
Predicting Tumor Perineural Invasion Status in High-Grade Prostate Cancer Based on a Clinical–Radiomics Model Incorporating T2-Weighted and Diffusion-Weighted Magnetic Resonance Images
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. MR Image Data
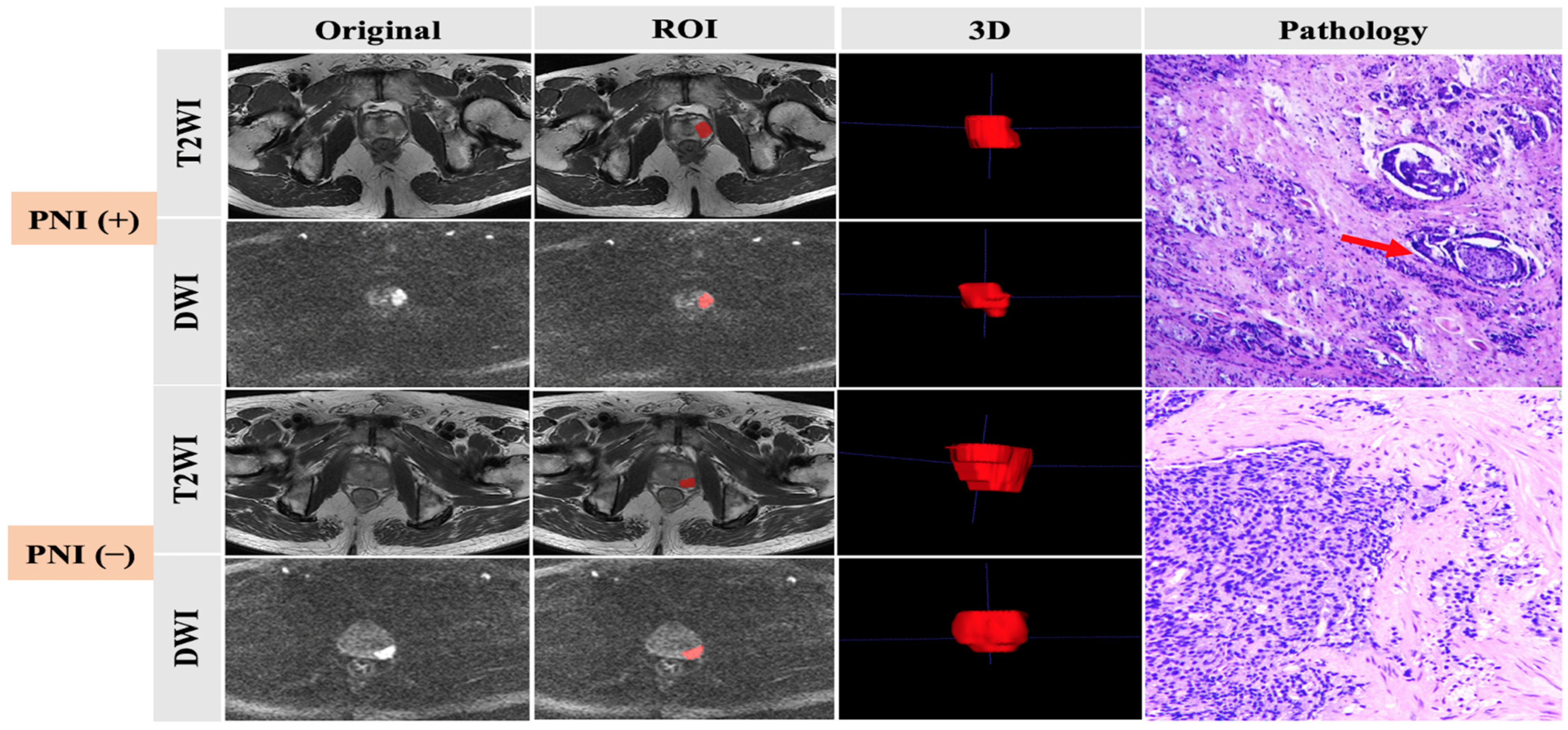
2.3. Histopathologic Analysis
2.4. Tumor Segmentation
2.5. Extraction of Radiomic Features
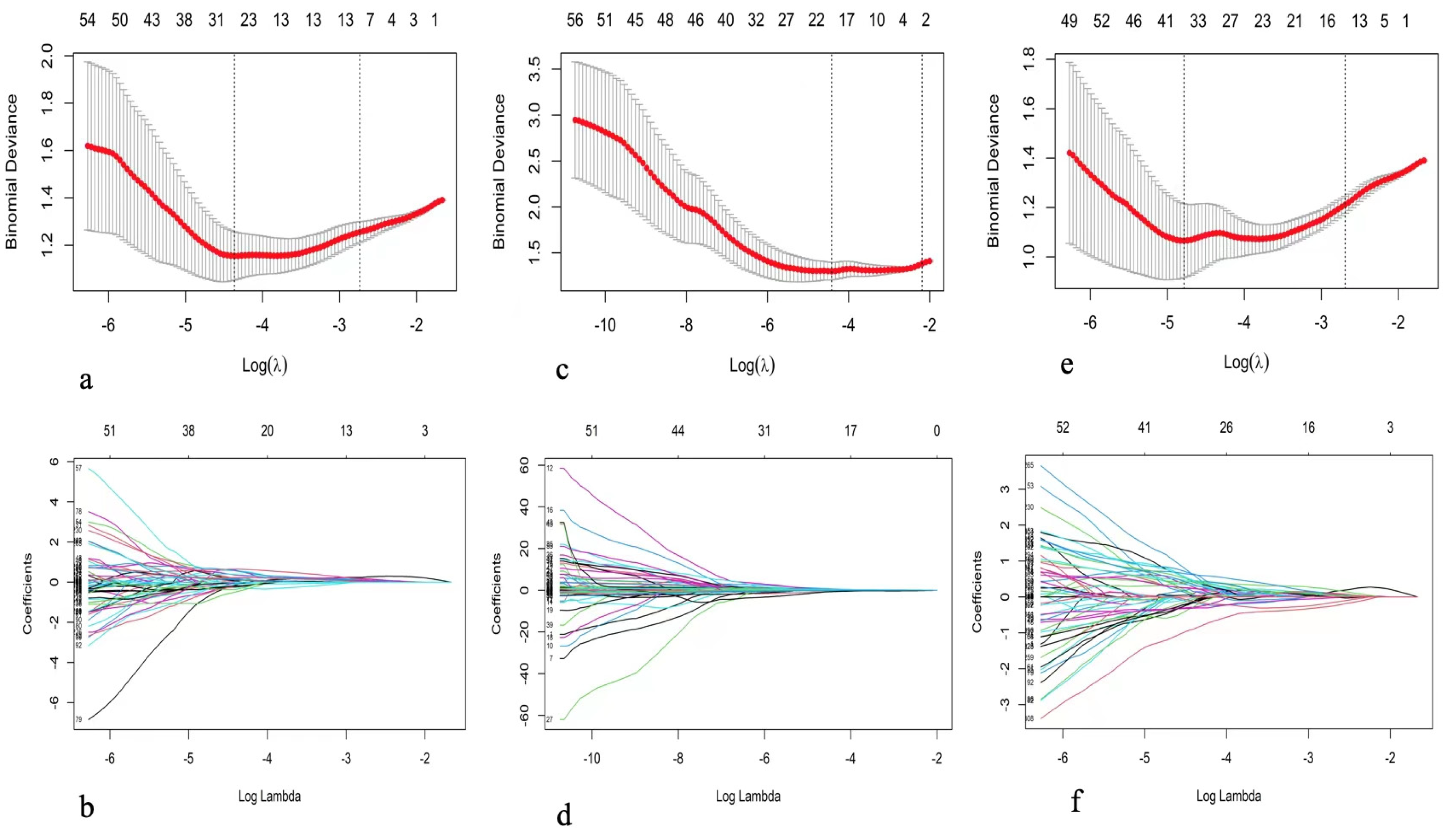
2.6. Feature Selection and Model Building
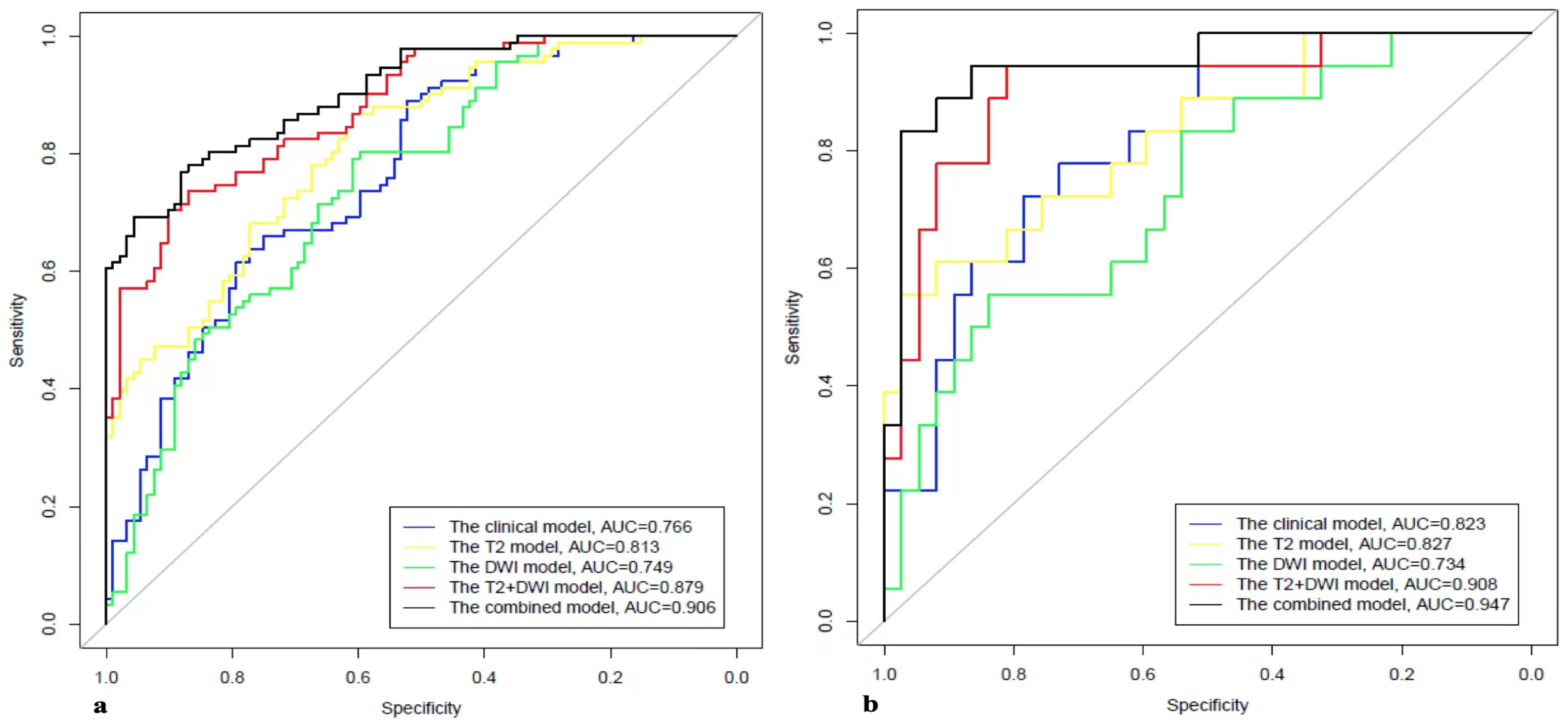
2.7. Model Evaluation
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Feature Selection and Comparison of Models
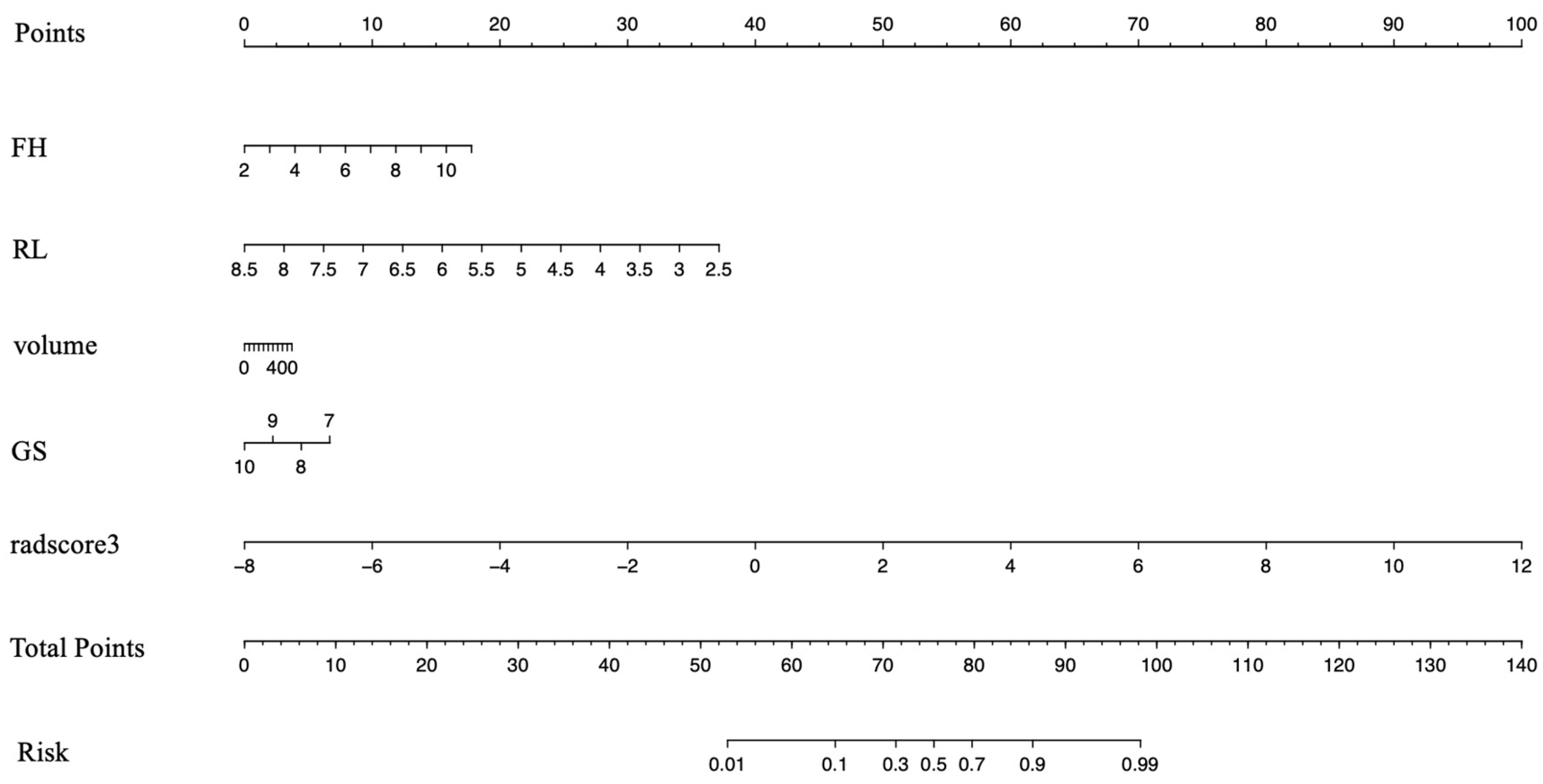
3.3. Development of the Clinical–Radiomics Predictive Model
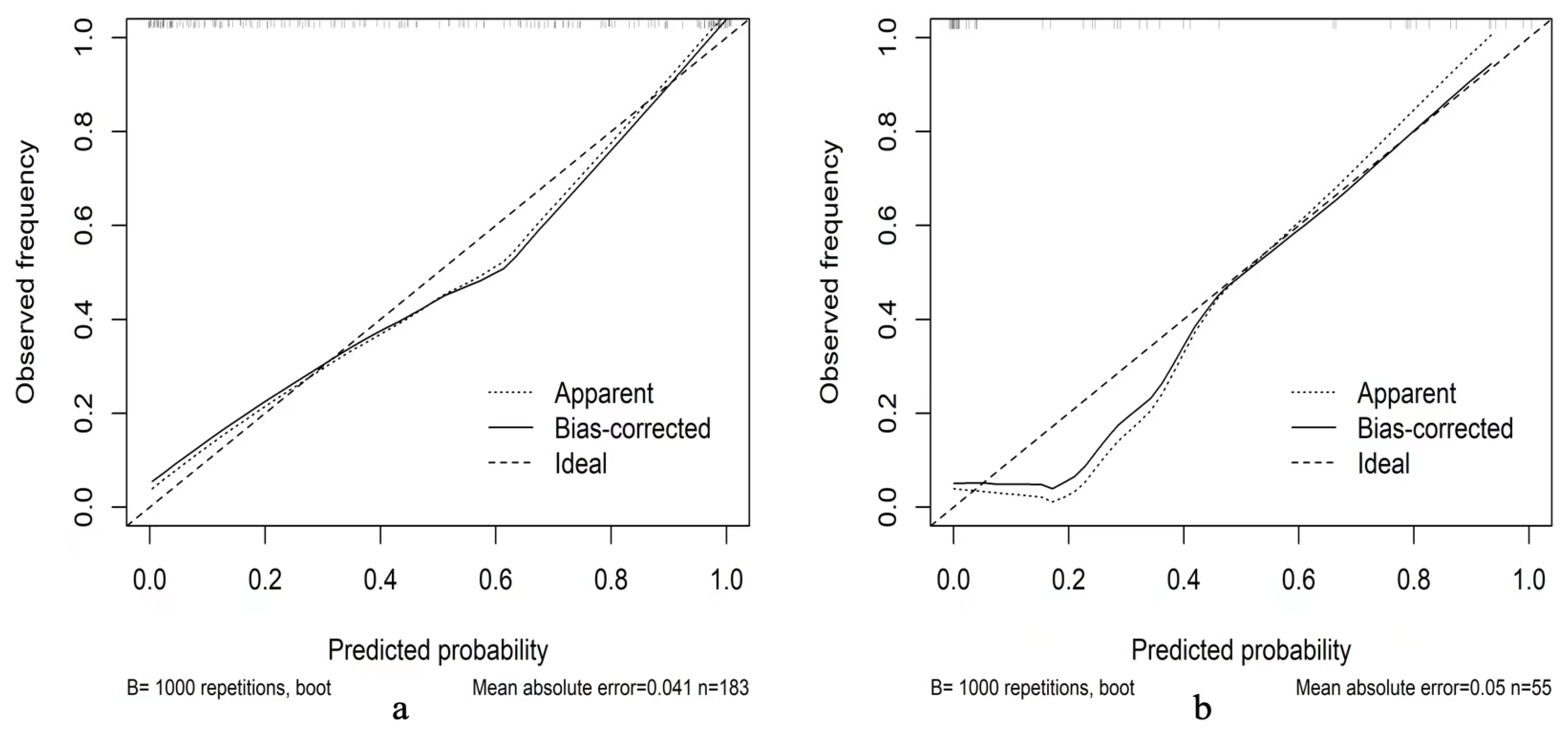
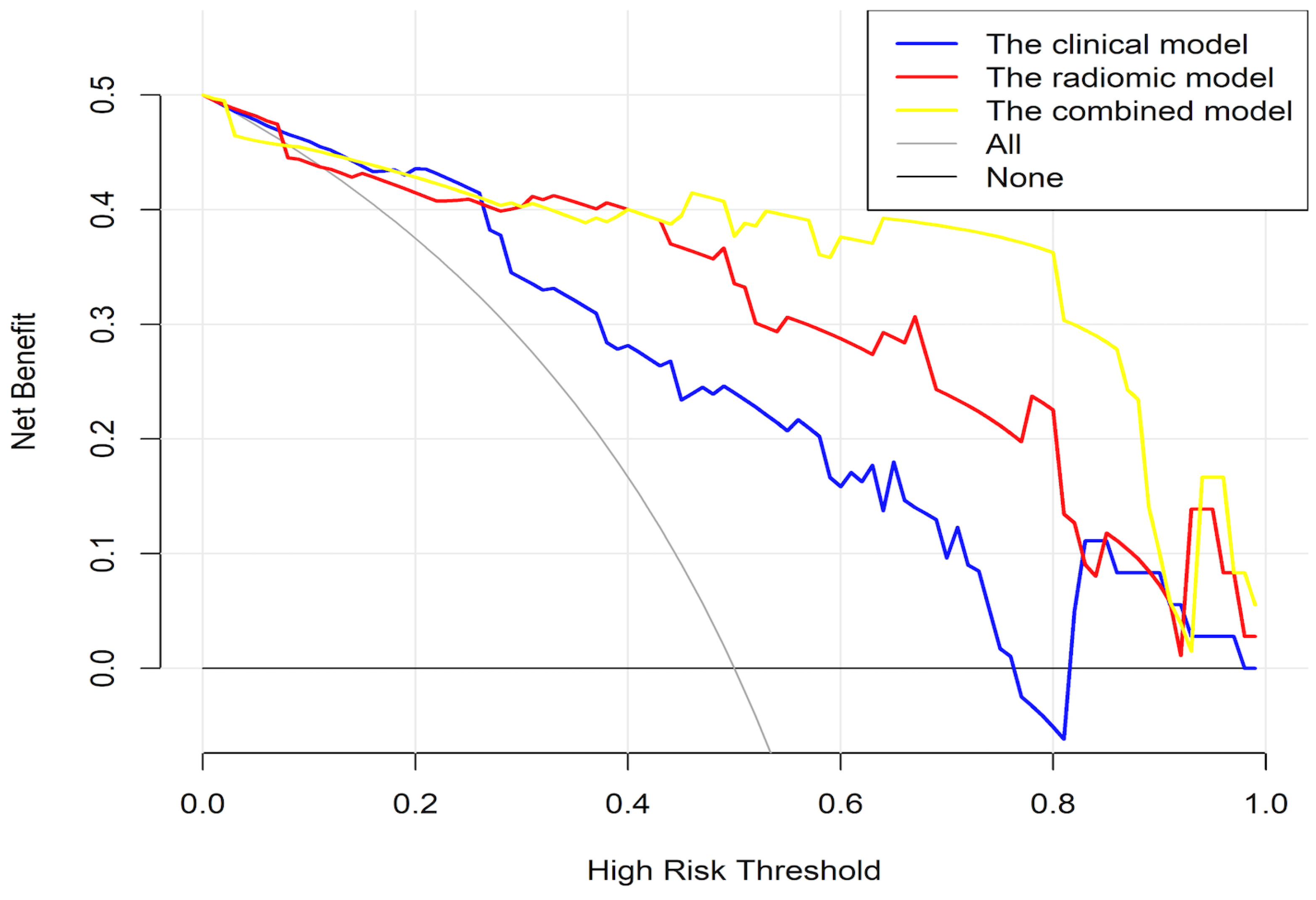
3.4. Validation of the Clinical–Radiomics Predictive Nomogram
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical Outcome After Radical Prostatectomy, External Beam Radiation Therapy, or Interstitial Radiation Therapy for Clinically Localized Prostate Cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Ward, J.F.; Blute, M.L.; Slezak, J.; Bergstralh, E.J.; Zincke, H. The Long-Term Clinical Impact of Biochemical Recurrence of Prostate Cancer 5 or More Years After Radical Prostatectomy. J. Urol. 2003, 170, 1872–1876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, A.S.; Parameshwaran, V.; Beltran, L.; Fisher, G.; North, B.V.; Greenberg, D.; Soosay, G.; Møller, H.; Scardino, P.; Cuzick, J.; et al. Should reporting of peri-neural invasion and extra prostatic extension be mandatory in prostate cancer biopsies? correlation with outcome in biopsy cases treated conservatively. Oncotarget 2018, 9, 20555–20562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, Y.; Liao, Y.-B.; Xu, P.; Wei, W.-R.; Wang, J. Perineural invasion is an independent predictor of biochemical recurrence of prostate cancer after local treatment: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 13267–13274. [Google Scholar]
- Bostwick, D.G.; Grignon, D.J.; Hammond, M.E.H.; Amin, M.B.; Cohen, M.; Crawford, D.; Gospadarowicz, M.; Kaplan, R.S.; Miller, D.S.; Montironi, R.; et al. Prognostic Factors in Prostate Cancer: College of American Pathologists Consensus Statement 1999. Arch. Pathol. Lab. Med. 2000, 124, 995–1000. [Google Scholar] [CrossRef]
- Pasoglou, V.; Larbi, A.; Collette, L.; Annet, L.; Jamar, F.; Machiels, J.; Michoux, N.; Berg, B.C.V.; Tombal, B.; Lecouvet, F.E. One-step TNM staging of high-risk prostate cancer using magnetic resonance imaging (MRI): Toward an upfront simplified “all-in-one” imaging approach? Prostate 2014, 74, 469–477. [Google Scholar] [CrossRef]
- Tamada, T.; Sone, T.; Kanomata, N.; Miyaji, Y.; Kido, A.; Jo, Y.; Yamamoto, A.; Ito, K. Value of preoperative 3T multiparametric MRI for surgical margin status in patients with prostate cancer. J. Magn. Reson. Imaging 2016, 44, 584–593. [Google Scholar] [CrossRef]
- Liu, B.; Cheng, J.; Guo, D.J.; He, X.J.; Luo, Y.D.; Zeng, Y.; Li, C.M. Prediction of prostate cancer aggressiveness with a combination of radiomics and machine learning-based analysis of dynamic contrast-enhanced MRI. Clin. Radiol. 2019, 74, 896.e1–896.e8. [Google Scholar] [CrossRef] [Green Version]
- Bourbonne, V.; Vallières, M.; Lucia, F.; Doucet, L.; Visvikis, D.; Tissot, V.; Pradier, O.; Hatt, M.; Schick, U. MRI-Derived Radiomics to Guide Post-operative Management for High-Risk Prostate Cancer. Front. Oncol. 2019, 9, 807. [Google Scholar] [CrossRef] [Green Version]
- Hébert-Blouin, M.N.; Amrami, K.K.; Myers, R.P.; Hanna, A.S.; Spinner, R.J. Adenocarcinoma of the prostate involving the lumbosacral plexus: MRI evidence to support direct perineural spread. Acta Neurochir. 2010, 152, 1567–1576. [Google Scholar] [CrossRef]
- Capek, S.; Howe, B.M.; Amrami, K.K.; Spinner, R.J. Perineural spread of pelvic malignancies to the lumbosacral plexus and beyond: Clinical and imaging patterns. Neurosurg. Focus 2015, 39, E14. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Zhang, J.; Zhang, Y.-D.; Hou, Y.; Yan, X.; Wang, Y.; Zhou, M.; Yao, Y.-F.; Yang, G. FeAture Explorer (FAE): A tool for developing and comparing radiomics models. PLoS ONE 2020, 15, e0237587. [Google Scholar] [CrossRef]
- Kuol, N.; Stojanovska, L.; Apostolopoulos, V.; Nurgali, K. Role of the nervous system in cancer metastasis. J. Exp. Clin. Cancer Res. 2018, 37, 5. [Google Scholar] [CrossRef] [Green Version]
- Cole, S.W.; Nagaraja, A.; Lutgendorf, S.K.; Green, P.; Sood, A.K. Sympathetic nervous system regulation of the tumour microenvironment. Nat. Rev. Cancer 2015, 15, 563–572. [Google Scholar] [CrossRef] [Green Version]
- He, S.; He, S.; Chen, C.-H.; Deborde, S.; Bakst, R.L.; Chernichenko, N.; McNamara, W.F.; Lee, S.Y.; Barajas, F.; Yu, Z.; et al. The Chemokine (CCL2–CCR2) Signaling Axis Mediates Perineural Invasion. Mol. Cancer Res. 2015, 13, 380–390. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Qi, L.; Li, M.; Zhang, D.; Xu, S.; Wang, N.; Sun, B. Chemokine CXCL12 and its receptor CXCR4 expression are associated with perineural invasion of prostate cancer. J. Exp. Clin. Cancer Res. 2008, 27, 62. [Google Scholar] [CrossRef] [Green Version]
- Suresh, N.; Teramoto, Y.; Goto, T.; Wang, Y.; Miyamoto, H. Clinical significance of perineural invasion by prostate cancer on magnetic resonance imaging–targeted biopsy. Hum. Pathol. 2022, 121, 65–72. [Google Scholar] [CrossRef]
- Niu, Y.; Förster, S.; Muders, M. The Role of Perineural Invasion in Prostate Cancer and Its Prognostic Significance. Cancers 2022, 14, 4065. [Google Scholar] [CrossRef]
- Truong, M.; Rais-Bahrami, S.; Nix, J.W.; Messing, E.M.; Miyamoto, H.; Gordetsky, J.B. Perineural invasion by prostate cancer on MR/US fusion targeted biopsy is associated with extraprostatic extension and early biochemical recurrence after radical prostatectomy. Hum. Pathol. 2017, 66, 206–211. [Google Scholar] [CrossRef]
- Lee, I.H.; Roberts, R.; Shah, R.B.; Wojno, K.J.; Wei, J.T.; Sandler, H.M. Perineural Invasion is a Marker for Pathologically Advanced Disease in Localized Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-J.; Wu, B.; Zha, Z.-L.; Qu, W.; Zhao, H.; Yuan, J.; Feng, Y.-J. Perineural invasion as an independent predictor of biochemical recurrence in prostate cancer following radical prostatectomy or radiotherapy: A systematic review and meta-analysis. BMC Urol. 2018, 18, 5. [Google Scholar] [CrossRef]
- Dell’Atti, L. Prognostic significance of perineural invasion in patients who underwent radical prostatectomy for localized prostate cancer. J. B.U.ON. Off. J. Balk. Union Oncol. 2016, 21, 1219–1223. [Google Scholar]
- DeLancey, J.O.; Wood, D.P.; He, C.; Montgomery, J.S.; Weizer, A.Z.; Miller, D.C.; Jacobs, B.L.; Montie, J.E.; Hollenbeck, B.K.; Skolarus, T.A. Evidence of Perineural Invasion on Prostate Biopsy Specimen and Survival After Radical Prostatectomy. Urology 2013, 81, 354–357. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Xie, L.; Lin, S.X.; Wirth, G.J.; Lu, M.; Zhang, Y.; Blute, M.L.; Dahl, D.M.; Wu, C.-L. Quantification of perineural invasion focus after radical prostatectomy could improve predictive power of recurrence. Hum. Pathol. 2020, 104, 96–104. [Google Scholar] [CrossRef]
- Sigorski, D.; Gulczyński, J.; Sejda, A.; Rogowski, W.; Iżycka-Świeszewska, E. Investigation of Neural Microenvironment in Prostate Cancer in Context of Neural Density, Perineural Invasion, and Neuroendocrine Profile of Tumors. Front. Oncol. 2021, 11, 710899. [Google Scholar] [CrossRef]
- Billis, A.; De Quintal, M.M.; Meirelles, L.; Freitas, L.L.L.; Magna, L.A.; Ferreira, U. Does tumor extent on needle prostatic biopsies influence the value of perineural invasion to predict pathologic stage > T2 in radical prostatectomies? Int. braz j urol 2010, 36, 439–447. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Kim, C.K.; Park, B.K.; Sung, H.H.; Han, D.H.; Jeon, H.G.; Jeong, B.C.; Seo, S.I.; Jeon, S.S.; Choi, H.Y.; et al. Accuracy of preoperative multiparametric magnetic resonance imaging for prediction of unfavorable pathology in patients with localized prostate cancer undergoing radical prostatectomy. World J. Urol. 2017, 35, 929–934. [Google Scholar] [CrossRef]
- Griffiths, L.; Kotamarti, S.; Mikhail, D.; Sarcona, J.; Rastinehad, A.R.; Villani, R.; Kreshover, J.; Hall, S.J.; Vira, M.A.; Schwartz, M.J.; et al. Extracapsular extension on multiparametric magnetic resonance imaging better predicts pT3 disease at radical prostatectomy compared to perineural invasion on biopsy. Can. Urol. Assoc. J. 2021, 15, 261–266. [Google Scholar] [CrossRef]
- Stone, J.J.; Adamo, D.A.; Khan, D.Z.; Packard, A.T.; Broski, S.M.; Nathan, M.A.; Howe, B.M.; Spinner, R.J. Multimodal Imaging Aids in the Diagnosis of Perineural Spread of Prostate Cancer. World Neurosurg. 2019, 122, e235–e240. [Google Scholar] [CrossRef]
- Siracusano, S.; Porcaro, A.B.; Tafuri, A.; Pirozzi, M.; Cybulski, A.; Shakir, A.; Tiso, L.; Talamini, R.; Mucelli, R.P. Visualization of peri-prostatic neurovascular fibers before and after radical prostatectomy by means of diffusion tensor imaging (DTI) with clinical correlations: Preliminary report. J. Robot. Surg. 2020, 14, 357–363. [Google Scholar] [CrossRef]
- You, H.; Shang, W.; Min, X.; Weinreb, J.; Li, Q.; Leapman, M.; Wang, L.; Tian, J. Sight and switch off: Nerve density visualization for interventions targeting nerves in prostate cancer. Sci. Adv. 2020, 6, eaax6040. [Google Scholar] [CrossRef]
- Sun, Y.; Reynolds, H.M.; Parameswaran, B.; Wraith, D.; Finnegan, M.E.; Williams, S.; Haworth, A. Multiparametric MRI and radiomics in prostate cancer: A review. Australas. Phys. Eng. Sci. Med. 2019, 42, 3–25. [Google Scholar] [CrossRef]
- Ma, S.; Xie, H.; Wang, H.; Han, C.; Yang, J.; Lin, Z.; Li, Y.; He, Q.; Wang, R.; Cui, Y.; et al. MRI-Based Radiomics Signature for the Preoperative Prediction of Extracapsular Extension of Prostate Cancer. J. Magn. Reson. Imaging 2019, 50, 1914–1925. [Google Scholar] [CrossRef]
- Peng, Y.; Jiang, Y.; Antic, T.; Giger, M.L.; Eggener, S.E.; Oto, A. Validation of Quantitative Analysis of Multiparametric Prostate MR Images for Prostate Cancer Detection and Aggressiveness Assessment: A Cross-Imager Study. Radiology 2014, 271, 461–471. [Google Scholar] [CrossRef]
- Vignati, A.; Mazzetti, S.; Giannini, V.; Russo, F.; Bollito, E.; Porpiglia, F.; Stasi, M.; Regge, D. Texture features on T2-weighted magnetic resonance imaging: New potential biomarkers for prostate cancer aggressiveness. Phys. Med. Biol. 2015, 60, 2685–2701. [Google Scholar] [CrossRef]
- Jajodia, A.; Gupta, A.; Prosch, H.; Mayerhoefer, M.; Mitra, S.; Pasricha, S.; Mehta, A.; Puri, S.; Chaturvedi, A. Combination of Radiomics and Machine Learning with Diffusion-Weighted MR Imaging for Clinical Outcome Prognostication in Cervical Cancer. Tomography 2021, 7, 344–357. [Google Scholar] [CrossRef]
- Linsalata, S.; Borgheresi, R.; Marfisi, D.; Barca, P.; Sainato, A.; Paiar, F.; Neri, E.; Traino, A.C.; Giannelli, M. Radiomics of Patients with Locally Advanced Rectal Cancer: Effect of Preprocessing on Features Estimation from Computed Tomography Imaging. BioMed Res. Int. 2022, 2022, 1–21. [Google Scholar] [CrossRef]
- Gill, T.S.; Varghese, B.A.; Hwang, D.H.; Cen, S.Y.; Aron, M.; Aron, M.; Duddalwar, V.A. Juxtatumoral perinephric fat analysis in clear cell renal cell carcinoma. Abdom. Radiol. 2019, 44, 1470–1480. [Google Scholar] [CrossRef]
- Fan, T.-W.; Malhi, H.; Varghese, B.; Cen, S.; Hwang, D.; Aron, M.; Rajarubendra, N.; Desai, M.; Duddalwar, V. Computed tomography-based texture analysis of bladder cancer: Differentiating urothelial carcinoma from micropapillary carcinoma. Abdom. Radiol. 2018, 44, 201–208. [Google Scholar] [CrossRef]
- De Santi, B.; Salvi, M.; Giannini, V.; Meiburger, K.M.; Marzola, F.; Russo, F.; Bosco, M.; Molinari, F. Comparison of Histogram-based Textural Features between Cancerous and Normal Prostatic Tissue in Multiparametric Magnetic Resonance Images. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; Volume 2020, pp. 1671–1674. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PNI (+) (N = 54) | PNI (−) (N = 129) | p Value |
|---|---|---|---|
| Age (years) | 69.7 ± 8.2 | 72.0 ± 9.0 | 0.121 |
| PSA level (ng/mL) | 15.9 (10–23) | 17.4 (11.4–25.7) | 0.406 |
| Prostate volume (mL) | 43.7 (31.3–59.7) | 53.7 (38.1–87.7) | 0.006 |
| Foot–head (FH) (cm) | 4.4 (3.6–5.1) | 4.7 (3.9–5.8) | 0.02 |
| Right–left (RL) (cm) | 4.7 (4–5) | 5.1 (4.5–5.9) | <0.001 |
| Anterior–posterior (AP) (cm) | 4.1 (3.6–4.9) | 4.3 (3.7–5.2) | 0.247 |
| PSAD (ng/mL/cm3) | 0.4 (0.2–0.5) | 0.3 (0.2–0.5) | 0.176 |
| Gleason Score (GS) | 9.13 (9–10) | 8.78 (8–9) | 0.005 |
| Grading Groups (GG) | <0.001 | ||
| Grade 1 | 0.0% (0/54) | 0.0% (0/129) | |
| Grade 2 | 0.0% (0/54) | 0.0% (0/129) | |
| Grade 3 | 0.0% (0/54) | 0.0% (0/129) | |
| Grade 4 | 22.2% (12/54) | 41.1% (53/129) | |
| Grade 5 | 77.8% (42/54) | 58.9% (76/129) | |
| Location | 0.196 | ||
| Central zone | 1.9% (1/54) | 2.3% (3/129) | |
| Transition zone | 13.0% (7/54) | 7.0% (9/129) | |
| Peripheral zone | 25.9% (14/54) | 17.1% (22/129) | |
| Multiple zone | 59.3% (32/54) | 73.6% (95/129) | |
| Rad-score | 1.52 ± 2.649 | −1.815 ± 2.065 | <0.001 |
| Characteristics | Training (N = 128) | Test (N = 55) | p Value |
|---|---|---|---|
| Age (years) | 72.0 ± 8.6 | 69.8 ± 9.1 | 0.117 |
| PSA level (ng/mL) | 42.4 (14.3–138.6) | 49.8 (13.9–169) | 0.716 |
| Prostate volume (mL) | 48.6 (35.2–77.4) | 52.9 (36.6–71.0) | 0.797 |
| Foot–head (FH) (cm) | 4.7 (3.8–5.7) | 4.6 (3.8–5.3) | 0.484 |
| Right–left (RL) (cm) | 4.9 (4.4–5.5) | 4.9 (4.2–5.5) | 0.796 |
| Anterior–posterior (AP) (cm) | 4.3 (3.7–5.2) | 4.1 (3.4–4.9) | 0.157 |
| PSAD (ng/mL/cm3) | 0.9 (0.3–2.9) | 0.9 (0.3–2.8) | 0.861 |
| Gleason Score (GS) | 9.0 (8–9) | 9.0 (8–9) | 0.092 |
| Location | 0.193 | ||
| Central zone | 1.6% (2/128) | 3.6% (2/55) | |
| Transition zone | 10.9% (14/128) | 3.6% (2/55) | |
| Peripheral zone | 21.1% (27/128) | 14.5% (8/55) | |
| Multiple zone | 66.4% (85/128) | 78.2% (43/55) | |
| Rad-score | −0.542 ± 2.518 | −1.503 ± 3.046 | 0.052 |
| Radiomics Features | Coefficient | Odds Ratio (95% CI) | p-Value | |
|---|---|---|---|---|
| T2WI | T2_wavelet.HHH_glrlm_RunPercentage | −0.220 | 0.802 (0.533–1.236) | 0.298 |
| T2_wavelet.HHH_ngtdm_Coarseness | 1.471 | 4.355 (0.800–29.392) | 0.106 | |
| T2_wavelet.HLH_gldm_ SmallDependenceHighGrayLevelEmphasis | −5.081 | 0.006 (5.54 × 10−6–0.687) | 0.080 | |
| T2_wavelet.HLH_glrlm_RunPercentage | 1.443 | 4.235 (1.481–26.510) | 0.045 | |
| T2_wavelet.HLL_ngtdm_Coarseness | −1.294 | 0.274 (0.043–1.324) | 0.134 | |
| T2_wavelet.LHH_gldm_ DependenceNonUniformityNormalized | 5.107 | 1.652 (1.358–4.033) | 0.104 | |
| T2_wavelet.LHH_glszm_ SizeZoneNonUniformityNormalized | 0.860 | 2.362 (1.187–5.205) | 0.022 | |
| T2_wavelet.LHH_ngtdm_Contrast | 0.722 | 2.058 (1.291–3.564) | 0.005 | |
| T2_wavelet.LHL_firstorder_RootMeanSquared | 0.270 | 1.310 (0.808–2.146) | 0.268 | |
| T2_wavelet.LLL_gldm_ SmallDependenceLowGrayLevelEmphasis | 0.025 | 1.025 (0.637–1.626) | 0.916 | |
| DWI | DWI_original_glszm_SizeZoneNonUniformityNormalized | 0.378 | 1.460 (1.0109–2.229) | 0.061 |
| DWI_original_shape_SurfaceArea | −0.443 | 0.642 (0.257–1.511) | 0.324 | |
| DWI_wavelet.HLH_glcm_MaximumProbability | −0.731 | 0.481 (0.272–0.763) | 0.005 | |
| DWI_wavelet.LLL_glrlm_RunLengthNonUniformity | −0.700 | 0.496 (0.200–1.136) | 0.109 | |
| T2WI + DWI | T2_wavelet.HLH_gldm_ SmallDependenceHighGrayLevelEmphasis | 0.947 | 2.579 (1.255–7.864) | 0.030 |
| T2_wavelet.HLH_glrlm_RunPercentage | −0.509 | 0.601 (0.278–1.236) | 0.176 | |
| T2_wavelet.HLL_ngtdm_Coarseness | 0.703 | 2.020 (0.844–6.290) | 0.181 | |
| T2_wavelet.LHH_gldm_ DependenceNonUniformityNormalized | 0.834 | 2.303 (1.171–5.080) | 0.023 | |
| T2_wavelet.LHH_glszm_ SizeZoneNonUniformityNormalized | 0.537 | 1.710 (1.059–2.955) | 0.039 | |
| T2_wavelet.LHH_ngtdm_Contrast | 0.304 | 1.355 (0.808–2.315) | 0.249 | |
| T2_wavelet.LHL_firstorder_RootMeanSquared | 0.343 | 1.409 (0.859–2.375) | 0.180 | |
| DWI_original_glszm_SizeZoneNonUniformityNormalized | 0.271 | 1.311 (0.829–2.266) | 0.289 | |
| DWI_original_shape_SurfaceArea | −0.896 | 0.408 (0.162–0.896) | 0.039 | |
| DWI_wavelet.HHH_glcm_DifferenceEntropy | 0.687 | 1.988 (1.010–4.306) | 0.064 | |
| DWI_wavelet.HLH_glcm_MaximumProbability | −0.494 | 0.610 (0.299–1.178) | 0.151 | |
| DWI_wavelet.HLL_gldm_ LargeDependenceLowGrayLevelEmphasis | 0.377 | 1.457 (0.873–2.460) | 0.152 | |
| DWI_wavelet.LHH_glszm_ZoneEntropy | −0.127 | 0.881 (0.463–1.668) | 0.697 |
| Model | Train | Test | ||||||
|---|---|---|---|---|---|---|---|---|
| AUC | Sensitivity | Specificity | P | AUC | Sensitivity | Specificity | P | |
| Clinical | 0.766 (0.698–0.834) | 0.890 | 0.522 | 0.823 (0.712–0.933) | 1 | 0.514 | ||
| T2WI | 0.813 (0.753–0.873) | 0.868 | 0.609 | 0.276 | 0.827 (0.707–0.947) | 0.611 | 0.919 | 0.959 |
| DWI | 0.749 (0.678–0.819) | 0.802 | 0.598 | 0.709 | 0.734 (0.593–0.975) | 0.556 | 0.838 | 0.269 |
| T2WI + DWI | 0.879 (0.832–0.926) | 0.736 | 0.870 | 0.003 | 0.908 (0.821–0.996) | 0.944 | 0.811 | 0.197 |
| Combined | 0.906 (0.866–0.947) | 0.780 | 0.870 | <0.01 | 0.947 (0.884–1) | 0.944 | 0.865 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, W.; Zhang, W.; Li, X.; Cao, X.; Yang, G.; Zhang, H. Predicting Tumor Perineural Invasion Status in High-Grade Prostate Cancer Based on a Clinical–Radiomics Model Incorporating T2-Weighted and Diffusion-Weighted Magnetic Resonance Images. Cancers 2023, 15, 86. https://doi.org/10.3390/cancers15010086
Zhang W, Zhang W, Li X, Cao X, Yang G, Zhang H. Predicting Tumor Perineural Invasion Status in High-Grade Prostate Cancer Based on a Clinical–Radiomics Model Incorporating T2-Weighted and Diffusion-Weighted Magnetic Resonance Images. Cancers. 2023; 15(1):86. https://doi.org/10.3390/cancers15010086
Chicago/Turabian StyleZhang, Wei, Weiting Zhang, Xiang Li, Xiaoming Cao, Guoqiang Yang, and Hui Zhang. 2023. "Predicting Tumor Perineural Invasion Status in High-Grade Prostate Cancer Based on a Clinical–Radiomics Model Incorporating T2-Weighted and Diffusion-Weighted Magnetic Resonance Images" Cancers 15, no. 1: 86. https://doi.org/10.3390/cancers15010086