
Spread Through Air Spaces (STAS) Is an Independent Prognostic Factor in Resected Lung Squamous Cell Carcinoma

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Histopathologic Evaluation
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
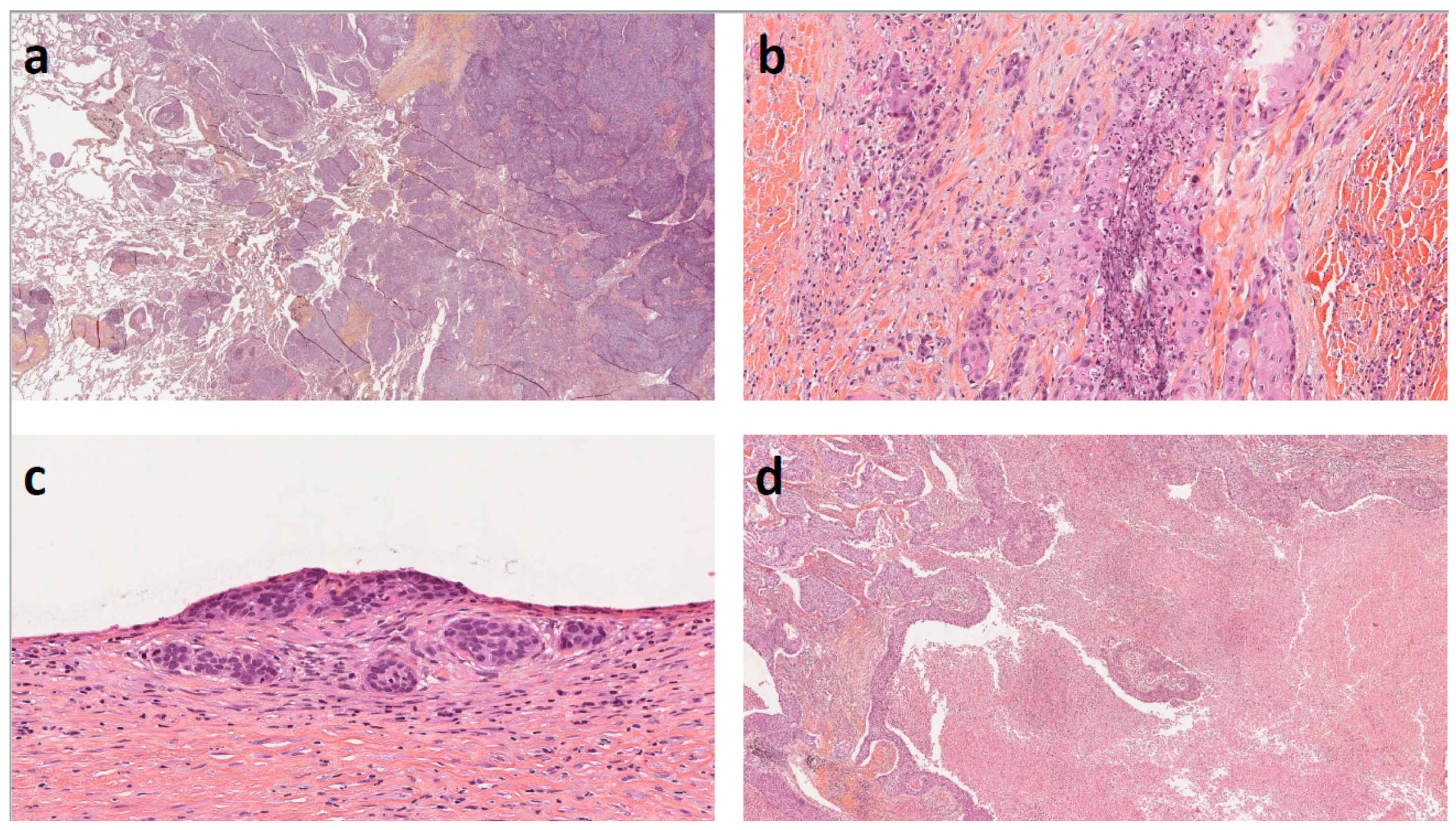
3.2. Histopathological Features
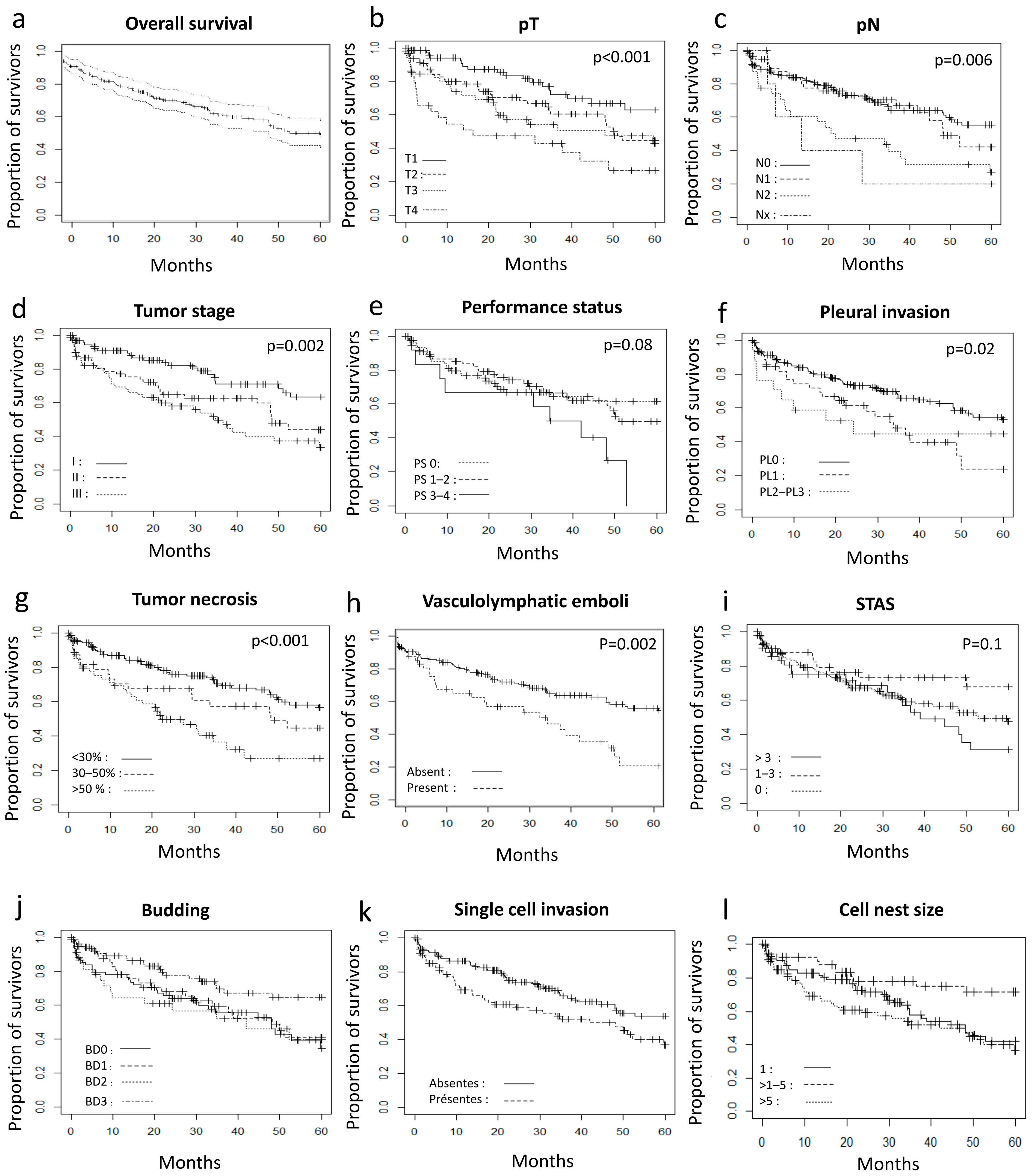
3.3. Correlation of Overall Survival with Clinicopathologic Data
3.4. Association between Clinicopathologic Factors and Survival
3.5. Subgroup Analysis in Stage I and II Patients Who Underwent Lobectomy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Statement
References
- WHO Classification of Tumors Editorial Board. Thoracic Tumors, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021; ISBN 978-92-832-4506-3. [Google Scholar]
- Moreira, A.L.; Ocampo, P.S.S.; Xia, Y.; Zhong, H.; Russell, P.A.; Minami, Y.; Cooper, W.A.; Yoshida, A.; Bubendorf, L.; Papotti, M.; et al. A Grading System for Invasive Pulmonary Adenocarcinoma: A Proposal from the International Association for the Study of Lung Cancer Pathology Committee. J. Thorac. Oncol. 2020, 15, 1599–1610. [Google Scholar] [CrossRef] [PubMed]
- Warth, A.; Muley, T.; Kossakowski, C.A.; Goeppert, B.; Schirmacher, P.; Dienemann, H.; Weichert, W. Prognostic Impact of Intra-alveolar Tumor Spread in Pulmonary Adenocarcinoma. Am. J. Surg. Pathol. 2015, 39, 793–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aly, R.G.; Rekhtman, N.; Li, X.; Takahashi, Y.; Eguchi, T.; Tan, K.S.; Rudin, C.M.; Adusumilli, P.S.; Travis, W.D. Spread through Air Spaces (STAS) Is Prognostic in Atypical Carcinoid, Large Cell Neuroendocrine Carcinoma, and Small Cell Carcinoma of the Lung. J. Thorac. Oncol. 2019, 14, 1583–1593. [Google Scholar] [CrossRef]
- Takeda-Miyata, N.; Konishi, E.; Tanaka, T.; Shimomura, M.; Tsunezuka, H.; Okada, S.; Ishihara, S.; Ishikawa, N.; Inoue, M. Prognostic significance of spread through air spaces in pulmonary metastases from colorectal cancer. Lung Cancer 2020, 149, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Tan, K.S.; Kadota, K.; Eguchi, T.; Bains, S.; Rekhtman, N.; Adusumilli, P.S.; Travis, W.D. Spread through Air Spaces (STAS) Is an Independent Predictor of Recurrence and Lung Cancer–Specific Death in Squamous Cell Carcinoma. J. Thorac. Oncol. 2017, 12, 223–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadota, K.; Kushida, Y.; Katsuki, N.; Ishikawa, R.; Ibuki, E.; Motoyama, M.; Nii, K.; Yokomise, H.; Bandoh, S.; Haba, R. Tumor Spread through Air Spaces Is an Independent Predictor of Recurrence-free Survival in Patients with Resected Lung Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2017, 41, 1077–1086. [Google Scholar] [CrossRef]
- Yanagawa, N.; Shiono, S.; Endo, M.; Ogata, S. Tumor spread through air spaces is a useful predictor of recurrence and prognosis in stage I lung squamous cell carcinoma, but not in stage II and III. Lung Cancer 2018, 120, 14–21. [Google Scholar] [CrossRef]
- Jia, M.; Yu, S.; Yu, J.; Li, Y.; Gao, H.; Sun, P.-L. Comprehensive analysis of spread through air spaces in lung adenocarcinoma and squamous cell carcinoma using the 8th edition AJCC/UICC staging system. BMC Cancer 2020, 20, 705. [Google Scholar] [CrossRef]
- Han, Y.B.; Kim, H.; Mino-Kenudson, M.; Cho, S.; Kwon, H.J.; Lee, K.R.; Kwon, S.; Lee, J.-S.J.; Kim, K.; Jheon, S.; et al. Tumor spread through air spaces (STAS): Prognostic significance of grading in non-small cell lung cancer. Mod. Pathol. 2021, 34, 549–561. [Google Scholar] [CrossRef]
- Ikeda, T.; Kadota, K.; Yoshida, C.; Ishikawa, R.; Go, T.; Haba, R.; Yokomise, H. The epithelial-mesenchymal transition phenotype is associated with the frequency of tumor spread through air spaces (STAS) and a High risk of recurrence after resection of lung carcinoma. Lung Cancer 2021, 153, 49–55. [Google Scholar] [CrossRef]
- Gürel, D.; Ulukuş, Ç.; Karaçam, V.; Ellidokuz, H.; Umay, C.; Öztop, İ.; Sarıoğlu, S. The prognostic value of morphologic findings for lung squamous cell carcinoma patients. Pathol. Res. Pract. 2016, 212, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Swinson, D.E.; Jones, J.L.; Richardson, D.; Cox, G.; Edwards, J.G.; O’Byrne, K.J. Tumour necrosis is an independent prognostic marker in non-small cell lung cancer: Correlation with biological variables. Lung Cancer 2002, 37, 235–240. [Google Scholar] [CrossRef]
- Park, S.Y.; Lee, H.-S.; Jang, H.-J.; Lee, G.K.; Chung, K.Y.; Zo, J.I. Tumor Necrosis as a Prognostic Factor for Stage IA Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2011, 91, 1668–1673. [Google Scholar] [CrossRef] [PubMed]
- Kadota, K.; Nitadori, J.I.; Woo, K.M.; Sima, C.S.; Finley, D.J.; Rusch, V.W.; Adusumilli, P.S.; Travis, W.D. Comprehensive Pathological Analyses in Lung Squamous Cell Carcinoma: Single Cell Invasion, Nuclear Diameter, and Tumor Budding Are Independent Prognostic Factors for Worse Outcomes. J. Thorac. Oncol. 2014, 9, 1126–1139. [Google Scholar] [CrossRef] [Green Version]
- Komaki, R.; Fujii, T.; Perkins, P.; Ro, J.Y.; Allen, P.K.; Mason, K.A.; Mountain, C.F.; Milas, L. Apoptosis and mitosis as prognostic factors in pathologically staged N1 nonsmall cell lung cancer. Int. J. Radiat. Oncol. 1996, 36, 601–605. [Google Scholar] [CrossRef]
- Kadota, K.; Miyai, Y.; Katsuki, N.; Kushida, Y.; Matsunaga, T.; Okuda, M.; Yokomise, H.; Kanaji, N.; Bandoh, S.; Haba, R. A Grading System Combining Tumor Budding and Nuclear Diameter Predicts Prognosis in Resected Lung Squamous Cell Carcinoma. Am. J. Surg. Pathol. 2017, 41, 750–760. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Ma, W.; Wang, J.; Yu, L.; Zhang, X.; Wang, Z.; Tan, B.; Wang, N.; Bai, B.; Yang, S.; et al. Tumor-Stroma Ratio Is an Independent Predictor for Survival in Esophageal Squamous Cell Carcinoma. J. Thorac. Oncol. 2012, 7, 1457–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xi, K.-X.; Wen, Y.-S.; Zhu, C.-M.; Yu, X.-Y.; Qin, R.-Q.; Zhang, X.-W.; Lin, Y.-B.; Rong, T.-H.; Wang, W.-D.; Chen, Y.-Q.; et al. Tumor-stroma ratio (TSR) in non-small cell lung cancer (NSCLC) patients after lung resection is a prognostic factor for survival. J. Thorac. Dis. 2017, 9, 4017–4026. [Google Scholar] [CrossRef] [Green Version]
- Zare, S.Y.; Aisagbonhi, O.; Hasteh, F.; Fadare, O. Independent Validation of Tumor Budding Activity and Cell Nest Size as Determinants of Patient Outcome in Squamous Cell Carcinoma of the Uterine Cervix. Am. J. Surg. Pathol. 2020, 44, 1151–1160. [Google Scholar] [CrossRef]
- The American Joint Committee on Cancer. AJCC Cancer Staging Atlas, 8th ed.; Springer Nature: Cham, Switzerland, 2016. [Google Scholar]
- Travis, W.D.; Brambilla, E.; Rami-Porta, R.; Vallières, E.; Tsuboi, M.; Rusch, V.; Goldstraw, P. Visceral Pleural Invasion: Pathologic Criteria and Use of Elastic Stains: Proposal for the 7th Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2008, 3, 1384–1390. [Google Scholar] [CrossRef] [Green Version]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.-F.F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Neppl, C.; Zlobec, I.; Schmid, R.A.; Berezowska, S. Validation of the International Tumor Budding Consensus Conference (ITBCC) 2016 recommendation in squamous cell carcinoma of the lung—A single-center analysis of 354 cases. Mod. Pathol. 2020, 33, 802–811. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. R Found. Stat. Comput. 2018, 2. Available online: https://www.R-project.org (accessed on 1 August 2021).
- Therneau, T. A Package for Survival Analysis in S. R Package Version. Survival (Lond). 2012. Available online: http://r-forge.r-project.org (accessed on 1 August 2021).
- Gross, D.J.; Hsieh, M.-S.; Li, Y.; Dux, J.; Rekhtman, N.; Jones, D.R.; Travis, W.D.; Adusumilli, P.S. Spread through Air Spaces (STAS) in Non−Small Cell Lung Carcinoma. Am. J. Surg. Pathol. 2021, 45, 1509–1515. [Google Scholar] [CrossRef]
- Onozato, M.L.; Klepeis, V.E.; Yagi, Y.; Mino-Kenudson, M. A role of three-dimensional (3D) reconstruction in the classification of lung adenocarcinoma. Stud. Health Technol. Inform. 2012, 179, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Onozato, M.L.; Kovach, A.E.; Yeap, B.Y.; Morales-Oyarvide, V.; Klepeis, V.E.; Tammireddy, S.; Heist, R.S.; Mark, E.J.; Dias-Santagata, D.; John Iafrate, A.; et al. Tumor islands in resected early-stage lung adenocarcinomas are associated with unique clinicopathologic and molecular characteristics and worse prognosis. Am. J. Surg. Pathol. 2013, 37, 287–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taira, T.; Ishii, G.; Nagai, K.; Yoh, K.; Takahashi, Y.; Matsumura, Y.; Kojima, M.; Ohmatsu, H.; Goto, K.; Niho, S.; et al. Characterization of the immunophenotype of the tumor budding and its prognostic implications in squamous cell carcinoma of the lung. Lung Cancer 2012, 76, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Takemoto, A.; Okitaka, M.; Takagi, S.; Takami, M.; Sato, S.; Nishio, M.; Okumura, S.; Fujita, N. A critical role of platelet TGF-β release in podoplanin-mediated tumour invasion and metastasis. Sci. Rep. 2017, 7, 42186. [Google Scholar] [CrossRef]
- Weichert, W.; Kossakowski, C.; Harms, A.; Schirmacher, P.; Muley, T.; Dienemann, H.; Warth, A. Proposal of a prognostically relevant grading scheme for pulmonary squamous cell carcinoma. Eur. Respir. J. 2016, 47, 938–946. [Google Scholar] [CrossRef]
- An, N.; Leng, X.; Wang, X.; Sun, Y.; Chen, Z. Survival comparison of Three histological subtypes of lung squamous cell carcinoma: A population-based propensity score matching analysis. Lung Cancer 2020, 142, 13–19. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | n (%) | 5-Year Survival Rate | p (Log-Rank Test) |
|---|---|---|---|
| Sex | 0.9 | ||
| M | 220 (91.3) | 60.4% | |
| F | 21 (8.7) | 61.9% | |
| Age | 0.9 | ||
| ≤65 years | 99 (41.1) | 58.6% | |
| >65 years | 142 (58.9) | 62% | |
| PS | 0.08 | ||
| 0 | 79 (32.8) | 68.3% | |
| 1–2 | 80 (33.2) | 65% | |
| 3–4 | 12 (5) | 25% | |
| Unknown | 70 (29) | 52.9% | |
| Tumor side | 0.5 | ||
| Right | 127 (52.7) | 59.8% | |
| Left | 114 (47.3) | 61.4% | |
| Location | 0.1 | ||
| Peripheral or intermediate | 113 (46.9) | 58.4% | |
| Central | 128 (47.3) | 62.5% | |
| pT | <0.001 | ||
| pT1 | 78 (32.4) | 76.9% | |
| pT2 | 78 (32.4) | 59% | |
| pT3 | 52 (21.6) | 54.7% | |
| pT4 | 30 (12.4) | 36.7% | |
| Not assessable | 2 (0.8) | 50% | |
| pN | 0.006 | ||
| pN0 | 143 (59.3) | 66.4% | |
| pN1 | 60 (24.9) | 63.3% | |
| pN2 | 32 (13.3) | 33.4% | |
| pNx | 6 (2.5) | 33.3% | |
| Pathological Stage | 0.002 | ||
| I | 93 (38.6) | 75.3% | |
| II | 70 (29) | 58.6% | |
| III | 70 (29) | 47.1% | |
| Not assessable | 8 (3.3) | 37.5% | |
| Number of metastatic lymph nodes station | 0.1 | ||
| 0 | 143 (59.3) | 64.4% | |
| 1 | 64 (26.5) | 56.2% | |
| ≥2 | 28 (11.6) | 46.4% | |
| Unknown | 6 (2.5) | 33% | |
| Pleural invasion | 0.02 | ||
| PL0 | 177 (73.4) | 65.5% | |
| PL1 or PL2 | 52 (21.6) | 48.1% | |
| PL 3 | 12 (5) | 50% | |
| Peritumoral pneumonitis | 0.3 | ||
| Absent | 150 (62.2) | 62.7% | |
| Present | 91 (37.8) | 57.1% | |
| Obstructive pneumonitis | 0.8 | ||
| Absent | 235 (97.5) | 60.4% | |
| Present | 6 (2.5) | 66.7% | |
| Type | 0.04 | ||
| Keratinizing | 93 (39.6) | 59.1% | |
| Not keratinizing | 135 (56) | 59.3% | |
| Basaloid | 13 (5.4) | 92.3% | |
| Quality of the resection | 0.5 | ||
| R0 | 228 (94.6) | 61.4% | |
| R1 | 13 (5.4) | 46.1% | |
| Differentiation | 0.8 | ||
| Poorly | 65 (27) | 63.1% | |
| Moderately | 125 (51.9) | 60% | |
| Well | 51 (21.2) | 58.8% | |
| Tumor to stroma ratio | 0.7 | ||
| <30% | 94 (39) | 59.6% | |
| ≥30% et <50% | 72 (29.9) | 59.9% | |
| ≥50% | 75 (31.1) | 65.3% | |
| Percentage of tumor necrosis | <0.001 | ||
| <30% | 146 (60.6) | 68.5% | |
| ≥30% et <50% | 39 (16.2) | 53.8% | |
| ≥50% | 56 (23.3) | 44.6% | |
| In situ carcinoma | 0.6 | ||
| Present | 47 (19.5) | 63.8% | |
| Absent | 194 (80.5) | 59.8% | |
| Vascular and/or lymphatic emboli | 0.002 | ||
| Absent | 194 (80.5) | 65.5% | |
| Present | 47 (19.5) | 42.5% | |
| STAS | 0.1 | ||
| Absent | 154 (63.9) | 59.7% | |
| ≤3 alveoli | 44 (18.2) | 75% | |
| >3 alveoli | 42 (17.4) | 50% | |
| Not assessable | 1 (0.4) | 0% | |
| STAS | 1 | ||
| Absent | 154 (63.9) | 59.7% | |
| ≤1 mm | 55 (22.8) | 61.8% | |
| >1 mm | 32 (13.3) | 62.5% | |
| Budding | 0.04 | ||
| Zero | 58 (24) | 73.4% | |
| BD1 | 40 (16.6) | 53.3% | |
| BD2 | 29 (12) | 56.9% | |
| BD3 | 17 (7) | 50% | |
| Not assessable | 2 (0.8) | 100% | |
| Single cell invasion | 0.02 | ||
| Absent | 153 (63.5) | 66% | |
| Present | 88 (36.5) | 51.1% | |
| Cell nests group | 0.006 | ||
| 1 | 88 (36.5) | 52.3% | |
| ≥1–<5 | 97 (40.2) | 58.8% | |
| ≥5 | 55 (22.8) | 78.2% | |
| Not assessable | 1 (0.4) | 100% | |
| Nuclear Diameter | 0.7 | ||
| Large | 112 (46.5) | 61.6% | |
| Small | 129 (53.5) | 59.7% | |
| Mitoses | 0.3 | ||
| <20/2 mm2 | 211 (87.5) | 59.2% | |
| ≥20/2 mm2 | 29 (12) | 69% | |
| Not assessable | 1 (0.4) | 100% |
| STAS | Absent | ≤3 Alveoli | >3 Alveoli | Not Assessable | p |
|---|---|---|---|---|---|
| Sex | 0.2 * | ||||
| M | 143 (59.3) | 37 (15.3) | 39 (16.2) | 1 (0.4) | |
| F | 11 (4.6) | 7 (2.9) | 3 (1.2) | 0 (0) | |
| Age | 0.472 | ||||
| ≤65 years | 68 (28.2) | 16 (6.6) | 15 (6.2) | 0 (0) | |
| >65 years | 86 (35.7) | 28 (11.6) | 27 (11.2) | 1 (0.4) | |
| PS | 0.293 * | ||||
| 0 | 50 (20.7) | 18 (7.5) | 11 (4.6) | 0 (0) | |
| 1–2 | 43 (17.8) | 18 (7.5) | 19 (7.9) | 0 (0) | |
| 3–4 | 10 (4.1) | 1 (0.4) | 1 (0.4) | 0 (0) | |
| Unknown | 51 (21.2) | 7 (2.9) | 11 (4.6) | 1 (0.4) | |
| Localization | <0.001 | ||||
| Peripheral or intermediate | 57 (23.6) | 31 (12.9) | 25 (10.4) | 0 (0) | |
| Central | 97 (40.2) | 13 (5.4) | 17 (7.1) | 1 (0.4) | |
| pT | 0.414 * | ||||
| pT1 | 44 (18.3) | 19 (7.9) | 14 (5.8) | 1 (0.4) | |
| pT2 | 50 (20.7) | 13 (5.4) | 15 (6.2) | 0 (0) | |
| pT3 | 40 (16.6) | 7 (2.9) | 6 (2.5) | 0 (0) | |
| pT4 | 18 (7.5) | 5 (2.1) | 7 (2.9) | 0 (0) | |
| Not assessable | 2 (0) | 0 (0) | 0 (0) | 0 (0) | |
| pN | 0.762 | ||||
| pN0 | 90 (37.3) | 24 (10) | 28 (11.6) | 1 (0.4) | |
| pN1 | 42 (17.4) | 10 (4.1) | 8 (3.3) | 0 (0) | |
| pN2 | 19 (7.9) | 7 (2.9) | 6 (2.5) | 0 (0) | |
| pNx | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Pathological Stage | 0.039 | ||||
| I | 50 (20.7) | 20 (8.3) | 22 (9.1) | 1 (0.4) | |
| II | 54 (22.4) | 10 (4.1) | 6 (2.5) | 0 (0) | |
| III | 45 (18.7) | 11 (4.6) | 14 (5.8) | 0 (0) | |
| Not assessable | 5 (2.1) | 3 (1.2) | 0 (0) | 0 (0) | |
| Number of metastatic lymph nodes station | 0.662 | ||||
| 0 | 89 (36.9) | 24 (10) | 28 (11.6) | 1 (0.4) | |
| 1 | 45 (18.7) | 11 (4.6) | 8 (3.3) | 0 (0) | |
| ≥2 | 16 (6.6) | 6 (2.5) | 6 (2.5) | 0 (0) | |
| Unknown | 4 (1.7) | 3 (1.2) | 0 (0) | 0 (0) | |
| Pleural invasion | 0.402 * | ||||
| PL0 | 111 (46.1) | 34 (14.1) | 31 (12.9) | 1 (0.4) | |
| PL1 or PL2 | 32 (13.3) | 10 (4.1) | 10 (4.1) | 0 (0) | |
| PL3 | 11 (4.6) | 0 (0) | 1 (0.4) | 0 (0) | |
| Type | 0.079 | ||||
| Keratinizing | 68 (28.2) | 15 (6.2) | 10 (4.1) | 0 (0) | |
| Non-keratinizing | 78 (32.4) | 28 (11.6) | 28 (11.6) | 1 (0.4) | |
| Basaloïd | 8 (3.3) | 1 (0.4) | 4 (1.7) | 0 (0) | |
| Quality of the resection | 0.374 * | ||||
| R0 | 143 (59.3) | 43 (17.8) | 41 (17) | 1 (0.4) | |
| R1 | 11 (4.6) | 1 (0.4) | 1 (0.4) | 0 (0) | |
| Differenciation | 0.029 * | ||||
| Poorly | 41 (17) | 7 (2.9) | 17 (7.1) | 0 (0) | |
| Moderate | 74 (30.7) | 30 (12.4) | 20 (8.3) | 1 (0.4) | |
| Well | 39 (16.2) | 7 (2.9) | 5 (2.1) | 0 (0) | |
| Tumor to stroma ratio | 0.845 | ||||
| <30% | 56 (23.2) | 20 (8.3) | 17 (7.1) | 1 (0.4) | |
| ≥30% et <50% | 49 (20.3) | 11 (4.6) | 12 (5) | 0 (0) | |
| ≥50% | 49 (20.3) | 13 (5.4) | 13 (5.4) | 0 (0) | |
| Percentage of tumor necrosis | 0.004 * | ||||
| <30% | 86 (35.7) | 24 (10) | 35 (14.5) | 1 (0.4) | |
| ≥30% et <50% | 27 (11.2) | 11 (4.6) | 1 (0.4) | 0 (0) | |
| ≥50% | 41 (17) | 9 (3.7) | 6 (2.5) | 0 (0) | |
| Vascular and/or lymphatic emboli | 0.02 * | ||||
| Absent | 132 (54.8) | 32 (13.3) | 29 (12) | 1 (0.4) | |
| Present | 22 (9.1) | 12 (5) | 13 (5.4) | 0 (0) | |
| BD | 0.02 * | ||||
| Zero | 39 (16.2) | 21 (8.7) | 18 (7.5) | 1 (0.4) | |
| BD1 | 48 (19.9) | 14 (5.8) | 13 (3.7) | 0 (0) | |
| BD2 | 37 (15.3) | 5 (2.1) | 9 (3.7) | 0 (0) | |
| BD3 | 28 (11.6) | 4 (1.7) | 2 (0.8) | 0 (0) | |
| Not assessable | 2 (0.8) | 0 (0) | 0 (0) | 0 (0) | |
| Single cell invasion | 0.002 | ||||
| Absent | 85 (35.3) | 34 (14.1) | 33 (13.7) | 1 (0.4) | |
| Present | 69 (28.6) | 10 (4.1) | 9 (3.7) | 0 (0) | |
| Cell nests group | 0.005 | ||||
| 1 | 69 (28.6) | 10 (4.1) | 9 (3.7) | 0 (0) | |
| >1–≤5 | 56 (23.2) | 18 (7.5) | 22 (9.1) | 1 (0.4) | |
| >5 | 28 (11.6) | 16 (6.6) | 11 (4.6) | 0 (0) | |
| Not assessable | 1 (0.4) | 0 (0) | 0 (0) | 0 (0) | |
| Nuclear diameter | 0.832 | ||||
| Large | 74 (30.7) | 19 (7.9) | 19 (7.9) | 0 (0) | |
| Small | 80 (33.2) | 25 (10.4) | 23 (9.5) | 1 (0.4) | |
| Mitotic activity | 0.845 | ||||
| <20/2 mm2 | 134 (55.6) | 38 (15.8) | 38 (15.8) | 1 (0.4) | |
| ≥20/2 mm2 | 19 (7.9) | 6 (2.5) | 4 (1.7) | 0 (0) | |
| Not assessable | 1 (0.4) | 0 (0) | 0 (0) | 0 (0) |
| Variable | IC95% | HR | p (Pr > z) |
|---|---|---|---|
| PS | |||
| 1–2 | 0.64–1.88 | 1.09 | 0.745 |
| 3–4 | 1.06–4.92 | 2.29 | 0.034 |
| Location (peripheral or intermediate) | 0.92–2.07 | 1.38 | 0.119 |
| pT | |||
| pT2 | 1.02–3.25 | 1.82 | 0.042 |
| pT3 | 1.18–4 | 2.17 | 0.013 |
| pT4 | 1.90–6.91 | 3.62 | <0.001 |
| pN | |||
| pN1 | 0.68–1.89 | 1.13 | 0.630 |
| pN2 | 1.32–3.69 | 2.21 | 0.002 |
| Pathological Stage | |||
| II | 1.09–3.27 | 1.89 | 0.022 |
| III | 1.485– 4.21 | 2.50 | >0.001 |
| Number of metastatic lymph nodes station | |||
| 1 | 0.87–2.25 | 1.40 | 0.162 |
| ≥2 | 0.96–3.01 | 1.71 | 0.069 |
| Pleural invasion | |||
| PL1–PL2 | 1.19–2.96 | 1.88 | 0.007 |
| PL3 | 0.74–3.97 | 1.72 | 0.210 |
| Histopathological subtype | |||
| Not keratinizing | 0.64–1.47 | 0.97 | 0.905 |
| Basaloid | 0.02–0.87 | 0.12 | 0.036 |
| Percentage of tumor necrosis | |||
| ≥30% et <50% | 0.89–2.67 | 1.54 | 0.119 |
| ≥50% | 1.69–4.28 | 2.69 | <0.001 |
| Vascular and/or lymphatic emboli present | 1.29–3.16 | 2.01 | 0.002 |
| Single cell invasion present | 1.095–2.47 | 1.64 | 0.017 |
| STAS | |||
| ≤3 alveoli | 0.32–1.15 | 0.60 | 0.123 |
| >3 alveoli | 0.79–2.14 | 1.30 | 0.297 |
| BD | |||
| BD1 | 1.18–3.49 | 2.03 | 0.010 |
| BD2 | 0.97-.3.22 | 1.77 | 0.062 |
| BD3 | 1.13–4.15 | 2.16 | 0.020 |
| Cell nests group ≥ 5 | |||
| ≥1–<5 | 0.67–2.51 | 1.30 | 0.431 |
| 1 | 1.23–3.65 | 2.12 | 0.006 |
| Variable | IC95% | HR | p (Pr > z) |
|---|---|---|---|
| PS | |||
| 1–2 | 0.37–1.38 | 0.72 | 0.324 |
| 3–4 | 0.81–5.06 | 2.02 | 0.131 |
| Location (peripheral or intermediate) | 0.39–1.47 | 0.75 | 0.41 |
| pT | |||
| pT2 | 0.60–3.17 | 1.38 | 0.452 |
| pT3 | 0.30–3.34 | 1.01 | 0.991 |
| pT4 | 0.49–13.18 | 2.55 | 0.263 |
| pN | |||
| pN1 | 0.19–3.62 | 0.83 | 0.807 |
| pN2 | 0.66–21.78 | 3.80 | 0.133 |
| Pathological Stage | |||
| II | 0.80–5.46 | 2.09 | 0.134 |
| III | 0.12–4.62 | 0.75 | 0.758 |
| Number of metastatic lymph nodes station | |||
| 1 | 0.29–3.07 | 0.95 | 0.934 |
| ≥2 | NA | NA | NA |
| Pleural invasion | |||
| PL1-PL2 | 0.73–3.1 | 1.51 | 0.263 |
| PL3 | 0.18–3.62 | 0.80 | 0.778 |
| Histopathological subtype | |||
| Not keratinizing | 0.47–1.66 | 0.88 | 0.698 |
| Basaloid | 0.02–1.38 | 0.018 | 0.098 |
| Percentage of tumor necrosis | |||
| ≥30% et <50% | 0.57–3.21 | 1.35 | 0.495 |
| ≥50% | 0.79–3.41 | 1.64 | 0.186 |
| Vascular and/or lymphatic emboli present | 0.64–2.89 | 1.36 | 0.418 |
| Single cell invasion present | 0.56–7.37 | 2.03 | 0.358 |
| STAS | |||
| ≤3 alveoli | 0.23–1.36 | 0.55 | 0.2 |
| >3 alveoli | 1.18–6.33 | 2.74 | 0.018 |
| BD | |||
| BD1 | 0.71–4.96 | 1.87 | 0.207 |
| BD2 | 0.31–3.04 | 0.97 | 0.968 |
| BD3 | 0.37–4.3 | 1.26 | 0.71 |
| Cell nests group ≥ 5 | |||
| ≥1–<5 | 0.44–4.50 | 1.41 | 0.565 |
| 1 | NA | NA | NA |
| Variable | n (%) | 5-Year Survival Rate | p (Log-Rank Test) |
|---|---|---|---|
| Age | 0.47 | ||
| ≤65 years | 60 (36.8) | 63.3% | |
| >65 years | 103 (63.2) | 70.9% | |
| PS | |||
| 0 | 56 (34.4) | 46.4% | 0.20 |
| 1–2 | 54 (33.1) | 48.2% | |
| 3–4 | 9 (5.5) | 11.1% | |
| Unknown | 44 (27) | 45.4% | |
| pT | 0.006 | ||
| pT1 | 71 (45.6) | 60.6% | |
| pT2 | 67 (41.1) | 34.3 | |
| pT3 | 25 (15.3) | 28% | |
| pN | 0.72 | ||
| pN0 | 130 (79.7) | 48.5% | |
| pN1 | 33 (20.2) | 30.3% | |
| Pathological Stage | 0.019 | ||
| I | 91 (55.8) | 56% | |
| II | 70 (42.9) | 31.4% | |
| Pleural invasion | 0.23 | ||
| PL0 | 127 (77.9) | 46.4% | |
| PL1 or PL2 | 29 (17.8) | 41.4% | |
| PL 3 | 7 (4.3) | 28.6% | |
| Percentage of tumor necrosis | 0.009 | ||
| <30% | 104 (63.8) | 61.5% | |
| ≥30% et <50% | 27 (16.6) | 11.% | |
| ≥50% | 32 (19.6) | 18.7% | |
| Vascular and/or lymphatic emboli | 0.15 | ||
| Absent | 135 (82.8) | 49.2% | |
| Present | 28 (17.2) | 28.6% | |
| STAS | 0.22 | ||
| Absent | 104 (63.8) | 42.3% | |
| ≤3 alveoli | 30 (18.4) | 50% | |
| >3 alveoli | 28 (17.2) | 50% | |
| Not assessable | |||
| STAS | 0.97 | ||
| Absent | 104 (63.8) | 42.3% | |
| ≤1 mm | 37 (22.7) | 45.9% | |
| >1 mm | 22 (13.5) | 54.5% | |
| Budding | 0.061 | ||
| Zero | 56 (34.4) | 57.1% | |
| BD1 | 57 (35) | 36.8% | |
| BD2 | 31 (19) | 38.7% | |
| BD3 | 17 (10.4) | 35.3% | |
| Not assessable | 6 (3.7) | 33.3% | |
| Single cell invasion | 0.11 | ||
| Absent | 112 (68.7) | 52.7% | |
| Present | 51 (31.3) | 27.4% | |
| Cell nests group | 0.062 | ||
| 1 | 51 (31.3) | 27.4% | |
| ≥1–<5 | 72 (44.2) | 45.8% | |
| ≥5 | 39 (23.9) | 62.3% | |
| Not assessable | 1 (0.6) | 100% | |
| Mitoses | 0.53 | ||
| <20/2 mm2 | 138 (64.7) | 43.5% | |
| ≥20/2 mm2 | 24 (14.7) | 50% | |
| Not assessable | 1 (0.6) | 100% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dagher, S.; Sulaiman, A.; Bayle-Bleuez, S.; Tissot, C.; Grangeon-Vincent, V.; Laville, D.; Fournel, P.; Tiffet, O.; Forest, F. Spread Through Air Spaces (STAS) Is an Independent Prognostic Factor in Resected Lung Squamous Cell Carcinoma. Cancers 2022, 14, 2281. https://doi.org/10.3390/cancers14092281
Dagher S, Sulaiman A, Bayle-Bleuez S, Tissot C, Grangeon-Vincent V, Laville D, Fournel P, Tiffet O, Forest F. Spread Through Air Spaces (STAS) Is an Independent Prognostic Factor in Resected Lung Squamous Cell Carcinoma. Cancers. 2022; 14(9):2281. https://doi.org/10.3390/cancers14092281
Chicago/Turabian StyleDagher, Sami, Abdulrazzaq Sulaiman, Sophie Bayle-Bleuez, Claire Tissot, Valérie Grangeon-Vincent, David Laville, Pierre Fournel, Olivier Tiffet, and Fabien Forest. 2022. "Spread Through Air Spaces (STAS) Is an Independent Prognostic Factor in Resected Lung Squamous Cell Carcinoma" Cancers 14, no. 9: 2281. https://doi.org/10.3390/cancers14092281