
Development and Validation of a Nomogram for Preoperative Prediction of Early Recurrence after Upfront Surgery in Pancreatic Ductal Adenocarcinoma by Integrating Deep Learning and Radiological Variables
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcomes and Data Collection
2.3. CT Acquisition and Image Processing
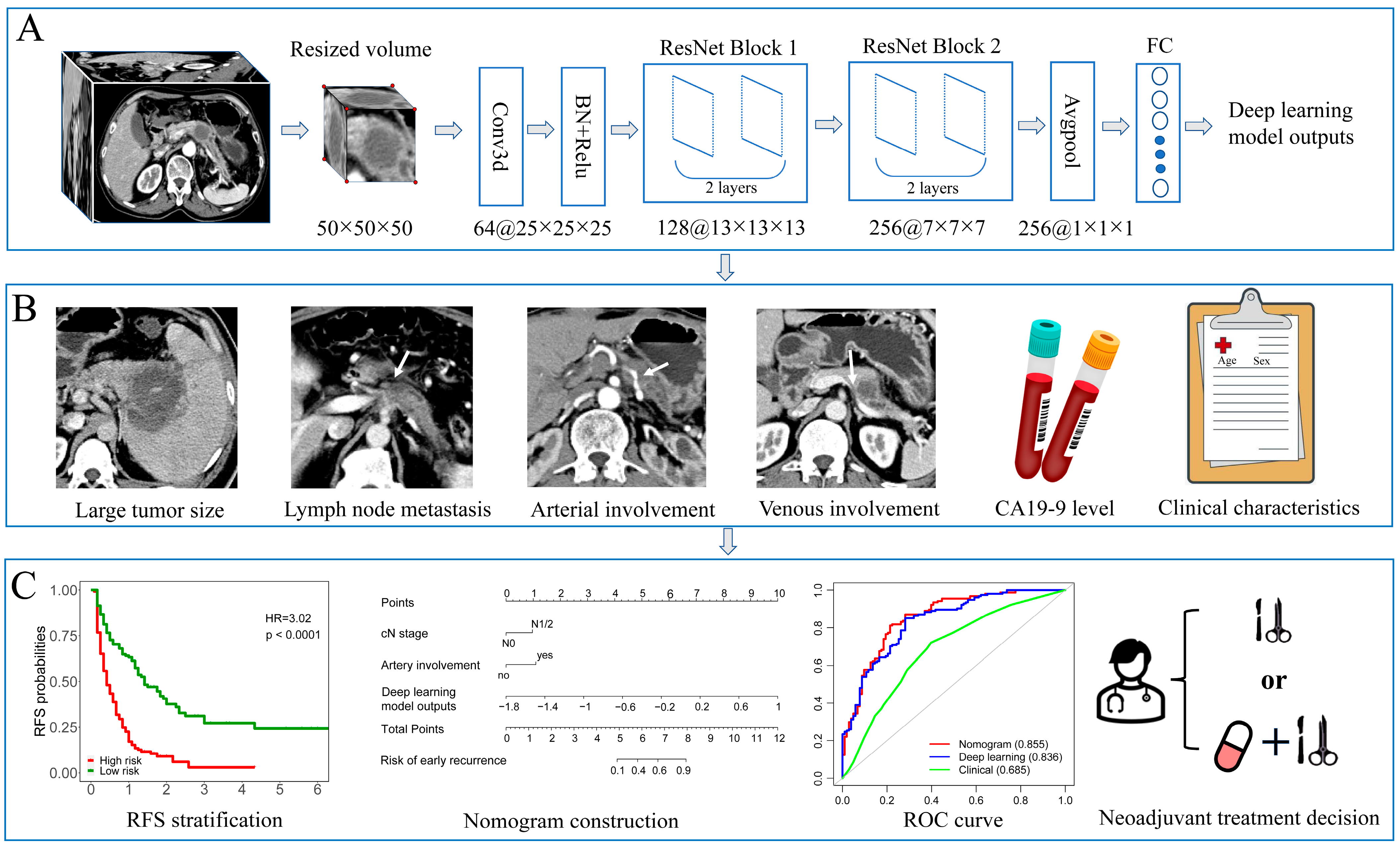
2.4. Deep Learning Model Development
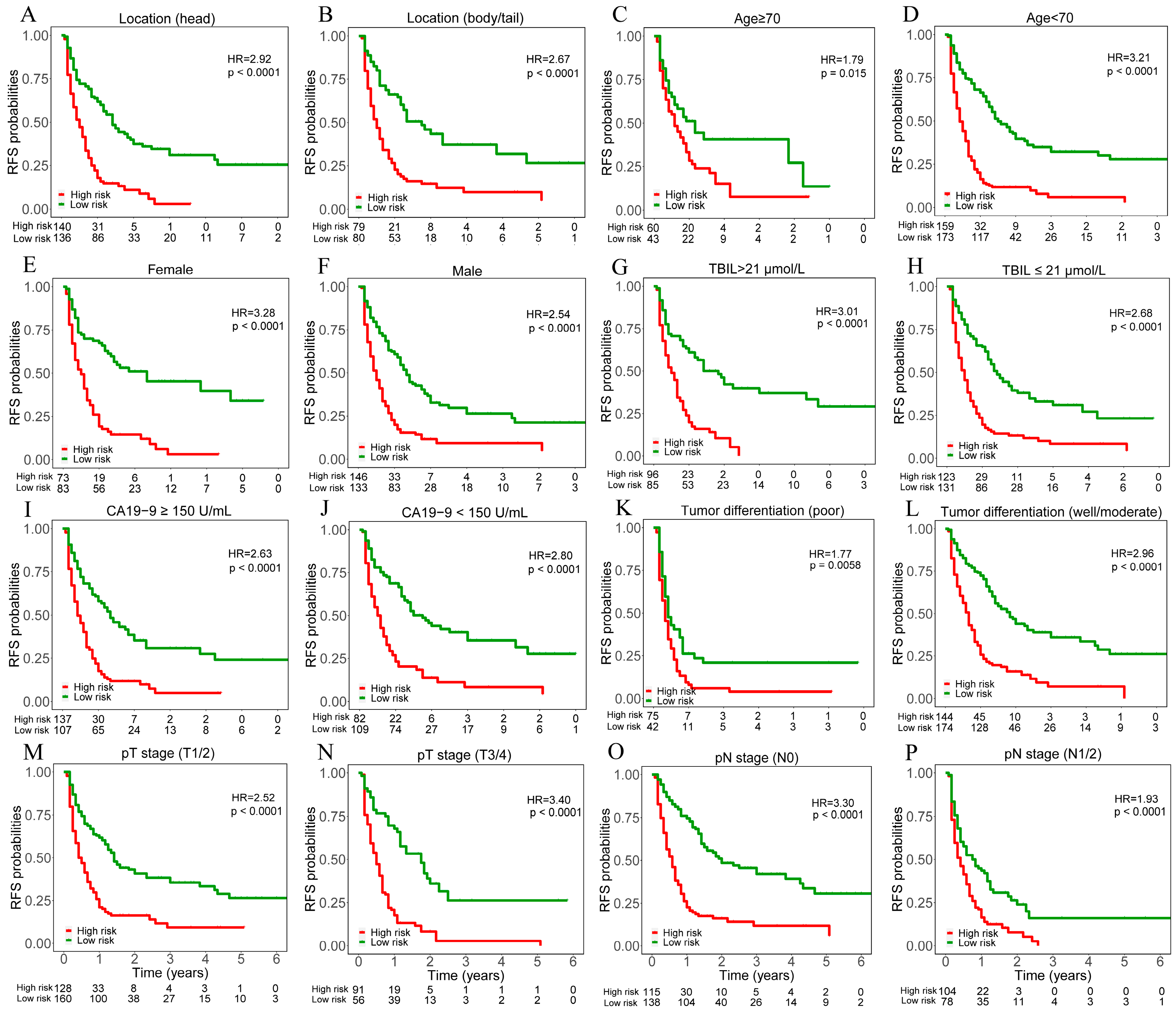
2.5. Performance Evaluation in Different Subgroups
2.6. Nomogram and Clinical Model Construction
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
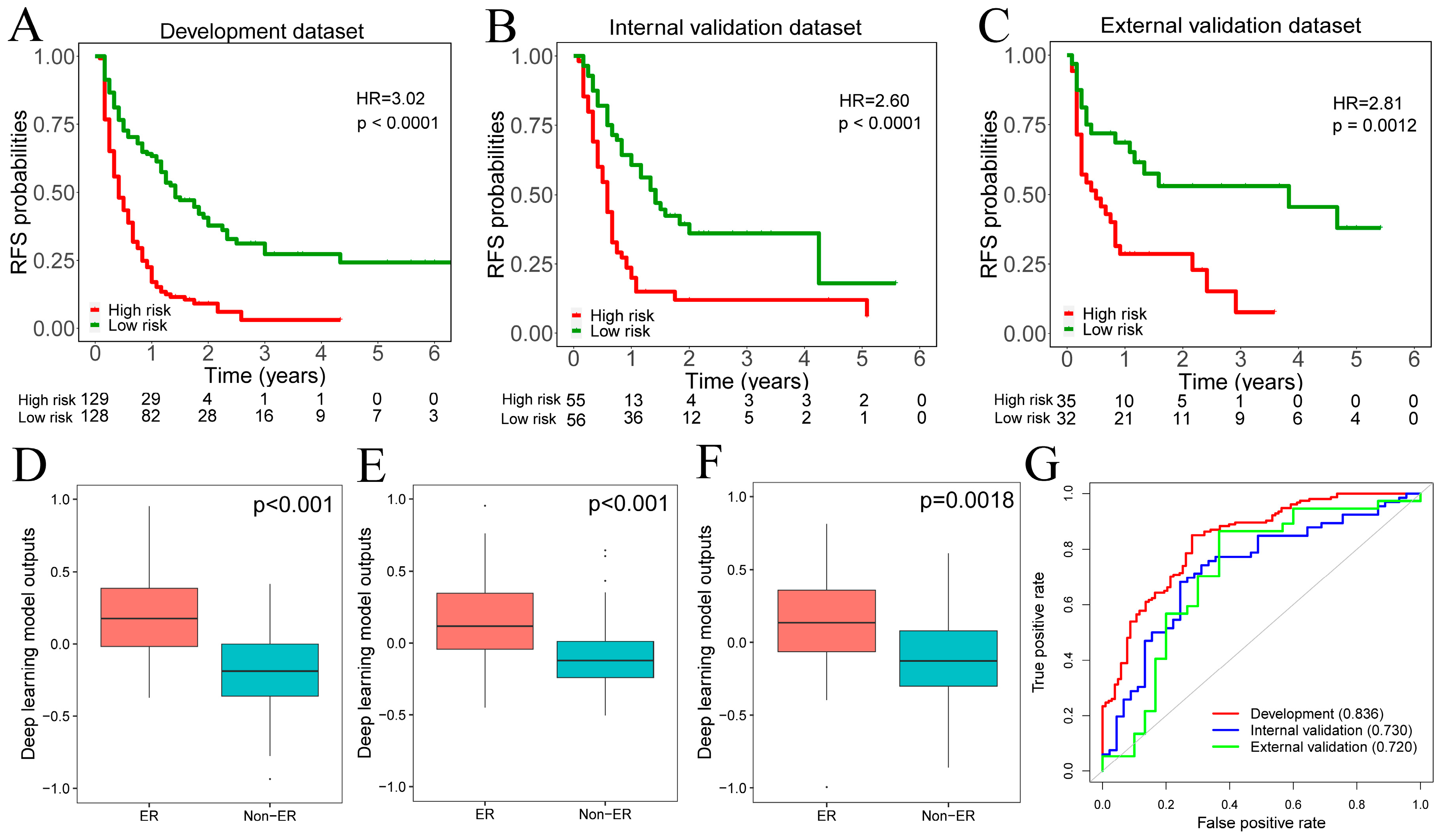
3.2. Development and Validation of Deep Learning Model
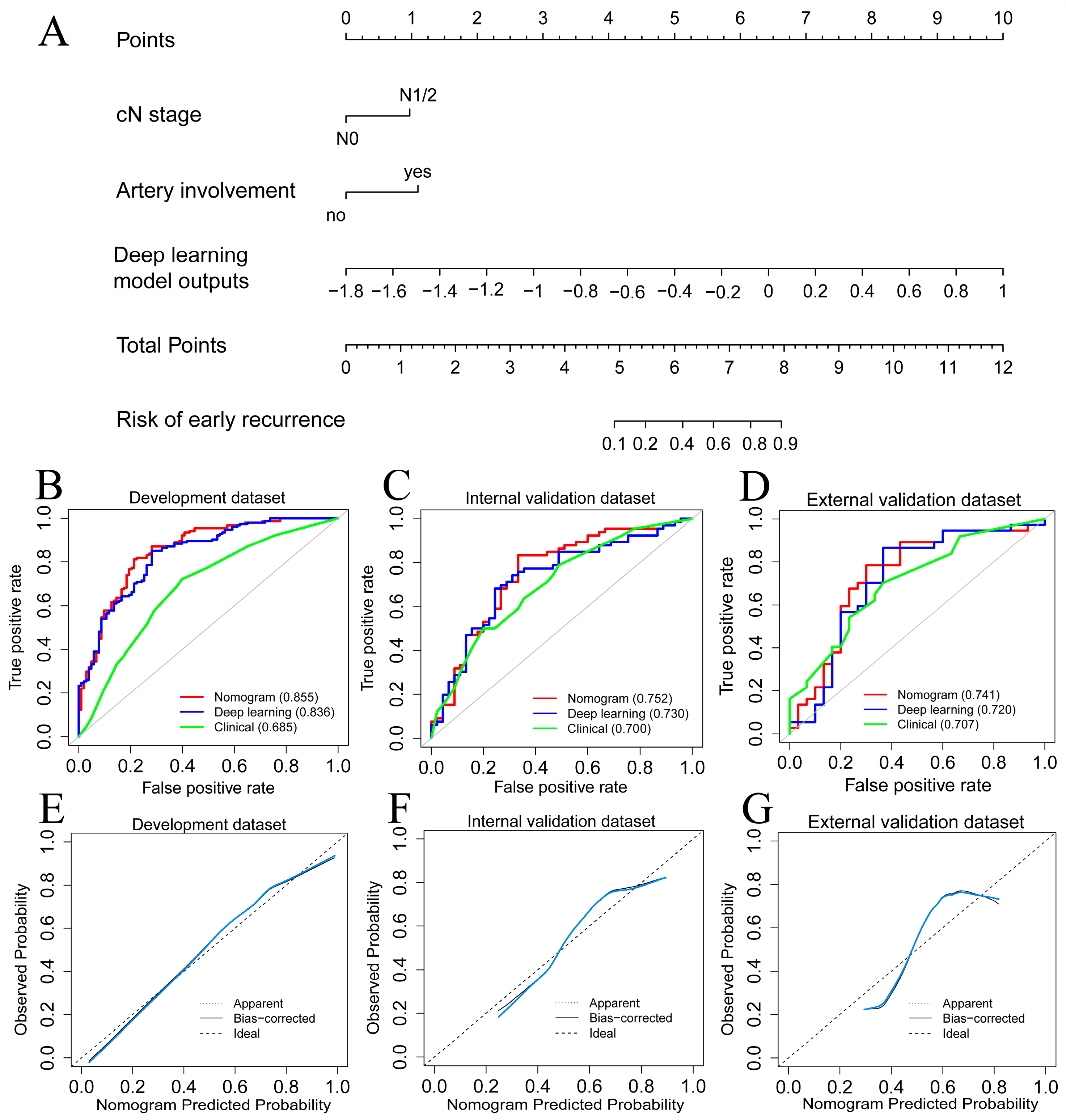
3.3. Nomogram and Clinical Modeling
3.4. Model Performance Comparison
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, C.; Gao, F.; Li, Q.; Liu, Q.; Lin, X. The distributional characteristic and growing trend of pancreatic cancer in China. Pancreas 2019, 48, 309–314. [Google Scholar] [CrossRef]
- Daamen, L.A.; Dorland, G.; Brada, L.J.H.; Groot, V.P.; van Oosten, A.F.; Besselink, M.G.; Bosscha, K.; Bonsing, B.A.; Busch, O.R.; Cirkel, G.A.; et al. Preoperative predictors for early and very early disease recurrence in patients undergoing resection of pancreatic ductal adenocarcinoma. HPB 2022, 24, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Groot, V.P.; Gemenetzis, G.; Blair, A.B.; Rivero-Soto, R.J.; Yu, J.; Javed, A.A.; Burkhart, R.A.; Rinkes, I.; Molenaar, I.Q.; Cameron, J.L.; et al. Defining and predicting early recurrence in 957 patients with resected pancreatic ductal adenocarcinoma. Ann. Surg. 2019, 269, 1154–1162. [Google Scholar] [CrossRef]
- Seelen, L.W.F.; Floortje van Oosten, A.; Brada, L.J.H.; Groot, V.P.; Daamen, L.A.; Walma, M.S.; van der Lek, B.F.; Liem, M.S.L.; Patijn, G.A.; Stommel, M.W.J.; et al. Early recurrence after resection of locally advanced pancreatic cancer following induction therapy: An international multicenter study. Ann. Surg. 2022, 278, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Barenboim, A.; Lahat, G.; Geva, R.; Nachmany, I.; Nakache, R.; Goykhman, Y.; Brazowski, E.; Rosen, G.; Isakov, O.; Wolf, I.; et al. Neoadjuvant FOLFIRINOX for locally advanced and borderline resectable pancreatic cancer: An intention to treat analysis. Eur. J. Surg. Oncol. 2018, 44, 1619–1623. [Google Scholar] [CrossRef]
- Ghaneh, P.; Palmer, D.; Cicconi, S.; Jackson, R.; Halloran, C.M.; Rawcliffe, C.; Sripadam, R.; Mukherjee, S.; Soonawalla, Z.; Wadsley, J.; et al. Immediate surgery compared with short-course neoadjuvant gemcitabine plus capecitabine, FOLFIRINOX, or chemoradiotherapy in patients with borderline resectable pancreatic cancer (ESPAC5): A four-arm, multicentre, randomised, phase 2 trial. Lancet Gastroenterol. Hepatol. 2022, 8, 157–168. [Google Scholar] [CrossRef]
- Lim, J.E.; Chien, M.W.; Earle, C.C. Prognostic factors following curative resection for pancreatic adenocarcinoma: A population-based, linked database analysis of 396 patients. Ann. Surg. 2003, 237, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.F.; Kattan, M.W.; Klimstra, D.; Conlon, K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann. Surg. 2004, 240, 293–298. [Google Scholar] [CrossRef]
- Yoon, S.J.; Shin, S.H.; Yoon, S.K.; Jung, J.H.; You, Y.; Han, I.W.; Choi, D.W.; Heo, J.S. Appraisal of 5-year recurrence-free survival after surgery in pancreatic ductal adenocarcinoma. J. Hepatobiliary Pancreat. Sci. 2021, 28, 287–296. [Google Scholar] [CrossRef]
- Matsumoto, I.; Murakami, Y.; Shinzeki, M.; Asari, S.; Goto, T.; Tani, M.; Motoi, F.; Uemura, K.; Sho, M.; Satoi, S.; et al. Proposed preoperative risk factors for early recurrence in patients with resectable pancreatic ductal adenocarcinoma after surgical resection: A multi-center retrospective study. Pancreatology 2015, 15, 674–680. [Google Scholar] [CrossRef]
- Ono, S.; Adachi, T.; Ohtsuka, T.; Kimura, R.; Nishihara, K.; Watanabe, Y.; Nagano, H.; Tokumitsu, Y.; Nanashima, A.; Imamura, N.; et al. Predictive factors for early recurrence after pancreaticoduodenectomy in patients with resectable pancreatic head cancer: A multicenter retrospective study. Surgery 2022, 172, 1782–1790. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.J.; Park, B.; Kwon, J.; Lim, C.S.; Shin, Y.C.; Jung, W.; Shin, S.H.; Heo, J.S.; Han, I.W. Development of nomograms for predicting prognosis of pancreatic cancer after pancreatectomy: A multicenter study. Biomedicines 2022, 10, 1341. [Google Scholar] [CrossRef]
- Kim, D.W.; Lee, S.S.; Kim, S.O.; Kim, J.H.; Kim, H.J.; Byun, J.H.; Yoo, C.; Kim, K.P.; Song, K.B.; Kim, S.C. Estimating recurrence after upfront surgery in patients with resectable pancreatic ductal adenocarcinoma by using pancreatic CT: Development and validation of a risk score. Radiology 2020, 296, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.H.; Kim, H.Y.; Lee, E.J.; Hwang, H.K.; Park, M.S.; Kim, M.J.; Lee, W.J.; Chung, Y.E.; Kang, C.M. Preoperative clinical and computed tomography (CT)-based nomogram to predict oncologic outcomes in patients with pancreatic head cancer resected with curative intent: A retrospective study. J. Clin. Med. 2019, 8, 1749. [Google Scholar] [CrossRef] [Green Version]
- Cassinotto, C.; Chong, J.; Zogopoulos, G.; Reinhold, C.; Chiche, L.; Lafourcade, J.P.; Cuggia, A.; Terrebonne, E.; Dohan, A.; Gallix, B. Resectable pancreatic adenocarcinoma: Role of CT quantitative imaging biomarkers for predicting pathology and patient outcomes. Eur. J. Radiol. 2017, 90, 152–158. [Google Scholar] [CrossRef]
- Zhang, Y.; Lobo-Mueller, E.M.; Karanicolas, P.; Gallinger, S.; Haider, M.A.; Khalvati, F. CNN-based survival model for pancreatic ductal adenocarcinoma in medical imaging. BMC Med. Imaging 2020, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Cao, K.; Hou, Y.; Zhou, J.; Xia, Y.; Nogues, I.; Song, Q.; Jiang, H.; Ye, X.; Lu, J.; et al. Deep learning for fully automated prediction of overall survival in patients undergoing resection for pancreatic cancer: A retrospective multicenter study. Ann. Surg. 2022, 278, e68–e79. [Google Scholar] [CrossRef]
- Lee, W.; Park, H.J.; Lee, H.J.; Jun, E.; Song, K.B.; Hwang, D.W.; Lee, J.H.; Lim, K.; Kim, N.; Lee, S.S.; et al. Preoperative data-based deep learning model for predicting postoperative survival in pancreatic cancer patients. Int. J. Surg. 2022, 105, 106851. [Google Scholar] [CrossRef] [PubMed]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Tian, N.; Wu, D.; Zhu, L.; Zeng, M.; Li, J.; Wang, X. A predictive model for recurrence after upfront surgery in patients with resectable pancreatic ductal adenocarcinoma (PDAC) by using preoperative clinical data and CT characteristics. BMC Med. Imaging 2022, 22, 116. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Dreyer, K.J.; Geis, J.R. When machines think: Radiology’s next frontier. Radiology 2017, 285, 713–718. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Kim, Y.J.; Kim, K.G.; Park, J.S. Preoperative CT texture features predict prognosis after curative resection in pancreatic cancer. Sci. Rep. 2019, 9, 17389. [Google Scholar] [CrossRef] [Green Version]
- Sandrasegaran, K.; Lin, Y.; Asare-Sawiri, M.; Taiyini, T.; Tann, M. CT texture analysis of pancreatic cancer. Eur. Radiol. 2019, 29, 1067–1073. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Takahashi, H.; Akita, H.; Tomokuni, A.; Kobayashi, S.; Ohigashi, H.; Fijiwara, Y.; Yano, M.; Sakon, M.; Ishikawa, O. Preoperative gemcitabine-based chemoradiation therapy for borderline resectable pancreatic cancer: Impact of venous and arterial involvement status on surgical outcome and pattern of recurrence. Ann. Surg. 2016, 264, 1091–1097. [Google Scholar] [CrossRef]
- Kang, J.S.; Choi, Y.J.; Byun, Y.; Han, Y.; Kim, J.H.; Lee, J.M.; Sohn, H.J.; Kim, H.; Kwon, W.; Jang, J.Y. Radiological tumour invasion of splenic artery or vein in patients with pancreatic body or tail adenocarcinoma and effect on recurrence and survival. Br. J. Surg. 2021, 109, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Noda, Y.; Pisuchpen, N.; Mercaldo, N.D.; Sekigami, Y.; Michelakos, T.; Parakh, A.; Wo, J.Y.; Qadan, M.; Ferrone, C.; Lillemoe, K.D.; et al. Arterial involvement and resectability scoring system to predict R0 resection in patients with pancreatic ductal adenocarcinoma treated with neoadjuvant chemoradiation therapy. Eur. Radiol. 2022, 32, 2470–2480. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.K.; Park, M.S.; Kim, S.S.; Han, K.; Lee, H.S.; Bang, S.; Hwang, H.K.; Hwang, S.H.; Yun, M.; Kim, M.J. Regional lymph node metastasis detected on preoperative CT and/or FDG-PET may predict early recurrence of pancreatic adenocarcinoma after curative resection. Sci. Rep. 2022, 12, 17296. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Development Dataset (n = 257) | Internal Validation Dataset (n = 111) | External Validation Dataset (n = 67) | p Value |
|---|---|---|---|---|
| Age, years | 0.946 | |||
| ≥70 | 62 (24) | 25 (22) | 16 (24) | |
| <70 | 195 (76) | 86 (78) | 51 (76) | |
| Sex | 0.044 | |||
| Female | 87 (34) | 36 (32) | 33 (49) | |
| Male | 170 (66) | 75 (68) | 34 (51) | |
| Diabetes | 0.004 | |||
| No | 197 (77) | 84 (76) | 38 (57) | |
| Yes | 60 (23) | 27 (24) | 29 (43) | |
| Alb | 0.173 | |||
| ≥35 U/mL | 221 (86) | 99 (89) | 53 (79) | |
| <35 U/mL | 36 (14) | 12 (11) | 14 (21) | |
| TBIL | 0.088 | |||
| >21 μmol/L | 109 (42) | 38 (34) | 34 (51) | |
| ≤21 μmol/L | 148 (58) | 73 (66) | 33 (49) | |
| CA19-9 | 0.222 | |||
| ≥150 U/mL | 139 (54) | 70 (63) | 35 (44) | |
| <150 U/mL | 118 (46) | 41 (37) | 32 (56) | |
| CT tumor size | 0.134 | |||
| ≥3.0 cm | 142 (55) | 50 (45) | 31 (46) | |
| <3.0 cm | 115 (45) | 61 (55) | 36 (54) | |
| Location | 0.088 | |||
| Head | 164 (64) | 63 (57) | 49 (73) | |
| Body/Tail | 93 (36) | 48 (43) | 18 (27) | |
| cT stage (AJCC 8th edition) | 0.184 | |||
| cT1-T2 | 195 (76) | 74 (67) | 48 (72) | |
| cT3-T4 | 62 (24) | 37 (33) | 19 (28) | |
| cN stage (AJCC 8th edition) | 0.677 | |||
| cN0 | 143 (56) | 61 (55) | 41 (61) | |
| cN1-N2 | 114 (44) | 50 (45) | 26 (39) | |
| Vascular involvement on CT imaging | 0.740 | |||
| No | 143 (56) | 57 (52) | 37 (55) | |
| Arterial | 17 (6) | 7 (6) | 3 (5) | |
| Venous | 46 (18) | 16 (14) | 12 (18) | |
| Both | 51 (20) | 31 (28) | 15 (22) | |
| Organ involvement on CT imaging | <0.001 | |||
| No | 223 (87) | 93 (84) | 35 (52) | |
| Yes | 34 (13) | 18 (16) | 32 (48) | |
| Resection Margin | 0.553 | |||
| R0 | 238 (93) | 99 (89) | 61 (91) | |
| R1 | 19 (7) | 12 (11) | 6 (9) | |
| pT stage (AJCC 8th edition) | 0.154 | |||
| pT1-T2 | 179 (70) | 66 (60) | 43 (64) | |
| pT3-T4 | 78 (30) | 45 (40) | 24 (36) | |
| pN stage (AJCC 8th edition) | 0.077 | |||
| pN0 | 139 (54) | 74 (67) | 40 (60) | |
| pN1-N2 | 118 (46) | 37 (33) | 27 (40) | |
| Perineural invasion | 0.021 | |||
| No | 49 (19) | 12 (11) | 5 (7) | |
| Yes | 208 (81) | 99 (89) | 62 (93) | |
| Tumor differentiation | 0.666 | |||
| Well | 31 (12) | 10 (9) | 6 (9) | |
| Moderate | 161 (63) | 66 (60) | 44 (66) | |
| Poor | 65 (25) | 35 (31) | 17 (25) |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age (≥70 vs. <70) | 1.417 | 0.779–2.576 | 0.253 | |||
| Sex (Male vs. Female) | 1.166 | 0.690–1.972 | 0.566 | |||
| Diabetes (yes vs. no) | 1.004 | 0.557–1.811 | 0.989 | |||
| Alb (<35 vs. ≥35) | 1.400 | 0.666–2.943 | 0.375 | |||
| TBIL (>21 vs. ≤21) | 1.196 | 0.720–1.985 | 0.489 | |||
| CA19-9 (≥150 vs. <150) | 1.768 | 1.068–2.927 | 0.027 | |||
| CT tumor size (≥3.0 vs. <3 cm) | 1.960 | 1.173–3.277 | 0.010 | |||
| Location (head vs. body/tail) | 1.297 | 0.774–2.175 | 0.324 | |||
| cT stage (cT3/4 vs. cT1/2) | 2.316 | 1.227–4.371 | 0.010 | |||
| cN stage (cN1/2 vs. cN0) | 2.194 | 1.307–3.684 | 0.003 | 1.964 | 1.036–3.774 | 0.040 |
| Arterial involvement (yes vs. no) | 2.505 | 1.349–4.652 | 0.004 | 2.207 | 1.043–4.870 | 0.043 |
| Venous involvement (yes vs. no) | 1.742 | 1.027–2.955 | 0.040 | |||
| Organ involvement (yes vs. no) | 2.024 | 0.903–4.536 | 0.087 | |||
| Deep learning model outputs (per 0.1 increase) | 1.699 | 1.477–1.954 | <0.001 | 1.675 | 1.467–1.950 | <0.001 |
| Models | Dataset | AIC | AUC (95% CI) | Accuracy (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|---|---|---|---|
| Nomogram | Development | 243.674 | 0.855 (0.787–0.886) | 79.0 (73.5–83.8) | 87.0 (80.7–91.9) | 67.0 (57.0–76.0) |
| Internal validation | 133.613 | 0.752 (0.657–0.848) | 73.9 (64.7–81.8) | 83.3 (72.1–91.4) | 60.0 (44.3–74.3) | |
| External validation | 86.133 | 0.741 (0.615–0.867) | 73.1 (60.9–83.2) | 78.4 (61.8–90.2) | 66.7 (47.2–82.7) | |
| Deep learning | Development | 249.189 | 0.836 (0.787–0.886) | 78.2 (72.7–83.1) | 82.5 (75.5–88.1) | 71.8 (62.1–80.3) |
| Internal validation | 137.467 | 0.730 (0.633–0.826) | 72.1 (62.8–80.2) | 75.8 (63.6–85.5) | 66.7 (51.0–80.0) | |
| External validation | 89.323 | 0.720 (0.589–0.851) | 70.1 (57.7–80.7) | 73.0 (55.9–86.2) | 66.7 (47.2–82.7) | |
| Clinical | Development | 330.916 | 0.685 (0.618–0.752) | 66.5 (60.4–72.3) | 77.3 (69.8–83.6) | 50.5 (40.5–60.5) |
| Internal validation | 139.637 | 0.700 (0.601–0.799) | 67.6 (58.0–76.1) | 78.8 (67.0–87.9) | 51.1 (35.8–66.3) | |
| External validation | 86.603 | 0.707 (0.583–0.831) | 67.2 (54.6–78.2) | 70.3 (53.0–84.1) | 63.3 (43.9–80.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiang, F.; He, X.; Liu, X.; Li, X.; Zhang, X.; Fan, Y.; Yan, S. Development and Validation of a Nomogram for Preoperative Prediction of Early Recurrence after Upfront Surgery in Pancreatic Ductal Adenocarcinoma by Integrating Deep Learning and Radiological Variables. Cancers 2023, 15, 3543. https://doi.org/10.3390/cancers15143543
Xiang F, He X, Liu X, Li X, Zhang X, Fan Y, Yan S. Development and Validation of a Nomogram for Preoperative Prediction of Early Recurrence after Upfront Surgery in Pancreatic Ductal Adenocarcinoma by Integrating Deep Learning and Radiological Variables. Cancers. 2023; 15(14):3543. https://doi.org/10.3390/cancers15143543
Chicago/Turabian StyleXiang, Fei, Xiang He, Xingyu Liu, Xinming Li, Xuchang Zhang, Yingfang Fan, and Sheng Yan. 2023. "Development and Validation of a Nomogram for Preoperative Prediction of Early Recurrence after Upfront Surgery in Pancreatic Ductal Adenocarcinoma by Integrating Deep Learning and Radiological Variables" Cancers 15, no. 14: 3543. https://doi.org/10.3390/cancers15143543