
Deep Learning-Based Screening of Urothelial Carcinoma in Whole Slide Images of Liquid-Based Cytology Urine Specimens


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical Cases and Cytopathological Records
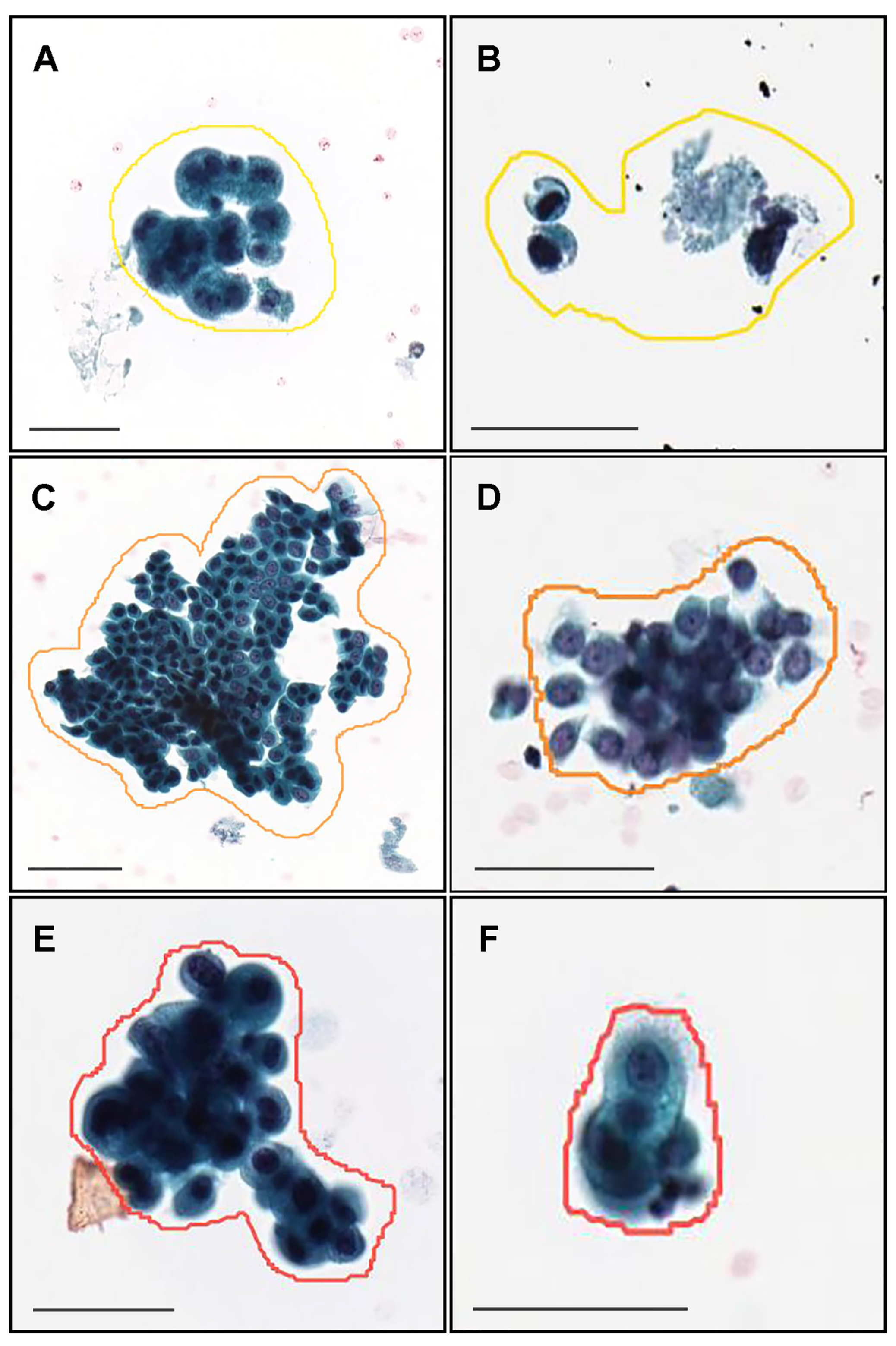
2.2. Annotation
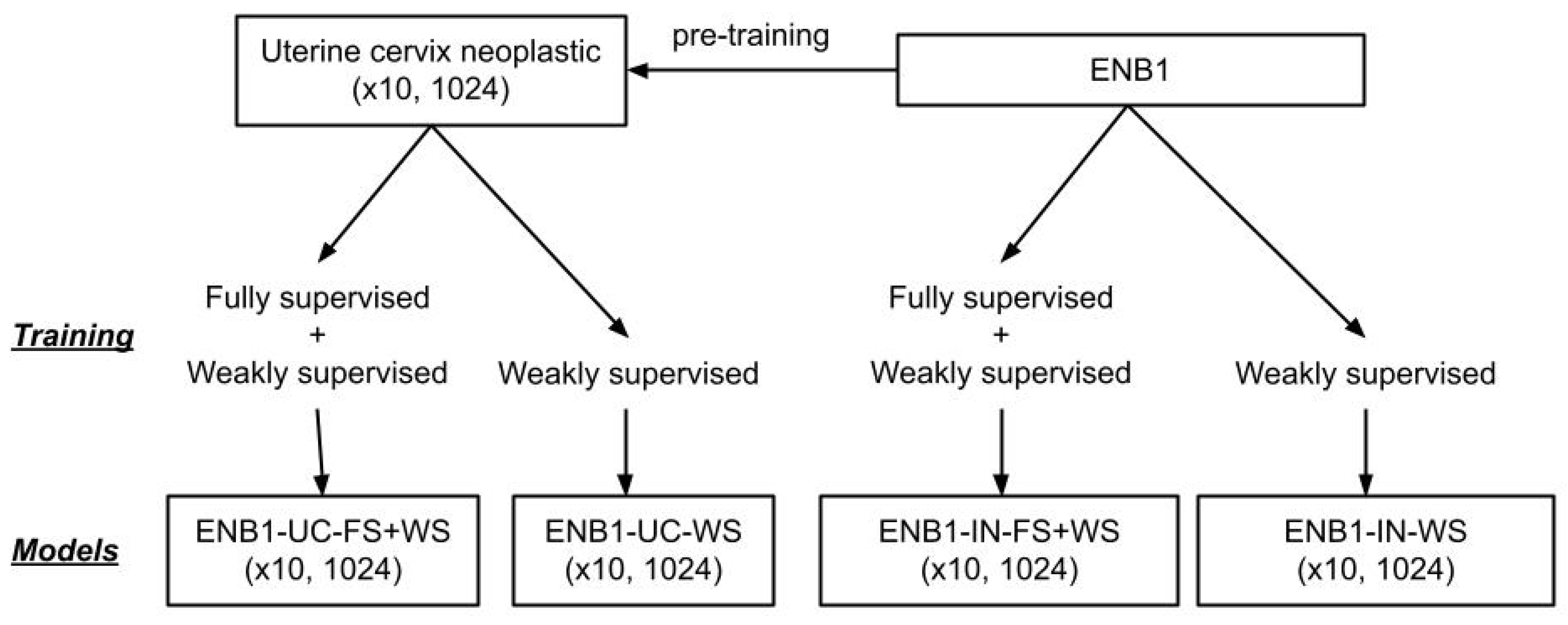
2.3. Deep Learning Models
2.4. Software and Statistical Analysis
3. Results
3.1. Insufficient AUC Performance of Whole Slide Image (WSI) Neoplastic Evaluation on Urine LBC WSIs Using Existing Series of LBC Cytopathological Model
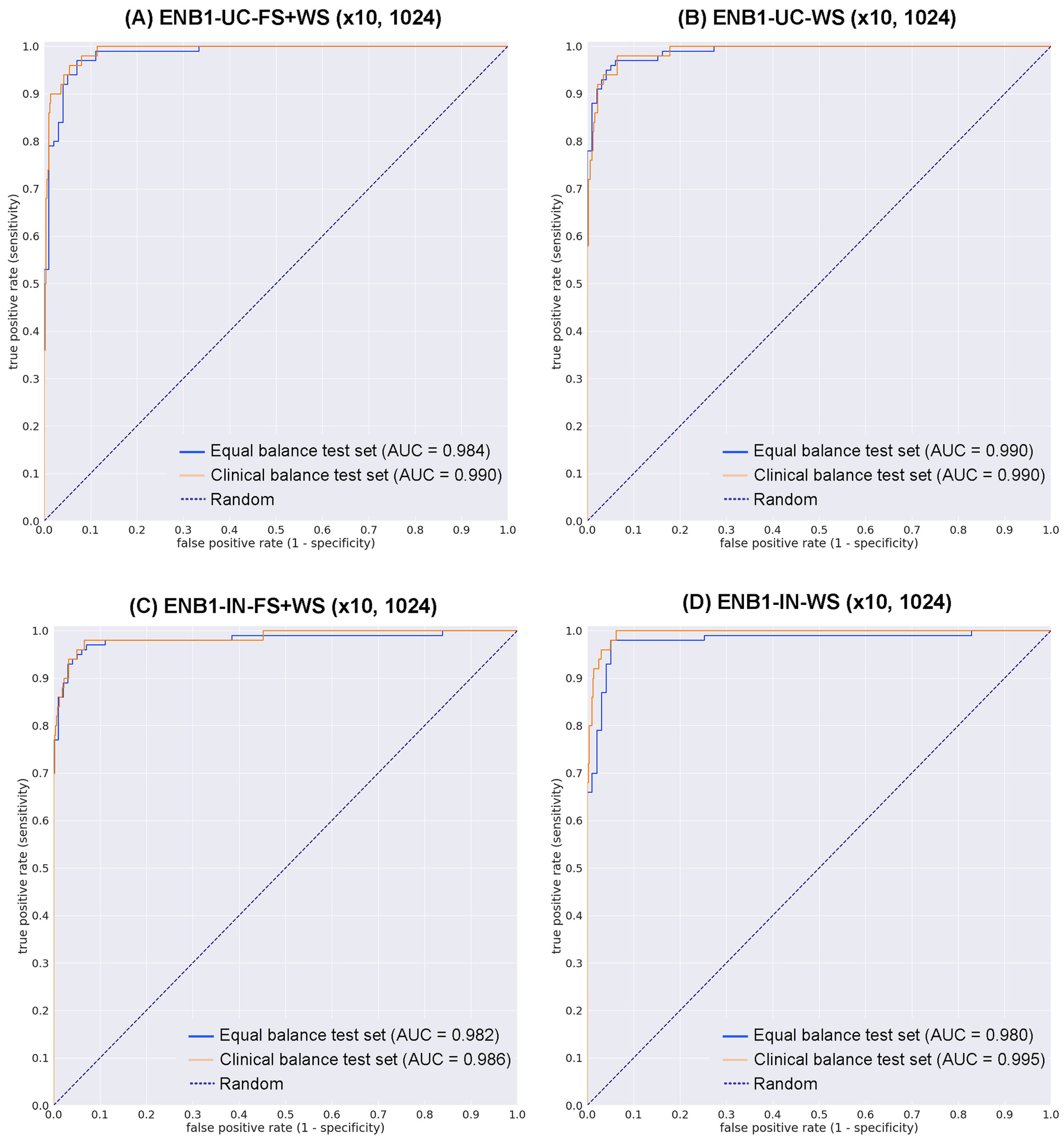
3.2. High ROC-AUC Performance of Urine LBC WSI Evaluation of Neoplastic Urothelial Epithelial Cell Screening
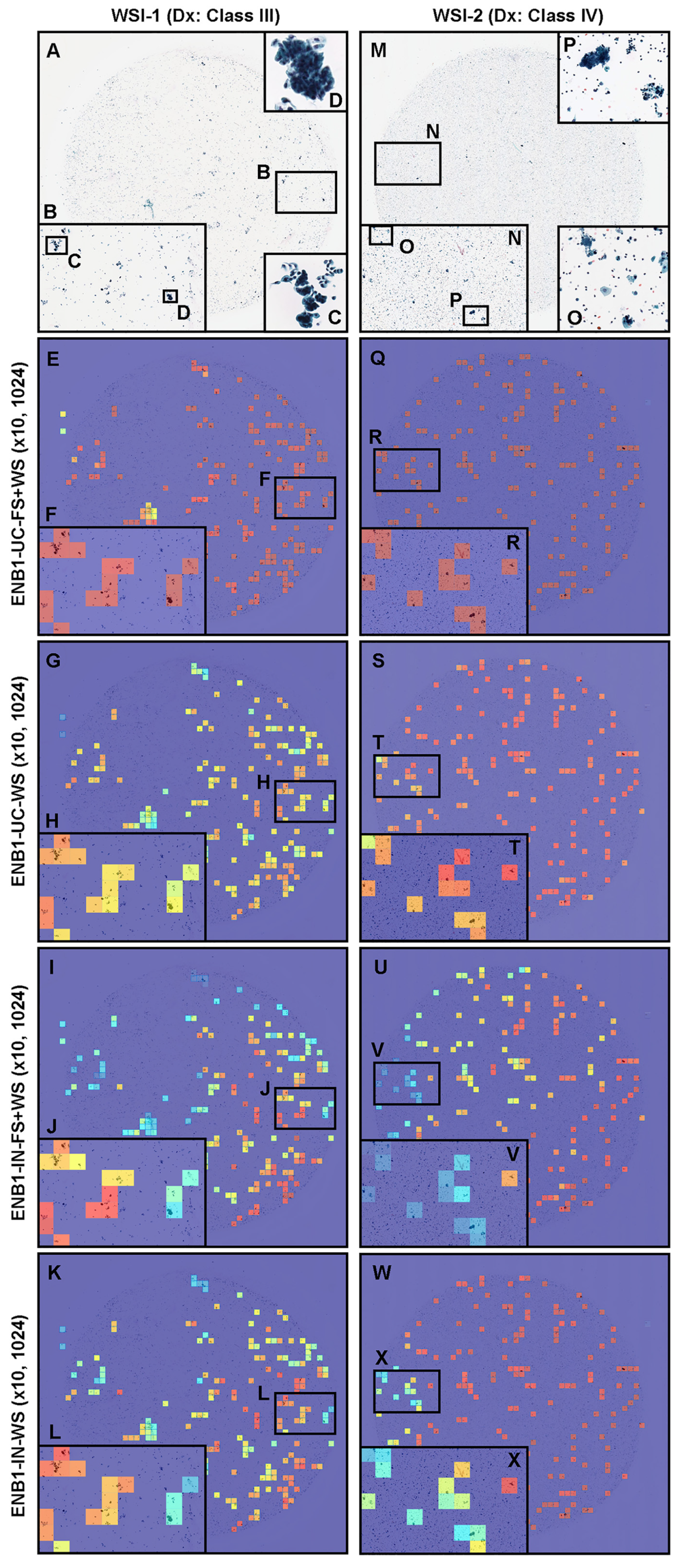
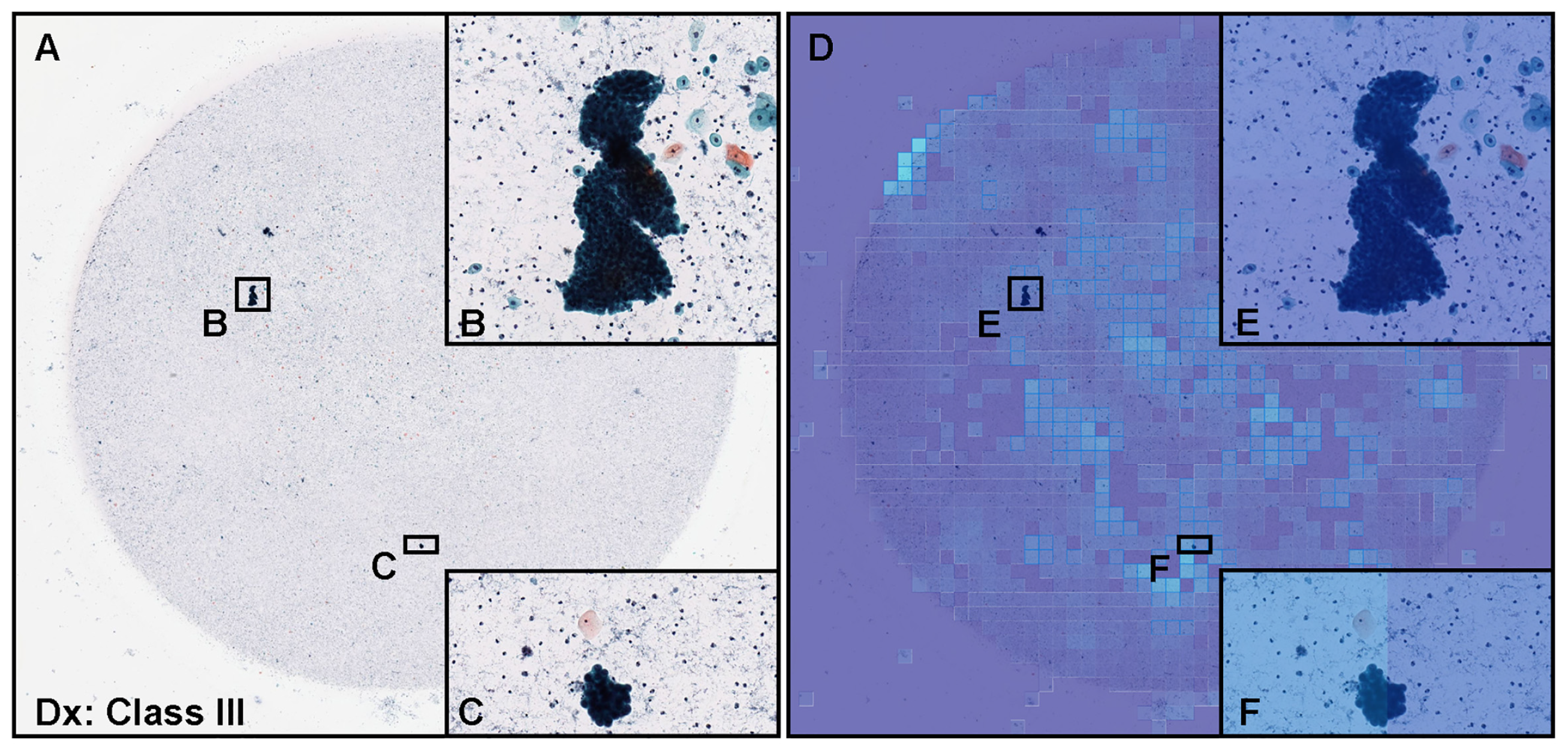
3.3. True Positive Prediction
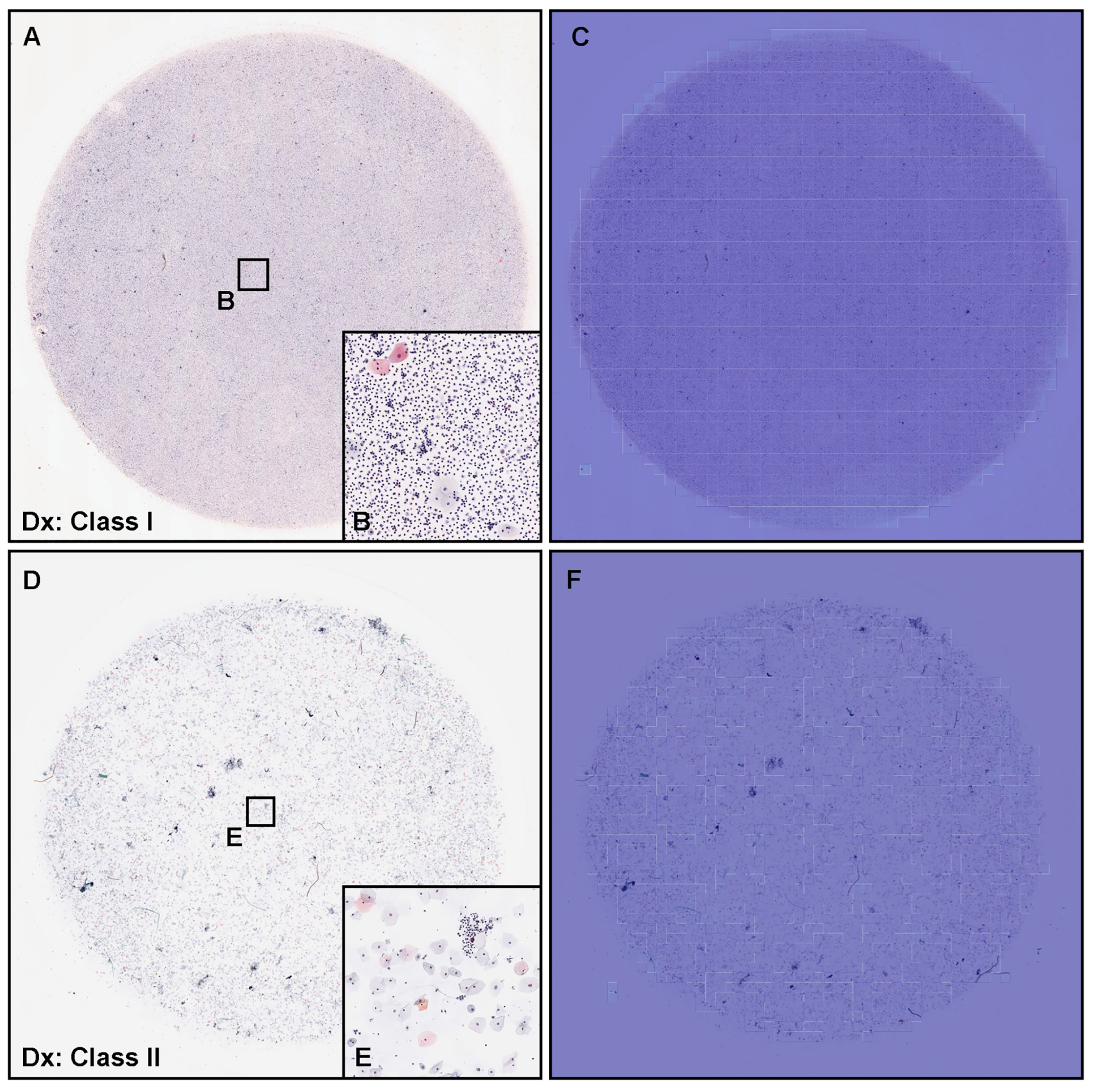
3.4. True Negative Prediction
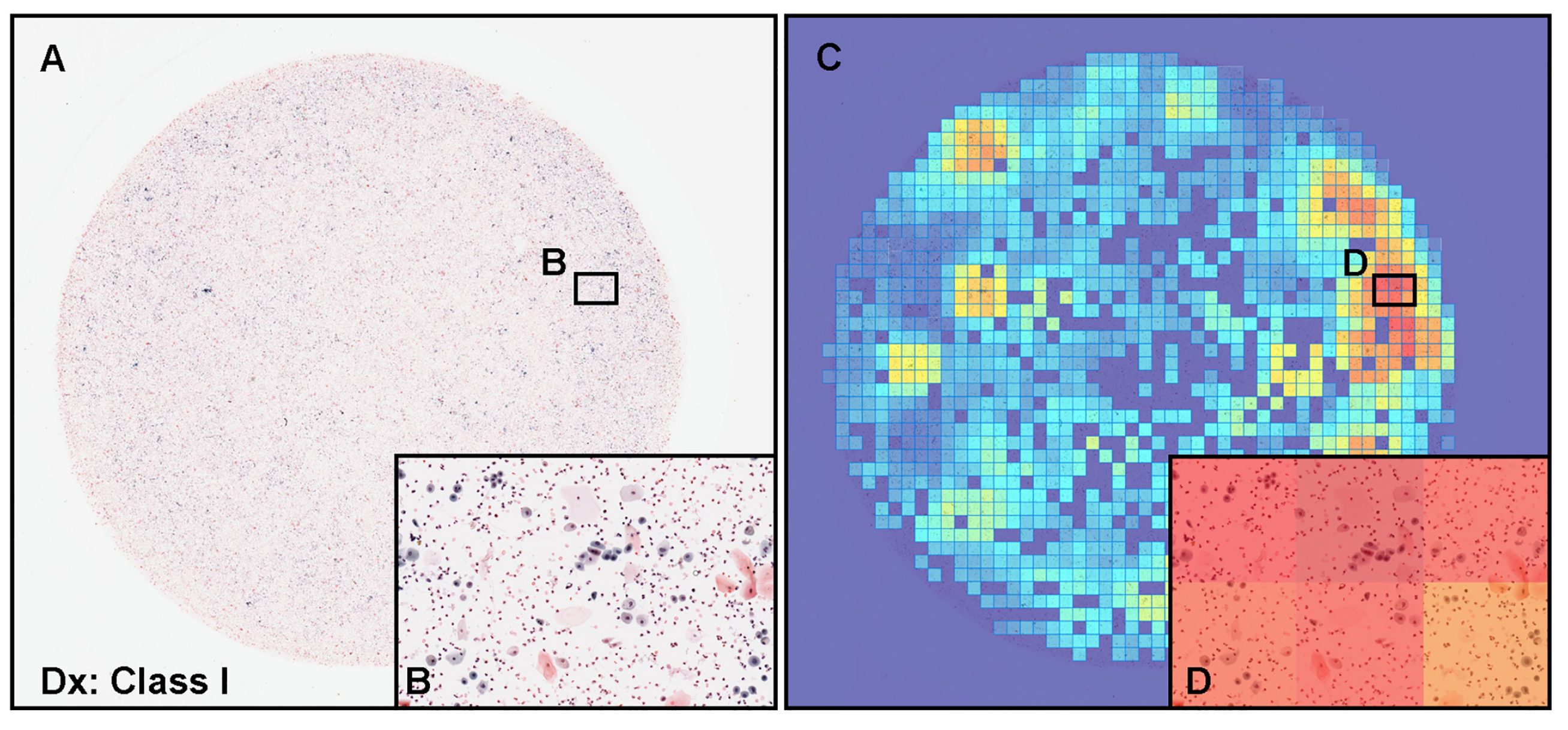
3.5. False Positive Prediction
3.6. False Negative Prediction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Northrup, V.; Acar, B.C.; Hossain, M.; Acker, M.R.; Manuel, E.; Rahmeh, T. Clinical follow up and the impact of the Paris system in the assessment of patients with atypical urine cytology. Diagn. Cytopathol. 2018, 46, 1022–1030. [Google Scholar] [CrossRef]
- Brown, F.M. Urine Cytology. Urol. Clin. N. Am. 2000, 27, 25–37. [Google Scholar] [CrossRef] [PubMed]
- DeSouza, K.; Chowdhury, S.; Hughes, S. Prompt diagnosis key in bladder cancer. Practitioner 2014, 258, 23–27. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Shanks, J.H.; Iczkowski, K.A. Divergent differentiation in urothelial carcinoma and other bladder cancer subtypes with selected mimics. Histopathology 2009, 54, 885–900. [Google Scholar] [CrossRef] [PubMed]
- Baio, R.; Spiezia, N.; Marani, C.; Schettini, M. Potential contribution of benzodiazepine abuse in the development of a bladder sarcomatoid carcinoma: A case report. Mol. Clin. Oncol. 2021, 15, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; She, D.L.; Xiong, H.; Yang, L.; Fu, S.J. Diagnostic value of liquid-based cytology in urothelial carcinoma diagnosis: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0134940. [Google Scholar] [CrossRef] [Green Version]
- Raab, S.S.; Grzybicki, D.M.; Vrbin, C.M.; Geisinger, K.R. Urine cytology discrepancies: Frequency, causes, and outcomes. Am. J. Clin. Pathol. 2007, 127, 946–953. [Google Scholar] [CrossRef]
- Sullivan, P.S.; Chan, J.B.; Levin, M.R.; Rao, J. Urine cytology and adjunct markers for detection and surveillance of bladder cancer. Am. J. Transl. Res. 2010, 2, 412. [Google Scholar]
- Bastacky, S.; Ibrahim, S.; Wilczynski, S.P.; Murphy, W.M. The accuracy of urinary cytology in daily practice. Cancer Cytopathol. Interdiscip. Int. J. Am. Cancer Soc. 1999, 87, 118–128. [Google Scholar] [CrossRef]
- Son, S.M.; Koo, J.H.; Choi, S.Y.; Lee, H.C.; Lee, Y.M.; Song, H.G.; Hwang, H.K.; Han, H.S.; Yun, S.J.; Kim, W.J.; et al. Evaluation of urine cytology in urothelial carcinoma patients: A comparison of CellprepPlus® liquid-based cytology and conventional smear. Korean J. Pathol. 2012, 46, 68. [Google Scholar] [CrossRef] [PubMed]
- Tripathy, K.; Misra, A.; Ghosh, J. Efficacy of liquid-based cytology versus conventional smears in FNA samples. J. Cytol. 2015, 32, 17. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.W.; Paik, W.H.; Lee, S.H.; Chun, J.W.; Huh, G.; Park, N.Y.; Kim, J.S.; Cho, I.R.; Ryu, J.K.; Kim, Y.T.; et al. Usefulness of Liquid-Based Cytology in Diagnosing Biliary Tract Cancer Compared to Conventional Smear and Forceps Biopsy. Dig. Dis. Sci. 2022. [Google Scholar] [CrossRef] [PubMed]
- Honarvar, Z.; Zarisfi, Z.; Sedigh, S.S.; Shahrbabak, M.M. Comparison of conventional and liquid-based Pap smear methods in the diagnosis of precancerous cervical lesions. J. Obstet. Gynaecol. 2022, 42, 2320–2324. [Google Scholar] [CrossRef] [PubMed]
- Laucirica, R.; Bentz, J.S.; Souers, R.J.; Wasserman, P.G.; Crothers, B.A.; Clayton, A.C.; Henry, M.R.; Chmara, B.A.; Clary, K.M.; Fraig, M.M.; et al. Do liquid-based preparations of urinary cytology perform differently than classically prepared cases? Observations from the College of American Pathologists Interlaboratory Comparison Program in Nongynecologic Cytology. Arch. Pathol. Lab. Med. 2010, 134, 19–22. [Google Scholar] [CrossRef]
- Grundhoefer, D.; Patterson, B.K. Determination of liquid-based cervical cytology specimen adequacy using cellular light scatter and flow cytometry. Cytometry 2001, 46, 340–344. [Google Scholar] [CrossRef]
- Austin, M.; Ramzy, I. Increased Detection of Epithelial Cell Abnormalities by Liquid-Based Gynecologic Cytology Preparations. Acta Cytol. 1998, 42, 178–184. [Google Scholar] [CrossRef]
- Makde, M.M.; Sathawane, P. Liquid-based cytology: Technical aspects. Cytojournal 2022, 19, 41. [Google Scholar] [CrossRef]
- Hussain, E.; Mahanta, L.B.; Borah, H.; Das, C.R. Liquid based-cytology Pap smear dataset for automated multi-class diagnosis of pre-cancerous and cervical cancer lesions. Data Brief 2020, 30, 105589. [Google Scholar] [CrossRef]
- Lahrmann, B.; Valous, N.A.; Eisenmann, U.; Wentzensen, N.; Grabe, N. Semantic focusing allows fully automated single-layer slide scanning of cervical cytology slides. PLoS ONE 2013, 8, e61441. [Google Scholar] [CrossRef] [Green Version]
- Shidham, V.B. Role of immunocytochemistry in cervical cancer screening. Cytojournal 2022, 19, 42. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.; Kostiuk, M.; Biron, V.L. Molecular Detection Methods in HPV-Related Cancers. Front. Oncol. 2022, 12, 864820. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.D.; Bizzarro, T.; Longatto-Filho, A.; Gerhard, R.; Schmitt, F. The diagnostic and prognostic role of liquid-based cytology: Are we ready to monitor therapy and resistance? Expert Rev. Anticancer. Ther. 2015, 15, 911–921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalantari, M.R.; Jahanshahi, M.A.; Gharib, M.; Hashemi, S.; Kalantari, S. Direct Smear Versus Liquid-Based Cytology in the Diagnosis of Bladder Lesions. Iran. J. Pathol. 2022, 17, 56. [Google Scholar] [CrossRef] [PubMed]
- Washiya, K.; Sato, T.; Miura, T.; Tone, K.; Kojima, K.; Watanabe, J.; Kijima, H. Cytologic difference between benignity and malignancy in suspicious cases employing urine cytodiagnosis using a liquid-based method. Anal. Quant. Cytol. Histol. 2011, 33, 169–174. [Google Scholar] [PubMed]
- Idrees, M.; Farah, C.S.; Sloan, P.; Kujan, O. Oral brush biopsy using liquid-based cytology is a reliable tool for oral cancer screening: A cost-utility analysis. Cancer Cytopathol. 2022, 130, 740–748. [Google Scholar] [CrossRef]
- Denton, K.J. Liquid based cytology in cervical cancer screening. BMJ 2007, 335, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Piaton, E.; Hutin, K.; Faynel, J.; Ranchin, M.; Cottier, M. Cost efficiency analysis of modern cytocentrifugation methods versus liquid based (Cytyc Thinprep®) processing of urinary samples. J. Clin. Pathol. 2004, 57, 1208–1212. [Google Scholar] [CrossRef]
- Mukhopadhyay, S.; Feldman, M.D.; Abels, E.; Ashfaq, R.; Beltaifa, S.; Cacciabeve, N.G.; Cathro, H.P.; Cheng, L.; Cooper, K.; Dickey, G.E.; et al. Whole slide imaging versus microscopy for primary diagnosis in surgical pathology: A multicenter blinded randomized noninferiority study of 1992 cases (pivotal study). Am. J. Surg. Pathol. 2018, 42, 39. [Google Scholar] [CrossRef] [Green Version]
- Malarkey, D.E.; Willson, G.A.; Willson, C.J.; Adams, E.T.; Olson, G.R.; Witt, W.M.; Elmore, S.A.; Hardisty, J.F.; Boyle, M.C.; Crabbs, T.A.; et al. Utilizing whole slide images for pathology peer review and working groups. Toxicol. Pathol. 2015, 43, 1149–1157. [Google Scholar] [CrossRef] [Green Version]
- Tsuneki, M. Deep learning models in medical image analysis. J. Oral Biosci. 2022, 64, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Tanaka, F.; Nakano, K.; Hara, T.; Yoshii, K.; Yamashita, K.; Ono, S.; Takabatake, K.; Kawai, H.; Nagatsuka, H.; et al. Effective deep learning for oral exfoliative cytology classification. Cancer Cytopathol. 2022, 130, 407–414. [Google Scholar] [CrossRef]
- Ou, Y.C.; Tsao, T.Y.; Chang, M.C.; Lin, Y.S.; Yang, W.L.; Hang, J.F.; Li, C.B.; Lee, C.M.; Yeh, C.H.; Liu, T.J. Evaluation of an artificial intelligence algorithm for assisting the Paris System in reporting urinary cytology: A pilot study. Cancer Cytopathol. 2022, 130, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Tao, X.; Chu, X.; Guo, B.; Pan, Q.; Ji, S.; Lou, W.; Lv, C.; Xie, G.; Hua, K. Scrutinizing high-risk patients from ASC-US cytology via a deep learning model. Cancer Cytopathol. 2022, preprint. [Google Scholar] [CrossRef] [PubMed]
- Kanavati, F.; Hirose, N.; Ishii, T.; Fukuda, A.; Ichihara, S.; Tsuneki, M. A Deep Learning Model for Cervical Cancer Screening on Liquid-Based Cytology Specimens in Whole Slide Images. Cancers 2022, 14, 1159. [Google Scholar] [CrossRef]
- Xie, X.; Fu, C.C.; Lv, L.; Ye, Q.; Yu, Y.; Fang, Q.; Zhang, L.; Hou, L.; Wu, C. Deep convolutional neural network-based classification of cancer cells on cytological pleural effusion images. Mod. Pathol. 2022, 35, 609–614. [Google Scholar] [CrossRef]
- Lin, Y.J.; Chao, T.K.; Khalil, M.A.; Lee, Y.C.; Hong, D.Z.; Wu, J.J.; Wang, C.W. Deep Learning Fast Screening Approach on Cytological Whole Slides for Thyroid Cancer Diagnosis. Cancers 2021, 13, 3891. [Google Scholar] [CrossRef]
- Bhatt, A.R.; Ganatra, A.; Kotecha, K. Cervical cancer detection in pap smear whole slide images using convnet with transfer learning and progressive resizing. PeerJ Comput. Sci. 2021, 7, e348. [Google Scholar] [CrossRef]
- Holmström, O.; Linder, N.; Kaingu, H.; Mbuuko, N.; Mbete, J.; Kinyua, F.; Törnquist, S.; Muinde, M.; Krogerus, L.; Lundin, M.; et al. Point-of-Care Digital Cytology With Artificial Intelligence for Cervical Cancer Screening in a Resource-Limited Setting. JAMA Netw. Open 2021, 4, e211740. [Google Scholar] [CrossRef]
- Lin, H.; Chen, H.; Wang, X.; Wang, Q.; Wang, L.; Heng, P.A. Dual-path network with synergistic grouping loss and evidence driven risk stratification for whole slide cervical image analysis. Med. Image Anal. 2021, 69, 101955. [Google Scholar] [CrossRef]
- Cheng, S.; Liu, S.; Yu, J.; Rao, G.; Xiao, Y.; Han, W.; Zhu, W.; Lv, X.; Li, N.; Cai, J.; et al. Robust whole slide image analysis for cervical cancer screening using deep learning. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, Long Beach, CA, USA, 10–15 May 2019; PMLR: London, UK, 2019; pp. 6105–6114. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity mappings in deep residual networks. In Proceedings of the European Conference on Computer Vision, Amsterdam, The Netherlands, 11–14 October 2016; Springer: Berlin/Heidelberg, Germany, 2016; pp. 630–645. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Kanavati, F.; Tsuneki, M. Partial transfusion: On the expressive influence of trainable batch norm parameters for transfer learning. arXiv 2021, arXiv:2102.05543. [Google Scholar]
- Tsuneki, M.; Abe, M.; Kanavati, F. Transfer Learning for Adenocarcinoma Classifications in the Transurethral Resection of Prostate Whole-Slide Images. Cancers 2022, 14, 4744. [Google Scholar] [CrossRef]
- Otsu, N. A threshold selection method from gray-level histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Goode, A.; Gilbert, B.; Harkes, J.; Jukic, D.; Satyanarayanan, M. OpenSlide: A vendor-neutral software foundation for digital pathology. J. Pathol. Inform. 2013, 4, 27. [Google Scholar] [CrossRef]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Abadi, M.; Agarwal, A.; Barham, P.; Brevdo, E.; Chen, Z.; Citro, C.; Corrado, G.S.; Davis, A.; Dean, J.; Devin, M.; et al. TensorFlow: Large-Scale Machine Learning on Heterogeneous Systems. 2015. Available online: tensorflow.org (accessed on 16 June 2021).
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Hunter, J.D. Matplotlib: A 2D graphics environment. Comput. Sci. Eng. 2007, 9, 90–95. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; CRC Press: Boca Raton, FL, USA, 1994. [Google Scholar]
- Kanavati, F.; Ichihara, S.; Rambeau, M.; Iizuka, O.; Arihiro, K.; Tsuneki, M. Deep learning models for gastric signet ring cell carcinoma classification in whole slide images. Technol. Cancer Res. Treat. 2021, 20, 15330338211027901. [Google Scholar] [CrossRef]
- Kanavati, F.; Toyokawa, G.; Momosaki, S.; Rambeau, M.; Kozuma, Y.; Shoji, F.; Yamazaki, K.; Takeo, S.; Iizuka, O.; Tsuneki, M. Weakly-supervised learning for lung carcinoma classification using deep learning. Sci. Rep. 2020, 10, 9297. [Google Scholar] [CrossRef]
- Sanghvi, A.B.; Allen, E.Z.; Callenberg, K.M.; Pantanowitz, L. Performance of an artificial intelligence algorithm for reporting urine cytopathology. Cancer Cytopathol. 2019, 127, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.; Solomides, C.; Draganova-Tacheva, R.; Bibbo, M. Overview of nongynecological samples prepared with liquid-based cytology medium. Acta Cytol. 2014, 58, 522–532. [Google Scholar] [CrossRef]
- Nasuti, J.F.; Tam, D.; Gupta, P.K. Diagnostic value of liquid-based (Thinprep®) preparations in nongynecologic cases. Diagn. Cytopathol. 2001, 24, 137–141. [Google Scholar] [CrossRef]
- Raisi, O.; Magnani, C.; Bigiani, N.; Cianciavicchia, E.; D’Amico, R.; Muscatello, U.; Ghirardini, C. The diagnostic reliability of urinary cytology: A retrospective study. Diagn. Cytopathol. 2012, 40, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.; Mulè, A.; Russo, R.; Pierconti, F.; Fadda, G. Application of liquid-based preparation to non-gynaecologic exfoliative cytology. Pathologica 2008, 100, 461–465. [Google Scholar] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training | Validation | Test (Equal Balance) | Test (Clinical Balance) | Total | |
|---|---|---|---|---|---|
| Negative | 724 | 10 | 100 | 500 | 1334 |
| Class I | 360 | 5 | 50 | 250 | 665 |
| Class II | 364 | 5 | 50 | 250 | 669 |
| Neoplastic | 62 | 10 | 100 | 50 | 222 |
| Class III | 38 | 4 | 48 | 20 | 110 |
| Class IV | 11 | 3 | 23 | 14 | 51 |
| Class V | 13 | 3 | 29 | 16 | 61 |
| Total | 786 | 20 | 200 | 550 | 1556 |
| Annotation Label | Number of Annotation |
|---|---|
| Atypical cell | 9950 |
| Low-grade urothelial carcinoma (LGUC) cell | 1646 |
| High-grade urothelial carcinoma (HGUC) cell | 1611 |
| Total | 13,207 |
| Existing Models | ROC-AUC | Log Loss |
|---|---|---|
| Liquid-based cytology (LBC) | ||
| Uterine cervix Neoplastic (×10, 1024) | 0.836 [0.775–0.885] | 0.778 [0.620–0.989] |
| Test Set | ||
|---|---|---|
| Equal Balance | Clinical Balance | |
| ENB1-UC-FS+WS (×10, 1024) | ||
| ROC-AUC | 0.984 [0.969–0.995] | 0.990 [0.982–0.996] |
| Log-loss | 0.180 [0.123–0.259] | 0.223 [0.181–0.284] |
| Accuracy | 0.945 [0.905–0.970] | 0.946 [0.924–0.962] |
| Sensitivity | 0.960 [0.920–0.990] | 0.940 [0.861–1.000] |
| Specificity | 0.929 [0.862–0.972] | 0.946 [0.924–0.964] |
| ENB1-UC-WS (×10, 1024) | ||
| ROC-AUC | 0.990 [0.985–0.999] | 0.990 [0.981–0.997] |
| Log-loss | 0.251 [0.178–0.295] | 0.098 [0.081–0.119] |
| Accuracy | 0.955 [0.935–0.985] | 0.940 [0.920–0.960] |
| Sensitivity | 0.950 [0.911–0.990] | 0.980 [0.933–1.000] |
| Specificity | 0.960 [0.931–1.000] | 0.936 [0.915–0.958] |
| ENB1-IN-FS+WS (×10, 1024) | ||
| ROC-AUC | 0.982 [0.957–0.996] | 0.986 [0.963–0.998] |
| Log-loss | 0.225 [0.156–0.321] | 0.082 [0.063–0.106] |
| Accuracy | 0.950 [0.910–0.975] | 0.936 [0.918–0.956] |
| Sensitivity | 0.930 [0.863–0.971] | 0.960 [0.894–1.000] |
| Specificity | 0.970 [0.930–1.000] | 0.934 [0.914–0.955] |
| ENB1-IN-WS (×10, 1024) | ||
| ROC-AUC | 0.980 [0.960–0.997] | 0.995 [0.990–0.998] |
| Log-loss | 0.258 [0.185–0.289] | 0.128 [0.114–0.144] |
| Accuracy | 0.960 [0.940–0.990] | 0.944 [0.924–0.960] |
| Sensitivity | 0.970 [0.945–1.000] | 1.000 [1.000–1.000] |
| Specificity | 0.950 [0.914–0.990] | 0.938 [0.915–0.956] |
| ResNet50V2-IN-FS+WS (×10, 1024) | ||
| ROC-AUC | 0.962 [0.919–0.986] | 0.972 [0.935–1.000] |
| Log-loss | 0.238 [0.145–0.357] | 0.085 [0.050–0.124] |
| Accuracy | 0.916 [0.865–0.955] | 0.915 [0.884–0.950] |
| Sensitivity | 0.888 [0.812–0.937] | 0.949 [0.874–1.000] |
| Specificity | 0.945 [0.895–0.993] | 0.914 [0.875–0.950] |
| DenseNet121-IN-FS+WS (×10, 1024) | ||
| ROC-AUC | 0.945 [0.905–0.977] | 0.957 [0.922–0.988] |
| Log-loss | 0.233 [0.152–0.345] | 0.185 [0.146–0.224] |
| Accuracy | 0.919 [0.867–0.962] | 0.925 [0.887–0.958] |
| Sensitivity | 0.919 [0.835–0.977] | 0.921 [0.846–0.971] |
| Specificity | 0.957 [0.905–1.000] | 0.906 [0.869–0.945] |
| InceptionV3-IN-FS+WS (×10, 1024) | ||
| ROC-AUC | 0.959 [0.923–0.983] | 0.978 [0.940–1.000] |
| Log-loss | 0.239 [0.151–0.354] | 0.186 [0.177–0.198] |
| Accuracy | 0.912 [0.857–0.955] | 0.924 [0.895–0.959] |
| Sensitivity | 0.898 [0.820–0.957] | 0.956 [0.878–1.000] |
| Specificity | 0.954 [0.895–0.995] | 0.906 [0.868–0.941] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsuneki, M.; Abe, M.; Kanavati, F. Deep Learning-Based Screening of Urothelial Carcinoma in Whole Slide Images of Liquid-Based Cytology Urine Specimens. Cancers 2023, 15, 226. https://doi.org/10.3390/cancers15010226
Tsuneki M, Abe M, Kanavati F. Deep Learning-Based Screening of Urothelial Carcinoma in Whole Slide Images of Liquid-Based Cytology Urine Specimens. Cancers. 2023; 15(1):226. https://doi.org/10.3390/cancers15010226
Chicago/Turabian StyleTsuneki, Masayuki, Makoto Abe, and Fahdi Kanavati. 2023. "Deep Learning-Based Screening of Urothelial Carcinoma in Whole Slide Images of Liquid-Based Cytology Urine Specimens" Cancers 15, no. 1: 226. https://doi.org/10.3390/cancers15010226