; Legnani, F.; DiMeco, F. Robot assisted laser-interstitial thermal therapy with iSYS1 and Visualase: How I do it. Acta Neurochir. 2021, 163, 3465–3471. [Google Scholar] [CrossRef]
- Bischoff, J. Asme VVUQ 40 Verification, Validation, and Uncertainty Quantification in Computa-Tional Modeling of Medical Devices. Available online: https://cstools.asme.org/csconnect/CommitteePages.cfm?Committee=100108782 (accessed on 17 August 2023).
- Vincelette, R.L.; Curran, M.P.; Danish, S.F.; Grissom, W.A. Appearance and modeling of bubble artifacts in intracranial magnetic resonance-guided laser interstitial thermal therapy (MRg-LITT) temperature images. Magn. Reson. Imaging 2023, 101, 67–75. [Google Scholar] [CrossRef]
- Desclides, M.; Ozenne, V.; Bour, P.; Faller, T.; Machinet, G.; Pierre, C.; Chemouny, S.; Quesson, B. Real-time automatic tem-perature regulation during in vivo MRI-guided laser-induced thermotherapy (MR-LITT). Sci. Rep. 2023, 13, 3297. [Google Scholar] [CrossRef]
- Palussière, J.; Salomir, R.; Le Bail, B.; Fawaz, R.; Quesson, B.; Grenier, N.; Moonen, C.T. Feasibility of MR-guided focused ultrasound with real-time temperature mapping and continuous sonication for ablation of VX2 carcinoma in rabbit thigh. Magn. Reson. Med. 2003, 49, 89–98. [Google Scholar] [CrossRef]
- Carlton, H.; Ivkov, R. A new method to measure magnetic nanoparticle heating efficiency in non-adiabatic systems using transient pulse analysis. J. Appl. Phys. 2023, 133, 044302. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Part | Heat Capacity at Constant Pressure,
| Density, | Thermal Conductivity,
| Dynamic Viscosity,
| Velocity,
| Refs. |
|---|---|---|---|---|---|---|
| Brain (grey & white matter) | 3630 | 1046 | 0.51 | - | - | [32,33,34] |
| Tumor | 3700 | 1056 | 0.57 | - | - | [32,33,34] |
| CSF (general and ventricles) | 4096 | 1007 | 0.62 | 7.84 × 10−4 | 0.08 | [30,32] |
| Laser Probe | 750 | 2200 | 1.38 | - | - | [35] |
| Blood | 3617 | 1050 | 0.52 | 3.65 × 10−4 | 1.5 × 10−3 | [32,33,34] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lad, Y.; Jangam, A.; Carlton, H.; Abu-Ayyad, M.; Hadjipanayis, C.; Ivkov, R.; Zacharia, B.E.; Attaluri, A. Development of a Treatment Planning Framework for Laser Interstitial Thermal Therapy (LITT). Cancers 2023, 15, 4554. https://doi.org/10.3390/cancers15184554
Lad Y, Jangam A, Carlton H, Abu-Ayyad M, Hadjipanayis C, Ivkov R, Zacharia BE, Attaluri A. Development of a Treatment Planning Framework for Laser Interstitial Thermal Therapy (LITT). Cancers. 2023; 15(18):4554. https://doi.org/10.3390/cancers15184554
Chicago/Turabian StyleLad, Yash, Avesh Jangam, Hayden Carlton, Ma’Moun Abu-Ayyad, Constantinos Hadjipanayis, Robert Ivkov, Brad E. Zacharia, and Anilchandra Attaluri. 2023. "Development of a Treatment Planning Framework for Laser Interstitial Thermal Therapy (LITT)" Cancers 15, no. 18: 4554. https://doi.org/10.3390/cancers15184554