
Adjusted CT Image-Based Radiomic Features Combined with Immune Genomic Expression Achieve Accurate Prognostic Classification and Identification of Therapeutic Targets in Stage III Colorectal Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Image Acquisition and Imaging Texture Analysis
2.3. Radiomics Workflow and Feature Extraction
2.4. Tumor Microenvironment-Based RNA Immune Response Gene Sequencing
2.5. Statistical Analysis for Clinical Data
2.6. CATCH Model
3. Results
3.1. Patient Characteristics
3.2. Identification of Genes Influencing Recurrence and Performance of the CATCH Model
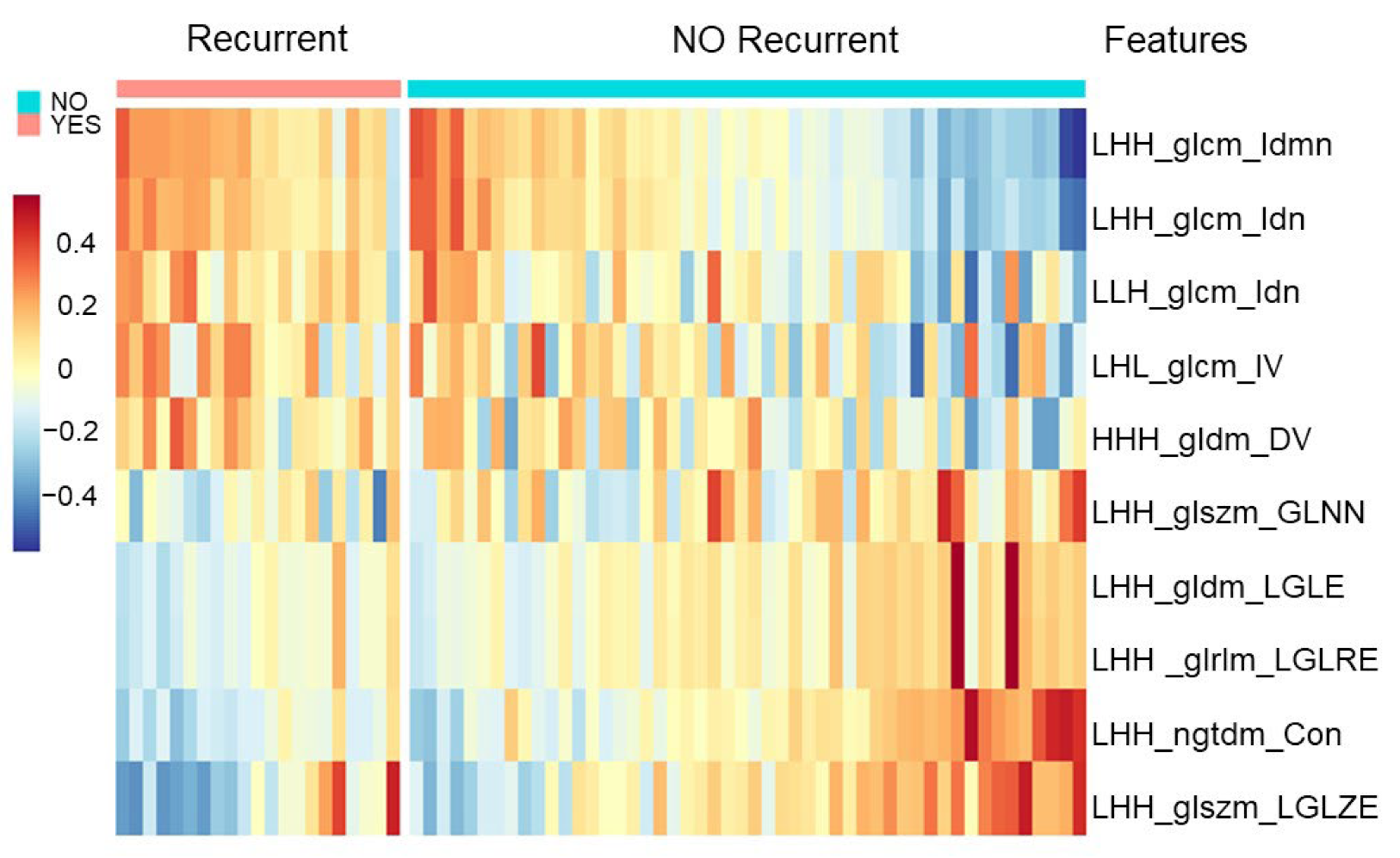
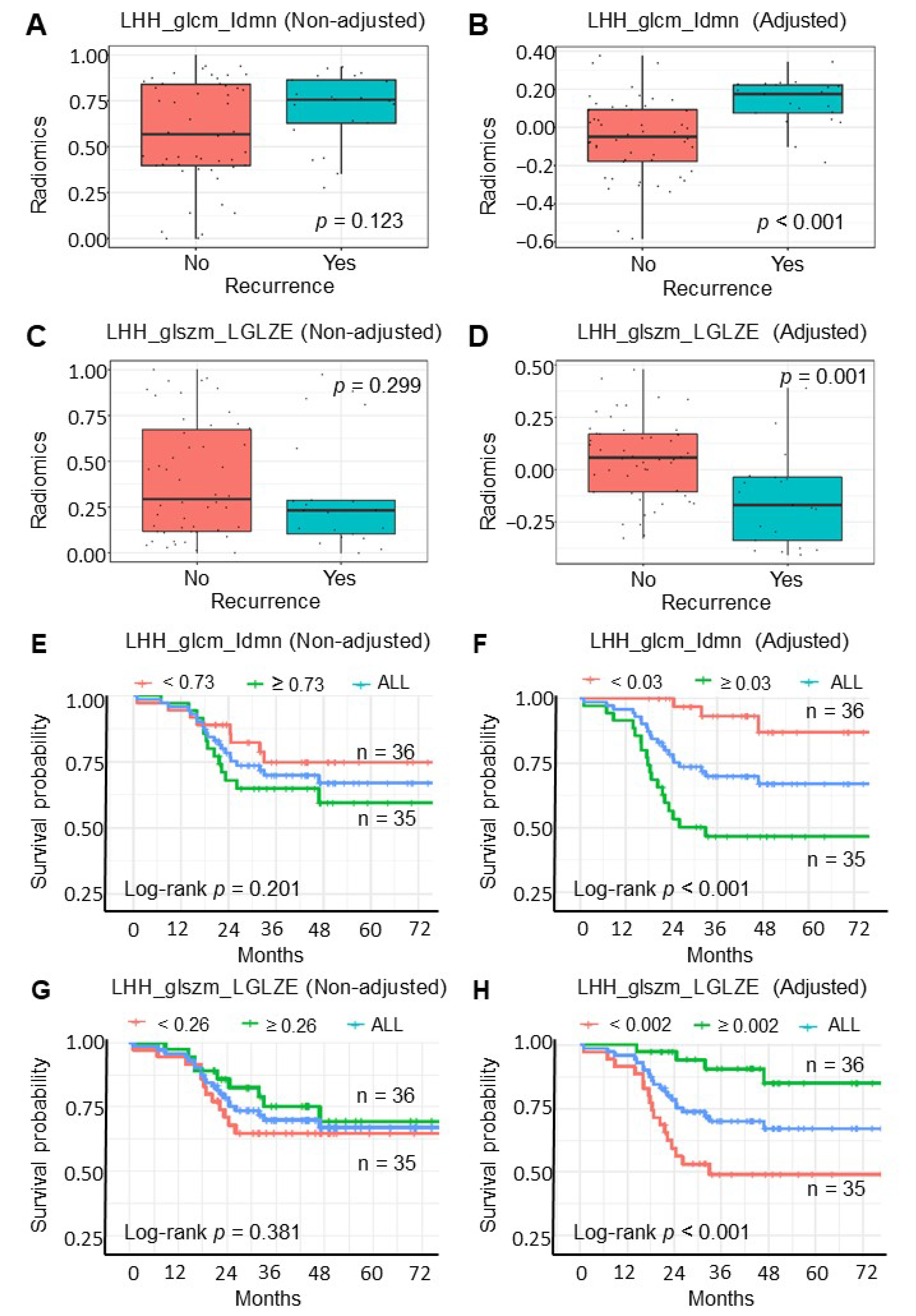
3.3. Adjusted Radiomic Features Obtained from CATCH Model for Cancer Recurrence
3.4. Adjusted Radiomic Features Impact Clinical Outcome
3.5. Correlation between Adjusted Radiomic Features and Immune Gene Expression
3.6. PECAM1 as a Therapeutic Target Identified by Adjusted Radiomic Features in Recurrent Colorectal Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUC | area under the curve |
| CATCH | covariate-adjusted tensor classification in the high-dimension |
| CRC | colorectal cancer |
| CT | computed tomography |
| CRC | colorectal cancer |
| DEGs | differentially expressed genes |
| DICOM | Digital Imaging and Communications in Medicine |
| DV | dependence variance |
| FOLFOX | leucovorin (folinic acid), fluorouracil, and oxaliplatin |
| IV | inverse variance |
| LDA | linear discriminant analysis |
| LGLZE | low gray level zone emphasis |
| mFOLFOX7 | modified FOLFOX |
| MMR | mismatch repair |
| NCCN | National Comprehensive Cancer Network |
| NCKUH | National Cheng Kung University Hospital |
| PACS | picture archiving and communication system |
| RF | random forest |
| RFS | recurrence-free survival |
| TME | tumor microenvironment |
| VOI | volume of interest |
References
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.; Cui, X.; Liu, C.; Li, X.; Zheng, L.; Song, Q.; Qi, J.; Ma, W.; Ye, Z. CT-based radiomics signature: A potential biomarker for predicting postoperative recurrence risk in stage II colorectal cancer. Front. Oncol. 2021, 11, 644933. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Q.; Liang, C.H.; He, L.; Tian, J.; Liang, C.S.; Chen, X.; Ma, Z.L.; Liu, Z.Y. Development and validation of a radiomics nomogram for preoperative prediction of lymph node metastasis in colorectal cancer. J. Clin. Oncol. 2016, 34, 2157–2164. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.; Huang, Y.; He, L.; Chen, X.; Ma, Z.; Dong, D.; Tian, J.; Liang, C.; Liu, Z. The development and validation of a CT-based radiomics signature for the preoperative discrimination of stage I-II and stage III-IV colorectal cancer. Oncotarget 2016, 7, 31401–31412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, W.; Mo, S.; Han, L.; Xiang, W.; Li, M.; Wang, R.; Tong, T.; Cai, G. Prognostic and predictive value of radiomics signatures in stage I-III colon cancer. Clin. Transl. Med. 2020, 10, 288–293. [Google Scholar] [CrossRef]
- Na, K.J.; Choi, H. Tumor metabolic features identified by (18)F-FDG PET correlate with gene networks of immune cell microenvironment in head and neck cancer. J. Nucl. Med. 2018, 59, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Zhang, L.; Mo, X.; You, J.; Chen, L.; Fang, J.; Wang, F.; Jin, Z.; Zhang, B.; Zhang, S. Current status and quality of radiomic studies for predicting immunotherapy response and outcome in patients with non-small cell lung cancer: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 49, 345–360. [Google Scholar] [CrossRef]
- Khalifa, N.E.M.; Taha, M.H.N.; Ali, D.E.; Slowik, A.; Hassanien, A.E. Artificial intelligence technique for gene expression by tumor RNA-Seq data: A novel optimized deep learning approach. IEEE Access 2020, 8, 22874–22883. [Google Scholar] [CrossRef]
- Pan, Y.; Mai, Q.; Zhang, X. Covariate-adjusted tensor classification in high dimensions. J. Am. Stat. Assoc. 2019, 114, 1305–1319. [Google Scholar] [CrossRef] [Green Version]
- Shaath, H.; Toor, S.M.; Nair, V.S.; Elkord, E.; Alajez, N.M. Transcriptomic analyses revealed systemic alterations in gene expression in circulation and tumor microenvironment of colorectal cancer patients. Cancers 2019, 11, 1994. [Google Scholar] [CrossRef] [Green Version]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negreros-Osuna, A.A.; Parakh, A.; Corcoran, R.B.; Pourvaziri, A.; Kambadakone, A.; Ryan, D.P.; Sahani, D.V. Radiomics texture features in advanced colorectal cancer: Correlation with BRAF mutation and 5-year overall survival. Radiol. Imaging Cancer 2020, 2, e190084. [Google Scholar] [CrossRef] [PubMed]
- González-Castro, V.; Cernadas, E.; Huelga, E.; Fernández-Delgado, M.; Porto, J.; Antunez, J.R.; Souto-Bayarri, M. CT Radiomics in colorectal cancer: Detection of KRAS mutation using texture analysis and machine learning. Appl. Sci. 2020, 10, 6214. [Google Scholar] [CrossRef]
- Badic, B.; Hatt, M.; Durand, S.; Jossic-Corcos, C.L.; Simon, B.; Visvikis, D.; Corcos, L. Radiogenomics-based cancer prognosis in colorectal cancer. Sci. Rep. 2019, 9, 9743. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Arshad, M.; Thornton, A.; Avesani, G.; Cunnea, P.; Curry, E.; Kanavati, F.; Liang, J.; Nixon, K.; Williams, S.T.; et al. A mathematical-descriptor of tumor-mesoscopic-structure from computed-tomography images annotates prognostic- and molecular-phenotypes of epithelial ovarian cancer. Nat. Commun. 2019, 10, 764. [Google Scholar] [CrossRef]
- Cao, G.; O’Brien, C.D.; Zhou, Z.; Sanders, S.M.; Greenbaum, J.N.; Makrigiannakis, A.; DeLisser, H.M. Involvement of human PECAM-1 in angiogenesis and in vitro endothelial cell migration. Am. J. Physiol. Cell Physiol. 2002, 282, C1181–C1190. [Google Scholar] [CrossRef]
- Engel, C.J.; Bennett, S.T.; Chambers, A.F.; Doig, G.S.; Kerkvliet, N.; O’Malley, F.P. Tumor angiogenesis predicts recurrence in invasive colorectal cancer when controlled for Dukes staging. Am. J. Surg. Pathol. 1996, 20, 1260–1265. [Google Scholar] [CrossRef]
- Rajaganeshan, R.; Prasad, R.; Guillou, P.J.; Chalmers, C.R.; Scott, N.; Sarkar, R.; Poston, G.; Jayne, D.G. The influence of invasive growth pattern and microvessel density on prognosis in colorectal cancer and colorectal liver metastases. Br. J. Cancer 2007, 96, 1112–1117. [Google Scholar] [CrossRef] [Green Version]
- Mohamed, S.Y.; Mohammed, H.L.; Ibrahim, H.M.; Mohamed, E.M.; Salah, M. Role of VEGF, CD105, and CD31 in the prognosis of colorectal cancer cases. J. Gastrointest. Cancer 2019, 50, 23–34. [Google Scholar] [CrossRef]
- Zhu, X.; Zhou, G.; Ni, P.; Jiang, X.; Huang, H.; Wu, J.; Shi, X.; Jiang, X.; Liu, J. CD31 and D2-40 contribute to peritoneal metastasis of colorectal cancer by promoting epithelial-mesenchymal transition. Gut Liver 2021, 15, 273–283. [Google Scholar] [CrossRef]
- Delisser, H.M. Targeting PECAM-1 for anti-cancer therapy. Cancer Biol. 2007, 6, 121–122. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2001, 19, 329–359. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority oversampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Fortin, J.P.; Parker, D.; Tunç, B.; Watanabe, T.; Elliott, M.A.; Ruparel, K.; Roalf, D.R.; Satterthwaite, T.D.; Gur, R.C.; Gur, R.E.; et al. Harmonization of multi-site diffusion tensor imaging data. NeuroImage 2017, 161, 149–170. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | Accuracy | Sensitivity | Specificity | F1 score | AUC |
|---|---|---|---|---|---|
| Random forest | 0.68 | 0.16 | 0.83 | 0.24 | 0.46 |
| LDA | 0.64 | 0.32 | 0.78 | 0.35 | 0.55 |
| CATCH | 0.60 | 0.66 | 0.48 | 0.69 | 0.56 |
| Features | Coefficient |
|---|---|
| wavelet LHH_glcm_Idmn | 6.57 |
| wavelet LHH_glcm_Idn | 4.45 |
| wavelet LLH_glcm_Idn | 0.69 |
| wavelet LHL_glcm_InverseVariance (IV) | 0.07 |
| wavelet HHH_gldm_DependenceVariance (DV) | 0.06 |
| wavelet LHH_glszm_GrayLevelNonUniformityNormalized (GLNN) | −0.11 |
| wavelet LHH_gldm_LowGrayLevelEmphasis (LGLE) | −0.20 |
| wavelet LHH_glrlm_LowGrayLevelRunEmphasis (LGLRE) | −0.73 |
| wavelet LHH_ngtdm_Contrast | −5.22 |
| wavelet LHH_glszm_LowGrayLevelZoneEmphasis (LGLZE) | −5.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-C.; Tsai, Y.-S.; Li, C.-I.; Chan, R.-H.; Yeh, Y.-M.; Chen, P.-C.; Shen, M.-R.; Lin, P.-C. Adjusted CT Image-Based Radiomic Features Combined with Immune Genomic Expression Achieve Accurate Prognostic Classification and Identification of Therapeutic Targets in Stage III Colorectal Cancer. Cancers 2022, 14, 1895. https://doi.org/10.3390/cancers14081895
Huang Y-C, Tsai Y-S, Li C-I, Chan R-H, Yeh Y-M, Chen P-C, Shen M-R, Lin P-C. Adjusted CT Image-Based Radiomic Features Combined with Immune Genomic Expression Achieve Accurate Prognostic Classification and Identification of Therapeutic Targets in Stage III Colorectal Cancer. Cancers. 2022; 14(8):1895. https://doi.org/10.3390/cancers14081895
Chicago/Turabian StyleHuang, Yi-Ching, Yi-Shan Tsai, Chung-I Li, Ren-Hao Chan, Yu-Min Yeh, Po-Chuan Chen, Meng-Ru Shen, and Peng-Chan Lin. 2022. "Adjusted CT Image-Based Radiomic Features Combined with Immune Genomic Expression Achieve Accurate Prognostic Classification and Identification of Therapeutic Targets in Stage III Colorectal Cancer" Cancers 14, no. 8: 1895. https://doi.org/10.3390/cancers14081895