
Role of IL-17A and IL-17RA in Prostate Cancer with Lymph Nodes Metastasis: Expression Patterns and Clinical Significance
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Selection
2.2. Tissue Microarrays (TMAs) and Immunohistochemical (IHC) Staining
2.3. Statistical Analysis
3. Results
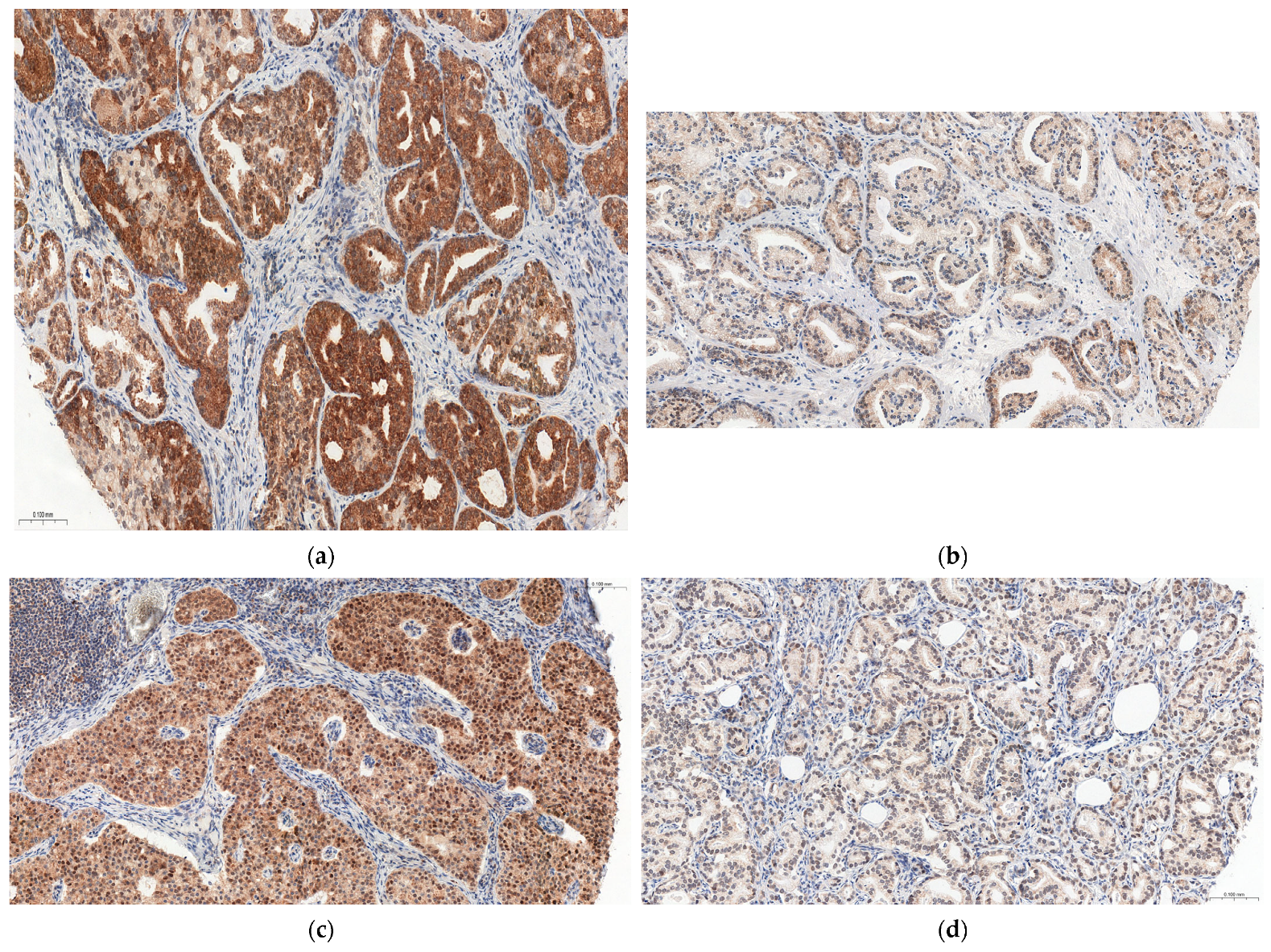
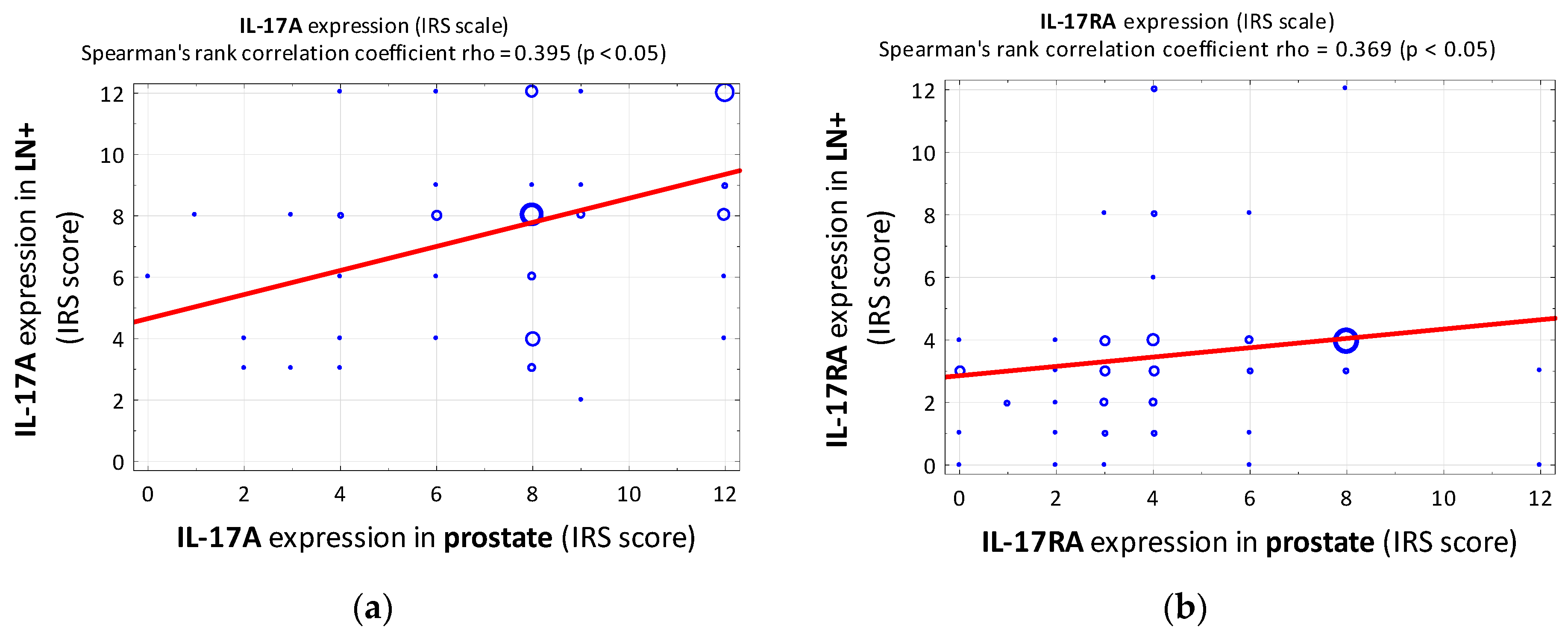
3.1. IL-17A
3.2. IL-17RA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| EAU | European Association of Urology |
| ECE | extracapsular extension |
| EMT | epithelial-to-mesenchymal transition |
| GGG ISUP | International Society of Urological Pathology grade (group) system |
| HE | hematoxylin and eosin |
| IHC | immunohistochemistry |
| IL | interleukin |
| IRS | immunoreactive scale |
| LN+ | metastatic/positive lymph node |
| LVI | lymphovascular invasion |
| MMP7 | matrix metalloproteinase 7 |
| MSKCC | Memorial Sloan Kettering Cancer Center |
| NVI | neurovascular invasion |
| PCa | prostate cancer |
| PIN | prostatic intraepithelial neoplasia |
| PSA | prostate-specific antigen |
| pT | pathological tumor stage |
| RP | radical prostatectomy |
| TMA | tissue microarray |
| TURP | transurethral resection of the prostate |
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer Incidence and Mortality Worldwide: Sources, Methods and Major Patterns in GLOBOCAN 2012: Globocan 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [PubMed]
- Van Baelen, A.; Mottet, N.; Spahn, M.; Briganti, A.; Gontero, P.; Joniau, S. Sense and Nonsense of an Extended Pelvic Lymph Node Dissection in Prostate Cancer. Adv. Urol. 2012, 2012, 983058. [Google Scholar] [CrossRef]
- Allaf, M.E.; Palapattu, G.S.; Trock, B.J.; Carter, H.B.; Walsh, P.C. Anatomical Extent of Lymph Node Dissection: Impact on Men with Clinically Localized Prostate Cancer. J. Urol. 2004, 172, 1840–1844. [Google Scholar] [CrossRef]
- Stabile, A.; Pellegrino, A.; Mazzone, E.; Cannoletta, D.; de Angelis, M.; Barletta, F.; Scuderi, S.; Cucchiara, V.; Gandaglia, G.; Raggi, D.; et al. Can Negative Prostate-Specific Membrane Antigen Positron Emission Tomography/Computed Tomography Avoid the Need for Pelvic Lymph Node Dissection in Newly Diagnosed Prostate Cancer Patients? A Systematic Review and Meta-Analysis with Backup Histology as Reference Standard. Eur. Urol. Oncol. 2022, 5, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Hövels, A.M.; Heesakkers, R.A.M.; Adang, E.M.; Jager, G.J.; Strum, S.; Hoogeveen, Y.L.; Severens, J.L.; Barentsz, J.O. The Diagnostic Accuracy of CT and MRI in the Staging of Pelvic Lymph Nodes in Patients with Prostate Cancer: A Meta-Analysis. Clin. Radiol. 2008, 63, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Fossati, N.; Willemse, P.-P.M.; Van den Broeck, T.; van den Bergh, R.C.N.; Yuan, C.Y.; Briers, E.; Bellmunt, J.; Bolla, M.; Cornford, P.; De Santis, M.; et al. The Benefits and Harms of Different Extents of Lymph Node Dissection During Radical Prostatectomy for Prostate Cancer: A Systematic Review. Eur. Urol. 2017, 72, 84–109. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Ohshima, H.; Bartsch, H. Chronic Infections and Inflammatory Processes as Cancer Risk Factors: Possible Role of Nitric Oxide in Carcinogenesis. Mutat. Res. 1994, 305, 253–264. [Google Scholar] [CrossRef]
- Lonkar, P.; Dedon, P.C. Reactive Species and DNA Damage in Chronic Inflammation: Reconciling Chemical Mechanisms and Biological Fates. Int. J. Cancer 2011, 128, 1999–2009. [Google Scholar] [CrossRef]
- Schetter, A.J.; Heegaard, N.H.H.; Harris, C.C. Inflammation and Cancer: Interweaving MicroRNA, Free Radical, Cytokine and P53 Pathways. Carcinogenesis 2010, 31, 37–49. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and Cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Jung, G.; Kim, J.K.; Kim, H.; Lee, J.; Hong, S.K. The Association between Prostatitis and Risk of Prostate Cancer: A National Health Insurance Database Study. World J. Urol. 2022, 40, 2781–2787. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Li, J.; Yunxia, Z.; Zhu, H.; Liu, J.; Pumill, C. The Role of Prostatitis in Prostate Cancer: Meta-Analysis. PLoS ONE 2013, 8, e85179. [Google Scholar] [CrossRef] [PubMed]
- Sutcliffe, S.; Giovannucci, E.; De Marzo, A.M.; Leitzmann, M.F.; Willett, W.C.; Platz, E.A. Gonorrhea, Syphilis, Clinical Prostatitis, and the Risk of Prostate Cancer. Cancer Epidemiol. Biomark. Prev. 2006, 15, 2160–2166. [Google Scholar] [CrossRef]
- Gurel, B.; Lucia, M.S.; Thompson, I.M.; Goodman, P.J.; Tangen, C.M.; Kristal, A.R.; Parnes, H.L.; Hoque, A.; Lippman, S.M.; Sutcliffe, S.; et al. Chronic Inflammation in Benign Prostate Tissue Is Associated with High-Grade Prostate Cancer in the Placebo Arm of the Prostate Cancer Prevention Trial. Cancer Epidemiol. Biomark. Prev. 2014, 23, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Platz, E.A.; Yegnasubramanian, S.; De Marzo, A.M.; Nelson, W.G. Anti-Inflammatory Drugs, Antioxidants, and Prostate Cancer Prevention. Curr. Opin. Pharmacol. 2009, 9, 419–426. [Google Scholar] [CrossRef]
- Thapa, D.; Ghosh, R. Antioxidants for Prostate Cancer Chemoprevention: Challenges and Opportunities. Biochem. Pharmacol. 2012, 83, 1319–1330. [Google Scholar] [CrossRef]
- Kiełb, P.; Kowalczyk, K.; Gurwin, A.; Nowak, Ł.; Krajewski, W.; Sosnowski, R.; Szydełko, T.; Małkiewicz, B. Novel Histopathological Biomarkers in Prostate Cancer: Implications and Perspectives. Biomedicines 2023, 11, 1552. [Google Scholar] [CrossRef]
- Onishi, R.M.; Gaffen, S.L. Interleukin-17 and Its Target Genes: Mechanisms of Interleukin-17 Function in Disease. Immunology 2010, 129, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Liu, S.; Parajuli, K.R.; Zhang, W.; Zhang, K.; Mo, Z.; Liu, J.; Chen, Z.; Yang, S.; Wang, A.R.; et al. Interleukin-17 Promotes Prostate Cancer via MMP7-Induced Epithelial-to-Mesenchymal Transition. Oncogene 2017, 36, 687–699. [Google Scholar] [CrossRef] [PubMed]
- Pappu, R.; Ramirez-Carrozzi, V.; Sambandam, A. The Interleukin-17 Cytokine Family: Critical Players in Host Defence and Inflammatory Diseases. Immunology 2011, 134, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Steiner, G.E.; Newman, M.E.; Paikl, D.; Stix, U.; Memaran-Dagda, N.; Lee, C.; Marberger, M.J. Expression and Function of Pro-Inflammatory Interleukin IL-17 and IL-17 Receptor in Normal, Benign Hyperplastic, and Malignant Prostate. Prostate 2003, 56, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Haudenschild, D.; Moseley, T.; Rose, L.; Reddi, A.H. Soluble and Transmembrane Isoforms of Novel Interleukin-17 Receptor-like Protein by RNA Splicing and Expression in Prostate Cancer. J. Biol. Chem. 2002, 277, 4309–4316. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhao, X.; Sun, X.; Li, Y.; Wang, Z.; Jiang, J.; Han, H.; Shen, W.; Corrigan, C.J.; Sun, Y. Expression of IL-17A, E, and F and Their Receptors in Human Prostatic Cancer: Comparison with Benign Prostatic Hyperplasia. Prostate 2015, 75, 1844–1856. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, S.; Ge, D.; Zhang, Q.; Xue, Y.; Xiong, Z.; Abdel-Mageed, A.B.; Myers, L.; Hill, S.M.; Rowan, B.G.; et al. Interleukin-17 Promotes Formation and Growth of Prostate Adenocarcinoma in Mouse Models. Cancer Res. 2012, 72, 2589–2599. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, S.; Zhang, Q.; Xiong, Z.; Wang, A.R.; Myers, L.; Melamed, J.; Tang, W.W.; You, Z. Interleukin-17 Promotes Development of Castration-Resistant Prostate Cancer Potentially through Creating an Immunotolerant and pro-Angiogenic Tumor Microenvironment. Prostate 2014, 74, 869–879. [Google Scholar] [CrossRef]
- Cunningham, D.; Zhang, Q.; Liu, S.; Parajuli, K.R.; Nie, Q.; Ma, L.; Zhang, A.; Chen, Z.; You, Z. Interleukin-17 Promotes Metastasis in an Immunocompetent Orthotopic Mouse Model of Prostate Cancer. Am. J. Clin. Exp. Urol. 2018, 6, 114–122. [Google Scholar]
- Janiczek, M.; Szylberg, Ł.; Antosik, P.; Kasperska, A.; Marszałek, A. Expression Levels of IL-17A, IL-17F, IL-17RA, and IL-17RC in Prostate Cancer with Taking into Account the Histological Grade According to Gleason Scale in Comparison to Benign Prostatic Hyperplasia: In Search of New Therapeutic Options. J. Immunol. Res. 2020, 2020, 4910595. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]
- Kaemmerer, D.; Peter, L.; Lupp, A.; Schulz, S.; Sänger, J.; Baum, R.P.; Prasad, V.; Hommann, M. Comparing of IRS and Her2 as Immunohistochemical Scoring Schemes in Gastroenteropancreatic Neuroendocrine Tumors. Int. J. Clin. Exp. Pathol. 2012, 5, 187–194. [Google Scholar]
- Moussa, A.S.; Li, J.; Soriano, M.; Klein, E.A.; Dong, F.; Jones, J.S. Prostate Biopsy Clinical and Pathological Variables That Predict Significant Grading Changes in Patients with Intermediate and High Grade Prostate Cancer. BJU Int. 2009, 103, 43–48. [Google Scholar] [CrossRef]
- Hyun, Y.S.; Han, D.S.; Lee, A.R.; Eun, C.S.; Youn, J.; Kim, H.-Y. Role of IL-17A in the Development of Colitis-Associated Cancer. Carcinogenesis 2012, 33, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yi, T.; Zhang, W.; Pardoll, D.M.; Yu, H. IL-17 Enhances Tumor Development in Carcinogen-Induced Skin Cancer. Cancer Res. 2010, 70, 10112–10120. [Google Scholar] [CrossRef]
- Jarocki, M.; Karska, J.; Kowalski, S.; Kiełb, P.; Nowak, Ł.; Krajewski, W.; Saczko, J.; Kulbacka, J.; Szydełko, T.; Małkiewicz, B. Interleukin 17 and Its Involvement in Renal Cell Carcinoma. J. Clin. Med. 2022, 11, 4973. [Google Scholar] [CrossRef] [PubMed]
- Benatar, T.; Cao, M.Y.; Lee, Y.; Li, H.; Feng, N.; Gu, X.; Lee, V.; Jin, H.; Wang, M.; Der, S.; et al. Virulizin Induces Production of IL-17E to Enhance Antitumor Activity by Recruitment of Eosinophils into Tumors. Cancer Immunol. Immunother. 2008, 57, 1757–1769. [Google Scholar] [CrossRef]
- Chen, L.; Deng, H.; Cui, H.; Fang, J.; Zuo, Z.; Deng, J.; Li, Y.; Wang, X.; Zhao, L. Inflammatory Responses and Inflammation-Associated Diseases in Organs. Oncotarget 2017, 9, 7204–7218. [Google Scholar] [CrossRef]
- Berraondo, P.; Sanmamed, M.F.; Ochoa, M.C.; Etxeberria, I.; Aznar, M.A.; Pérez-Gracia, J.L.; Rodríguez-Ruiz, M.E.; Ponz-Sarvise, M.; Castañón, E.; Melero, I. Cytokines in Clinical Cancer Immunotherapy. Br. J. Cancer 2019, 120, 6–15. [Google Scholar] [CrossRef]
- Locy, H.; de Mey, S.; de Mey, W.; De Ridder, M.; Thielemans, K.; Maenhout, S.K. Immunomodulation of the Tumor Microenvironment: Turn Foe Into Friend. Front. Immunol. 2018, 9, 2909. [Google Scholar] [CrossRef]
- Chen, K.; Kolls, J.K. Interluekin-17A (IL17A). Gene 2017, 614, 8–14. [Google Scholar] [CrossRef]
- Yan, R.; Dai, W.; Mao, Y.; Yu, G.; Li, W.; Shu, M.; Xu, B. Melittin Inhibits Tumor Cell Migration and Enhances Cisplatin Sensitivity by Suppressing IL-17 Signaling Pathway Gene LCN2 in Castration-Resistant Prostate Cancer. Prostate 2023, 1–16. [Google Scholar] [CrossRef]
- McDowell, K.L.; Begley, L.A.; Mor-Vaknin, N.; Markovitz, D.M.; Macoska, J.A. Leukocytic Promotion of Prostate Cellular Proliferation. Prostate 2010, 70, 377–389. [Google Scholar] [CrossRef] [PubMed]
- De Marzo, A.M.; Platz, E.A.; Sutcliffe, S.; Xu, J.; Grönberg, H.; Drake, C.G.; Nakai, Y.; Isaacs, W.B.; Nelson, W.G. Inflammation in Prostate Carcinogenesis. Nat. Rev. Cancer 2007, 7, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Bardan, R.; Dumache, R.; Dema, A.; Cumpanas, A.; Bucuras, V. The Role of Prostatic Inflammation Biomarkers in the Diagnosis of Prostate Diseases. Clin. Biochem. 2014, 47, 909–915. [Google Scholar] [CrossRef]
- Stark, T.; Livas, L.; Kyprianou, N. Inflammation in Prostate Cancer Progression and Therapeutic Targeting. Transl. Androl. Urol. 2015, 4, 455–463. [Google Scholar] [CrossRef]
- Liu, S.; Zhang, Q.; Chen, C.; Ge, D.; Qu, Y.; Chen, R.; Fan, Y.-M.; Li, N.; Tang, W.W.; Zhang, W.; et al. Hyperinsulinemia Enhances Interleukin-17-Induced Inflammation to Promote Prostate Cancer Development in Obese Mice through Inhibiting Glycogen Synthase Kinase 3-Mediated Phosphorylation and Degradation of Interleukin-17 Receptor. Oncotarget 2016, 7, 13651–13666. [Google Scholar] [CrossRef]
- Khanna, D.; Khanna, S.; Khanna, P.; Kahar, P.; Patel, B.M. Obesity: A Chronic Low-Grade Inflammation and Its Markers. Cureus 2022, 14, e22711. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and Inflammation: The Linking Mechanism and the Complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef]
- Cohen, E.; Margalit, I.; Shochat, T.; Goldberg, E.; Krause, I. Markers of Chronic Inflammation in Overweight and Obese Individuals and the Role of Gender: A Cross-Sectional Study of a Large Cohort. J. Inflamm. Res. 2021, 14, 567–573. [Google Scholar] [CrossRef]
- Briganti, A.; Larcher, A.; Abdollah, F.; Capitanio, U.; Gallina, A.; Suardi, N.; Bianchi, M.; Sun, M.; Freschi, M.; Salonia, A.; et al. Updated Nomogram Predicting Lymph Node Invasion in Patients with Prostate Cancer Undergoing Extended Pelvic Lymph Node Dissection: The Essential Importance of Percentage of Positive Cores. Eur. Urol. 2012, 61, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Fossati, N.; Zaffuto, E.; Bandini, M.; Dell’Oglio, P.; Bravi, C.A.; Fallara, G.; Pellegrino, F.; Nocera, L.; Karakiewicz, P.I.; et al. Development and Internal Validation of a Novel Model to Identify the Candidates for Extended Pelvic Lymph Node Dissection in Prostate Cancer. Eur. Urol. 2017, 72, 632–640. [Google Scholar] [CrossRef] [PubMed]
- Cimino, S.; Reale, G.; Castelli, T.; Favilla, V.; Giardina, R.; Russo, G.I.; Privitera, S.; Morgia, G. Comparison between Briganti, Partin and MSKCC Tools in Predicting Positive Lymph Nodes in Prostate Cancer: A Systematic Review and Meta-Analysis. Scand. J. Urol. 2017, 51, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Małkiewicz, B.; Ptaszkowski, K.; Knecht, K.; Gurwin, A.; Wilk, K.; Kiełb, P.; Dudek, K.; Zdrojowy, R. External Validation of the Briganti Nomogram to Predict Lymph Node Invasion in Prostate Cancer-Setting a New Threshold Value. Life 2021, 11, 479. [Google Scholar] [CrossRef] [PubMed]
- Gandaglia, G.; Ploussard, G.; Valerio, M.; Mattei, A.; Fiori, C.; Fossati, N.; Stabile, A.; Beauval, J.-B.; Malavaud, B.; Roumiguié, M.; et al. A Novel Nomogram to Identify Candidates for Extended Pelvic Lymph Node Dissection Among Patients with Clinically Localized Prostate Cancer Diagnosed with Magnetic Resonance Imaging-Targeted and Systematic Biopsies. Eur. Urol. 2019, 75, 506–514. [Google Scholar] [CrossRef]
- Suardi, N.; Ficarra, V.; Willemsen, P.; De Wil, P.; Gallina, A.; De Naeyer, G.; Schatteman, P.; Montorsi, F.; Carpentier, P.; Mottrie, A. Long-Term Biochemical Recurrence Rates After Robot-Assisted Radical Prostatectomy: Analysis of a Single-Center Series of Patients With a Minimum Follow-up of 5 Years. Urology 2012, 79, 133–138. [Google Scholar] [CrossRef]
- Detre, S.; Saclani Jotti, G.; Dowsett, M. A “Quickscore” Method for Immunohistochemical Semiquantitation: Validation for Oestrogen Receptor in Breast Carcinomas. J. Clin. Pathol. 1995, 48, 876–878. [Google Scholar] [CrossRef]
- Fedchenko, N.; Reifenrath, J. Different Approaches for Interpretation and Reporting of Immunohistochemistry Analysis Results in the Bone Tissue—A Review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Immunoreactive Scale (IRS) | |||
| A—Percentage of Positive Cancer Cells | B—Staining Intensity | ||
| Score | Score | ||
| 0 | no cells with positive reaction | 0 | no color reaction |
| 1 | <10% cells with positive reaction | 1 | mild reaction |
| 2 | 10–50% cells with positive reaction | 2 | moderate reaction |
| 3 | 51–80% cells with positive reaction | 3 | intense reaction |
| 4 | >80% cells with positive reaction | ||
| IRS SCORE (A X B): 0–12 points | |||
| Final score | Level of expression | ||
| 1–7 | Low expression | ||
| 8–12 | High expression | ||
| Variable | Statistics |
|---|---|
| General characteristics of patients | |
| Age (years): | |
| M ± SD | 64.9 ± 5.5 |
| BMI (kg/m2): | |
| M ± SD | 28.1 ± 3.7 |
| Preoperative PSA (ng/mL): | |
| Me (Q1; Q3) | 19.8 (12; 36.1) |
| EAU risk group, n (%): | |
| Low-risk | 1 (1.3) |
| Intermediate-risk | 8 (10.4) |
| High-risk | 38 (49.3) |
| High-risk locally advanced | 30 (39) |
| Clinicopathological parameters | |
| pT, n (%): | |
| 2a | 1 (1.3) |
| 2c | 9 (11.7) |
| 3a | 14 (18.2) |
| 3b | 53 (68.8) |
| Postoperative Gleason, n (%): | |
| 3 + 3 | 1 (1.3) |
| 3 + 4 | 10 (13) |
| 3 + 5 | 4 (5.2) |
| 4 + 3 | 19 (24.7) |
| 4 + 4 | 3 (3.9) |
| 4 + 5 | 29 (37.6) |
| 5 + 3 | 2 (2.6) |
| 5 + 4 | 8 (10.4) |
| 5 + 5 | 1 (1.3) |
| Postoperative GGG ISUP, n (%): | |
| 1 | 1 (1.3) |
| 2 | 10 (13) |
| 3 | 19 (24.7) |
| 4 | 9 (11.7) |
| 5 | 38 (48.3) |
| Extracapsular extension of prostate, n (%): | |
| Yes | 66 (85.7) |
| No | 11 (14.3) |
| Extracapsular extension of lymph node, n (%): | |
| Yes | 19 (24.7) |
| No | 58 (75.3) |
| Resection margin, n (%): | |
| Positive | 54 (70.1) |
| Negative | 23 (29.9) |
| Neurovascular invasion, n (%): | |
| Yes | 70 (90.9) |
| No | 1 (1.3) |
| No data | 6 (7.8) |
| Lymphovascular invasion, n (%): | |
| Yes | 57 (74) |
| No | 15 (19.5) |
| No data | 5 (6.5) |
| Affected lymph nodes (%): | |
| Me (Q1; Q3) | 12.5 (8.3; 27.3) |
| Radical procedure, n (%): | |
| Yes | 36 (46.7) |
| No | 41 (53.3) |
| Expression (IRS Scale) | ||||||
|---|---|---|---|---|---|---|
| IL-17A | IL-17RA | |||||
| Prostate | Metastatic Lymph Node | p-Value | Prostate | Metastatic Lymph Node | p-Value | |
| A—Percentage of positively stained cancer cells (score) | 0.634 | 0.271 | ||||
| Me (Q1; Q3) | 4 [3; 4] | 4 [3; 4] | 3 [3; 4] | 3 [2; 4] | ||
| Min–Max | 0–4 | 2–4 | 0–4 | 0–4 | ||
| B—Intensity of staining (score) | 0.446 | 0.112 | ||||
| Me (Q1; Q3) | 2 [2; 3] | 2 [2; 3] | 1 [1; 2] | 1 [1; 1] | ||
| Min–Max | 0–3 | 1–3 | 0–3 | 0–3 | ||
| IRS score (A × B) | 0.415 | 0.009 | ||||
| Me (Q1; Q3) | 8 [6; 12] | 8 [6; 9] | 4 [3; 6] | 3 [2; 4] | ||
| Min–Max | 0–12 | 2–12 | 0–12 | 0–12 | ||
| Expression level: | 0.308 | 0.012 | ||||
| Low expression (1–7 score), n (%) | 19 (25) | 25 (32.5) | 52 (74.3) | 65 (90.3) | ||
| High expression (8–12 score), n (%) | 57 (75) | 52 (67.5) | 18 (25.7) | 7 (9.7) | ||
| IL-17A | IL-17RA | |||||||
|---|---|---|---|---|---|---|---|---|
| Prostate | Metastatic Lymph Node | Prostate | Metastatic Lymph Node | |||||
| rho | p | rho | p | rho | p | rho | p | |
| Preoperative PSA (ng/mL) | 0.033 | 0.778 | 0.027 | 0.813 | 0.057 | 0.623 | 0.100 | 0.387 |
| Affected lymph nodes (%) | −0.007 | 0.952 | 0.312 | 0.006 | 0.100 | 0.385 | 0.144 | 0.211 |
| Age (years) | −0.037 | 0.752 | −0.037 | 0.749 | 0.047 | 0.682 | 0.019 | 0.873 |
| BMI (kg/m2) | 0.251 | 0.028 | 0.013 | 0.912 | 0.096 | 0.404 | 0.079 | 0.494 |
| EAU risk group | 0.159 | 0.168 | 0.376 | 0.001 | 0.051 | 0.660 | 0.229 | 0.045 |
| Postoperative GGG ISUP | −0.020 | 0.862 | 0.146 | 0.205 | −0.111 | 0.335 | −0.023 | 0.841 |
| IL-17A Expression Level (IRS Score-Based) | |||||||
|---|---|---|---|---|---|---|---|
| Variables | Expression of IL-17A in PROSTATE | Expression of IL-17A in METASTATIC LYMPH NODE | |||||
| Level of Expression | p-Value | Level of Expression | p-Value | ||||
| Low (N = 19) | High (N = 57) | Low (N = 25) | High (N = 52) | ||||
| n (%) | n (%) | n (%) | n (%) | ||||
| pT | 3a and 3b | 15 (79.0%) | 51 (89.5%) | 0.257 | 20 (80.0%) | 47 (90.4%) | 0.279 |
| 2a and 2c | 4 (21.0%) | 6 (10.5%) | 5 (20.0%) | 5 (9.6%) | |||
| ECE of prostate | Yes | 16 (84.2%) | 49 (86.0%) | 1.000 | 18 (72.0%) | 48 (92.3%) | 0.033 |
| No | 3 (15.8%) | 8 (14.0%) | 7 (28.0%) | 4 (7.7%) | |||
| Resection margin | Positive | 11 (57.9%) | 42 (73.7%) | 0.251 | 18 (72.0%) | 36 (69.2%) | 0.986 |
| Negative | 8 (42.1%) | 15 (26.3%) | 7 (28.0%) | 16 (30.8%) | |||
| ECE of lymph node | Yes | 6 (31.6%) | 13 (22.8%) | 0.543 | 3 (12.0%) | 16 (30.8%) | 0.094 |
| No | 13 (68.4%) | 44 (77.2%) | 22 (88.0%) | 36 (69.2%) | |||
| NVI | Yes | 16 (100.0%) | 53 (98.2%) | 1.000 | 20 (95.2%) | 50 (100.0%) | 0.296 |
| No | 0 (0.0%) | 1 (1.8%) | 1 (4.8%) | 0 (0.0%) | |||
| LVI | Yes | 12 (80.0%) | 44 (78.6%) | 1.000 | 16 (69.6%) | 41 (83.7%) | 0.288 |
| No | 3 (20.0%) | 12 (21.4%) | 7 (30.4%) | 8 (16.3%) | |||
| Radical procedure | Yes | 7 (43.8%) | 28 (58.3%) | 0.389 | 12 (57.1%) | 24 (54.5%) | 0.944 |
| No | 9 (56.3%) | 20 (41.7%) | 9 (42.9%) | 20 (45.5%) | |||
| Expression of IL-17A in metastatic lymph node | Low | 8 (42.1%) | 16 (28.1%) | 0.287 | XX | XX | XX |
| High | 11 (57.9%) | 41 (71.9%) | XX | XX | |||
| Expression of IL-17A in prostate | Low | XX | XX | XX | 8 (33.3%) | 11 (21.2%) | 0.178 |
| High | XX | XX | 16 (66.7%) | 41 (78.8%) | |||
| IL-17RA Expression Level (IRS Score-Based) | |||||||
|---|---|---|---|---|---|---|---|
| Variables | Expression of IL-17RA in PROSTATE | Expression of IL-17RA in METASTATIC LYMPH NODE | |||||
| Level of Expression | p-Value | Level of Expression | p-Value | ||||
| Low (N = 52) | High (N = 18) | Low (N = 65) | High (N = 7) | ||||
| n (%) | n (%) | n (%) | n (%) | ||||
| pT | 3a and 3b | 45 (86.5%) | 16 (88.9%) | 1.000 | 57 (87.7%) | 6 (85.7%) | 1.000 |
| 2a and 2c | 7 (13.5%) | 2 (11.1%) | 8 (12.3%) | 1 (14.3%) | |||
| ECE of prostate | Yes | 47 (90.4%) | 14 (77.8%) | 0.222 | 58 (89.2%) | 5 (71.4%) | 0.209 |
| No | 5 (9.6%) | 4 (22.2%) | 7 (10.8%) | 2 (28.6%) | |||
| Resection margin | Positive | 37 (71.2%) | 13 (72.2%) | 1.000 | 45 (69.2%) | 6 (85.7%) | 0.665 |
| Negative | 15 (28.8%) | 5 (27.8%) | 20 (30.8%) | 1 (14.3%) | |||
| ECE of lymph node | Yes | 13 (25.0%) | 3 (16.7%) | 0.745 | 13 (20.0%) | 5 (71.4%) | 0.009 |
| No | 39 (75.0%) | 15 (83.3%) | 52 (80.0%) | 2 (28.6%) | |||
| NVI | Yes | 45 (97.8%) | 18 (100.0%) | 1.000 | 59 (100.0%) | 7 (100.0%) | 1.000 |
| No | 1 (2.2%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |||
| LVI | Yes | 40 (81.6%) | 12 (70.6%) | 0.491 | 48 (80.0%) | 6 (85.7%) | 1.000 |
| No | 9 (18.4%) | 5 (29.4%) | 12 (20.0%) | 1 (14.3%) | |||
| Radical procedure | Yes | 25 (58.1%) | 8 (50.0%) | 0.769 | 31 (57.4%) | 2 (33.3%) | 0.394 |
| No | 18 (41.9%) | 8 (50.0%) | 23 (42.6%) | 4 (66.7%) | |||
| Expression of IL-17RA in metastatic lymph node | Low | 43 (87.8%) | 16 (94.1%) | 0.667 | XX | XX | XX |
| High | 6 (12.2%) | 1 (5.9%) | XX | XX | |||
| Expression of IL-17RA in prostate | Low | XX | XX | XX | 43 (72.9%) | 6 (85.7%) | 0.667 |
| High | XX | XX | 16 (27.1%) | 1 (14.3%) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiełb, P.; Kaczorowski, M.; Kowalczyk, K.; Piotrowska, A.; Nowak, Ł.; Krajewski, W.; Chorbińska, J.; Dudek, K.; Dzięgiel, P.; Hałoń, A.; et al. Role of IL-17A and IL-17RA in Prostate Cancer with Lymph Nodes Metastasis: Expression Patterns and Clinical Significance. Cancers 2023, 15, 4578. https://doi.org/10.3390/cancers15184578
Kiełb P, Kaczorowski M, Kowalczyk K, Piotrowska A, Nowak Ł, Krajewski W, Chorbińska J, Dudek K, Dzięgiel P, Hałoń A, et al. Role of IL-17A and IL-17RA in Prostate Cancer with Lymph Nodes Metastasis: Expression Patterns and Clinical Significance. Cancers. 2023; 15(18):4578. https://doi.org/10.3390/cancers15184578
Chicago/Turabian StyleKiełb, Paweł, Maciej Kaczorowski, Kamil Kowalczyk, Aleksandra Piotrowska, Łukasz Nowak, Wojciech Krajewski, Joanna Chorbińska, Krzysztof Dudek, Piotr Dzięgiel, Agnieszka Hałoń, and et al. 2023. "Role of IL-17A and IL-17RA in Prostate Cancer with Lymph Nodes Metastasis: Expression Patterns and Clinical Significance" Cancers 15, no. 18: 4578. https://doi.org/10.3390/cancers15184578