

‘Stealth’ Prostate Tumors


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
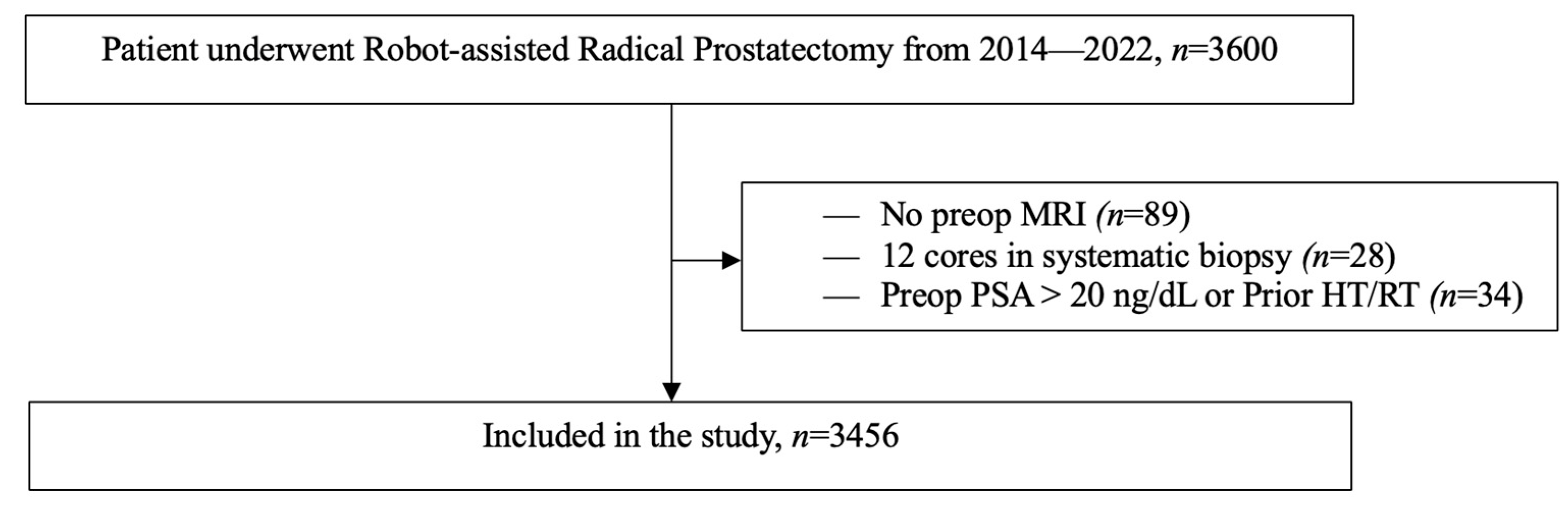
2.1. Study Design
2.1.1. Inclusion and Exclusion Criteria
2.1.2. MRI Protocol
2.1.3. Biopsy Protocol and Technique
2.1.4. Pathological Assessment
2.1.5. Outcome Definitions and Statistical Analysis
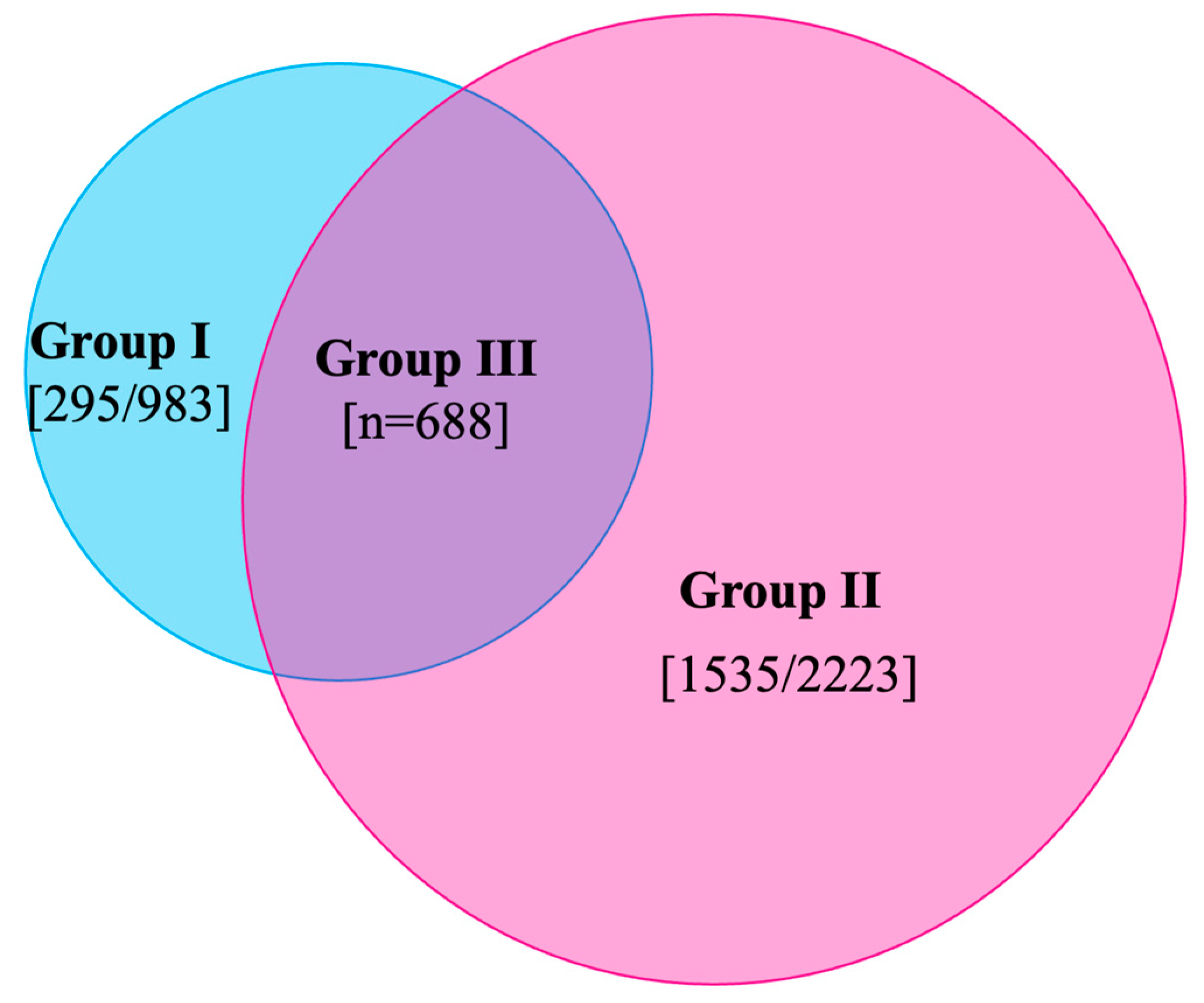
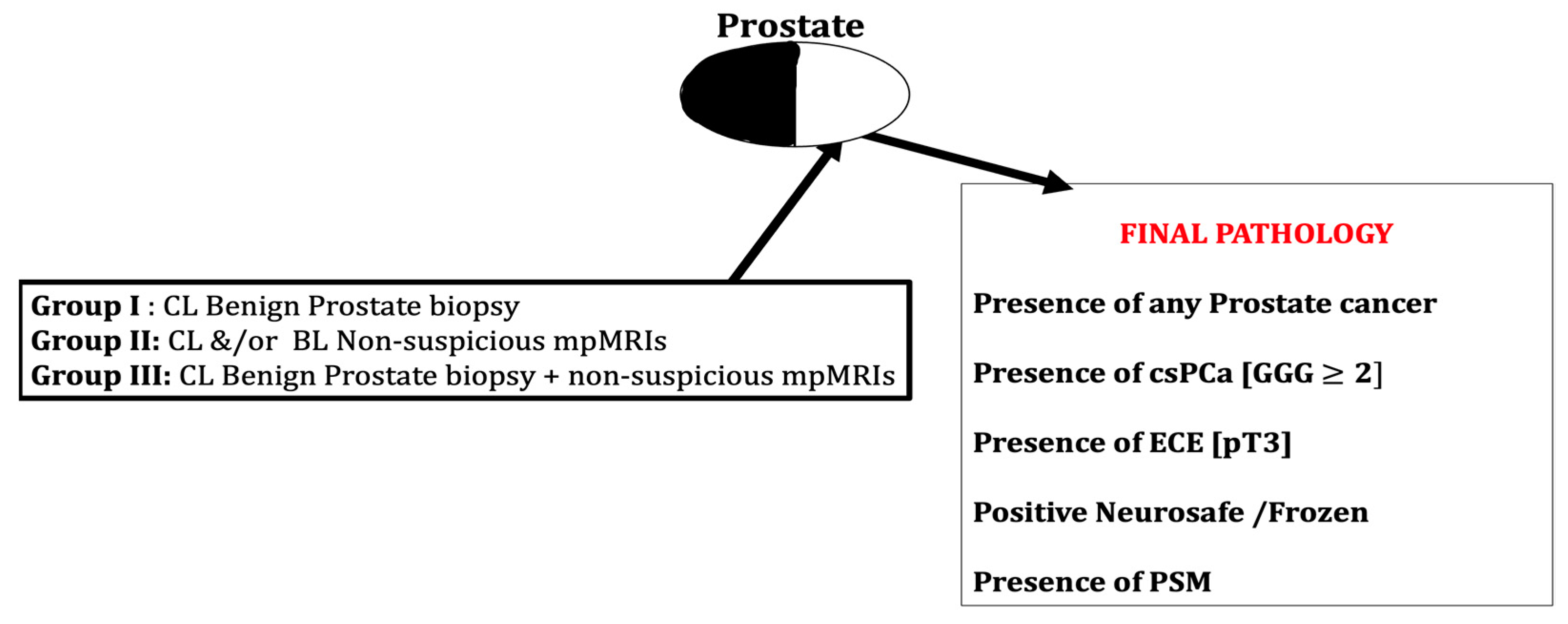
- I.
- Contralateral (CL) benign PBx (n = 983).
- II.
- CL and/or bilateral (BL) non-suspicious mpMRI (n = 2223).
- III.
- CL benign PBx + non-suspicious mpMRI (n = 688).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zaytoun, O.M.; Jones, J.S. Prostate cancer detection after a negative prostate biopsy: Lessons learnt in the Cleveland Clinic experience. Int. J. Urol. 2011, 18, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, A.; Aus, G.; Bolla, M.; Joniau, S.; Matveev, V.B.; Schmid, H.P.; Zattoni, F. EAU guidelines on prostate cancer. Eur. Urol. 2008, 53, 68–80. [Google Scholar] [CrossRef] [PubMed]
- Scattoni, V.; Zlotta, A.; Montironi, R.; Schulman, C.; Rigatti, P.; Montorsi, F. Extended and saturation prostatic biopsy in the diagnosis and characterisation of prostate cancer: A critical analysis of the literature. Eur. Urol. 2007, 52, 1309–1322. [Google Scholar] [CrossRef]
- Roehl, K.A.; Antenor, J.A.; Catalona, W.J. Serial biopsy results in prostate cancer screening study. J. Urol. 2002, 167, 2435–2439. [Google Scholar] [CrossRef] [PubMed]
- Serefoglu, E.C.; Altinova, S.; Ugras, N.S.; Akincioglu, E.; Asil, E.; Balbay, M.D. How reliable is 12-core prostate biopsy procedure in the detection of prostate cancer? Can Urol. Assoc. J. 2013, 7, E293–E298. [Google Scholar] [CrossRef] [Green Version]
- Sonn, G.A.; Chang, E.; Natarajan, S.; Margolis, D.J.; Macairan, M.; Lieu, P.; Huang, J.; Dorey, F.J.; Reiter, R.E.; Marks, L.S. Value of targeted prostate biopsy using magnetic resonance-ultrasound fusion in men with prior negative biopsy and elevated prostate-specific antigen. Eur. Urol. 2014, 65, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Valerio, M.; Donaldson, I.; Emberton, M.; Ehdaie, B.; Hadaschik, B.A.; Marks, L.S.; Mozer, P.; Rastinehad, A.R.; Ahmed, H.U. Detection of Clinically Significant Prostate Cancer Using Magnetic Resonance Imaging-Ultrasound Fusion Targeted Biopsy: A Systematic Review. Eur. Urol. 2015, 68, 8–19. [Google Scholar] [CrossRef]
- Tonttila, P.P.; Lantto, J.; Pääkkö, E.; Piippo, U.; Kauppila, S.; Lammentausta, E.; Ohtonen, P.; Vaarala, M.H. Prebiopsy Multiparametric Magnetic Resonance Imaging for Prostate Cancer Diagnosis in Biopsy-naive Men with Suspected Prostate Cancer Based on Elevated Prostate-specific Antigen Values: Results from a Randomized Prospective Blinded Controlled Trial. Eur. Urol. 2016, 69, 419–425. [Google Scholar] [CrossRef]
- Wagaskar, V.G.; Levy, M.; Ratnani, P.; Moody, K.; Garcia, M.; Pedraza, A.M.; Parekh, S.; Pandav, K.; Shukla, B.; Prasad, S.; et al. Clinical Utility of Negative Multiparametric Magnetic Resonance Imaging in the Diagnosis of Prostate Cancer and Clinically Significant Prostate Cancer. Eur. Urol. Open Sci. 2021, 28, 9–16. [Google Scholar] [CrossRef]
- Wagaskar, V.G.; Ratnani, P.; Levy, M.; Moody, K.; Garcia, M.; Pedraza, A.M.; Parekh, S.; Pandav, K.; Shukla, B.; Sobotka, S.; et al. Clinical characteristics and oncological outcomes in negative multiparametric MRI patients undergoing robot-assisted radical prostatectomy. Prostate 2021, 81, 772–777. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate Imaging-Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Kanao, K.; Kajikawa, K.; Kobayashi, I.; Muramatsu, H.; Morinaga, S.; Nishikawa, G.; Kato, Y.; Watanabe, M.; Nakamura, K.; Sumitomo, M. Utility of a novel biopsy instrument with long side-notch needle in the selection of patients for active surveillance. J. Clin. Oncol. 2017, 35 (Suppl. 15), e16581. [Google Scholar] [CrossRef]
- Wagaskar, V.G.; Zaytoun, O.; Kale, P.; Pedraza, A.; Haines, K., 3rd; Tewari, A. Robot-assisted simple prostatectomy for prostates greater than 100 g. World J. Urol. 2023, 41, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Protocol for the Examination of Radical Prostatectomy Specimens from Patients with Carcinoma of the Prostate Gland. Available online: https://documents.cap.org/protocols/Prostate_4.2.0.0.REL_CAPCP.pdf (accessed on 8 February 2023).
- Epstein, J.I.; Zelefsky, M.J.; Sjoberg, D.D.; Nelson, J.B.; Egevad, L.; Magi-Galluzzi, C.; Vickers, A.J.; Parwani, A.V.; Reuter, V.E.; Fine, S.W.; et al. A Contemporary Prostate Cancer Grading System: A Validated Alternative to the Gleason Score. Eur. Urol. 2016, 69, 428–435. [Google Scholar] [CrossRef] [Green Version]
- Wagaskar, V.G.; Sobotka, S.; Ratnani, P.; Young, J.; Lantz, A.; Parekh, S.; Falagario, U.G.; Li, L.; Lewis, S.; Haines, K., 3rd; et al. A 4K score/MRI-based nomogram for predicting prostate cancer, clinically significant prostate cancer, and unfavorable prostate cancer. Cancer Rep. 2021, 4, e1357. [Google Scholar] [CrossRef]
- Wagaskar, V.G.; Levy, M.; Ratnani, P.; Sullimada, S.; Gerenia, M.; Schlussel, K.; Choudhury, S.; Gabriele, M.; Haas, I.; Haines, K., 3rd; et al. A SelectMDx/magnetic resonance imaging-based nomogram to diagnose prostate cancer. Cancer Rep. 2023, 6, e1668. [Google Scholar] [CrossRef]
- Wagaskar, V.G.; Lantz, A.; Sobotka, S.; Ratnani, P.; Parekh, S.; Falagario, U.G.; Li, L.; Lewis, S.; Haines Iii, K.; Punnen, S.; et al. Development and External Validation of a Prediction Model to Identify Candidates for Prostate Biopsy. Urol. J. 2022, 19, 379–385. [Google Scholar] [PubMed]
- Parker, M. Chapter 18-Radar Basics. In Digital Signal Processing 101, 2nd ed.; Parker, M., Ed.; Newnes: London, UK, 2017; pp. 231–240. [Google Scholar]
- Oishi, M.; Shin, T.; Ohe, C.; Nassiri, N.; Palmer, S.L.; Aron, M.; Ashrafi, A.N.; Cacciamani, G.E.; Chen, F.; Duddalwar, V.; et al. Which Patients with Negative Magnetic Resonance Imaging Can Safely Avoid Biopsy for Prostate Cancer? J. Urol. 2019, 201, 268–276. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Cheng, L.; Mazzucchelli, R.; Jones, T.D.; Lopez-Beltran, A.; Montironi, R. Chapter 3—The Pathology of Prostate Cancer. In Early Diagnosis and Treatment of Cancer Series: Prostate Cancer; Su, L.-M., Ed.; W.B. Saunders: Philadelphia, PA, USA, 2010; pp. 45–83. [Google Scholar]
- Kim, J.J.; Kim, T.; Lee, H.; Byun, S.S.; Lee, S.E.; Choe, G.; Hong, S.K. Prediction of unilateral prostate cancer by the combination of transrectal ultrasonography-guided prostate biopsy and multi-parametric magnetic resonance imaging: A real-life experience. PLoS ONE 2018, 13, e0202872. [Google Scholar]
- Kim, J.J.; Byun, S.-S.; Lee, S.E.; Lee, H.J.; Choe, G.; Hong, S.K. A negative multiparametric magnetic resonance imaging finding does not guarantee the absence of significant cancer among biopsy-proven prostate cancer patients: A real-life clinical experience. Int. Urol. Nephrol. 2018, 50, 1989–1997. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Final Pathology Parameters | Group I: n = 983 (%) | Group II: n = 2223 (%) | Group III: n = 688 (%) |
|---|---|---|---|
| Presence of any PCa, no (%) | 212 (21.5) | 825 (37.7) | 134 (19.5) |
| Presence of csPCa, no (%) | 111 (11.3) | 362 (16.3) | 71 (10.3) |
| Presence of ECE (pT3), no (%) | 45 (4.5) | 85 (3.8) | 38 (5.5) |
| Positive frozen section analysis, no (%) | 51 (5.2) | 102 (4.5) | 27 (4) |
| Presence of PSMs, no (%) | 18 (1.8) | 61 (2.7) | 11 (1.5) |
| Variable | Patients with No CL Cancer on Final Pathology: Accurate, n = 771 (78.5%) | Patient with CL Cancer on Final Pathology: False Negative, n = 212 (21.5%) | p Value |
|---|---|---|---|
| Median age in years | 64 | 63 | 0.429 |
| Race | <0.023 * | ||
| AA | 80 (10.4) | 37 (17.5) | |
| White | 437 (56.7) | 119 (56.1) | |
| Others | 254 (32.9) | 56 (26.4) | |
| BMI | 26.9 | 27.1 | 0.362 |
| Family history of PCa | 0.320 | ||
| No | 582 (75.5) | 164 (77.4) | |
| Yes | 189 (24.5) | 48 (22.6) | |
| Median PSA at diagnosis | 6.1 | 6.3 | 0.258 |
| Median prostate volume (cc) | 40 | 39 | 0.381 |
| Biopsy GGG | 0.019 * | ||
| 1 | 101 (13.1) | 21 (9.9) | |
| 2 | 295 (38.3) | 93 (43.9) | |
| 3 | 201 (26.1) | 51 (24.1) | |
| 4 | 122 (15.8) | 22 (10.4) | |
| 5 | 52 (6.7) | 25 (11.8) | |
| MRI PI-RADS lesions | 0.129 | ||
| 1–2 | 105 (13.6) | 23 (10.8) | |
| 3 | 81 (10.5) | 13 (6.1) | |
| 4 | 368 (47.7) | 107 (50.5) | |
| 5 | 217 (28.1) | 69 (32.5) | |
| Final pathology GGG | 0.056 | ||
| 1 | 71 (9.2) | 16 (7.5) | |
| 2 | 412 (53.4) | 103 (48.6) | |
| 3 | 202 (26.2) | 63 (29.7) | |
| 4 | 38 (4.9) | 10 (4.7) | |
| 5 | 48 (6.2) | 20 (9.4) | |
| Pathology T stage | <0.001 * | ||
| T2 | 660 (85.6) | 133 (62.7) | |
| T3 | 111 (14.4) | 79 (37.3) | |
| PSMs | <0.001 * | ||
| Absent | 736 (95.5) | 187 (88.2) | |
| Present | 35 (4.5) | 25 (11.8) |
| Variable | Patients with No CL Cancer on Final Pathology: Accurate n = 1398 (62.3%) | Patient with CL Cancer on Final Pathology: False Negative n = 825 (37.7%) | p Value |
|---|---|---|---|
| Median age in years | 64 | 63 | 0.429 |
| Race | <0.001 * | ||
| AA | 158 (11.3) | 131 (15.9) | |
| White | 855 (61.2) | 497 (60.2) | |
| Others | 385 (22.4) | 197 (23.9) | |
| BMI | 26.9 | 27.1 | 0.362 |
| Family history of PCa | 0.067 | ||
| No | 1072 (76.7) | 656 (79.5) | |
| Yes | 326 (23.3) | 169 (20.5) | |
| Median PSA at diagnosis | 6.0 | 6.0 | 0.258 |
| Median prostate volume (cc) | 39 | 39 | 0.381 |
| Biopsy GGG | 0.032 * | ||
| 1 | 225 (16.1) | 175 (21.2) | |
| 2 | 553 (39.6) | 323 (39.2) | |
| 3 | 305 (21.8) | 165 (20.0) | |
| 4 | 196 (14.0) | 98 (11.9) | |
| 5 | 119 (8.5) | 64 (7.8) | |
| MRI PI-RADS lesions | <0.001 * | ||
| 1–2 | 13(1) | 332 (40.2) | |
| 3 | 162 (11.6) | 62 (7.5) | |
| 4 | 716 (51.2) | 252 (30.5) | |
| 5 | 507 (36.3) | 179 (21.7) | |
| Final pathology GGG | 0.017 * | ||
| 1 | 127 (9.1) | 98 (11.9) | |
| 2 | 764 (54.6) | 480 (58.2) | |
| 3 | 344 (24.6) | 174 (21.1) | |
| 4 | 60 (4.3) | 24 (2.9) | |
| 5 | 103 (7.4) | 49 (5.9) | |
| Pathology T stage | <0.001 * | ||
| T2 | 1154 (82.5) | 570 (69.1) | |
| T3 | 244 (17.5) | 255 (30.9) | |
| PSMs | <0.001 * | ||
| Absent | 1336 (95.6) | 738 (89.5) | |
| Present | 62 (4.4) | 87 (10.5) |
| Variable | Patients with No CL Cancer on Final Pathology: Accurate, n = 554 (81.5%) | Patient with CL Cancer on Final Pathology: False Negative, n = 134 (19.5%) | p Value |
|---|---|---|---|
| Median age in years | 64 | 63 | 0.429 |
| Race | 0.093 | ||
| AA | 53 (9.6) | 19 (14.2) | |
| White | 314 (56.7) | 82 (61.2) | |
| Others | 187 (33.8) | 33 (24.6) | |
| BMI | 26.9 | 27.1 | 0.362 |
| Family history of PCa | 0.320 | ||
| No | 416 (75.1) | 103 (76.9) | |
| Yes | 138 (24.9) | 31 (23.1) | |
| Median PSA at diagnosis | 6.1 | 6.3 | 0.258 |
| Median prostate volume (cc) | 40 | 39 | 0.381 |
| Biopsy GGG | 0.001 * | ||
| 1 | 66 (11.9) | 4 (3) | |
| 2 | 210 (37.9) | 57 (42.5) | |
| 3 | 142 (25.6) | 44 (32.8) | |
| 4 | 92 (16.6) | 13 (9.7) | |
| 5 | 44 (7.9) | 16 (11.9) | |
| MRI PI-RADS lesions | 0.129 | ||
| 1–2 | 5 (1) | 2 (1) | |
| 3 | 57 (10.3) | 8 (6) | |
| 4 | 317 (57.2) | 72 (53.7) | |
| 5 | 175 (31.6) | 52 (38.8) | |
| Final pathology GGG | 0.056 | ||
| 1 | 71 (9.2) | 16 (7.5) | |
| 2 | 412 (53.4) | 103 (48.6) | |
| 3 | 202 (26.2) | 63 (29.7) | |
| 4 | 38 (4.9) | 10 (4.7) | |
| 5 | 48 (6.2) | 20 (9.4) | |
| Pathology T stage | <0.001 * | ||
| T2 | 465 (83.9) | 81(60.4) | |
| T3 | 89 (16.1) | 53 (39.6) | |
| PSMs | <0.001 * | ||
| Absent | 532 (96) | 118 (88.1) | |
| Present | 22 (4) | 16 (11.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagaskar, V.G.; Zaytoun, O.; Bhardwaj, S.; Tewari, A. ‘Stealth’ Prostate Tumors. Cancers 2023, 15, 3487. https://doi.org/10.3390/cancers15133487
Wagaskar VG, Zaytoun O, Bhardwaj S, Tewari A. ‘Stealth’ Prostate Tumors. Cancers. 2023; 15(13):3487. https://doi.org/10.3390/cancers15133487
Chicago/Turabian StyleWagaskar, Vinayak G., Osama Zaytoun, Swati Bhardwaj, and Ash Tewari. 2023. "‘Stealth’ Prostate Tumors" Cancers 15, no. 13: 3487. https://doi.org/10.3390/cancers15133487