
Analysis of Selected Nutritional Parameters in Patients with HPV-Related and Non-HPV-Related Oropharyngeal Cancer before and after Radiotherapy Alone or Combined with Chemotherapy

 ,
,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Funding Statement and Ethics Approval and Consent to Participate
2.3. Study Design
2.4. Confirmation of the HPV Etiology
2.4.1. Tissue Material
2.4.2. Analysis of cfHPV16 DNA in Plasma
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Correlation between Local Tumor Stage and Treatment Regimen in HPV- and HPV+ Patients
3.3. Comparison of Nutritional Parameters before and after Treatment in HPV- and HPV+ Patients
3.4. Comparison of Nutritional Parameters before and after Treatment in HPV- and HPV+ Patients Undergoing RT and CRT Separately
3.5. Comparison of Selected Clinicopathological Factors between Groups with Low and High Prognostic Nutritional Index (PNI)
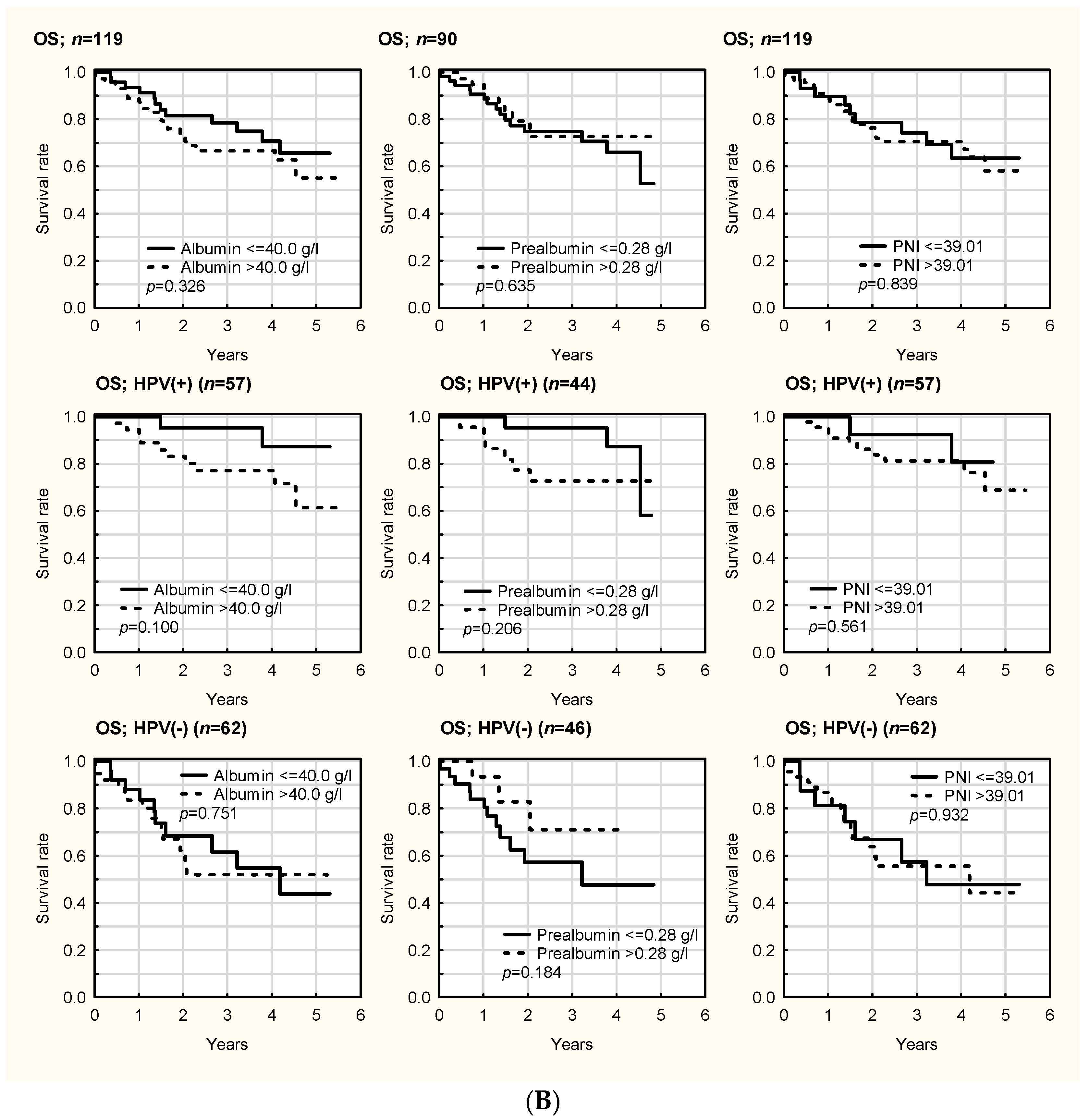
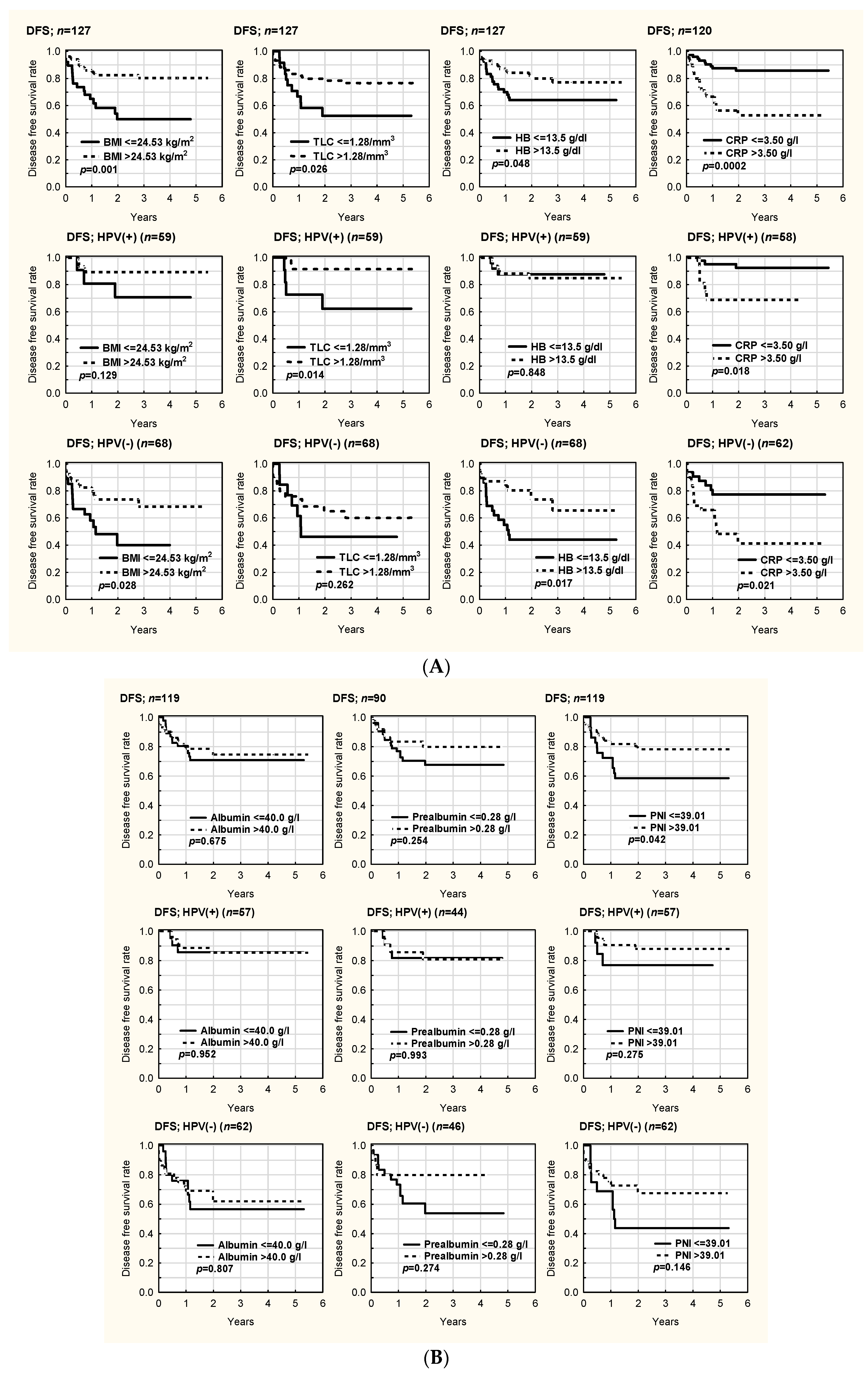
3.6. OS and DFS in HPV- and HPV+ Patients
3.6.1. Kaplan–Meier Analysis
3.6.2. Prognostic Factors for Survival in Cox Regression Analysis in HPV- and HPV+ Patients
Prognostic Factors for OS
Prognostic Factors for DFS
3.6.3. Prognostic Factors for Survival in Cox Regression Analysis in the Whole Cohort (without Division into Groups According to HPV Status)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- You, E.L.; Henry, M.; Zeitouni, A.G. Human papillomavirus-associated oropharyngeal cancer: Review of current evidence and management. Curr. Oncol. 2019, 26, 119–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsbeih, G.; Al-Harbi, N.; Bin Judia, S.; Al-Qahtani, W.; Khoja, H.; El-Sebaie, M.; Tulbah, A. Prevalence of Human Papillomavirus (HPV) Infection and the Association with Survival in Saudi Patients with Head and Neck Squamous Cell Carcinoma. Cancers 2019, 11, 820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Felice, F.; Tombolini, V.; Valentini, V.; de Vincentiis, M.; Mezi, S.; Brugnoletti, O.; Polimeni, A. Advances in the Management of HPV-Related Oropharyngeal Cancer. J. Oncol. 2019, 2019, 9173729. [Google Scholar] [CrossRef] [PubMed]
- Malm, I.J.; Fan, C.J.; Yin, L.X.; Li, D.X.; Koch, W.M.; Gourin, C.G.; Pitman, K.T.; Richmon, J.D.; Westra, W.H.; Kang, H.; et al. Evaluation of proposed staging systems for human papillomavirus-related oropharyngeal squamous cell carcinoma. Cancer 2017, 123, 1768–1777. [Google Scholar] [CrossRef] [Green Version]
- Masterson, L.; Moualed, D.; Liu, Z.W.; Howard, J.E.; Dwivedi, R.C.; Tysome, J.R.; Benson, R.; Sterling, J.C.; Sudhoff, H.; Jani, P.; et al. De-escalation treatment protocols for human papillomavirus-associated oropharyngeal squamous cell carcinoma: A systematic review and meta-analysis of current clinical trials. Eur. J. Cancer 2014, 50, 2636–2648. [Google Scholar] [CrossRef]
- Yamashita, Y.; Ikegami, T.; Hirakawa, H.; Uehara, T.; Deng, Z.; Agena, S.; Uezato, J.; Kondo, S.; Kiyuna, A.; Maeda, H.; et al. Staging and prognosis of oropharyngeal carcinoma according to the 8th Edition of the American Joint Committee on Cancer Staging Manual in human papillomavirus infection. Eur. Arch. Otorhinolaryngol. 2019, 276, 827–836. [Google Scholar] [CrossRef] [Green Version]
- Mallen-St Clair, J.; Ho, A.S. American Joint Committee on Cancer 8th edition staging-an improvement in prognostication in HPV-associated oropharyngeal cancer? Ann. Transl. Med. 2019, 7 (Suppl. 1), S10. [Google Scholar]
- Hong, J.S.; Hua YJSu, L.; Zhang, H.R.; Lv, W.L.; Chen, X.Y.; Tian, J.; Zhang, W.J. Modified-Nutrition Index is a Significant Prognostic Factor for the Overall Survival of the Nasopharyngeal Carcinoma Patients who Undergo Intensity-modulated Radiotherapy. Nutr. Cancer 2017, 69, 1011–1018. [Google Scholar] [CrossRef]
- Hong, J.S.; Wu, L.H.; Su, L.; Zhang, H.R.; Lv, W.L.; Zhang, W.J.; Tian, J. Effect of chemoradiotherapy on nutrition status of patients with nasopharyngeal cancer. Nutr. Cancer 2016, 68, 63–69. [Google Scholar] [CrossRef]
- Citak, E.; Tulek, Z.; Uzel, O. Nutritional status in patients with head and neck cancer undergoing radiotherapy: A longitudinal study. Support Care Cancer 2019, 27, 239–247. [Google Scholar] [CrossRef]
- Orell, H.; Schwab, U.; Saarilahti, K.; Österlund, P.; Ravasco, P.; Mäkitie, A. Nutritional Counseling for Head and Neck Cancer Patients Undergoing (Chemo) Radiotherapy-A Prospective Randomized Trial. Front. Nutr. 2019, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO consultation on obesity; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar] [PubMed]
- Li, H.; Park, H.S.; Osborn, H.A.; Judson, B.L. Sex differences in patients with high risk HPV associated and HPV negative oropharyngeal andoral cavity squamous cell carcinomas. Cancers Head Neck. 2018, 3, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goon, P.K.; Stanley, M.A.; Ebmeyer, J.; Steinsträsser, L.; Upile, T.; Jerjes, W.; Bernal-Sprekelsen, M.; Görner, M.; Sudhoff, H.H. HPV & head and neck cancer: A descriptive update. Head Neck Oncol. 2009, 1, 36. [Google Scholar] [PubMed] [Green Version]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Grønhøj, C.; Kronberg Jakobsen, K.; Kjær, E.; Friborg, J.; von Buchwald, C. Comorbidity in HPV+ and HPV− oropharyngeal cancer patients: A population-based, case-control study. Oral Oncol. 2019, 96, 1–6. [Google Scholar] [CrossRef]
- Liu, C.; Talmor, G.; Low, G.M.; Wang, T.V.; Mann, D.S.; Sinha, U.K.; Kokot, N.C. How Does Smoking Change the Clinicopathological Characteristics of Human Papillomavirus-Positive Oropharyngeal Squamous Cell Carcinoma? One Medical Center Experience. Clin. Med. Insights Ear Nose Throat 2018, 11, 1179550618792248. [Google Scholar] [CrossRef] [Green Version]
- Brown, T.E.; Wittholz, K.; Way, M.; Banks, M.D.; Hughes, B.G.; Lin, C.Y.; Kenny, L.M.; Bauer, J.D. Investigation of p16 status, chemotherapy regimen, and other nutrition markers for predicting gastrostomy in patients with head and neck cancer. Head Neck 2017, 39, 868–875. [Google Scholar] [CrossRef]
- Becker–Schiebe, M.; Sperling, M.; Pinkert, U.; Hoffmann, W. Impact of p16 alterations and pretreatment anemia on toxicity in head and neck cancer patients undergoing definitive radiochemotherapy. Oncol. Res. Treat 2015, 38, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Tehrany, N.; Kitz, J.; Rave–Frank, M.; Lorenzen, S.; Li, L.; Küffer, S.; Hess, C.F.; Burfeind, P.; Reichardt, H.M.; Canis, M.; et al. High grade acute organ toxicity and p16 (INK4A) expression as positive prognostic factors in primary radio(chemo)therapy for patients with head and neck squamous cell carcinoma. Strahlenther. Onkol. 2015, 191, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.B.; Isenring, E.; Brown, B. Nutrition and swallowing therapy strategies for patients with head and neck cancer. Nutrition 2020, 69, 110548. [Google Scholar] [CrossRef]
- Ding, H.; Dou, S.; Ling, Y.; Zhu, G.; Wang, Q.; Wu, Y.; Qian, Y. Longitudinal Body Composition Changes and the Importance of Fat-Free Mass Index in Locally Advanced Nasopharyngeal Carcinoma Patients Undergoing Concurrent Chemoradiotherapy. Integr. Cancer Ther. 2018, 17, 1125–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vangelov, B.; Venchiarutti, R.L.; Smee, R.I. Critical Weight Loss in Patients With Oropharynx Cancer During Radiotherapy (±Chemotherapy). Nutr. Cancer 2017, 69, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Przekop, Z.; Milewska, M.; Szostak-Węgierek, D.; Panczyk, M.; Sobocki, J. GLIM-Defined Malnutrition in Patients with Head and Neck Cancer during the Qualification Visit for Home Enteral Nutrition. Nutrients 2022, 14, 502. [Google Scholar] [CrossRef]
- Vangelov, B.; Kotevski, D.P.; Williams, J.R.; Smee, R.I. The impact of HPV status on weight loss and feeding tube use in oropharyngeal carcinoma. Oral Oncol. 2018, 79, 33–39. [Google Scholar] [CrossRef]
- Ottosson, S.; Söderström, K.; Kjellén, E.; Nilsson, P.; Zackrisson, B.; Laurell, G. Weight and body mass index in relation to irradiated volume and to overall survival in patients with oropharyngeal cancer: A retrospective cohort study. Radiat Oncol. 2014, 9, 160. [Google Scholar] [CrossRef] [Green Version]
- Moon, H.; Roh, J.L.; Lee, S.W.; Kim, S.B.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Prognostic value of nutritional and hematologic markers in head and neck squamous cell carcinoma treated by chemoradiotherapy. Radiother Oncol. 2016, 118, 330–334. [Google Scholar] [CrossRef]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and necksquamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Licitra, L.; Perrone, F.; Bossi, P.; Suardi, S.; Mariani, L.; Artusi, R.; Oggionni, M.; Rossini, C.; Cantù, G.; Squadrelli, M.; et al. High-risk human papillomavirus affects prognosis in patients with surgically treated oropharyngeal squamous cell carcinoma. J. Clin. Oncol. 2006, 24, 5630–5636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindquist, D.; Romanitan, M.; Hammarstedt, L.; Näsman, A.; Dahlstrand, H.; Lindholm, J.; Onelöv, L.; Ramqvist, T.; Ye, W.; Munck-Wikland, E.; et al. Human papillomavirus is a favourable prognostic factor in tonsillar cancer and its oncogenic role is supported by the expression of E6 and E7. Mol. Oncol. 2007, 1, 350–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lassen, P.; Eriksen, J.G.; Hamilton-Dutoit, S.; Tramm, T.; Alsner, J.; Overgaard, J. Effect of HPV-associated p16INK4A expression on response to radiotherapy and survival in squamous cell carcinoma of the head and neck. J. Clin. Oncol. 2009, 27, 1992–1998. [Google Scholar] [CrossRef] [Green Version]
- Settle, K.; Posner, M.R.; Schumaker, L.M.; Tan, M.; Suntharalingam, M.; Goloubeva, O.; Strome, S.E.; Haddad, R.I.; Patel, S.S.; Cambell, E.V., 3rd; et al. Racial survival disparity in head and neck cancer results from low prevalence of human papillomavirus infection in black oropharyngeal cancer patients. Cancer Prev. Res. 2009, 2, 776–781. [Google Scholar] [CrossRef] [Green Version]
- Bonner, J.A.; Giralt, J.; Harari, P.M.; Baselga, J.; Spencer, S.; Bell, D.; Raben, D.; Liu, J.; Schulten, J.; Ang, K.K.; et al. Association of human papillomavirus and p16 status with mucositis and dysphagia for head and neck cancer patients treated with radiotherapy with or without cetuximab: Assessment from a phase 3 registration trial. Eur. J. Cancer 2016, 64, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrowfield, J.; Isenring, E.; Kiss, N.; Laing, E.; Lipson-Smith, R.; Britton, B. The Impact of Human Papillomavirus (HPV) Associated Oropharyngeal Squamous Cell Carcinoma (OPSCC) on Nutritional Outcomes. Nutrients 2021, 13, 514. [Google Scholar] [CrossRef]
- Ye, L.L.; Oei, R.W.; Kong, F.F.; Du, C.R.; Zhai, R.P.; Ji, Q.H.; Hu, C.S.; Ying, H.M. The prognostic value of preoperative prognostic nutritional index in patients with hypopharyngeal squamous cell carcinoma: A retrospective study. J. Transl. Med. 2018, 16, 12. [Google Scholar] [CrossRef] [Green Version]
- Dai, Y.; Fu, X.; Li, T.; Yao, Q.; Su, L.; Su, H.; Li, J. Long-term impact of prognostic nutritional index in cervical esophageal squamous cell carcinoma patients undergoing definitive radiotherapy. Ann. Transl. Med. 2019, 7, 175. [Google Scholar] [CrossRef]
- Miao, J.; Xiao, W.; Wang, L.; Han, F.; Wu, H.; Deng, X.; Guo, X.; Zhao, C. The value of the Prognostic Nutritional Index (PNI) in predicting outcomes and guiding the treatment strategy of nasopharyngeal carcinoma (NPC) patients receiving intensity-modulated radiotherapy (IMRT) with or without chemotherapy. J. Cancer Res. Clin. Oncol. 2017, 143, 1263–1273. [Google Scholar] [CrossRef]
- Vatca, M.; Lucas, J.T., Jr.; Laudadio, J.; D’Agostino, R.B.; Waltonen, J.D.; Sullivan, C.A.; Rouchard-Plasser, R.; Matsangou, M.; Browne, J.D.; Greven, K.M.; et al. Retrospective analysis of the impact of HPV status and smoking on mucositis in patients with oropharyngeal squamous cell carcinoma treated with concurrent chemotherapy and radiotherapy. Oral Oncol. 2014, 50, 869–876. [Google Scholar] [CrossRef] [Green Version]
- Anderson, N.J.; Jackson, J.E.; Wada, M.; Schneider, M.; Poulsen, M.; Rolfo, M.; Fahandej, M.; Gan, H.; Khoo, V. The changing landscape of head and neck cancer radiotherapy patients: Is high-risk, prolonged feeding tube use indicative of on-treatment weight loss? J. Med. Radiat. Sci. 2019, 66, 250–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewczyński, A.; Jabłońska, B.; Mrowiec, S.; Składowski, K.; Rutkowski, T. Nutritional Support in Head and Neck Radiotherapy Patients Considering HPV Status. Nutrients 2020, 13, 57. [Google Scholar] [CrossRef] [PubMed]
- Powell, S.F.; Vu, L.; Spanos, W.C.; Pyeon, D. The Key Differences between Human Papillomavirus-Positive and -Negative Head and Neck Cancers: Biological and Clinical Implications. Cancers 2021, 13, 5206. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | All | HPV(-) | HPV(+) | p |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age (years) | 60.62 ± 8.54 (30–80) | 60.85 ± 7.48 (37–79) | 60.36 ± 9.67 (30–80) | 0.745 |
| Male/female | 87 (68.5%)/40 (31.5%) | 51 (75.1%)/17 (25.0%) | 36 (61.0%)/23 (39.0%) | 0.133 |
| Weight (kg) | ||||
| Before treatment | 75.65 ± 15.24 (44–111) | 72.38 ± 15.24 (44–104.80) | 79.41 ± 14.64 (46–111) | 0.009 |
| After treatment | 71.88 ± 14.17 (42–110) | 70.56 ± 15.24 (42–94.70) | 72.96 ± 14.81 (45–110) | 0.419 |
| Weight difference (kg) | −5.08 ± 4.04 (−17.20–3.00) | −4.32 ± 3.71 (−12.00–3.00) | −5.71 ± 4.23 (−17.20–1.00) | 0.099 |
| Weight difference (%) | −6.49 ± 5.07 (−20.56–4.84) | −5.65 ± 4.85 (−19.35–4.84) | −7.19 ± 5.19 (−20.56–1.85) | 0.144 |
| BMI (kg/m2) groups | 0.371 | |||
| <18.5 | 5 (3.90%) | 4 (5.90%) | 1 (1.70%) | |
| >18.5 | 122 (96.10%) | 64 (94.10%) | 58 (98.30%) | |
| BMI (kg/m2) groups | 0.232 | |||
| <20 | 10 (7.90%) | 9 (13.20%) | 1 (1.70%) | |
| 20–25 | 39 (30.70%) | 24 (35.30%) | 15 (25.40%) | |
| 25–30 | 51 (40.20%) | 21 (30.90%) | 30 (50.80%) | |
| >30 | 27 (21.30%) | 14 (20.60%) | 13 (22.00%) | |
| NRS 2002 | ||||
| Before treatment | 0.35 ± 0.77 (0–4) | 0.41 ± 0.87 (0–4) | 0.28 ± 0.64 (0–4) | 0.680 |
| After treatment | 3.20 ± 1.11 (1–5) | 2.98 ± 1.09 (1–5) | 3.39 ± 1.10 (1–5) | 0.074 |
| Smoking | 0.0004 | |||
| No | 35 (27.60%) | 8 (11.80%) | 27 (45.80%) | |
| Yes | 74 (58.30%) | 51 (75.00%) | 23 (39.00%) | |
| Smoking cessation | 18 (14.20%) | 9 (13.20%) | 9 (15.30%) | |
| Alcohol | 0.012 | |||
| No | 41 (32.30%) | 15 (22.10%) | 26 (44.10%) | |
| Normal drinking | 83 (65.40%) | 50 (73.50%) | 33 (55.90%) | |
| Alcohol abuse | 3 (2.40%) | 3 (4.40%) | 0 (0.00%) | |
| Detailed tumor location | 0.010 | |||
| Tonsil | 91 (71.70%) | 44 (64.70%) | 47 (79.70%) | |
| Palate | 10 (7.90%) | 10 (14.70%) | 0 (0.00%) | |
| Root of the tongue | 22 (17.30%) | 13 (19.10%) | 9 (15.30%) | |
| Other oropharynx | 4 (3.10%) | 1 (1.50%) | 3 (5.10%) | |
| Histopathological grading | 0.049 | |||
| G1 | 7 (8.6%) | 6 (12.8%) | 1 (2.9%) | |
| G2 | 55 (67.9%) | 34 (72.3%) | 21 (61.8%) | |
| G3 | 18 (23.5%) | 7 (14.9%) | 12 (35.3%) | |
| Tumor depth (T) | 0.743 | |||
| T1 | 13 (10.2%) | 8 (11.8%) | 5 (8.5%) | |
| T2 | 42 (33.1%) | 24 (35.3%) | 18 (30.5%) | |
| T3 | 44 (34.6%) | 22 (32.4%) | 22 (37.3%) | |
| T4 | 27 (21.3%) | 13 (19.1%) | 14 (23.7%) | |
| Tx | 1 (0.8%) | 1 (1.5%) | 0 (0.0%) | |
| Lymph node metastasis (N) | 0.029 | |||
| N0 | 26 (20.50%) | 20 (29.40%) | 6 (10.20%) | |
| N1 | 26 (20.50%) | 16 (23.50%) | 10 (16.90%) | |
| N2 | 57 (44.90%) | 24 (35.30%) | 33 (55.90%) | |
| N3 | 17 (13.40%) | 8 (11.80%) | 9 (15.30%) | |
| Nx | 1 (0.80%) | 0 (0.00%) | 1 (1.70%) | |
| Clinical manifestation | ||||
| Pain | 73 (57.50%) | 39 (57.40%) | 34 (57.60%) | 0.882 |
| Neck mass | 46 (36.20%) | 17 (25.00%) | 29 (49.20%) | 0.008 |
| Cough | 6 (4.70%) | 5 (7.40%) | 1 (1.70%) | 0.215 |
| Hoarseness | 11 (8.70%) | 7 (10.30%) | 4 (6.80%) | 0.543 |
| Dysphagia | 34 (26.80%) | 19 (27.90%) | 15 (25.40%) | 0.906 |
| Dyspnea | 2 (1.60%) | 2 (2.90%) | 0 (0.00%) | 0.499 |
| Hemoptysis | 6 (4.70%) | 4 (5.90%) | 2 (3.40%) | 0.685 |
| Weight loss | 8 (6.30%) | 5 (7.40%) | 3 (5.10%) | 0.724 |
| Hearing impairment | 2 (1.60%) | 0 (0.00%) | 2 (3.40%) | 0.214 |
| Duration of medical history (months) | 5.55 ± 6.85 | 5.92 ± 60 | 5.13 ± 7.26 | 0.403 |
| Treatment duration (days) | 45.88 ± 9.76 | 43.64 ± 9.00 | 48.51 ± 10.04 | 0.005 |
| General treatment regimen | 0.003 | |||
| RT | 31 (24.4%) | 24 (35.3%) | 7 (11.9%) | |
| CRT | 96 (75.6%) | 44 (64.7%) | 52 (88.1%) | |
| Detailed treatment regimen | 0.006 | |||
| RT | 25 (19.70%) | 18 (26.50%) | 7 (11.90%) | |
| CRT | 51 (40.20%) | 18 (26.50%) | 33 (55.90%) | |
| pRT | 6 (4.70%) | 6 (8.80%) | 0 (0.00%) | |
| IndCT RT | 14 (11.00%) | 8 (11.80%) | 6 (10.20%) | |
| IndCT CRT | 30 (23.60%) | 17 (25.00%) | 13 (22.00%) | |
| Lymph node invasion according to treatment | ||||
| RT | 0.053 | |||
| N0–1 | 23 (74.19%) | 20 (87.00%) | 3 (13.00%) | |
| N2–3 | 8 (25.81%) | 4 (50.00%) | 4 (50.00%) | |
| CRT | 0.268 | |||
| N0–1 | 29 (30.20%) | 16 (55.20%) | 13 (44.80%) | |
| N2–3 | 67 (69.80%) | 28 (41.80%) | 39 (58.20%) |
| Feature | RT | CRT | p | p H–B |
|---|---|---|---|---|
| All | ||||
| N0–1 | 23 (44.20%) | 29 (55.80%) | <0.0001 | 0.00012 |
| N2–3 | 8 (10.70%) | 67 (89.30%) | ||
| HPV(-) | ||||
| N0–1 | 20 (55.60%) | 16 (44.40%) | 0.0003 | 0.0006 |
| N2–3 | 4 (12.50%) | 28 (87.50%) | ||
| HPV(+) | ||||
| N0–1 | 3 (18.75%) | 13 (81.25%) | 0.3750 | 0.3750 |
| N2–3 | 4 (9.30%) | 39 (90.70%) |
| HPV(-) | HPV(+) | p | H–B | |
|---|---|---|---|---|
| Weight 0–Weight 1 (kg) | 4.32 ± 3.71 | 5.71 ± 4.23 | 0.099 | 0.891 |
| Weight 0–Weight 1 (%) | 5.65 ± 4.85 | 7.19 ± 5.19 | 0.144 | 1.000 |
| BMI 0–BMI 1 | 1.54 ± 1.34 | 1.98 ± 1.40 | 0.134 | 1.000 |
| CRP 0–CRP 1 | −24.00 ± 44.48 | −18.77 ± 23.41 | 0.431 | 1.000 |
| Albumin 0–Albumin 1 (g/L) | 4.50 ± 4.35 | 5.02 ± 4.96 | 0.553 | 1.000 |
| Prealbumin 0–Prealbumin 1 (g/L) | 0.07 ± 0.10 | 0.08 ± 0.10 | 0.563 | 1.000 |
| Hemoglobin 0–Hemoglobin 1 (g/dL) | 1.75 ± 1.46 | 1.85 ± 1.58 | 0.717 | 0.717 |
| TLC 0–TLC 1 (/mm3) | 1.20 ± 0.72 | 1.37 ± 0.69 | 0.174 | 1.000 |
| PNI 0–PNI 1 | 4.51 ± 4.35 | 5.92 ± 4.96 | 0.552 | 1.000 |
| Feature | All | HPV(-) | HPV(+) |
|---|---|---|---|
| Weight 0 (kg) | 75.65 ± 15.24 (44–111) | 72.38 ± 15.24 (44–104.80) | 79.41 ± 14.64 (46–111) |
| Weight 1(kg) | 71.88 ± 14.17 (42–110) | 70.56 ± 15.24 (42–94.70) | 72.96 ± 14.81 (45–110) |
| p | <0.0001 | <0.0001 | <0.0001 |
| p H–B | <0.0001 | <0.0001 | <0.0001 |
| BMI 0 (kg/m2) | 26.84 ± 4.65 (17.21–40.44) | 25.75 ± 4.70 (17.21–37.58) | 28.10 ± 4.30 (18.20–40.44) |
| BMI 1 (kg/m2) | 25.26 ± 4.16 (17.26–31.81) | 24.69 ± 4.04 (17.26–33.96) | 25.72 ± 4.24 (17.80–37.81) |
| p | <0.0001 | <0.0001 | <0.0001 |
| p H–B | <0.0001 | <0.0001 | <0.0001 |
| NRS 2002 0 | 0.35 ± 0.77 (0–4) | 0.41 ± 0.87 (0–4) | 0.28 ± 0.64 (0–4) |
| NRS 2002 1 | 3.20 ± 1.11 (1–5) | 2.98 ± 1.09 (1–5) | 3.39 ± 1.10 (1–5) |
| p | <0.0001 | <0.0001 | <0.0001 |
| p H–B | <0.0001 | <0.0001 | <0.0001 |
| CRP 0 (g/L) | 5.15 ± 7.07 (0.16–36.90) | 6.79 ± 8.39 (0.16–36.90) | 3.40 ± 4.80 (0.17–27.20) |
| CRP 1 (g/L) | 26.60 ± 35.93 (0.17–197.00) | 30.96 ± 44.43 (0.20–197.00) | 22.00 ± 23.50 (0.17–87.20) |
| p | <0.0001 | <0.0001 | <0.0001 |
| p H–B | <0.0001 | <0.0001 | <0.0001 |
| Albumin 0 (g/L) | 41.67 ± 3.68 (33.00–50.00) | 41.58 ± 3.65 (33.00–49.00) | 41.77 ± 3.74 (32.00–50.00) |
| Albumin 1 (g/L) | 36.95 ± 3.92 (30.00–49.00) | 37.05 ± 4.11 (30.00–47.00) | 36.84 ± 3.75 (30.00–49.00) |
| p | <0.0001 | <0.0001 | <0.0001 |
| p H–B | <0.0001 | <0.0001 | <0.0001 |
| Prealbumin 0 (g/L) | 0.28 ± 0.08 (0.13–0.52) | 0.26 ± 0.09 (0.13–0.52) | 0.29 ± 0.07 (0.18–0.45) |
| Prealbumin 1 (g/L) | 0.20 ± 0.08 (0.08–0.49) | 0.19 ± 0.07 (0.08–0.35) | 0.21 ± 0.09 (0.09–0.49) |
| p | <0.0001 | 0.005 | 0.0004 |
| p H–B | <0.0001 | 0.005 | 0.0008 |
| Hemoglobin 0 (g/dL) | 13.97 ± 1.50 (10.60–17.40) | 10.60 ± 1.51 (12.85–15.35) | 13.88 ± 1.51 (10.80–16.90) |
| Hemoglobin 1 (g/dL) | 12.70 ± 1.50 (9.40–16.30) | 12.29 ± 1.46 (9.40–16.30) | 12.03 ± 1.54 (9.50–15.80) |
| p | <0.0001 | <0.0001 | <0.0001 |
| p H–B | <0.0001 | <0.0001 | <0.0001 |
| TLC 0 (/mm3) | 1.90 ± 0.72 (0.57–4.84) | 1.91 ± 0.71 (0.65–3.94) | 1.89 ± 0.73 (0.57–4.54) |
| TLC 1 (/mm3) | 0.62 ± 0.37 (0.11–2.84) | 0.71 ± 0.44 (0.11–2.84) | 0.52 ± 0.24 (0.17–1.34) |
| p | <0.0001 | <0.0001 | <0.0001 |
| p H–B | <0.0001 | <0.0001 | <0.0001 |
| PNI 0 | 41.68 ± 3.68 (32.00–50.00) | 41.59 ± 3.65 (33.01–49.01) | 41.78 ± 3.74 (32.00–50.00) |
| PNI 1 | 36.95 ± 3.92 (30.00–49.00) | 37.05 ± 4.11 (30.00–47.00) | 36.85 ± 3.75 (30.00–49.00) |
| p | <0.0001 | <0.0001 | <0.0001 |
| p H–B | <0.0001 | <0.0001 | <0.0001 |
| Feature | CRT | RT | ||
|---|---|---|---|---|
| HPV(-) | HPV(+) | HPV(-) | HPV(+) | |
| Weight 0 (kg) | 72.60 ± 14.13 | 78.58 ± 14.92 | 71.99 ± 17.04 | 85.53 ± 11.43 |
| Weight 1(kg) | 68.96 ± 13.24 | 72.10 ± 14.71 | 75.08 ± 13.44 | 86.73 ± 9.72 |
| p | <0.0001 | <0.0001 | 0.004 | 0.248 |
| p H–B | 0.0004 | <0.0001 | 0.062 | 0.993 |
| BMI 0 (kg/m2) | 25.11 ± 4.00 | 27.78 ± 4.31 | 26.92 ± 5.69 | 30.52 ± 3.58 |
| BMI 1 (kg/m2) | 23.56 ± 3.21 | 25.40 ± 4.10 | 27.91 ± 4.53 | 30.91 ± 3.47 |
| p | <0.0001 | <0.0001 | 0.004 | 0.248 |
| p H–B | 0.0004 | <0.0001 | 0.066 | 1.000 |
| NRS 2002 0 | 0.36 ± 0.84 | 0.20 ± 0.40 | 0.50 ± 0.93 | 0.86 ± 1.46 |
| NRS 2002 1 | 3.06 ± 1.15 | 3.40 ± 1.12 | 2.73 ± 0.90 | 3.33 ± 0.58 |
| p | <0.0001 | <0.0001 | 0.004 | 0.480 |
| p H–B | <0.0001 | <0.0001 | 0.058 | 1.000 |
| CRP 0 (g/L) | 7.18 ± 9.76 | 2.94 ± 3.77 | 6.02 ± 4.84 | 6.81 ± 9.24 |
| CRP 1 (g/L) | 27.13 ± 35.78 | 20.66 ± 22.49 | 38.63 ± 58.38 | 31.59 ± 30.05 |
| p | 0.0014 | <0.0001 | 0.014 | 1.000 |
| p H–B | 0.025 | <0.0001 | 0.167 | 1.000 |
| Albumin 0 (g/L) | 42.05 ± 3.91 | 41.92 ± 3.93 | 40.67 ± 2.96 | 40.71 ± 1.80 |
| Albumin 1 (g/L) | 37.23 ± 4.16 | 37.02 ± 3.77 | 36.71 ± 4.10 | 35.57 ± 3.60 |
| p | <0.0001 | <0.0001 | 0.004 | 0.131 |
| p H–B | 0.0004 | <0.0001 | 0.062 | 1.000 |
| Prealbumin 0 (g/L) | 0.277 ± 0.079 | 0.301 ± 0.070 | 0.230 ± 0.098 | 0.213 ± 0.029 |
| Prealbumin 1 (g/L) | 0.213 ± 0.072 | 0.217 ± 0.081 | 0.150 ± 0.048 | 0.200 ± 0.120 |
| p | 0.054 | 0.0003 | 0.061 | 1.000 |
| p H–B | 0.543 | 0.006 | 0.552 | 1.000 |
| Hemoglobin 0 (g/dL) | 14.08 ± 1.50 | 13.85 ± 1.56 | 14.00 ± 1.54 | 14.09 ± 1.10 |
| Hemoglobin 1 (g/dL) | 11.98 ± 1.40 | 11.82 ± 1.41 | 12.87 ± 1.41 | 13.64 ± 1.65 |
| p | <0.0001 | <0.0001 | 0.0002 | 0.221 |
| p H–B | <0.0001 | <0.0001 | 0.003 | 1.000 |
| TLC 0 (/mm3) | 1.91 ± 0.78 | 1.89 ± 0.75 | 1.91 ± 0.56 | 1.85 ± 0.57 |
| TLC 1 (/mm3) | 0.69 ± 0.47 | 0.53 ± 0.25 | 0.74 ± 0.38 | 0.40 ± 0.16 |
| p | <0.0001 | <0.0001 | <0.0001 | 0.023 |
| p H–B | <0.0001 | <0.0001 | 0.0002 | 0.257 |
| PNI 0 | 42.06 ± 3.91 | 41.93 ± 3.93 | 40.68 ± 2.96 | 40.72 ± 1.80 |
| PNI 1 | 37.23 ± 4.16 | 37.02 ± 3.77 | 36.72 ± 4.10 | 35.57 ± 3.60 |
| p | <0.0001 | <0.0001 | 0.004 | 0.131 |
| p H–B | 0.0003 | <0.0001 | 0.058 | 0.914 |
| Variable | OS HPV- | OS HPV+ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-value | HR (95%CI) | p-Value | |||
| CRP > 3.50 vs. < 3.50 | 62 | 2.08 (0.90–4.82) | 0.088 | 3.45 1.37–8.68 | 0.008 | 58 | 2.23 (0.70–7.13) | 0.176 | 2.92 0.90–9.46 | 0.075 |
| Albumin (g/L) > 40.0 vs. < 40.0 | 62 | 1.14 (0.50–2.62) | 0.755 | 57 | 3.26 (0.71–14.89) | 0.127 | 4.21 0.89–19.86 | 0.070 | ||
| Prealbumin (g/L) > 0.28 vs. < 0.28 | 46 | 0.44 (0.12–1.58) | 0.208 | 44 | 2.37 (0.59–9.54) | 0.223 | ||||
| Hb 0 (g/dL) > 13.5 vs. < 13.5 | 68 | 0.69 (0.32–1.49) | 0.345 | 59 | 1.31 (0.39–4.37) | 0.659 | ||||
| LC 0 (/mm3) > 1.28 vs. < 1.28 | 68 | 0.63 (0.26–1.50) | 0.299 | 59 | 0.63 (0.17–2.35) | 0.496 | ||||
| PNI > 39.01 vs. < 39.01 | 62 | 1.04 (0.42–2.53) | 0.935 | 57 | 1.56 (0.34–7.16) | 0.569 | ||||
| Age > 60 vs. ≤ 60 | 68 | 0.788 (0.36–1.71) | 0.546 | 59 | 0.85 (0.27–2.63) | 0.772 | ||||
| Gender F vs. M | 0.49 (0.18–1.31) | 0.157 | 0.12 0.02–0.58 | 0.009 | 59 | 0.58 (0.16–2.15) | 0.414 | |||
| General location tonsils vs. others | 68 | 1.57 (0.68–3.63) | 0.289 | |||||||
| Tumor depth (T) T3–4 vs. T1–2 | 67 | 0.95 (0.44–2.06) | 0.899 | 59 | 1.79 (0.48–6.62) | 0.385 | ||||
| Lymph node metastasis N2–3 vs. N0–1 | 68 | 1.80 (0.83–3.93) | 0.139 | 58 | 1.15 (0.31–4.26) | 0.832 | ||||
| Radiotherapy vs. chemoradiotherapy | 68 | 0.93 (0.42–2.06) | 0.858 | 59 | 0.60 (0.08–4.64) | 0.623 | ||||
| BMI 0 > 24.53 vs. < 24.53 | 68 | 0.39 (0.17–0.87) | 0.022 | 59 | 0.57 (0.15–2.12) | 0.400 | ||||
| NRS 2002 > 1 vs. ≤ 1 | 4.03 (1.56–10.37) | 0.004 | 3.83 1.22–12.01 | 0.021 | 58 | 0.00 | 1.00 | |||
| Smoking Yes vs. no | 68 | 1.18 (0.49–2.84) | 0.706 | 59 | 0.63 (0.17–2.32) | 0.483 | ||||
| Alcohol abuse Yes vs. no | 68 | 4.17 (1.20–14.47) | 0.025 | 6.39 1.40–29.14 | 0.017 | |||||
| Variable | DFS HPV- | DFS HPV+ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||
| HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | HR (95%CI) | p-Value | |||
| CRP >3.50 vs. <3.50 | 62 | 2.78 1.13–6.82 | 0.026 | 2.90 1.08–7.76 | 0.034 | 58 | 4.95 1.18–20.76 | 0.029 | ||
| Albumin (g/L) >40.0 vs. <40.0 | 62 | 0.902 0.39–2.09 | 0.810 | 57 | 0.96 0.23–4.05 | 0.957 | ||||
| Prealbumin (g/L) >0.28 vs. <0.28 | 46 | 0.50 0.14–1.79 | 0.288 | 44 | 1.01 0.25–4.02 | 0.993 | ||||
| Hb 0 (g/dL) >13.5 vs. <13.5 | 68 | 0.38 (0.17–0.87) | 0.021 | 0.34 0.13–0.90 | 0.029 | 59 | 1.15 (0.27–4.82) | 0.848 | ||
| TLC 0 (/mm3) >1.28 vs. <1.28 | 68 | 0.61 (0.25–1.47) | 0.271 | 59 | 0.19 (0.05–0.77) | 0.020 | 0.20 (0.05–0.82) | 0.025 | ||
| PNI > 39.01 vs. < 39.01 | 62 | 0.55 0.23–1.28 | 0.163 | 57 | 0.45 0.11–1.89 | 0.276 | ||||
| Age > 60 vs. ≤ 60 | 68 | 0.75 0.34–1.65 | 0.474 | 59 | 0.88 0.22–3.53 | 0.859 | ||||
| Gender F vs. M | 68 | 0.99 0.41–2.39 | 0.984 | 59 | 0.95 0.22–3.96 | 0.941 | ||||
| General location tonsils vs. others | 68 | 1.35 0.58–3.15 | 0.482 | 59 | 1.00 | |||||
| Tumor depth (T) T3–4 vs. T1–2 | 67 | 1.20 0.54–2.64 | 0.655 | 59 | 2.02 0.41–10.00 | 0.390 | ||||
| Lymph node metastasisN2–3 vs. N0–1 | 68 | 3.55 (1.51–8.34) | 0.004 | 4.26 (1.59–11.43) | 0.004 | 58 | 2.86 (0.35–23.24) | 0.326 | ||
| Radiotherapy vs. chemoradiotherapy | 68 | 0.71 (0.31–1.64) | 0.422 | 0.00 | 1.00 | |||||
| BMI 0 >24.53 vs. <24.53 | 68 | 0.41 0.18–0.91 | 0.028 | 59 | 0.377 0.09–1.58 | 0.182 | ||||
| NRS 2002 >1 vs. ≤1 | 68 | 4.46 1.74–11.45 | 0.002 | 5.89 1.79–19.37 | 0.003 | 58 | 0.00 | 1.00 | ||
| Smoking Yes vs. no | 68 | 0.88 0.39–1.99 | 0.760 | 59 | 1.20 0.29–5.03 | 0.801 | ||||
| Alcohol abuse Yes vs. no | 68 | 2.92 0.68–12.59 | 0.150 | 8.01 1.41–45.39 | 0.019 | 59 | 1.00 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brewczyński, A.; Jabłońska, B.; Mazurek, A.M.; Mrochem-Kwarciak, J.; Mrowiec, S.; Śnietura, M.; Kentnowski, M.; Kotylak, A.; Kołosza, Z.; Składowski, K.; et al. Analysis of Selected Nutritional Parameters in Patients with HPV-Related and Non-HPV-Related Oropharyngeal Cancer before and after Radiotherapy Alone or Combined with Chemotherapy. Cancers 2022, 14, 2335. https://doi.org/10.3390/cancers14092335
Brewczyński A, Jabłońska B, Mazurek AM, Mrochem-Kwarciak J, Mrowiec S, Śnietura M, Kentnowski M, Kotylak A, Kołosza Z, Składowski K, et al. Analysis of Selected Nutritional Parameters in Patients with HPV-Related and Non-HPV-Related Oropharyngeal Cancer before and after Radiotherapy Alone or Combined with Chemotherapy. Cancers. 2022; 14(9):2335. https://doi.org/10.3390/cancers14092335
Chicago/Turabian StyleBrewczyński, Adam, Beata Jabłońska, Agnieszka Maria Mazurek, Jolanta Mrochem-Kwarciak, Sławomir Mrowiec, Mirosław Śnietura, Marek Kentnowski, Anna Kotylak, Zofia Kołosza, Krzysztof Składowski, and et al. 2022. "Analysis of Selected Nutritional Parameters in Patients with HPV-Related and Non-HPV-Related Oropharyngeal Cancer before and after Radiotherapy Alone or Combined with Chemotherapy" Cancers 14, no. 9: 2335. https://doi.org/10.3390/cancers14092335