
Phase II Trial of the Combination of Alectinib with Bevacizumab in Alectinib Refractory ALK-Positive Nonsquamous Non-Small-Cell Lung Cancer (NLCTG1501)
 , , and add
Show full author list
, , and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Treatment
2.3. Study Design
2.4. Clinical Assessments
2.5. Biomarker Studies
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Drug Exposure and Tumor Response
3.3. Efficacy
3.4. Safety
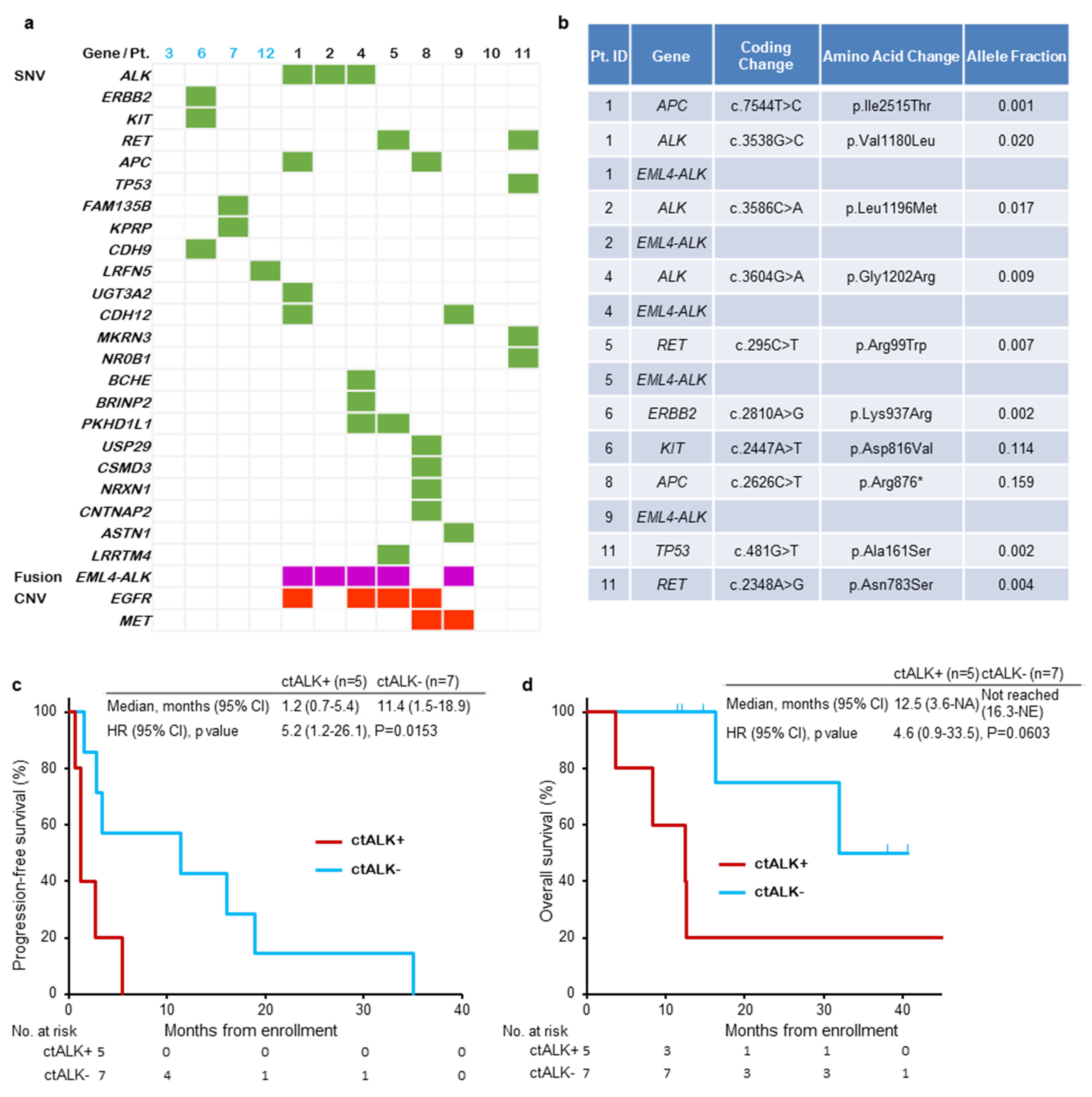
3.5. Biomarker Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jordan, E.J.; Kim, H.R.; Arcila, M.E.; Barron, D.; Chakravarty, D.; Gao, J.; Chang, M.T.; Ni, A.; Kundra, R.; Jonsson, P.; et al. Prospective comprehensive molecular characterization of lung adenocarcinomas for efficient patient matching to approved and emerging therapies. Cancer Discov. 2017, 7, 596–609. [Google Scholar] [CrossRef] [Green Version]
- Soda, M.; Choi, Y.L.; Enomoto, M.; Takada, S.; Yamashita, Y.; Ishikawa, S.; Fujiwara, S.; Watanabe, H.; Kurashina, K.; Hatanaka, H.; et al. Identification of the transforming eml4-alk fusion gene in non-small-cell lung cancer. Nature 2007, 448, 561–566. [Google Scholar] [CrossRef]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Wu, Y.L.; Nakagawa, K.; Mekhail, T.; Felip, E.; Cappuzzo, F.; Paolini, J.; Usari, T.; et al. First-line crizotinib versus chemotherapy in alk-positive lung cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [Green Version]
- Soria, J.-C.; Tan, D.S.W.; Chiari, R.; Wu, Y.-L.; Paz-Ares, L.; Wolf, J.; Geater, S.L.; Orlov, S.; Cortinovis, D.; Yu, C.-J.; et al. First-line ceritinib versus platinum-based chemotherapy in advanced alk -rearranged non-small-cell lung cancer (ascend-4): A randomised, open-label, phase 3 study. Lancet 2017, 389, 917–929. [Google Scholar] [CrossRef] [PubMed]
- Hida, T.; Nokihara, H.; Kondo, M.; Kim, Y.H.; Azuma, K.; Seto, T.; Takiguchi, Y.; Nishio, M.; Yoshioka, H.; Imamura, F.; et al. Alectinib versus crizotinib in patients with alk -positive non-small-cell lung cancer (j-alex): An open-label, randomised phase 3 trial. Lancet 2017, 390, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.W.; Ou, S.I.; Perol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus crizotinib in untreated alk-positive non-small-cell lung cancer. N. Engl. J. Med. 2017, 377, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Bauer, T.M.; de Marinis, F.; Felip, E.; Goto, Y.; Liu, G.; Mazieres, J.; Kim, D.W.; Mok, T.; Polli, A.; et al. First-line lorlatinib or crizotinib in advanced alk-positive lung cancer. N. Engl. J. Med. 2020, 383, 2018–2029. [Google Scholar] [CrossRef]
- Camidge, D.R.; Kim, H.R.; Ahn, M.J.; Yang, J.C.; Han, J.Y.; Lee, J.S.; Hochmair, M.J.; Li, J.Y.; Chang, G.C.; Lee, K.H.; et al. Brigatinib versus crizotinib in alk-positive non-small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2027–2039. [Google Scholar] [CrossRef]
- Sandler, A.; Gray, R.; Perry, M.C.; Brahmer, J.; Schiller, J.H.; Dowlati, A.; Lilenbaum, R.; Johnson, D.H. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N. Engl. J. Med. 2006, 355, 2542–2550. [Google Scholar] [CrossRef] [Green Version]
- Seto, T.; Kato, T.; Nishio, M.; Goto, K.; Atagi, S.; Hosomi, Y.; Yamamoto, N.; Hida, T.; Maemondo, M.; Nakagawa, K.; et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring egfr mutations (jo25567): An open-label, randomised, multicentre, phase 2 study. Lancet Oncol. 2014, 15, 1236–1244. [Google Scholar] [CrossRef]
- Saito, H.; Fukuhara, T.; Furuya, N.; Watanabe, K.; Sugawara, S.; Iwasawa, S.; Tsunezuka, Y.; Yamaguchi, O.; Okada, M.; Yoshimori, K.; et al. Erlotinib plus bevacizumab versus erlotinib alone in patients with egfr-positive advanced non-squamous non-small-cell lung cancer (nej026): Interim analysis of an open-label, randomised, multicentre, phase 3 trial. Lancet Oncol. 2019, 20, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Oxnard, G.R.; Arcila, M.E.; Chmielecki, J.; Ladanyi, M.; Miller, V.A.; Pao, W. New strategies in overcoming acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in lung cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2011, 17, 5530–5537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaft, J.E.; Oxnard, G.R.; Sima, C.S.; Kris, M.G.; Miller, V.A.; Riely, G.J. Disease flare after tyrosine kinase inhibitor discontinuation in patients with egfr-mutant lung cancer and acquired resistance to erlotinib or gefitinib: Implications for clinical trial design. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2011, 17, 6298–6303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pop, O.; Pirvu, A.; Toffart, A.C.; Moro-Sibilot, D. Disease flare after treatment discontinuation in a patient with eml4-alk lung cancer and acquired resistance to crizotinib. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2012, 7, e1–e2. [Google Scholar] [CrossRef] [Green Version]
- Ou, S.H.; Janne, P.A.; Bartlett, C.H.; Tang, Y.; Kim, D.W.; Otterson, G.A.; Crino, L.; Selaru, P.; Cohen, D.P.; Clark, J.W.; et al. Clinical benefit of continuing alk inhibition with crizotinib beyond initial disease progression in patients with advanced alk-positive nsclc. Ann. Oncol. 2014, 25, 415–422. [Google Scholar] [CrossRef]
- Park, K.; Yu, C.J.; Kim, S.W.; Lin, M.C.; Sriuranpong, V.; Tsai, C.M.; Lee, J.S.; Kang, J.H.; Chan, K.C.; Perez-Moreno, P.; et al. First-line erlotinib therapy until and beyond response evaluation criteria in solid tumors progression in asian patients with epidermal growth factor receptor mutation-positive non-small-cell lung cancer: The aspiration study. JAMA Oncol. 2016, 2, 305–312. [Google Scholar] [CrossRef]
- Hida, T.; Seto, T.; Horinouchi, H.; Maemondo, M.; Takeda, M.; Hotta, K.; Hirai, F.; Kim, Y.H.; Matsumoto, S.; Ito, M.; et al. Phase ii study of ceritinib in alectinib-pretreated patients with anaplastic lymphoma kinase-rearranged metastatic non-small-cell lung cancer in japan: Ascend-9. Cancer Sci. 2018, 109, 2863–2872. [Google Scholar] [CrossRef]
- Solomon, B.J.; Besse, B.; Bauer, T.M.; Felip, E.; Soo, R.A.; Camidge, D.R.; Chiari, R.; Bearz, A.; Lin, C.C.; Gadgeel, S.M.; et al. Lorlatinib in patients with alk-positive non-small-cell lung cancer: Results from a global phase 2 study. Lancet Oncol. 2018, 19, 1654–1667. [Google Scholar] [CrossRef]
- Seto, T.; Hayashi, H.; Satouchi, M.; Goto, Y.; Niho, S.; Nogami, N.; Hida, T.; Takahashi, T.; Sakakibara-Konishi, J.; Morise, M.; et al. Lorlatinib in previously treated anaplastic lymphoma kinase-rearranged non-small cell lung cancer: Japanese subgroup analysis of a global study. Cancer Sci. 2020, 111, 3726–3738. [Google Scholar] [CrossRef]
- Lin, J.J.; Zhu, V.W.; Schoenfeld, A.J.; Yeap, B.Y.; Saxena, A.; Ferris, L.A.; Dagogo-Jack, I.; Farago, A.F.; Taber, A.; Traynor, A.; et al. Brigatinib in patients with alectinib-refractory alk-positive nsclc. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2018, 13, 1530–1538. [Google Scholar] [CrossRef]
- Lin, J.J.; Muzikansky, A.; Kennedy, E.; Kuberski, H.; Stober, L.L.; Wanat, A.C.; Azzoli, C.G.; Lennes, I.; Sequist, L.V.; Dagogo-Jack, I.; et al. Safety and activity of alectinib plus bevacizumab in patients with advanced alk-rearranged non-small-cell lung cancer: A phase i/ii study. ESMO Open 2021, 7, 100342. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.T.; Chiang, C.L.; Hung, J.Y.; Lee, M.H.; Su, W.C.; Wu, S.Y.; Wei, Y.F.; Lee, K.Y.; Tseng, Y.H.; Su, J.; et al. Resistance profiles of anaplastic lymphoma kinase tyrosine kinase inhibitors in advanced non-small-cell lung cancer: A multicenter study using targeted next-generation sequencing. Eur. J. Cancer 2021, 156, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Gainor, J.F.; Dardaei, L.; Yoda, S.; Friboulet, L.; Leshchiner, I.; Katayama, R.; Dagogo-Jack, I.; Gadgeel, S.; Schultz, K.; Singh, M.; et al. Molecular mechanisms of resistance to first- and second-generation alk inhibitors in alk-rearranged lung cancer. Cancer Discov. 2016, 6, 1118–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, T.; Gorbunova, V.; Juhasz, E.; Szima, B.; Burdaeva, O.; Orlov, S.; Yu, C.J.; Archer, V.; Hilton, M.; Delmar, P.; et al. A correlative biomarker analysis of the combination of bevacizumab and carboplatin-based chemotherapy for advanced nonsquamous non-small-cell lung cancer: Results of the phase ii randomized abigail study (bo21015). J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2014, 9, 848–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, H.; Ichihara, E.; Kayatani, H.; Makimoto, G.; Ninomiya, K.; Nishii, K.; Higo, H.; Ando, C.; Okawa, S.; Nakasuka, T.; et al. Vegfr2 blockade augments the effects of tyrosine kinase inhibitors by inhibiting angiogenesis and oncogenic signaling in oncogene-driven non-small-cell lung cancers. Cancer Sci. 2021, 112, 1853–1864. [Google Scholar] [CrossRef]
- Masuda, C.; Yanagisawa, M.; Yorozu, K.; Kurasawa, M.; Furugaki, K.; Ishikura, N.; Iwai, T.; Sugimoto, M.; Yamamoto, K. Bevacizumab counteracts vegf-dependent resistance to erlotinib in an egfr-mutated nsclc xenograft model. Int. J. Oncol. 2017, 51, 425–434. [Google Scholar] [CrossRef] [Green Version]
- Nakagawa, K.; Hida, T.; Nokihara, H.; Morise, M.; Azuma, K.; Kim, Y.H.; Seto, T.; Takiguchi, Y.; Nishio, M.; Yoshioka, H.; et al. Final progression-free survival results from the j-alex study of alectinib versus crizotinib in alk-positive non-small-cell lung cancer. Lung Cancer 2020, 139, 195–199. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 12 | % |
|---|---|---|
| Age (y) | ||
| Median (range) | 67 (30–77) | |
| Gender | ||
| Male | 2 | 17 |
| Female | 10 | 83 |
| Performance status | ||
| 0/1/2 | 1/10/1 | 8/83/8 |
| Histology | ||
| Adenocarcinoma | 12 | 100 |
| Clinical Stage | ||
| Stage IIIB | 2 | 17 |
| Stage IV | 10 | 83 |
| Diagnosis methods | ||
| FISH | 11 | 92 |
| IHC | 10 | 83 |
| RT-PCR | 2 | 17 |
| Previous regimens | ||
| 1/2/≥3 | 3/3/6 | 25/25/50 |
| Previous ALK-TKI | ||
| Alectinib | 12 | 100 |
| Crizotinib | 9 | 75 |
| Ceritinib | 2 | 17 |
| Best response to prior alectinib | ||
| CR/PR/SD | 1/7/4 | 8/58/33 |
| Grade 1/2 | Grade≥ 3 | |
| Anemia | 3 | 1 |
| Stomatitis | 2 | |
| Appetite loss | 5 | |
| Nausea/vomiting | 1 | |
| Diarrhea | 1 | 1 |
| Constipation | 1 | |
| Hypertension | 4 | |
| Fatigue | 4 | |
| Blood bilirubin increased | 1 | |
| AST/ALT elevation | 1 | |
| Creatinin elevation | 3 | |
| Hyponatremia | 1 | |
| Hypokalemia | 1 | |
| Proteinuria | 4 | 1 |
| Edema | 2 | |
| Infection | 1 | |
| Pain | 2 | |
| Epistaxis | 2 | |
| Headache | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, S.; Sakai, K.; Matsumoto, N.; Koshio, J.; Ishida, A.; Abe, T.; Ishikawa, D.; Tanaka, T.; Aoki, A.; Kajiwara, T.; et al. Phase II Trial of the Combination of Alectinib with Bevacizumab in Alectinib Refractory ALK-Positive Nonsquamous Non-Small-Cell Lung Cancer (NLCTG1501). Cancers 2023, 15, 204. https://doi.org/10.3390/cancers15010204
Watanabe S, Sakai K, Matsumoto N, Koshio J, Ishida A, Abe T, Ishikawa D, Tanaka T, Aoki A, Kajiwara T, et al. Phase II Trial of the Combination of Alectinib with Bevacizumab in Alectinib Refractory ALK-Positive Nonsquamous Non-Small-Cell Lung Cancer (NLCTG1501). Cancers. 2023; 15(1):204. https://doi.org/10.3390/cancers15010204
Chicago/Turabian StyleWatanabe, Satoshi, Kazuko Sakai, Naoya Matsumoto, Jun Koshio, Akira Ishida, Tetsuya Abe, Daisuke Ishikawa, Tomohiro Tanaka, Ami Aoki, Tomosue Kajiwara, and et al. 2023. "Phase II Trial of the Combination of Alectinib with Bevacizumab in Alectinib Refractory ALK-Positive Nonsquamous Non-Small-Cell Lung Cancer (NLCTG1501)" Cancers 15, no. 1: 204. https://doi.org/10.3390/cancers15010204