
Identification of CT Imaging Phenotypes of Colorectal Liver Metastases from Radiomics Signatures—Towards Assessment of Interlesional Tumor Heterogeneity

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
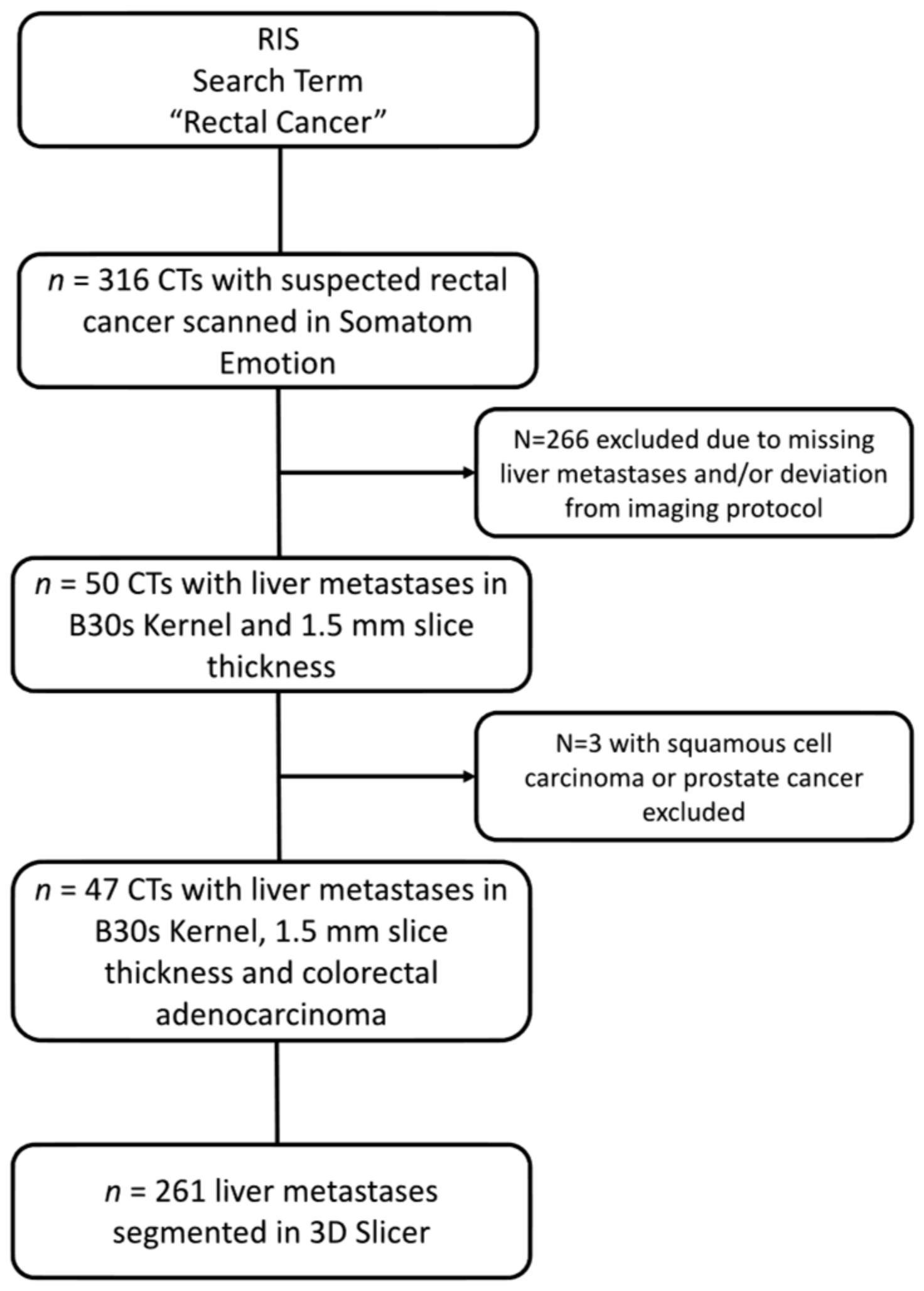
2.1. Patient Collective and Imaging Protocols
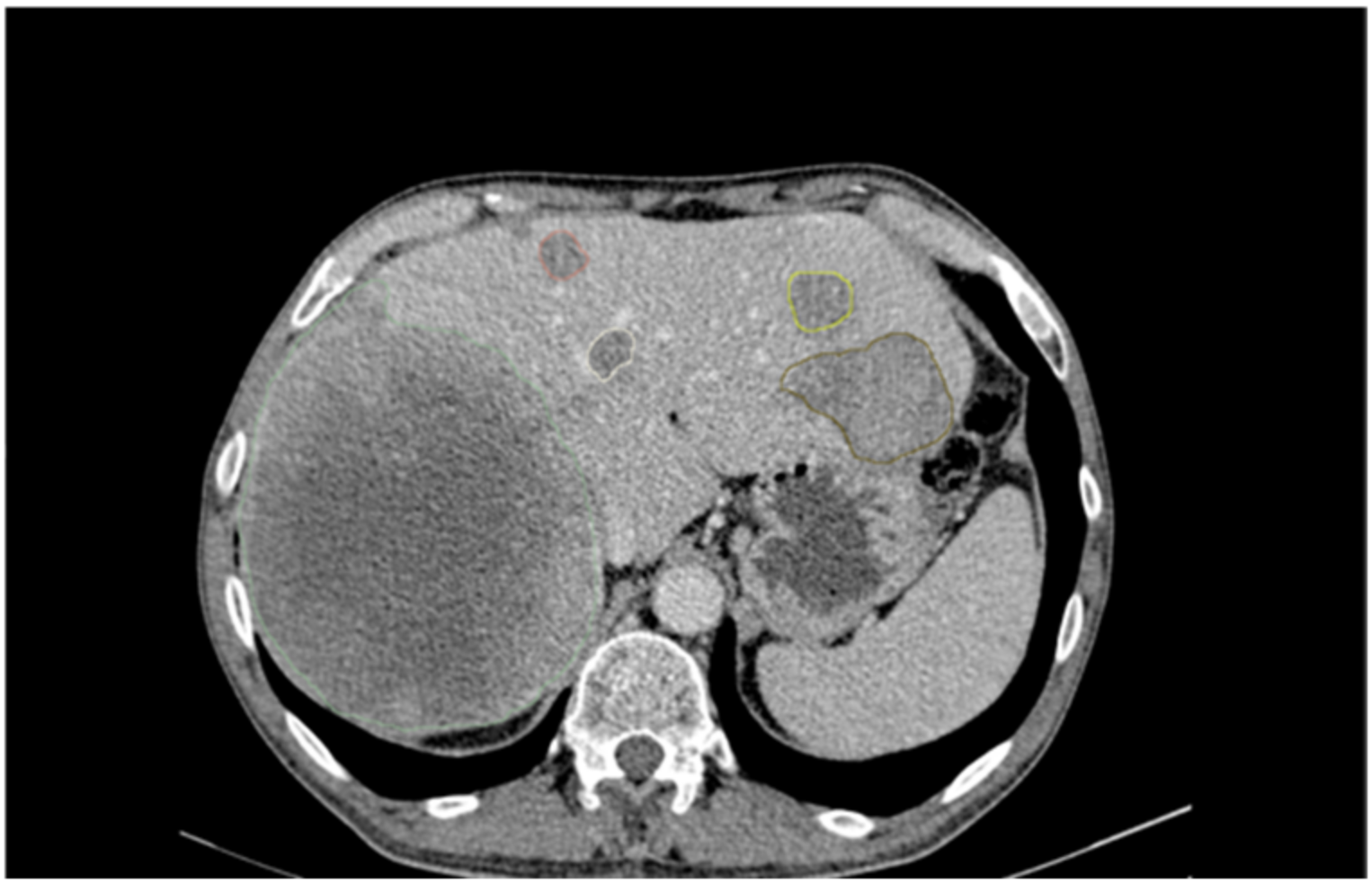
2.2. Image Analysis and Segmentation
2.3. Radiomics Feature Extraction
2.4. Clustering, Feature Selection, and Statistical Analysis
2.5. Cluster Analysis
3. Results
3.1. Patient Collective
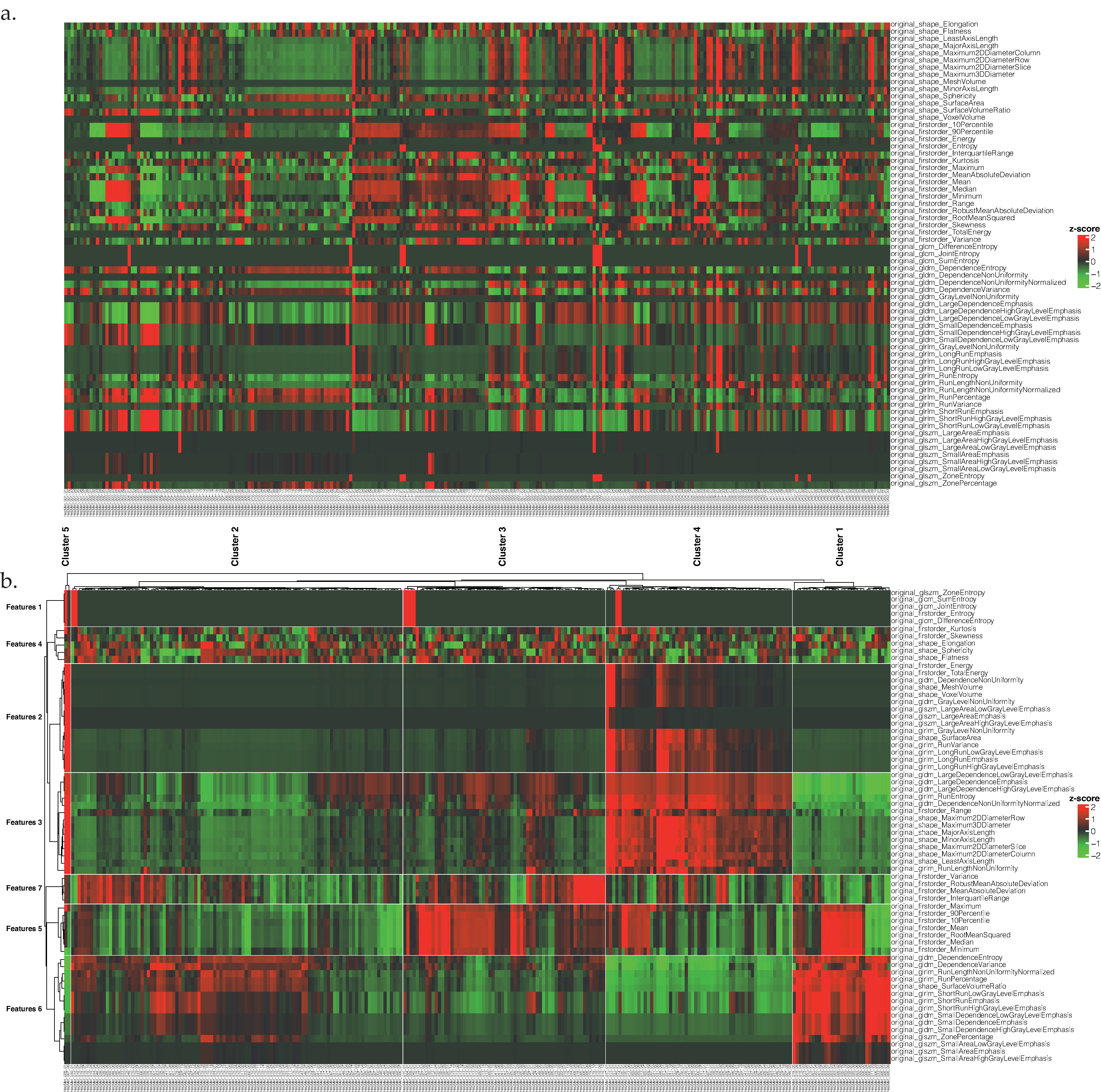
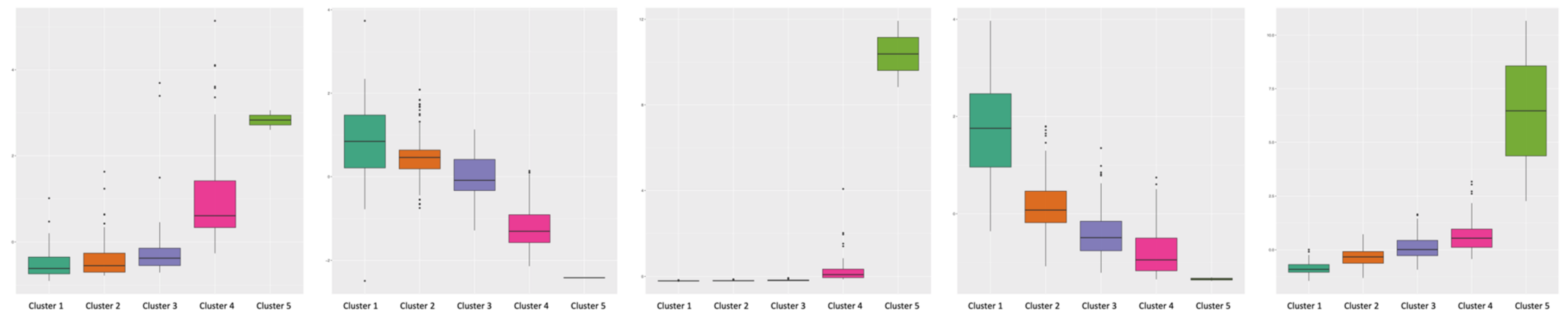
3.2. Cluster Analysis
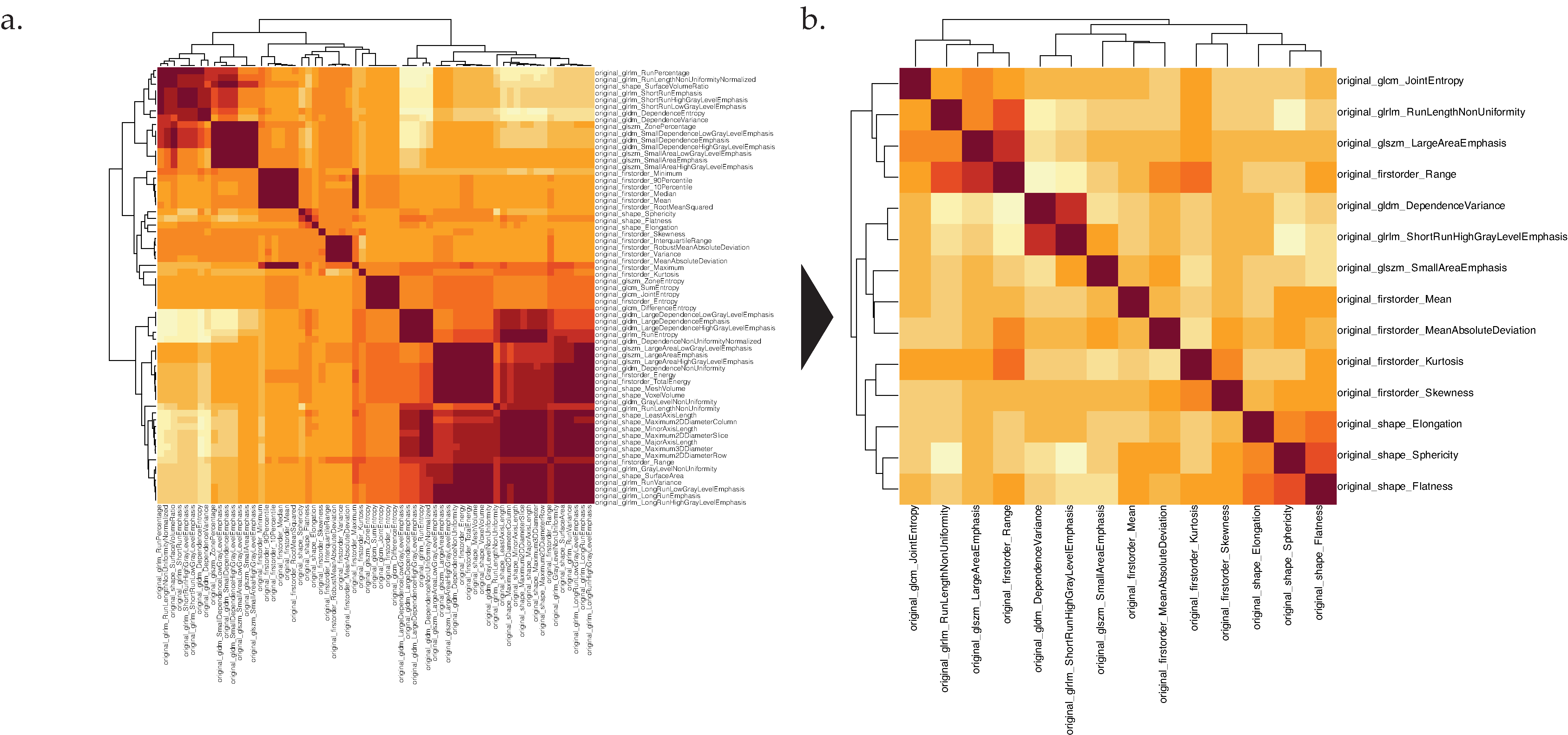
3.3. Reduction of Feature Redundancy
3.4. Feature Importance Assessment
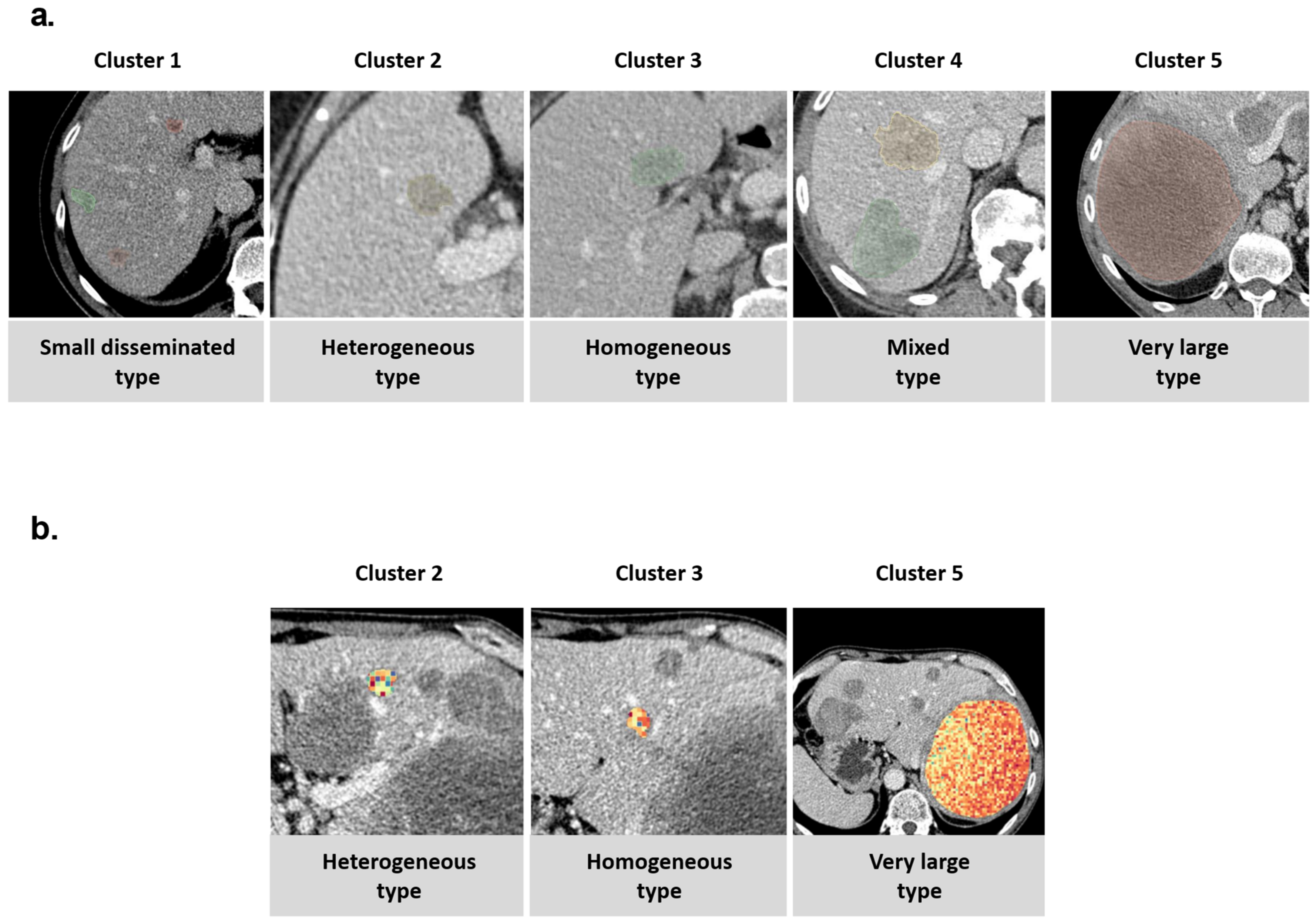
3.5. Visual Cluster Analysis
3.6. Association of Clusters with Clinical Patterns and Parameters
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Cancer of the Colon and Rectum—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/colorect.html (accessed on 22 December 2021).
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aranda Aguilar, E.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO Consensus Guidelines for the Management of Patients with Metastatic Colorectal Cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.H.; Lee, J.M.; Chang, W.; Kang, H.; Bandos, A.; Lim, H.; Kang, S.Y.; Kang, K.W.; Ryoo, S.-B.; Jeong, S.-Y.; et al. Initial M Staging of Rectal Cancer: FDG PET/MRI with a Hepatocyte-Specific Contrast Agent versus Contrast-Enhanced CT. Radiology 2020, 294, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Dagogo-Jack, I.; Shaw, A.T. Tumour Heterogeneity and Resistance to Cancer Therapies. Nat. Rev. Clin. Oncol. 2018, 15, 81–94. [Google Scholar] [CrossRef]
- Russo, M.; Siravegna, G.; Blaszkowsky, L.S.; Corti, G.; Crisafulli, G.; Ahronian, L.G.; Mussolin, B.; Kwak, E.L.; Buscarino, M.; Lazzari, L.; et al. Tumor Heterogeneity and Lesion-Specific Response to Targeted Therapy in Colorectal Cancer. Cancer Discov. 2016, 6, 147–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Cancer Genome Atlas Network. Comprehensive Molecular Characterization of Human Colon and Rectal Cancer. Nature 2012, 487, 330–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting More Information from Medical Images Using Advanced Feature Analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Mühlberg, A.; Holch, J.W.; Heinemann, V.; Huber, T.; Moltz, J.; Maurus, S.; Jäger, N.; Liu, L.; Froelich, M.F.; Katzmann, A.; et al. The Relevance of CT-Based Geometric and Radiomics Analysis of Whole Liver Tumor Burden to Predict Survival of Patients with Metastatic Colorectal Cancer. Eur. Radiol. 2021, 31, 834–846. [Google Scholar] [CrossRef]
- Sala, E.; Mema, E.; Himoto, Y.; Veeraraghavan, H.; Brenton, J.D.; Snyder, A.; Weigelt, B.; Vargas, H.A. Unravelling Tumour Heterogeneity Using Next-Generation Imaging: Radiomics, Radiogenomics, and Habitat Imaging. Clin. Radiol. 2017, 72, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Park, B.W.; Kim, J.K.; Heo, C.; Park, K.J. Reliability of CT Radiomic Features Reflecting Tumour Heterogeneity According to Image Quality and Image Processing Parameters. Sci. Rep. 2020, 10, 3852. [Google Scholar] [CrossRef]
- Goto, K.; Honda, Y.; Ikeda, K.; Takemoto, K.; Higaki, T.; Hayashi, T.; Kobatake, K.; Nakamura, Y.; Sekino, Y.; Inoue, S.; et al. Tumor Heterogeneity Evaluated by Computed Tomography Detects Muscle-Invasive Upper Tract Urothelial Carcinoma That Is Associated with Inflammatory Tumor Microenvironment. Sci. Rep. 2021, 11, 14251. [Google Scholar] [CrossRef]
- Shi, R.; Chen, W.; Yang, B.; Qu, J.; Cheng, Y.; Zhu, Z.; Gao, Y.; Wang, Q.; Liu, Y.; Li, Z.; et al. Prediction of KRAS, NRAS and BRAF Status in Colorectal Cancer Patients with Liver Metastasis Using a Deep Artificial Neural Network Based on Radiomics and Semantic Features. Am. J. Cancer Res. 2020, 10, 4513. [Google Scholar]
- Dercle, L.; Lu, L.; Schwartz, L.H.; Qian, M.; Tejpar, S.; Eggleton, P.; Zhao, B.; Piessevaux, H. Radiomics Response Signature for Identification of Metastatic Colorectal Cancer Sensitive to Therapies Targeting EGFR Pathway. JNCI J. Natl. Cancer Inst. 2020, 112, 902–912. [Google Scholar] [CrossRef]
- Siravegna, G.; Lazzari, L.; Crisafulli, G.; Sartore-Bianchi, A.; Mussolin, B.; Cassingena, A.; Martino, C.; Lanman, R.B.; Nagy, R.J.; Fairclough, S.; et al. Radiologic and Genomic Evolution of Individual Metastases during HER2 Blockade in Colorectal Cancer. Cancer Cell 2018, 34, 148–162.e7. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding Tumour Phenotype by Noninvasive Imaging Using a Quantitative Radiomics Approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Lafata, K.J.; Corradetti, M.N.; Gao, J.; Jacobs, C.D.; Weng, J.; Chang, Y.; Wang, C.; Hatch, A.; Xanthopoulos, E.; Jones, G.; et al. Radiogenomic Analysis of Locally Advanced Lung Cancer Based on CT Imaging and Intratreatment Changes in Cell-Free DNA. Radiol. Imaging Cancer 2021, 3, e200157. [Google Scholar] [CrossRef]
- Starmans, M.P.A.; Buisman, F.E.; Renckens, M.; Willemssen, F.E.J.A.; van der Voort, S.R.; Groot Koerkamp, B.; Grünhagen, D.J.; Niessen, W.J.; Vermeulen, P.B.; Verhoef, C.; et al. Distinguishing Pure Histopathological Growth Patterns of Colorectal Liver Metastases on CT Using Deep Learning and Radiomics: A Pilot Study. Clin. Exp. Metastasis 2021, 38, 483–494. [Google Scholar] [CrossRef]
- Huang, X.; Cheng, Z.; Huang, Y.; Liang, C.; He, L.; Ma, Z.; Chen, X.; Wu, X.; Li, Y.; Liang, C.; et al. CT-Based Radiomics Signature to Discriminate High-Grade From Low-Grade Colorectal Adenocarcinoma. Acad. Radiol. 2018, 25, 1285–1297. [Google Scholar] [CrossRef]
- Yang, L.; Dong, D.; Fang, M.; Zhu, Y.; Zang, Y.; Liu, Z.; Zhang, H.; Ying, J.; Zhao, X.; Tian, J. Can CT-Based Radiomics Signature Predict KRAS/NRAS/BRAF Mutations in Colorectal Cancer? Eur. Radiol. 2018, 28, 2058–2067. [Google Scholar] [CrossRef]
- Bodalal, Z.; Trebeschi, S.; Nguyen-Kim, T.D.L.; Schats, W.; Beets-Tan, R. Radiogenomics: Bridging Imaging and Genomics. Abdom. Radiol. 2019, 44, 1960–1984. [Google Scholar] [CrossRef] [Green Version]
- Froelich, M.F.; Petersen, E.L.; Heinemann, V.; Nörenberg, D.; Hesse, N.; Gesenhues, A.B.; Modest, D.P.; Sommer, W.H.; Hofmann, F.O.; Stintzing, S.; et al. Impact of Size and Location of Metastases on Early Tumor Shrinkage and Depth of Response in Patients With Metastatic Colorectal Cancer: Subgroup Findings of the Randomized, Open-Label Phase 3 Trial FIRE-3/AIO KRK-0306. Clin. Colorectal Cancer 2020, 19, 291–300.e5. [Google Scholar] [CrossRef] [PubMed]
- Staal, F.C.R.; van der Reijd, D.J.; Taghavi, M.; Lambregts, D.M.J.; Beets-Tan, R.G.H.; Maas, M. Radiomics for the Prediction of Treatment Outcome and Survival in Patients With Colorectal Cancer: A Systematic Review. Clin. Colorectal Cancer 2021, 20, 52–71. [Google Scholar] [CrossRef] [PubMed]
- Lennartz, S.; O’Shea, A.; Parakh, A.; Persigehl, T.; Baessler, B.; Kambadakone, A. Robustness of Dual-Energy CT-Derived Radiomic Features across Three Different Scanner Types. Eur. Radiol. 2022, 32, 1959–1970. [Google Scholar] [CrossRef]
- Jensen, L.J.; Kim, D.; Elgeti, T.; Steffen, I.G.; Hamm, B.; Nagel, S.N. Stability of Radiomic Features across Different Region of Interest Sizes—A CT and MR Phantom Study. Tomography 2021, 7, 238–252. [Google Scholar] [CrossRef]
- Zhao, B. Understanding Sources of Variation to Improve the Reproducibility of Radiomics. Front. Oncol. 2021, 11, 633176. [Google Scholar] [CrossRef] [PubMed]
- Korte, J.C.; Cardenas, C.; Hardcastle, N.; Kron, T.; Wang, J.; Bahig, H.; Elgohari, B.; Ger, R.; Court, L.; Fuller, C.D.; et al. Radiomics Feature Stability of Open-Source Software Evaluated on Apparent Diffusion Coefficient Maps in Head and Neck Cancer. Sci. Rep. 2021, 11, 17633. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-Based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [Green Version]
- Zhao, B.; Tan, Y.; Tsai, W.-Y.; Qi, J.; Xie, C.; Lu, L.; Schwartz, L.H. Reproducibility of Radiomics for Deciphering Tumor Phenotype with Imaging. Sci. Rep. 2016, 6, 23428. [Google Scholar] [CrossRef] [Green Version]
- Van Timmeren, J.E.; Leijenaar, R.T.H.; van Elmpt, W.; Wang, J.; Zhang, Z.; Dekker, A.; Lambin, P. Test–Retest Data for Radiomics Feature Stability Analysis: Generalizable or Study-Specific? Tomography 2016, 2, 361–365. [Google Scholar] [CrossRef]
- Yang, L.; Gu, D.; Wei, J.; Yang, C.; Rao, S.; Wang, W.; Chen, C.; Ding, Y.; Tian, J.; Zeng, M. A Radiomics Nomogram for Preoperative Prediction of Microvascular Invasion in Hepatocellular Carcinoma. Liver Cancer 2019, 8, 373–386. [Google Scholar] [CrossRef]
- Michallek, F.; Genske, U.; Niehues, S.M.; Hamm, B.; Jahnke, P. Deep Learning Reconstruction Improves Radiomics Feature Stability and Discriminative Power in Abdominal CT Imaging: A Phantom Study. Eur. Radiol. 2022. [Google Scholar] [CrossRef]
- Kaissis, G.A.; Ziegelmayer, S.; Lohöfer, F.K.; Harder, F.N.; Jungmann, F.; Sasse, D.; Muckenhuber, A.; Yen, H.-Y.; Steiger, K.; Siveke, J.; et al. Image-Based Molecular Phenotyping of Pancreatic Ductal Adenocarcinoma. J. Clin. Med. 2020, 9, 724. [Google Scholar] [CrossRef] [Green Version]
- Rajendran, K.; Petersilka, M.; Henning, A.; Shanblatt, E.R.; Schmidt, B.; Flohr, T.G.; Ferrero, A.; Baffour, F.; Diehn, F.E.; Yu, L.; et al. First Clinical Photon-Counting Detector CT System: Technical Evaluation. Radiology 2021, 303, 130–138. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | |
|---|---|---|
| n | 47 | |
| Age at CT (median [IQR]) | 65.79 [56.99, 74.62] | |
| Sex (%) | ||
| F | 17 (36.2%) | |
| M | 30 (63.8%) | |
| Tumor Location (%) | ||
| Colon | 1 (2.1%) | |
| Colon asc | 2 (4.3%) | |
| Colon desc | 3 (6.4%) | |
| Colon tran. | 3 (6.4%) | |
| Rectum | 29 (61.7%) | |
| Rectosigmoid Junction | 2 (4.3%) | |
| Sigma | 7 (14.9%) | |
| T-Stage (%) | ||
| T1 | 2 (4.3%) | |
| T2 | 4 (8.5%) | |
| T3 | 24 (51.1%) | |
| T4 | 15 (31.9%) | |
| Tx | 2 (4.3%) | |
| N-Stage (%) | ||
| N0 | 8 (17.0%) | |
| N1 | 18 (38.3%) | |
| N2 | 20 (42.6%) | |
| Nx | 1 (2.1%) | |
| M-Stage (%) | ||
| M1 | 47 (100.0%) | |
| pre-CT Surgery (%) | ||
| No | 6 (30.0%) | |
| Yes | 14 (70.0%) | |
| Unknown | 27 | |
| pre-CT Chemotherapy (%) | ||
| No | 21 (46.7%) | |
| Yes | 24 (53.3%) | |
| Unknown | 2 | |
| KRAS-Mutation (%) | ||
| No | 23 (67.6%) | |
| Yes | 11 (32.4%) | |
| Unknown | 13 | |
| NRAS-Mutation (%) | ||
| No | 32 (94.1%) | |
| Yes | 2 (5.9%) | |
| Unknown | 13 | |
| BRAF-Mutation (%) | ||
| No | 13 (86.7%) | |
| Yes | 2 (13.3%) | |
| Unknown | 32 | |
| MSS/MSI (%) | ||
| MSI | 1 (5.0%) | |
| MSS | 19 (95.0%) | |
| Unknown | 27 | |
| Variable | Cluster 1 | Cluster 2 | Cluster 3 | Cluster 4 | Cluster 5 | p | |
|---|---|---|---|---|---|---|---|
| n (lesions) | 31 | 105 | 64 | 59 | 2 | ||
| Sex (%) | F | 18 (20.22%) | 14 (15.73%) | 34 (38.2%) | 22 (24.72%) | 1 (1.12%) | <0.001 |
| M | 13 (7.56%) | 91 (52.91%) | 30 (17.44%) | 37 (21.51%) | 1 (0.58%) | ||
| Tumor Location (%) | Colon | 0 (0%) | 0 (0%) | 2 (100%) | 0 (0%) | 0 (0%) | <0.001 |
| Colon asc. | 0 (0%) | 8 (50%) | 4 (25%) | 4 (25%) | 0 (0%) | ||
| Colon desc. | 0 (0%) | 8 (38.1%) | 3 (14.29%) | 10 (47.62%) | 0 (0%) | ||
| Colon tran. | 3 (21.43%) | 1 (7.14%) | 2 (14.29%) | 8 (57.14%) | 0 (0%) | ||
| Rectum | 25 (15.15%) | 74 (44.85%) | 44 (26.67%) | 21 (12.73%) | 1 (0.61%) | ||
| Rectosigmoid Junction | 0 (0%) | 0 (0%) | 4 (44.44%) | 5 (55.56%) | 0 (0%) | ||
| Sigma | 3 (8.82%) | 14 (41.18%) | 5 (14.71%) | 11 (32.35%) | 1 (2.94%) | ||
| T-Stage (%) | T1 | 0 (0.0%) | 2 (1.9%) | 3 (4.7%) | 1 (1.7%) | 0 (0.0%) | 0.009 |
| T2 | 6 (19.4%) | 13 (12.4%) | 3 (4.7%) | 6 (10.2%) | 0 (0.0%) | ||
| T3 | 16 (51.6%) | 57 (54.3%) | 22 (34.4%) | 24 (40.7%) | 1 (50.0%) | ||
| T4 | 6 (19.4%) | 33 (31.4%) | 32 (50.0%) | 28 (47.5%) | 1 (50.0%) | ||
| Tx | 3 (9.7%) | 0 (0.0%) | 4 (6.2%) | 0 (0.0%) | 0 (0.0%) | ||
| N-Stage (%) | N0 | 2 (6.5%) | 9 (8.6%) | 12 (18.8%) | 5 (8.5%) | 0 (0.0%) | <0.001 |
| N1 | 9 (29.0%) | 68 (64.8%) | 14 (21.9%) | 34 (57.6%) | 2 (100.0%) | ||
| N2 | 17 (54.8%) | 28 (26.7%) | 36 (56.2%) | 20 (33.9%) | 0 (0.0%) | ||
| Nx | 3 (9.7%) | 0 (0.0%) | 2 (3.1%) | 0 (0.0%) | 0 (0.0%) | ||
| pre-CT Surgery (%) | No | 7 (28%) | 13 (52%) | 3 (12%) | 2 (8%) | 0 (0%) | NA |
| Yes | 13 (12.26%) | 43 (40.57%) | 36 (33.96%) | 14 (13.21%) | 0 (0%) | ||
| pre-CT Chemotherapy (%) | No | 11 (9.48%) | 61 (52.59%) | 23 (19.83%) | 20 (17.24%) | 1 (0.86%) | 0.006 |
| Yes | 20 (15.27%) | 38 (29.01%) | 41 (31.3%) | 31 (23.66%) | 1 (0.76%) | ||
| KRAS-Mutation (%) | No | 21 (16.15%) | 37 (28.46%) | 37 (28.46%) | 35 (26.92%) | 0 (0%) | <0.001 |
| Yes | 2 (2.3%) | 51 (58.62%) | 20 (22.99%) | 13 (14.94%) | 1 (1.15%) | ||
| NRAS-Mutation (%) | No | 16 (7.77%) | 87 (42.23%) | 54 (26.21%) | 48 (23.3%) | 1 (0.49%) | <0.001 |
| Yes | 7 (63.64%) | 1 (9.09%) | 3 (27.27%) | 0 (0%) | 0 (0%) | ||
| BRAF-Mutation (%) | No | 7 (7.53%) | 26 (27.96%) | 33 (35.48%) | 26 (27.96%) | 1 (1.08%) | <0.001 |
| Yes | 2 (5.88%) | 29 (85.29%) | 3 (8.82%) | 0 (0%) | 0 (0%) | ||
| MSS/MSI (%) | MSI | 0 (0%) | 0 (0%) | 0 (0%) | 2 (100%) | 0 (0%) | 0.095 |
| MSS | 10 (6.9%) | 63 (43.45%) | 43 (29.66%) | 28 (19.31%) | 1 (0.69%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tharmaseelan, H.; Hertel, A.; Tollens, F.; Rink, J.; Woźnicki, P.; Haselmann, V.; Ayx, I.; Nörenberg, D.; Schoenberg, S.O.; Froelich, M.F. Identification of CT Imaging Phenotypes of Colorectal Liver Metastases from Radiomics Signatures—Towards Assessment of Interlesional Tumor Heterogeneity. Cancers 2022, 14, 1646. https://doi.org/10.3390/cancers14071646
Tharmaseelan H, Hertel A, Tollens F, Rink J, Woźnicki P, Haselmann V, Ayx I, Nörenberg D, Schoenberg SO, Froelich MF. Identification of CT Imaging Phenotypes of Colorectal Liver Metastases from Radiomics Signatures—Towards Assessment of Interlesional Tumor Heterogeneity. Cancers. 2022; 14(7):1646. https://doi.org/10.3390/cancers14071646
Chicago/Turabian StyleTharmaseelan, Hishan, Alexander Hertel, Fabian Tollens, Johann Rink, Piotr Woźnicki, Verena Haselmann, Isabelle Ayx, Dominik Nörenberg, Stefan O. Schoenberg, and Matthias F. Froelich. 2022. "Identification of CT Imaging Phenotypes of Colorectal Liver Metastases from Radiomics Signatures—Towards Assessment of Interlesional Tumor Heterogeneity" Cancers 14, no. 7: 1646. https://doi.org/10.3390/cancers14071646