
Histology Classification Highlights Differences in Efficacy of S-1 versus Capecitabine, in Combination with Cisplatin, for HER2-Negative Unresectable Advanced or Recurrent Gastric Cancer with Measurable Disease
 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Design and Treatment
2.2. Patients
2.3. Endpoints and Assessments
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Survival
ORR, Distribution of Tumor Shrinkage, and Changes in Tumor Burden
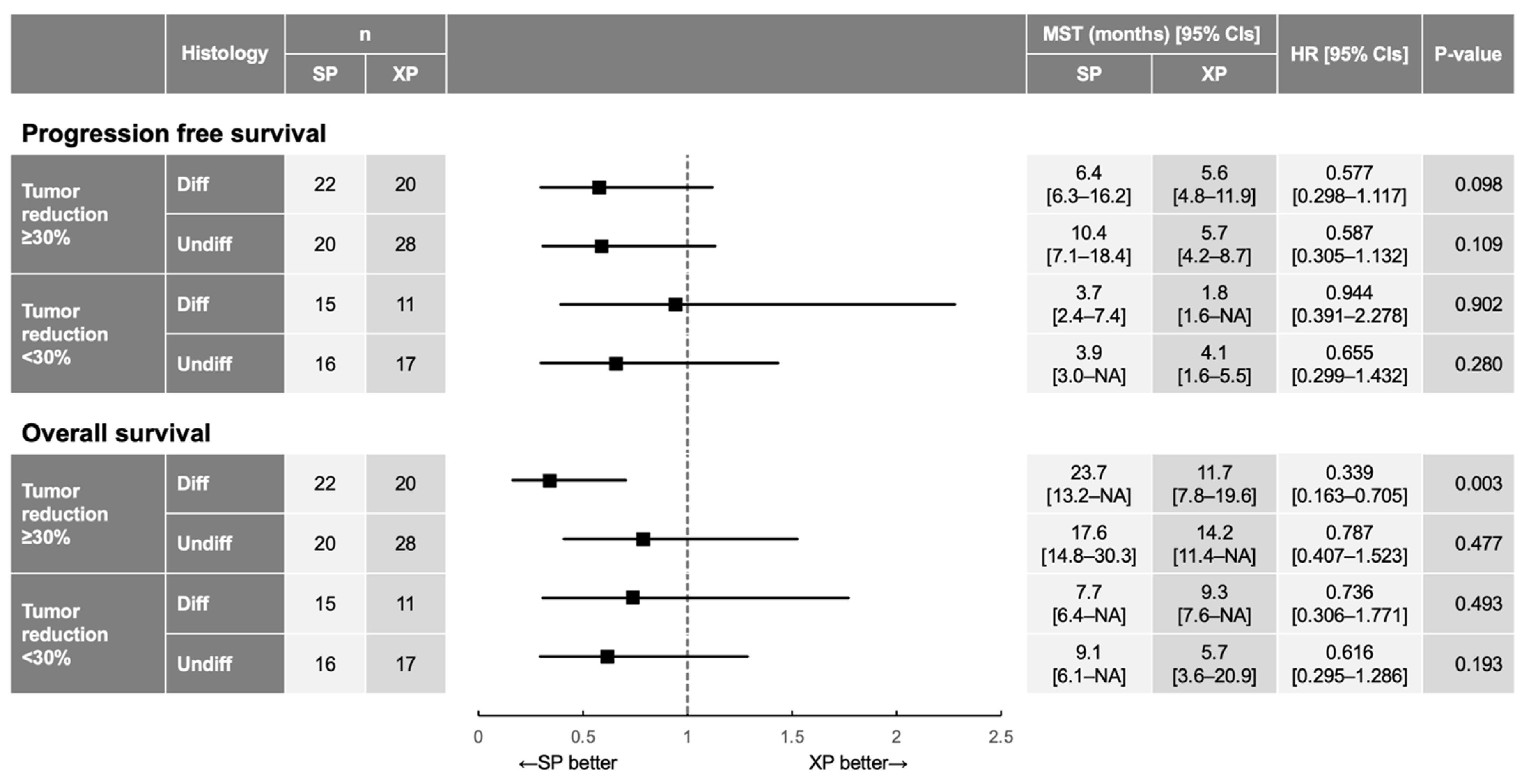
3.3. Differences in Treatment Effects between SP and XP According to Histology
3.4. Association of the Longer OS in the SP Arm with Deeper Tumor Shrinkage for Differentiated Tumors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Shirasaka, T.; Shimamato, Y.; Ohshimo, H.; Yamaguchi, M.; Kato, T.; Yonekura, K.; Fukushima, M. Development of a novel form of an oral 5-fluorouracil derivative (S-1) directed to the potentiation of the tumor selective cytotoxicity of 5-fluorouracil by two biochemical modulators. Anti-Cancer Drugs 1996, 7, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, W.; Narahara, H.; Hara, T.; Takagane, A.; Akiya, T.; Takagi, M.; Miyashita, K.; Nishizaki, T.; Kobayashi, O.; Takiyama, W.; et al. S-1 plus cisplatin versus S-1 alone for first-line treatment of advanced gastric cancer (SPIRITS trial): A phase III trial. Lancet Oncol. 2008, 9, 215–221. [Google Scholar] [CrossRef]
- Miwa, M.; Ura, M.; Nishida, M.; Sawada, N.; Ishikawa, T.; Mori, K.; Shimma, N.; Umeda, I.; Ishitsuka, H. Design of a novel oral fluoropyrimidine carbamate, capecitabine, which generates 5-fluorouracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur. J. Cancer 1998, 34, 1274–1281. [Google Scholar] [CrossRef]
- Bang, Y.-J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Ohtsu, A.; Shah, M.A.; Van Cutsem, E.; Rha, S.Y.; Sawaki, A.; Park, S.R.; Lim, H.Y.; Yamada, Y.; Wu, J.; Langer, B.; et al. Bevacizumab in Combination with Chemotherapy as First-Line Therapy in Advanced Gastric Cancer: A Randomized, Double-Blind, Placebo-Controlled Phase III Study. J. Clin. Oncol. 2011, 29, 3968–3976. [Google Scholar] [CrossRef]
- Lordick, F.; Kang, Y.-K.; Chung, H.-C.; Salman, P.; Oh, S.C.; Bodoky, G.; Kurteva, G.; Volovat, C.; Moiseyenko, V.M.; Gorbunova, V.; et al. Capecitabine and cisplatin with or without cetuximab for patients with previously untreated advanced gastric cancer (EXPAND): A randomised, open-label phase 3 trial. Lancet Oncol. 2013, 14, 490–499. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Shin, D.-B.; Chen, J.; Xiong, J.; Wang, J.; Lichinitser, M.; Guan, Z.; Khasanov, R.; Zheng, L.; Philco-Salas, M.; et al. Capecitabine/cisplatin versus 5-fluorouracil/cisplatin as first-line therapy in patients with advanced gastric cancer: A randomised phase III noninferiority trial. Ann. Oncol. 2009, 20, 666–673. [Google Scholar] [CrossRef]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer 2021, 24, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, H.; for the Osaka Gastrointestinal Cancer Chemotherapy Study Group (OGSG); Fujitani, K.; Matsuyama, J.; Akamaru, Y.; Tamura, S.; Endo, S.; Kimura, Y.; Makari, Y. Comparison of S-1–cisplatin every 5 weeks with capecitabine-cisplatin every 3 weeks for HER2-negative gastric cancer (recurrent after S-1 adjuvant therapy or chemotherapy-naïve advanced): Pooled analysis of HERBIS-2 (OGSG 1103) and HERBIS-4A (OGSG 1105) trials. Int. J. Clin. Oncol. 2020, 25, 1635–1643. [Google Scholar] [CrossRef]
- Kawakami, H.; Takeno, A.; Endo, S.; Makari, Y.; Kawada, J.; Taniguchi, H.; Tamura, S.; Sugimoto, N.; Kimura, Y.; Tamura, T.; et al. Randomized, Open-Label Phase II Study Comparing Capecitabine-Cisplatin Every 3 Weeks with S-1-Cisplatin Every 5 Weeks in Chemotherapy-Naïve Patients with HER2-Negative Advanced Gastric Cancer: OGSG1105, HERBIS-4A Trial. Oncologist 2018, 23, 1411–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishikawa, K.; Tsuburaya, A.; Yoshikawa, T.; Kobayashi, M.; Kawada, J.; Fukushima, R.; Matsui, T.; Tanabe, K.; Yamaguchi, K.; Yoshino, S.; et al. A randomised phase II trial of capecitabine plus cisplatin versus S-1 plus cisplatin as a first-line treatment for advanced gastric cancer: Capecitabine plus cisplatin ascertainment versus S-1 plus cisplatin randomised PII trial (XParTS II). Eur. J. Cancer 2018, 101, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, Z.; Qu, J.; Song, N.; Chen, Y.; Cheng, Y.; Zhang, S.; Qu, X.; Liu, Y. Clinical outcomes of capecitabine-based versus S-1-based regimens as first-line chemotherapy in patients with unresectable or metastatic gastric cancer: A propensity score matched single-center comparison. J. Gastrointest. Oncol. 2020, 11, 674–684. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Yan, P.; Hou, X.; Feng, J.; He, X.; Yang, K. The efficacy and safety of capecitabine-based versus S-1-based chemotherapy for metastatic or recurrent gastric cancer: A systematic review and meta-analysis of clinical randomized trials. Ann. Palliat. Med. 2020, 9, 883–894. [Google Scholar] [CrossRef] [PubMed]
- He, M.-M.; Wu, W.-J.; Wang, F.; Wang, Z.-Q.; Zhang, D.-S.; Luo, H.-Y.; Qiu, M.-Z.; Ren, C.; Zeng, Z.-L.; Xu, R.-H. S-1-Based Chemotherapy versus Capecitabine-Based Chemotherapy as First-Line Treatment for Advanced Gastric Carcinoma: A Meta-Analysis. PLoS ONE 2013, 8, e82798. [Google Scholar] [CrossRef] [Green Version]
- Ye, Z.; Chen, J.; Rao, Y.; Yang, W. Should S-1 be better than capecitabine for patients with advanced gastric cancer in Asia? A systematic review and meta-analysis. OncoTargets Ther. 2018, 12, 269–277. [Google Scholar] [CrossRef] [Green Version]
- Ter Veer, E.; Ngai, L.L.; Van Valkenhoef, G.; Mohammad, N.H.; Anderegg, M.C.J.; Van Oijen, M.G.H.; Van Laarhoven, H.W.M. Capecitabine, 5-fluorouracil and S-1 based regimens for previously untreated advanced oesophagogastric cancer: A network meta-analysis. Sci. Rep. 2017, 7, 7142. [Google Scholar] [CrossRef] [Green Version]
- He, A.-B.; Peng, X.-L.; Song, J.; Zhang, J.-X.; Dong, W.-G.; Luo, R.-F.; Tang, Y. Efficacy of S-1vscapecitabine for the treatment of gastric cancer: A meta-analysis. World J. Gastroenterol. 2015, 21, 4358–4364. [Google Scholar] [CrossRef]
- Kadowaki, S.; Masuishi, T.; Eto, T.; Narita, Y.; Taniguchi, H.; Ura, T.; Ando, M.; Tajika, M.; Niwa, Y.; Yatabe, Y.; et al. Depth of response predicts the clinical outcome of advanced HER2-positive gastric cancer to trastuzumab-based first-line chemotherapy. Cancer Chemother. Pharmacol. 2017, 80, 807–813. [Google Scholar] [CrossRef]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lonardi, S.; Masi, G.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Spadi, R.; Zaniboni, A.; et al. Early tumor shrinkage and depth of response predict long-term outcome in metastatic colorectal cancer patients treated with first-line chemotherapy plus bevacizumab: Results from phase III TRIBE trial by the Gruppo Oncologico del Nord Ovest. Ann. Oncol. 2015, 26, 1188–1194. [Google Scholar] [CrossRef]
- Heinemann, V.; Stintzing, S.; Modest, D.P.; Giessen-Jung, C.; Michl, M.; Mansmann, U.R. Early tumour shrinkage (ETS) and depth of response (DpR) in the treatment of patients with metastatic colorectal cancer (mCRC). Eur. J. Cancer 2015, 51, 1927–1936. [Google Scholar] [CrossRef] [PubMed]
- Stintzing, S.; Modest, D.P.; Rossius, L.; Lerch, M.M.; von Weikersthal, L.F.; Decker, T.; Kiani, A.; Vehling-Kaiser, U.; Al-Batran, S.-E.; Heintges, T.; et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab for metastatic colorectal cancer (FIRE-3): A post-hoc analysis of tumour dynamics in the final RAS wild-type subgroup of this randomised open-label phase 3 trial. Lancet Oncol. 2016, 17, 1426–1434. [Google Scholar] [CrossRef]
- Kim, G.M.; Jeung, H.-C.; Rha, S.Y.; Kim, H.S.; Jung, I.; Nam, B.H.; Lee, K.H.; Chung, H.C. A randomized phase II trial of S-1-oxaliplatin versus capecitabine–oxaliplatin in advanced gastric cancer. Eur. J. Cancer 2012, 48, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Janjigian, Y.Y.; Shitara, K.; Moehler, M.; Garrido, M.; Salman, P.; Shen, L.; Wyrwicz, L.; Yamaguchi, K.; Skoczylas, T.; Bragagnoli, A.C.; et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): A randomised, open-label, phase 3 trial. Lancet 2021, 3, 27–40. [Google Scholar] [CrossRef]
- Kang, Y.-K.; Chen, L.-T.; Ryu, M.-H.; Oh, D.-Y.; Oh, S.C.; Chung, H.C.; Lee, K.-W.; Omori, T.; Shitara, K.; Sakuramoto, S.; et al. Nivolumab plus chemotherapy versus placebo plus chemotherapy in patients with HER2-negative, untreated, unresectable advanced or recurrent gastric or gastro-oesophageal junction cancer (ATTRACTION-4): A randomised, multicentre, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2022, 23, 234–247. [Google Scholar] [CrossRef]
- Boku, N.; Ryu, M.-H.; Kato, K.; Chung, H.; Minashi, K.; Lee, K.-W.; Cho, H.; Kang, W.; Komatsu, Y.; Tsuda, M.; et al. Safety and efficacy of nivolumab in combination with S-1/capecitabine plus oxaliplatin in patients with previously untreated, unresectable, advanced, or recurrent gastric/gastroesophageal junction cancer: Interim results of a randomized, phase II trial (ATTRACTION-4). Ann. Oncol. 2019, 30, 250–258. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, S.; Haratani, K.; Hayashi, H.; Chiba, Y.; Tanizaki, J.; Kato, R.; Mitani, S.; Kawanaka, Y.; Kurosaki, T.; Hasegawa, Y.; et al. Association of tumour burden with the efficacy of programmed cell death-1/programmed cell death ligand-1 inhibitors for treatment-naïve advanced non-small-cell lung cancer. Eur. J. Cancer 2021, 161, 44–54. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SP | XP | |||||||
|---|---|---|---|---|---|---|---|---|
| All (n = 79) | HERBIS-2 (n = 5) | HERBIS-4A (n = 41) | XParTS II (n = 33) | All (n = 83) | HERBIS-2 (n = 4) | HERBIS-4A (n = 43) | XParTS II (n = 36) | |
| Age (years) | ||||||||
| Median [min, max] | 66 [37, 77] | 71 [64, 73] | 68 [37, 77] | 65 [44, 74] | 65 [31, 79] | 73 [72, 74] | 64 [34, 79] | 65 [31, 74] |
| Sex | ||||||||
| Male | 60 (75.9) | 5 (100.0) | 33 (80.5) | 22 (66.7) | 71 (85.5) | 4 (100.0) | 36 (83.7) | 31 (86.1) |
| Female | 19 (24.1) | 0 (0.0) | 8 (19.5) | 11 (33.3) | 12 (14.5) | 0 (0.0) | 7 (16.3) | 5 (13.9) |
| ECOG PS | ||||||||
| 0 | 54 (68.4) | 4 (80.0) | 22 (53.7) | 28 (84.8) | 59 (71.1) | 4 (100.0) | 24 (55.8) | 31 (86.1) |
| 1 | 24 (30.4) | 1 (20.0) | 19 (46.3) | 4 (12.1) | 23 (27.7) | 0 (0.0) | 19 (44.2) | 4 (11.1) |
| 2 | 1 (1.3) | 0 (0.0) | 0 (0.0) | 1 (3.0) | 1 (1.2) | 0 (0.0) | 0 (0.0) | 1 (2.8) |
| HER2 status | ||||||||
| Positive | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Negative | 76 (96.2) | 4 (80.0) | 41 (100.0) | 31 (93.9) | 79 (95.2) | 4 (100.0) | 42 (97.7) | 33 (91.7) |
| Unknown | 3 (3.8) | 1 (20.0) | 0 (0.0) | 2 (6.1) | 4 (4.8) | 0 (0.0) | 1 (2.3) | 3 (8.3) |
| Tumor localization | ||||||||
| U | 21 (26.6) | 2 (40.0) | 7 (17.1) | 12 (36.4) | 26 (31.3) | 2 (50.0) | 14 (32.6) | 10 (27.8) |
| M | 33 (41.8) | 2 (40.0) | 21 (51.2) | 10 (30.3) | 25 (30.1) | 0 (0.0) | 11 (25.6) | 14 (38.9) |
| L | 22 (27.8) | 1 (20.0) | 13 (31.7) | 8 (24.2) | 31 (37.3) | 2 (50.0) | 18 (41.9) | 11 (30.6) |
| E | 1 (1.3) | 0 (0.0) | 0 (0.0) | 1 (3.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| D | 2 (2.5) | 0 (0.0) | 0 (0.0) | 2 (6.1) | 1 (1.2) | 0 (0.0) | 0 (0.0) | 1 (2.8) |
| Histology | ||||||||
| pap | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 3 (3.6) | 0 (0.0) | 2 (4.7) | 1 (2.8) |
| tub1 | 10 (12.7) | 0 (0.0) | 8 (19.5) | 2 (6.1) | 6 (7.2) | 1 (25.0) | 4 (9.3) | 1 (2.8) |
| tub2 | 29 (36.7) | 2 (40.0) | 15 (36.6) | 12 (36.4) | 23 (27.7) | 1 (25.0) | 15 (34.9) | 7 (19.4) |
| por1 | 22 (27.8) | 0 (0.0) | 10 (24.4) | 12 (36.4) | 22 (26.5) | 0 (0.0) | 9 (20.9) | 13 (36.1) |
| por2 | 10 (12.7) | 2 (40.0) | 3 (7.3) | 5 (15.2) | 15 (18.1) | 0 (0.0) | 9 (20.9) | 6 (16.7) |
| sig | 4 (5.1) | 0 (0.0) | 3 (7.3) | 1 (3.0) | 7 (8.4) | 1 (25.0) | 0 (0.0) | 6 (16.7) |
| muc | 2 (2.5) | 1 (20.0) | 0 (0.0) | 1 (3.0) | 2 (2.4) | 1 (25.0) | 1 (2.3) | 0 (0.0) |
| Other | 2 (2.5) | 0 (0.0) | 2 (4.9) | 0 (0.0) | 5 (6.0) | 0 (0.0) | 3 (7.0) | 2 (5.6) |
| TNM classification | ||||||||
| M stage | ||||||||
| MX | 2 (2.5) | 0 (0.0) | 2 (4.9) | 0 (0.0) | 2 (2.4) | 0 (0.0) | 1 (2.3) | 1 (2.9) |
| M0 | 17 (21.5) | 5 (100.0) | 6 (14.6) | 6 (18.2) | 15 (18.3) | 4 (100.0) | 4 (9.3) | 7 (20.0) |
| M1 | 60 (75.9) | 0 (0.0) | 33 (80.5) | 27 (81.8) | 65 (79.3) | 0 (0.0) | 38 (88.4) | 27 (77.1) |
| Prior surgery | ||||||||
| No | 62 (78.5) | 0 (0.0) | 34 (82.9) | 28 (84.8) | 68 (81.9) | 0 (0.0) | 39 (90.7) | 29 (80.6) |
| Yes | 17 (21.5) | 5 (100.0) | 7 (17.1) | 5 (15.2) | 15 (18.1) | 4 (100.0) | 4 (9.3) | 7 (19.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawakami, H.; Nishikawa, K.; Shimokawa, T.; Fujitani, K.; Tamura, S.; Endo, S.; Kobayashi, M.; Kawada, J.; Kurokawa, Y.; Tsuburaya, A.; et al. Histology Classification Highlights Differences in Efficacy of S-1 versus Capecitabine, in Combination with Cisplatin, for HER2-Negative Unresectable Advanced or Recurrent Gastric Cancer with Measurable Disease. Cancers 2022, 14, 5673. https://doi.org/10.3390/cancers14225673
Kawakami H, Nishikawa K, Shimokawa T, Fujitani K, Tamura S, Endo S, Kobayashi M, Kawada J, Kurokawa Y, Tsuburaya A, et al. Histology Classification Highlights Differences in Efficacy of S-1 versus Capecitabine, in Combination with Cisplatin, for HER2-Negative Unresectable Advanced or Recurrent Gastric Cancer with Measurable Disease. Cancers. 2022; 14(22):5673. https://doi.org/10.3390/cancers14225673
Chicago/Turabian StyleKawakami, Hisato, Kazuhiro Nishikawa, Toshio Shimokawa, Kazumasa Fujitani, Shigeyuki Tamura, Shunji Endo, Michiya Kobayashi, Junji Kawada, Yukinori Kurokawa, Akira Tsuburaya, and et al. 2022. "Histology Classification Highlights Differences in Efficacy of S-1 versus Capecitabine, in Combination with Cisplatin, for HER2-Negative Unresectable Advanced or Recurrent Gastric Cancer with Measurable Disease" Cancers 14, no. 22: 5673. https://doi.org/10.3390/cancers14225673