
Serum Extracellular Vesicle-Derived microRNAs as Potential Biomarkers for Pleural Mesothelioma in a European Prospective Study
 , , , , , , , , , , , , add
Show full author list
, , , , , , , , , , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Isolation of Serum Extracellular Vesicles and RNA Extraction
2.3. Library Preparation and Next Generation Sequencing
2.4. Nanoparticle Tracking Analysis and Electron Microscopy
2.5. miRNAs Sequencing Data Analysis
2.6. Technical Validation by RT-qPCR Analysis
2.7. Functional Enrichment Analysis of miRNAs Target Genes
2.8. Investigation of Selected miRNAs in a Retrospective Cohort
3. Results
3.1. Validation of miRNA-seq Data by RT-qPCR
3.2. miRNAs Target Genes and KEGG Enrichment Analysis
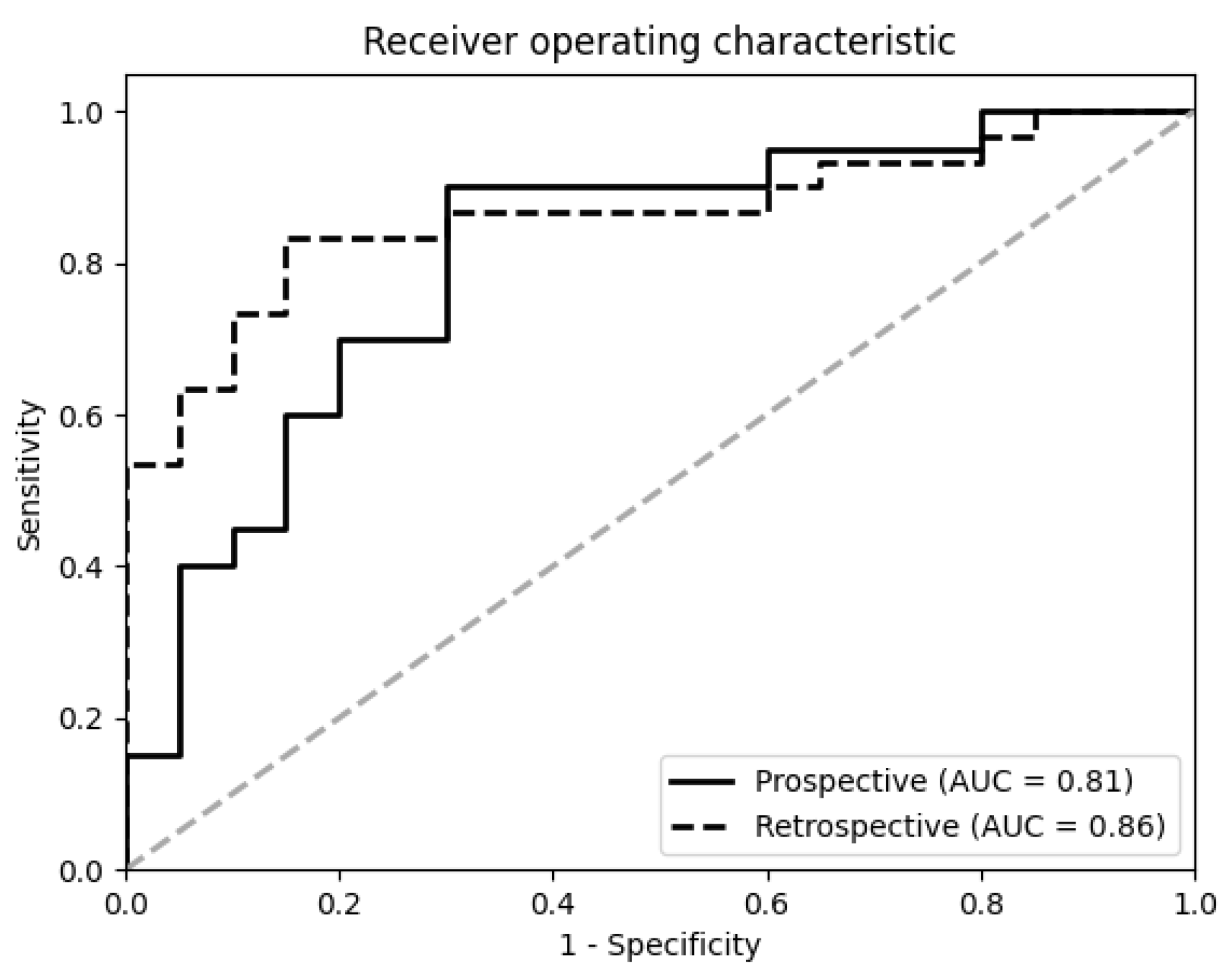
3.3. Prediction Model and Validation in a Retrospective Study
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hung, Y.P.; Chirieac, L.R. Pathology of Malignant Pleural Mesothelioma. Thorac. Surg. Clin. 2020, 30, 367–382. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Ruan, J.; Zheng, Y.; Xiang, D.; Li, N.; Hu, J.; Shen, J.; Deng, Y.; Yao, J.; Zhao, P.; et al. Assessment of Global Trends in the Diagnosis of Mesothelioma From 1990 to 2017. JAMA Netw. Open 2021, 4, e2120360. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, M.R.; Neal, J.W. Novel systemic therapy against malignant pleural mesothelioma. Transl. Lung. Cancer Res. 2017, 6, 295–314. [Google Scholar] [CrossRef] [Green Version]
- Nicole, L.; Cappellesso, R.; Sanavia, T.; Guzzardo, V.; Fassina, A. MiR-21 over-expression and Programmed Cell Death 4 down-regulation features malignant pleural mesothelioma. Oncotarget 2018, 9, 17300–17308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wald, O.; Sugarbaker, D.J. New Concepts in the Treatment of Malignant Pleural Mesothelioma. Annu. Rev. Med. 2018, 69, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.K.; Chansky, K.; Rice, D.C.; Pass, H.I.; . Kindler, H.L.; Shemanski, L.; Bille, A.; Rintoul, R.C.; Batirel, H.F.; Thomas, C.F.; et al. The IASLC Mesothelioma Staging Project: Proposals for Revisions of the T Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Pleural Mesothelioma. J. Thorac. Oncol. 2016, 11, 2089–2099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mielgo-Rubio, X.; Cardena Gutierrez, A.; Sotelo Pena, V.; Sanchez Becerra, M.V.; Gonzalez Lopez, A.M.; Rosero, A.; Trujillo-Reyes, J.C.; Counago, F. Tsunami of immunotherapy reaches mesothelioma. World J. Clin. Oncol. 2022, 13, 267–275. [Google Scholar] [CrossRef]
- Li, J.; Guan, X.; Fan, Z.; Ching, L.M.; Li, Y.; Wang, X.; Cao, W.M.; Liu, D.X. Non-Invasive Biomarkers for Early Detection of Breast Cancer. Cancers 2020, 12, 2767. [Google Scholar] [CrossRef]
- van Zandwijk, N.; Clarke, C.; Henderson, D.; Musk, A.W.; Fong, K.; Nowak, A.; Loneragan, R.; McCaughan, B.; Boyer, M.; Feigen, M.; et al. Guidelines for the diagnosis and treatment of malignant pleural mesothelioma. J. Thorac. Dis. 2013, 5, E254–E307. [Google Scholar]
- Xu, R.; Rai, A.; Chen, M.; Suwakulsiri, W.; Greening, D.W.; Simpson, R.J. Extracellular vesicles in cancer—implications for future improvements in cancer care. Nat. Rev. Clin. Oncol. 2018, 15, 617–638. [Google Scholar] [CrossRef]
- Doyle, L.M.; Wang, M.Z. Overview of Extracellular Vesicles, Their Origin, Composition, Purpose, and Methods for Exosome Isolation and Analysis. Cells 2019, 8, 727. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Wang, H.; Yao, X.; Zhang, D.; Xie, Y.; Cui, R.; Zhang, X. Circulating MicroRNAs in Cancer: Potential and Challenge. Front. Genet. 2019, 10, 626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrari, L.; Carugno, M.; Mensi, C.; Pesatori, A.C. Circulating Epigenetic Biomarkers in Malignant Pleural Mesothelioma: State of the Art and critical Evaluation. Front. Oncol. 2020, 10, 445. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Rivera, V.; Negrete-Garcia, M.C.; Avila-Moreno, F.; Ortiz-Quintero, B. Secreted and Tissue miRNAs as Diagnosis Biomarkers of Malignant Pleural Mesothelioma. Int. J. Mol. Sci 2018, 19, 595. [Google Scholar] [CrossRef] [Green Version]
- Kirschner, M.B.; Cheng, Y.Y.; Badrian, B.; Kao, S.C.; Creaney, J.; Edelman, J.J.; Armstrong, N.J.; Vallely, M.P.; Musk, A.W.; Robinson, B.W.; et al. Increased circulating miR-625-3p: A potential biomarker for patients with malignant pleural mesothelioma. J. Thorac. Oncol. 2012, 7, 1184–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muraoka, T.; Soh, J.; Toyooka, S.; Aoe, K.; Fujimoto, N.; Hashida, S.; Maki, Y.; Tanaka, N.; Shien, K.; Furukawa, M.; et al. The degree of microRNA-34b/c methylation in serum-circulating DNA is associated with malignant pleural mesothelioma. Lung Cancer 2013, 82, 485–490. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, C.A.; Riboli, E. Diet and cancer prevention: Contributions from the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Eur. J. Cancer 2010, 46, 2555–2562. [Google Scholar] [CrossRef]
- Ferrero, G.; Cordero, F.; Tarallo, S.; Arigoni, M.; Riccardo, F.; Gallo, G.; Ronco, G.; Allasia, M.; Kulkarni, N.; Matullo, G.; et al. Small non-coding RNA profiling in human biofluids and surrogate tissues from healthy individuals: Description of the diverse and most represented species. Oncotarget 2018, 9, 3097–3111. [Google Scholar] [CrossRef] [Green Version]
- Verta, R.; Grange, C.; Skovronova, R.; Tanzi, A.; Peruzzi, L.; Deregibus, M.C.; Camussi, G.; Bussolati, B. Generation of Spike-Extracellular Vesicles (S-EVs) as a Tool to Mimic SARS-CoV-2 Interaction with Host Cells. Cells 2022, 11, 146. [Google Scholar] [CrossRef]
- Rani, A.; Barter, J.; Kumar, A.; Stortz, J.A.; Hollen, M.; Nacionales, D.; Moldawer, L.L.; Efron, P.A.; Foster, T.C. Influence of age and sex on microRNA response and recovery in the hippocampus following sepsis. Aging 2022, 14, 728–746. [Google Scholar] [CrossRef]
- Francavilla, A.; Gagliardi, A.; Piaggeschi, G.; Tarallo, S.; Cordero, F.; Pensa, R.G.; Impeduglia, A.; Caviglia, G.P.; Ribaldone, D.G.; Gallo, G.; et al. Faecal miRNA profiles associated with age, sex, BMI, and lifestyle habits in healthy individuals. Sci. Rep. 2021, 11, 20645. [Google Scholar] [CrossRef] [PubMed]
- Ru, Y.; Kechris, K.J.; Tabakoff, B.; Hoffman, P.; Radcliffe, R.A.; Bowler, R.; Mahaffey, S.; Rossi, S.; Calin, G.A.; Bemis, L.; et al. The multiMiR R package and database: Integration of microRNA-target interactions along with their disease and drug associations. Nucleic Acids Res. 2014, 42, e133. [Google Scholar] [CrossRef] [PubMed]
- Sticht, C.; De La Torre, C.; Parveen, A.; Gretz, N. miRWalk: An online resource for prediction of microRNA binding sites. PLoS ONE 2018, 13, e0206239. [Google Scholar] [CrossRef] [PubMed]
- Ge, S.X.; Jung, D.; Yao, R. ShinyGO: A graphical gene-set enrichment tool for animals and plants. Bioinformatics 2020, 36, 2628–2629. [Google Scholar] [CrossRef]
- Sculco, M.; La Vecchia, M.; Aspesi, A.; Pinton, G.; Clavenna, M.G.; Casalone, E.; Allione, A.; Grosso, F.; Libener, R.; Muzio, A.; et al. Malignant pleural mesothelioma: Germline variants in DNA repair genes may steer tailored treatment. Eur. J. Cancer 2022, 163, 44–54. [Google Scholar] [CrossRef]
- Filiberti, R.; Marroni, P.; Spigno, F.; Merlo, D.F.; Mortara, V.; Caruso, P.; Cioe, A.; Michelazzi, L.; Bruzzone, A.; Bobbio, B.; et al. Is soluble mesothelin-related protein an upfront predictive marker of pleural mesothelioma? A prospective study on Italian workers exposed to asbestos. Oncology 2014, 86, 33–43. [Google Scholar] [CrossRef]
- Xu, Y.; Zheng, M.; Merritt, R.E.; Shrager, J.B.; Wakelee, H.A.; Kratzke, R.A.; Hoang, C.D. miR-1 induces growth arrest and apoptosis in malignant mesothelioma. Chest 2013, 144, 1632–1643. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Wu, L.; Wang, A.; Tang, W.; Zhao, Y.; Zhao, H.; Teschendorff, A.E. dbDEMC 2.0: Updated database of differentially expressed miRNAs in human cancers. Nucleic Acids Res. 2017, 45, D812–D818. [Google Scholar] [CrossRef]
- Sekido, Y. Targeting the Hippo Pathway Is a New Potential Therapeutic Modality for Malignant Mesothelioma. Cancers 2018, 10, 90. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Pan, D. The Hippo Signaling Pathway in Development and Disease. Dev. Cell 2019, 50, 264–282. [Google Scholar] [CrossRef]
- Cavalleri, T.; Angelici, L.; Favero, C.; Dioni, L.; Mensi, C.; Bareggi, C.; Palleschi, A.; Rimessi, A.; Consonni, D.; Bordini, L.; et al. Plasmatic extracellular vesicle microRNAs in malignant pleural mesothelioma and asbestos-exposed subjects suggest a 2-miRNA signature as potential biomarker of disease. PLoS ONE 2017, 12, e0176680. [Google Scholar] [CrossRef] [PubMed]
- Goricar, K.; Holcar, M.; Mavec, N.; Kovac, V.; Lenassi, M.; Dolzan, V. Extracellular Vesicle Enriched miR-625-3p Is Associated with Survival of Malignant Mesothelioma Patients. J. Pers. Med. 2021, 11, 1014. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.G.; Gawrych, K.; Casjens, S.; Brik, A.; Lehnert, M.; Taeger, D.; Pesch, B.; Kollmeier, J.; Bauer, T.T.; Johnen, G.; et al. Circulating miR-132-3p as a Candidate Diagnostic Biomarker for Malignant Mesothelioma. Dis. Markers 2017, 2017, 9280170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Zhou, Q.; Han, Y.Q.; Li, P.; Ouyang, P.H.; Wang, M.Y.; Hu, Z.D. Diagnostic accuracy of circulating miR-126 for malignant pleural mesothelioma: A systematic review and meta-analysis. Transl. Cancer Res. 2021, 10, 1856–1862. [Google Scholar] [CrossRef]
- Weber, D.G.; Brik, A.; Casjens, S.; Burek, K.; Lehnert, M.; Pesch, B.; Taeger, D.; Bruning, T.; Johnen, G. Are circulating microRNAs suitable for the early detection of malignant mesothelioma? Results from a nested case-control study. BMC Res. Notes 2019, 12, 77. [Google Scholar] [CrossRef]
- Ng, K.T.; Lo, C.M.; Wong, N.; Li, C.X.; Qi, X.; Liu, X.B.; Geng, W.; Yeung, O.W.; Ma, Y.Y.; Chan, S.C.; et al. Early-phase circulating miRNAs predict tumor recurrence and survival of hepatocellular carcinoma patients after liver transplantation. Oncotarget 2016, 7, 19824–19839. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Yu, J.; Ma, Y.; Wang, F.; Liu, H. miR-148a and miR-375 may serve as predictive biomarkers for early diagnosis of laryngeal carcinoma. Oncol. Lett. 2016, 12, 871–878. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Zou, W.; Wang, Y.; Liao, Z.; Li, L.; Zhai, Y.; Zhang, L.; Gu, S.; Zhao, X. Plasma-based microRNA signatures in early diagnosis of breast cancer. Mol. Genet. Genomic Med. 2020, 8, e1092. [Google Scholar] [CrossRef] [Green Version]
- Josson, S.; Gururajan, M.; Sung, S.Y.; Hu, P.; Shao, C.; Zhau, H.E.; Liu, C.; Lichterman, J.; Duan, P.; Li, Q.; et al. Stromal fibroblast-derived miR-409 promotes epithelial-to-mesenchymal transition and prostate tumorigenesis. Oncogene 2015, 34, 2690–2699. [Google Scholar] [CrossRef]
- Sun, Q.; Jia, X.; Gao, J.; Zhang, P.; Mou, W.; Yang, C.; Tong, H.; Wen, X.; Tian, Y. Identification and characterization of novel serum microRNAs in unstable angina pectoris and subclinical atherosclerotic patients. Exp. Cell Res. 2015, 333, 220–227. [Google Scholar] [CrossRef]
- Zolondick, A.A.; Gaudino, G.; Xue, J.; Pass, H.I.; Carbone, M.; Yang, H. Asbestos-induced chronic inflammation in malignant pleural mesothelioma and related therapeutic approaches-a narrative review. Precis Cancer Med. 2021, 4, 27. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.X.; Zhang, Y.; Park, H.W.; Jewell, J.L.; Chen, Q.; Deng, Y.; Pan, D.; Taylor, S.S.; Lai, Z.C.; Guan, K.L. Protein kinase A activates the Hippo pathway to modulate cell proliferation and differentiation. Genes Dev. 2013, 27, 1223–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, F.; Bazille, C.; Levallet, J.; Maille, E.; Brosseau, S.; Madelaine, J.; Bergot, E.; Zalcman, G.; Levallet, G. Molecular Alterations in Malignant Pleural Mesothelioma: A Hope for Effective Treatment by Targeting YAP. Target. Oncol. 2022, 17, 407–431. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Xu, D.; Schmid, R.A.; Peng, R.W. Biomarker-guided targeted and immunotherapies in malignant pleural mesothelioma. Ther. Adv. Med. Oncol. 2020, 12, 1758835920971421. [Google Scholar] [CrossRef]
- Suzuki, R.; Amatya, V.J.; Kushitani, K.; Kai, Y.; Kambara, T.; Takeshima, Y. miR-182 and miR-183 Promote Cell Proliferation and Invasion by Targeting FOXO1 in Mesothelioma. Front. Oncol. 2018, 8, 446. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Jia, X.; Yang, F.; Shi, P. miR-148a-3p suppresses the progression of acute myeloid leukemia via targeting cyclin-dependent kinase 6 (CDK6). Bioengineered 2021, 12, 4508–4519. [Google Scholar] [CrossRef]
- Mills, J.; Capece, M.; Cocucci, E.; Tessari, A.; Palmieri, D. Cancer-Derived Extracellular Vesicle-Associated MicroRNAs in Intercellular Communication: One Cell’s Trash Is Another Cell’s Treasure. Int. J. Mol. Sci. 2019, 20, 6109. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.A.; Weng, S.L.; Yang, S.F.; Chou, C.H.; Huang, W.C.; Tu, S.J.; Chang, T.H.; Huang, C.N.; Jong, Y.J.; Huang, H.D. A Three-MicroRNA Signature as a Potential Biomarker for the Early Detection of Oral Cancer. Int. J. Mol. Sci. 2018, 19, 758. [Google Scholar] [CrossRef] [Green Version]
- Yee, N.S.; Zhang, S.; He, H.Z.; Zheng, S.Y. Extracellular Vesicles as Potential Biomarkers for Early Detection and Diagnosis of Pancreatic Cancer. Biomedicines 2020, 8, 581. [Google Scholar] [CrossRef]
- Johnen, G.; Burek, K.; Raiko, I.; Wichert, K.; Pesch, B.; Weber, D.G.; Lehnert, M.; Casjens, S.; Hagemeyer, O.; Taeger, D.; et al. Prediagnostic detection of mesothelioma by circulating calretinin and mesothelin—A case-control comparison nested into a prospective cohort of asbestos-exposed workers. Sci. Rep. 2018, 8, 14321. [Google Scholar] [CrossRef] [Green Version]
- Pass, H.I.; Alimi, M.; Carbone, M.; Yang, H.; Goparaju, C.M. Mesothelioma Biomarkers: A Review Highlighting Contributions from the Early Detection Research Network. Cancer Epidemiol. Biomarkers Prev. 2020, 29, 2524–2540. [Google Scholar] [CrossRef] [PubMed]
- Casjens, S.; Johnen, G.; Raiko, I.; Pesch, B.; Taeger, D.; Topfer, C.; Schonefeld, S.; Moebus, S.; Jockel, K.H.; Bruning, T.; et al. Re-evaluation of potential predictors of calretinin and mesothelin in a population-based cohort study using assays for the routine application in clinical medicine. BMJ Open 2021, 11, e039079. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALL EPIC-MESO (n = 164) | EPIC-MESO 5 Years (n = 48) | |||
|---|---|---|---|---|
| CA = 82 | CO = 82 | CA = 24 | CO = 24 | |
| GENDER | ||||
| M (%) | 59 (72) | 59 (72) | 20 (83.3) | 20(83.3) |
| F (%) | 23 (28) | 23 (28) | 4 (16.7) | 4(16.7) |
| AGE (mean ± sd) | 57.7 ± 8.1 | 57.8±8.1 | 60.4 ± 7.6 | 60.4 ± 7.6 |
| ASBESTOS EXPOSURE | ||||
| unexposed (%) | 18 (22) | 18 (22) | 3 (12.5) | 3 (12.5) |
| exposed (%) | 40 (48.7) | 40 (48.7) | 17 (70.8) | 17 (70.8) |
| NA | 24 (29.3) | 24 (29.3) | 4(16.7) | 4(16.7) |
| COUNTRY | ||||
| Germany (%) | 12 (14.6) | 12 (14.6) | 9 (37.5) | 9 (37.5) |
| Spain (%) | 10 (12.2) | 10 (12.2) | 1 (4.2) | 1 (4.2) |
| France (%) | 1 (1.2) | 1 (1.2) | 1 (4.2) | 1 (4.2) |
| Italy (%) | 21 (25.6) | 21 (25.6) | 4 (16.6) | 4 (16.6) |
| The Netherlands (%) | 8 (9.8) | 8 (9.8) | 1 (4.2) | 1 (4.2) |
| United Kingdom (%) | 30 (36.6) | 30 (36.6) | 8 (33.3) | 8 (33.3) |
| Prospective | Retrospective | |
|---|---|---|
| AUC | 81% | 86% |
| Sensitivity | 75% | 53% |
| Specificity | 70% | 95% |
| PPV | 71% | 94% |
| NPV | 74 % | 57% |
| Accuracy | 73% | 70% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casalone, E.; Birolo, G.; Pardini, B.; Allione, A.; Russo, A.; Catalano, C.; Mencoboni, M.; Ferrante, D.; Magnani, C.; Sculco, M.; et al. Serum Extracellular Vesicle-Derived microRNAs as Potential Biomarkers for Pleural Mesothelioma in a European Prospective Study. Cancers 2023, 15, 125. https://doi.org/10.3390/cancers15010125
Casalone E, Birolo G, Pardini B, Allione A, Russo A, Catalano C, Mencoboni M, Ferrante D, Magnani C, Sculco M, et al. Serum Extracellular Vesicle-Derived microRNAs as Potential Biomarkers for Pleural Mesothelioma in a European Prospective Study. Cancers. 2023; 15(1):125. https://doi.org/10.3390/cancers15010125
Chicago/Turabian StyleCasalone, Elisabetta, Giovanni Birolo, Barbara Pardini, Alessandra Allione, Alessia Russo, Chiara Catalano, Manlio Mencoboni, Daniela Ferrante, Corrado Magnani, Marika Sculco, and et al. 2023. "Serum Extracellular Vesicle-Derived microRNAs as Potential Biomarkers for Pleural Mesothelioma in a European Prospective Study" Cancers 15, no. 1: 125. https://doi.org/10.3390/cancers15010125