
CT-Based Radiomics Analysis to Predict Histopathological Outcomes Following Liver Resection in Colorectal Liver Metastases

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset Characteristics
2.2. CT Imaging Protocol
2.3. Image Processing
2.4. CT Post-Processing with Pyradiomic Tool
2.5. Statistical Analysis
2.5.1. Univariate Analysis
2.5.2. Multivariate Analysis
3. Results
3.1. Univariate Analysis Findings
3.2. Multivariate Analysis Findings
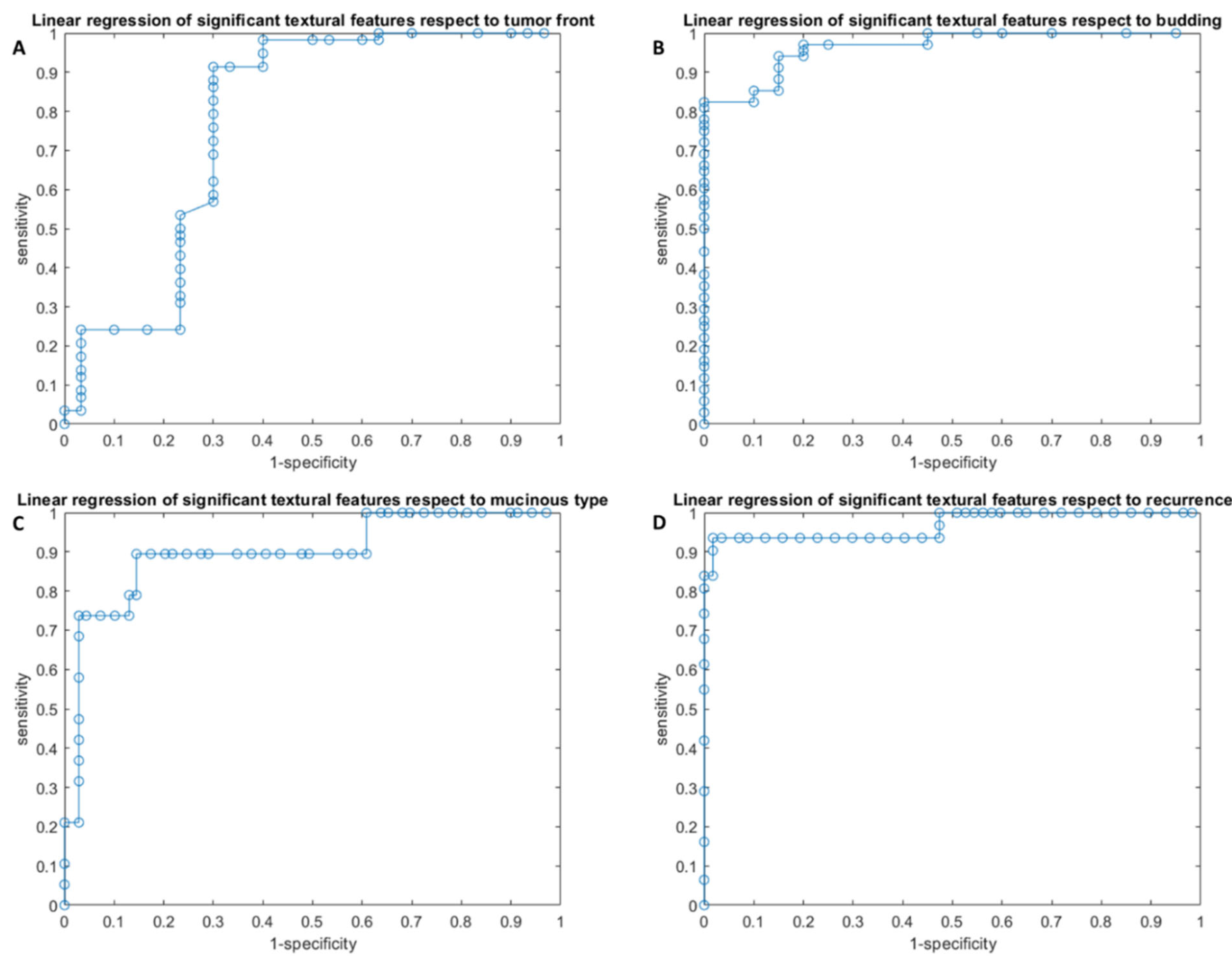
3.2.1. Linear Regression Analysis Findings
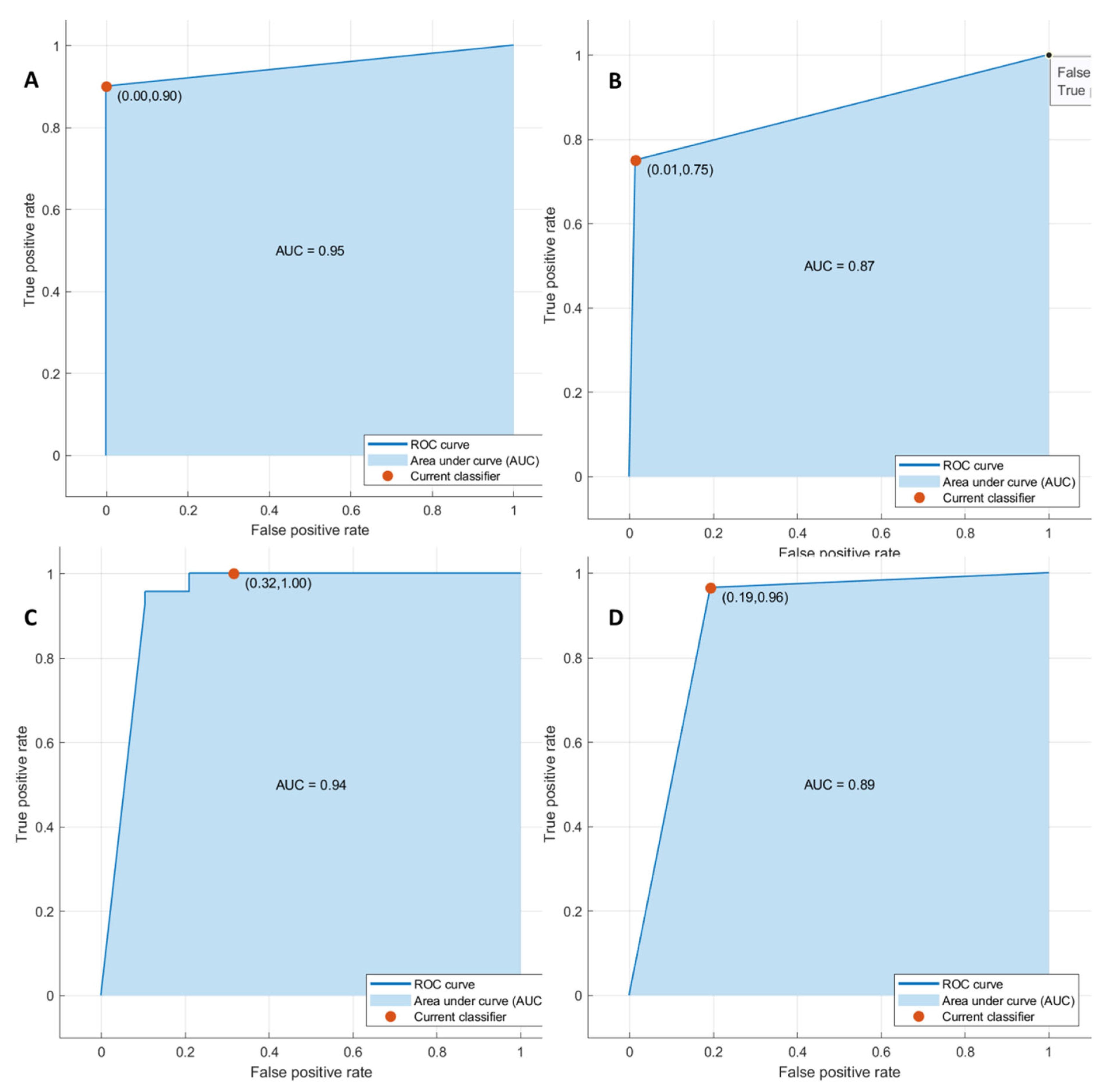
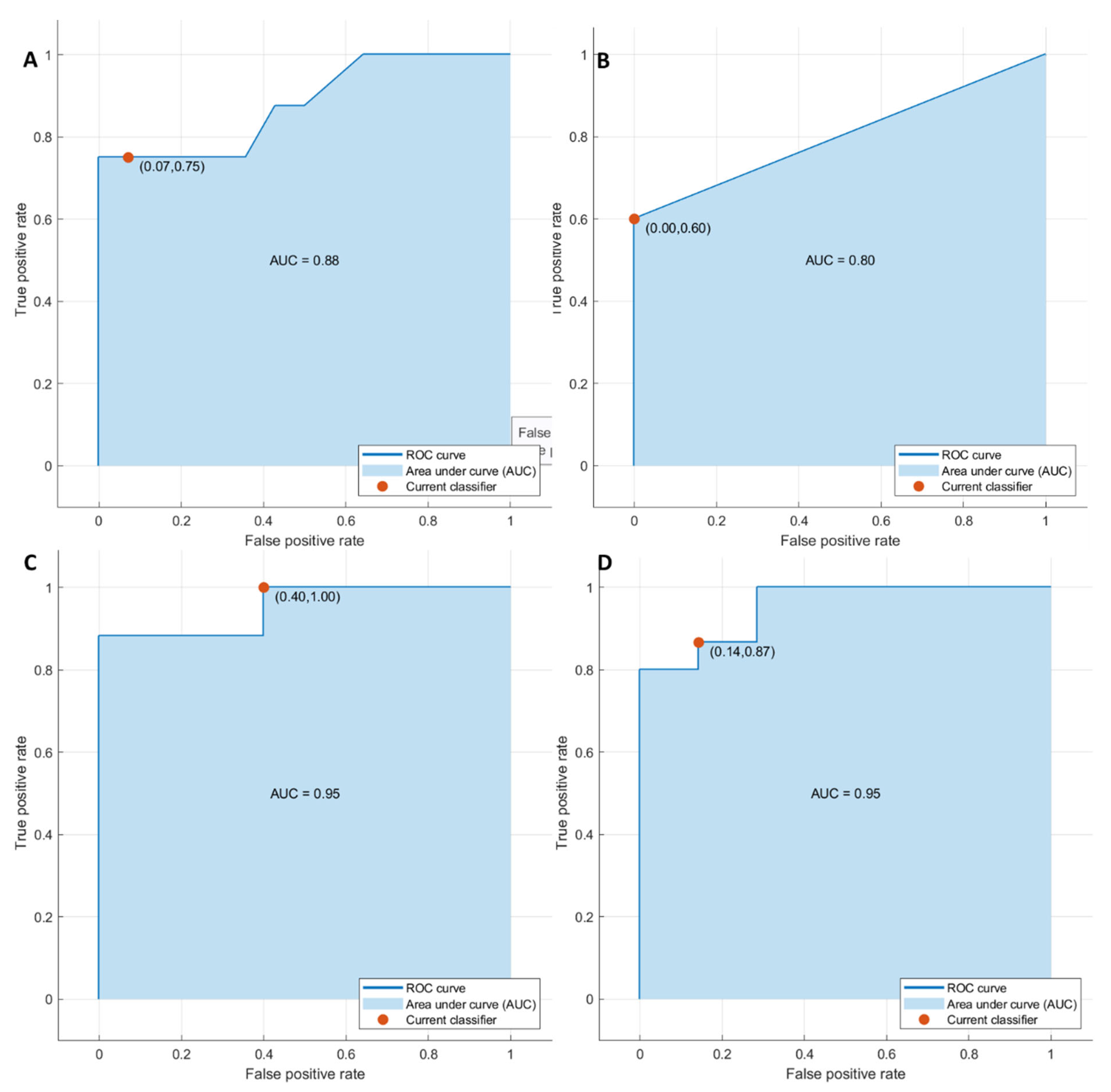
3.2.2. Pattern Recognition Approaches Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Granata, V.; Fusco, R.; Costa, M.; Picone, C.; Cozzi, D.; Moroni, C.; La Casella, G.; Montanino, A.; Monti, R.; Mazzoni, F.; et al. Preliminary Report on Computed Tomography Radiomics Features as Biomarkers to Immunotherapy Selection in Lung Adenocarcinoma Patients. Cancers 2021, 13, 3992. [Google Scholar] [CrossRef] [PubMed]
- Nardone, V.; Reginelli, A.; Grassi, R.; Boldrini, L.; Vacca, G.; D’Ippolito, E.; Annunziata, S.; Farchione, A.; Belfiore, M.P.; Desideri, I.; et al. Delta radiomics: A systematic review. Radiol. Med. 2021, 126, 1571–1583. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.-T.; Shan, Q.-Y.; Chen, S.-L.; Li, B.; Feng, S.-T.; Xu, E.-J.; Li, X.; Long, J.-Y.; Xie, X.-Y.; Lu, M.-D.; et al. CT-based radiomics for preoperative prediction of early recurrent hepatocellular carcinoma: Technical reproducibility of acquisition and scanners. Radiol. Med. 2020, 125, 697–705. [Google Scholar] [CrossRef]
- Nazari, M.; Shiri, I.; Hajianfar, G.; Oveisi, N.; Abdollahi, H.; Deevband, M.R.; Oveisi, M.; Zaidi, H. Noninvasive Fuhrman grading of clear cell renal cell carcinoma using computed tomography radiomic features and machine learning. Radiol. Med. 2020, 125, 754–762. [Google Scholar] [CrossRef] [Green Version]
- Granata, V.; Fusco, R.; Avallone, A.; De Stefano, A.; Ottaiano, A.; Sbordone, C.; Brunese, L.; Izzo, F.; Petrillo, A. Radiomics-Derived Data by Contrast Enhanced Magnetic Resonance in RAS Mutations Detection in Colorectal Liver Metastases. Cancers 2021, 13, 453. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Risi, C.; Ottaiano, A.; Avallone, A.; De Stefano, A.; Grimm, R.; Grassi, R.; Brunese, L.; Izzo, F.; et al. Diffusion-Weighted MRI and Diffusion Kurtosis Imaging to Detect RAS Mutation in Colorectal Liver Metastasis. Cancers 2020, 12, 2420. [Google Scholar] [CrossRef]
- Petralia, G.; Summers, P.E.; Agostini, A.; Ambrosini, R.; Cianci, R.; Cristel, G.; Calistri, L.; Colagrande, S. Dynamic contrast-enhanced MRI in oncology: How we do it. Radiol. Med. 2020, 125, 1288–1300. [Google Scholar] [CrossRef]
- Ria, F.; Samei, E. Is regulatory compliance enough to ensure excellence in medicine? Radiol. Med. 2020, 125, 904–905. [Google Scholar] [CrossRef]
- Zhang, A.; Song, J.; Ma, Z.; Chen, T. Combined dynamic contrast-enhanced magnetic resonance imaging and diffusion-weighted imaging to predict neoadjuvant chemotherapy effect in FIGO stage IB2-IIA2 cervical cancers. Radiol. Med. 2020, 125, 1233–1242. [Google Scholar] [CrossRef]
- Crimi, F.; Capelli, G.; Spolverato, G.; Bao, Q.R.; Florio, A.; Milite Rossi, S.; Cecchin, D.; Albertoni, L.; Campi, C.; Pucciarelli, S.; et al. MRI T2-weighted sequences-based texture analysis (TA) as a predictor of response to neoadjuvant chemo-radiotherapy (nCRT) in patients with locally advanced rectal cancer (LARC). Radiol. Med. 2020, 125, 1216–1224. [Google Scholar] [CrossRef]
- Kirienko, M.; Ninatti, G.; Cozzi, L.; Voulaz, E.; Gennaro, N.; Barajon, I.; Ricci, F.; Carlo-Stella, C.; Zucali, P.; Sollini, M.; et al. Computed tomography (CT)-derived radiomic features differentiate prevascular mediastinum masses as thymic neoplasms versus lymphomas. Radiol. Med. 2020, 125, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Kang, L.; Li, G.; Zhang, X.; Ren, J.; Shi, Z.; Li, J.; Yu, S. Computed tomography-based radiomics model for discriminating the risk stratification of gastrointestinal stromal tumors. Radiol. Med. 2020, 125, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Gurgitano, M.; Angileri, S.A.; Rodà, G.M.; Liguori, A.; Pandolfi, M.; Ierardi, A.M.; Wood, B.J.; Carrafiello, G. Interventional Radiology ex-machina: Impact of Artificial Intelligence on practice. Radiol. Med. 2021, 126, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A deep look into radiomics. Radiol. Med. 2021, 126, 1296–1311. [Google Scholar] [CrossRef]
- Wei, J.; Jiang, H.; Gu, D.; Niu, M.; Fu, F.; Han, Y.; Song, B.; Tian, J. Radiomics in liver diseases: Current progress and future opportunities. Liver Int. 2020, 40, 2050–2063. [Google Scholar] [CrossRef]
- Xiang, F.; Liang, X.; Yang, L.; Liu, X.; Yan, S. CT radiomics nomogram for the preoperative prediction of severe post-hepatectomy liver failure in patients with huge (≥10 cm) hepatocellular carcinoma. World J. Surg. Oncol. 2021, 19, 344. [Google Scholar] [CrossRef]
- Ma, X.; Wei, J.; Gu, D.; Zhu, Y.; Feng, B.; Liang, M.; Wang, S.; Zhao, X.; Tian, J. Preoperative radiomics nomogram for microvascular invasion prediction in hepatocellular carcinoma using contrast-enhanced CT. Eur. Radiol. 2019, 29, 3595–3605. [Google Scholar] [CrossRef]
- Zhang, D.; Wei, Q.; Wu, G.G.; Zhang, X.Y.; Lu, W.W.; Lv, W.Z.; Liao, J.T.; Cui, X.W.; Ni, X.J.; Dietrich, C.F. Preoperative Prediction of Microvascular Invasion in Patients with Hepatocellular Carcinoma Based on Radiomics Nomogram Using Contrast-Enhanced Ultrasound. Front. Oncol. 2021, 11, 709339. [Google Scholar] [CrossRef]
- Rocca, A.; Brunese, M.C.; Santone, A.; Avella, P.; Bianco, P.; Scacchi, A.; Scaglione, M.; Bellifemine, F.; Danzi, R.; Varriano, G.; et al. Early Diagnosis of Liver Metastases from Colorectal Cancer through CT Radiomics and Formal Methods: A Pilot Study. J. Clin. Med. 2021, 11, 31. [Google Scholar] [CrossRef]
- de la Pinta, C.; Castillo, M.E.; Collado, M.; Galindo-Pumariño, C.; Peña, C. Radiogenomics: Hunting Down Liver Metastasis in Colorectal Cancer Patients. Cancers 2021, 13, 5547. [Google Scholar] [CrossRef]
- Borhani, A.A.; Catania, R.; Velichko, Y.S.; Hectors, S.; Taouli, B.; Lewis, S. Radiomics of hepatocellular carcinoma: Promising roles in patient selection, prediction, and assessment of treatment response. Abdom. Radiol. 2021, 46, 3674–3685. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Catalano, O.; Filice, S.; Amato, D.M.; Nasti, G.; Avallone, A.; Izzo, F.; Petrillo, A. Early Assessment of Colorectal Cancer Patients with Liver Metastases Treated with Antiangiogenic Drugs: The Role of Intravoxel Incoherent Motion in Diffusion-Weighted Imaging. PLoS ONE 2015, 10, e0142876. [Google Scholar]
- Hof, J.; Kok, K.; Sijmons, R.H.; De Jong, K.P. Systematic Review of the Prognostic Role of the Immune System After Surgery of Colorectal Liver Metastases. Front. Oncol. 2019, 9, 148. [Google Scholar] [CrossRef] [PubMed]
- Ottaiano, A.; Caraglia, M.; Di Mauro, A.; Botti, G.; Lombardi, A.; Galon, J.; Luce, A.; D’Amore, L.; Perri, F.; Santorsola, M.; et al. Evolution of Mutational Landscape and Tumor Immune-Microenvironment in Liver Oligo-Metastatic Colorectal Cancer. Cancers 2020, 12, 3073. [Google Scholar] [CrossRef]
- Patrone, R.; Granata, V.; Belli, A.; Palaia, R.; Albino, V.; Piccirillo, M.; Fusco, R.; Tatangelo, F.; Nasti, G.; Avallone, A.; et al. The safety and efficacy of Glubran 2 as biliostatic agent in liver resection. Infect. Agents Cancer 2021, 16, 19. [Google Scholar] [CrossRef]
- Rega, D.; Granata, V.; Petrillo, A.; Pace, U.; Sassaroli, C.; Di Marzo, M.; Cervone, C.; Fusco, R.; D’Alessio, V.; Nasti, G.; et al. Organ Sparing for Locally Advanced Rectal Cancer after Neoadjuvant Treatment Followed by Electrochemotherapy. Cancers 2021, 13, 3199. [Google Scholar] [CrossRef]
- Huang, R.; Jiang, L.; Xu, Y.; Gong, Y.; Ran, H.; Wang, Z.; Sun, Y. Comparative Diagnostic Accuracy of Contrast-Enhanced Ultrasound and Shear Wave Elastography in Differentiating Benign and Malignant Lesions: A Network Meta-Analysis. Front. Oncol. 2019, 9, 102. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://pyradiomics.readthedocs.io/en/latest/features.html (accessed on 16 April 2021).
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Im-age-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar]
- Fusco, R.; Sansone, M.; Filice, S.; Carone, G.; Amato, D.M.; Sansone, C.; Petrillo, A. Pattern Recognition Approaches for Breast Cancer DCE-MRI Classification: A Systematic Review. J. Med. Biol. Eng. 2016, 36, 449–459. [Google Scholar] [CrossRef] [Green Version]
- Ahn, S.J.; Kim, J.H.; Park, S.J.; Han, J.K. Prediction of the therapeutic response after FOLFOX and FOLFIRI treatment for patients with liver metastasis from colorectal cancer using computerized CT texture analysis. Eur. J. Radiol. 2016, 85, 1867–1874. [Google Scholar]
- Giannini, V.; Rosati, S.; DeFeudis, A.; Balestra, G.; Vassallo, L.; Cappello, G.; Mazzetti, S.; De Mattia, C.; Rizzetto, F.; Torresin, A.; et al. Radiomics predicts response of individual HER2 -amplified colorectal cancer liver metastases in patients treated with HER2-targeted therapy. Int. J. Cancer 2020, 147, 3215–3223. [Google Scholar] [PubMed]
- Beckers, R.C.J.; Trebeschi, S.; Maas, M.; Schnerr, R.S.; Sijmons, J.M.L.; Beets, G.L.; Houwers, J.B.; Beets-Tan, R.G.H.; Lambregts, D.M.J. CT texture analysis in colorectal liver metastases and the surrounding liver parenchyma and its potential as an imaging biomarker of disease aggressiveness, response and survival. Eur. J. Radiol. 2018, 102, 15–21. [Google Scholar] [PubMed]
- Andersen, I.R.; Thorup, K.; Andersen, M.B.; Olesen, R.; Mortensen, F.V.; Nielsen, D.T.; Rasmussen, F. Texture in the monitoring of regorafenib therapy in patients with colorectal liver metastases. Acta Radiol. 2019, 60, 1084–1093. [Google Scholar]
- Zhang, H.; Li, W.; Hu, F.; Sun, Y.; Hu, T.; Tong, T. MR texture analysis: Potential imaging biomarker for predicting the chemotherapeutic response of patients with colorectal liver metastases. Abdom. Radiol. 2018, 44, 65–71. [Google Scholar]
- Lubner, M.G.; Stabo, N.; Lubner, S.J.; del Rio, A.M.; Song, C.; Halberg, R.B.; Pickhardt, P.J. CT textural analysis of hepatic metastatic colorectal cancer: Pre-treatment tumor heterogeneity correlates with pathology and clinical outcomes. Abdom. Imaging 2015, 40, 2331–2337. [Google Scholar]
- Simpson, A.L.; Doussot, A.; Creasy, J.M.; Adams, L.B.; Allen, P.J.; DeMatteo, R.P.; Gönen, M.; Kemeny, N.E.; Kingham, T.P.; Shia, J.; et al. Computed Tomography Image Texture: A Noninvasive Prognostic Marker of Hepatic Recurrence After Hepatectomy for Metastatic Colorectal Cancer. Ann. Surg. Oncol. 2017, 24, 2482–2490. [Google Scholar]
- Ganeshan, B.; Miles, K.A.; Young, R.C.; Chatwin, C.R. Hepatic Enhancement in Colorectal Cancer: Texture Analysis Correlates with Hepatic Hemodynamics and Patient Survival. Acad. Radiol. 2007, 14, 1520–1530. [Google Scholar]
- Rahmim, A.; Bak-Fredslund, K.P.; Ashrafinia, S.; Lu, L.; Schmidtlein, C.; Subramaniam, R.M.; Morsing, A.; Keiding, S.; Horsager, J.; Munk, O.L. Prognostic modeling for patients with colorectal liver metastases incorporating FDG PET radiomic features. Eur. J. Radiol. 2019, 113, 101–109. [Google Scholar]
- Dercle, L.; Lu, L.; Schwartz, L.H.; Qian, M.; Tejpar, S.; Eggleton, P.; Zhao, B.; Piessevaux, H. Radiomics Response Signature for Identification of Metastatic Colorectal Cancer Sensitive to Therapies Targeting EGFR Pathway. J. Natl. Cancer Inst. 2020, 112, 902–912. [Google Scholar]
- Ravanelli, M.; Agazzi, G.M.; Tononcelli, E.; Roca, E.; Cabassa, P.; Baiocchi, G.L.; Berruti, A.; Maroldi, R.; Farina, D. Texture features of colorectal liver metastases on pretreatment contrast-enhanced CT may predict response and prognosis in patients treated with bevacizumab-containing chemotherapy: A pilot study including comparison with standard chemotherapy. Radiol. Med. 2019, 124, 877–886. [Google Scholar]
- Rizzetto, F.; Calderoni, F.; de Mattia, C.; Defeudis, A.; Giannini, V.; Mazzetti, S.; Vassallo, L.; Ghezzi, S.; Sartore-Bianchi, A.; Marsoni, S.; et al. Impact of inter-reader contouring variability on textural radiomics of colorectal liver metastases. Eur. Radiol. Exp. 2020, 4, 62. [Google Scholar] [PubMed]
- Esposito, A.; Buscarino, V.; Raciti, D.; Casiraghi, E.; Manini, M.; Biondetti, P.; Forzenigo, L. Characterization of liver nodules in patients with chronic liver disease by MRI: Performance of the Liver Imaging Reporting and Data System (LI-RADS v.2018) scale and its comparison with the Likert scale. Radiol. Med. 2020, 125, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, M.; Eldem, G.; Bozbulut, U.B.; Bozkurt, M.F.; Kılıçkap, S.; Peynircioğlu, B.; Çil, B.; Lay Ergün, E.; Volkan-Salanci, B. Factors affecting the response to Y-90 microsphere therapy in the cholangiocarcinoma patients. Radiol. Med. 2021, 126, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Karmazanovsky, G.; Gruzdev, I.; Tikhonova, V.; Kondratyev, E.; Revishvili, A. Computed tomography-based radiomics approach in pancreatic tumors characterization. Radiol. Med. 2021, 126, 1388–1395. [Google Scholar] [CrossRef]
- Cusumano, D.; Meijer, G.; Lenkowicz, J.; Chiloiro, G.; Boldrini, L.; Masciocchi, C.; Dinapoli, N.; Gatta, R.; Casà, C.; Damiani, A.; et al. A field strength independent MR radiomics model to predict pathological complete response in locally advanced rectal cancer. Radiol. Med. 2021, 126, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Bertocchi, E.; Barugola, G.; Nicosia, L.; Mazzola, R.; Ricchetti, F.; Dell’Abate, P.; Alongi, F.; Ruffo, G. A comparative analysis between radiation dose intensification and conventional fractionation in neoadjuvant locally advanced rectal cancer: A monocentric prospective observational study. Radiol. Med. 2020, 125, 990–998. [Google Scholar] [CrossRef] [PubMed]
- Fornell-Perez, R.; Vivas-Escalona, V.; Aranda-Sanchez, J.; Gonzalez-Dominguez, M.C.; Rubio-Garcia, J.; Aleman-Flores, P.; Rodríguez, Á.L.; Porcel-De-Peralta, G.; Loro, J. Primary and post-chemoradiotherapy MRI detection of extramural venous invasion in rectal cancer: The role of diffusion-weighted imaging. Radiol. Med. 2020, 125, 522–530. [Google Scholar] [CrossRef]
- Schicchi, N.; Fogante, M.; Palumbo, P.; Agliata, G.; Esposto Pirani, P.; Di Cesare, E.; Giovagnoni, A. The sub-millisievert era in CTCA: The technical basis of the new radiation dose approach. Radiol. Med. 2020, 125, 1024–1039. [Google Scholar]
- Park, S.H.; Kim, Y.S.; Choi, J. Dosimetric analysis of the effects of a temporary tissue expander on the radiotherapy technique. Radiol. Med. 2021, 126, 437–444. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patient Description | Numbers (%)/Range |
|---|---|
| Sex | Men 50 (64.9%) |
| Women 27 (35.1%) | |
| Age | 61 year; range: 36–82 year |
| Primary cancer site | |
| Colon | 52 (67.5%) |
| Rectum | 25 (32.5%) |
| Hepatic metastases description | |
| Patients with single nodule | 48 (62.3%) |
| Patients with multiple nodules | 29 (37.7%)/range: 2–13 metastases |
| Nodule size (mm) | median size 35.8 mm; range 7–58 mm |
| Front of tumor growth | |
| Expansive | 28 (36.4%) |
| Infiltrative | 49 (63.6%) |
| Tumor budding | |
| Absent | 11 (14.3%) |
| Low grade | 13 (16.9%) |
| High grade | 53 (68.8%) |
| Mucinous carcinoma | 25 (32.5%) |
| Recurrence presence | 19 (24.7%) |
| RAS mutational status | 39 (50.6%) |
| Outcome Variable | Predictors | Accuracy Threshold on Univariate Analysis | |
|---|---|---|---|
| Dataset 1 | Front of tumor growth | Significant radiomic metrics on lesion by univariate analysis | ≥0.75 |
| Dataset 2 | Tumor budding | ≥0.80 | |
| Dataset 3 | Mucinous type | ≥0.80 | |
| Dataset 4 | Recurrence presence | ≥0.80 |
| Best Predictor at Univariate Analysis | Respect to Tumor Growth Front | Respect to Tumor Budding | Respect to Mucinous Type | Respect to Recurrences |
|---|---|---|---|---|
| wavelet_HHL_glcm_Imc2 | wavelet_LLL_firstorder_Mean | original_firstorder_RobustMeanAbsoluteDeviation | wavelet_HLH_glcm_Idmn | |
| AUC | 0.73 | 0.73 | 0.62 | 0.8 |
| Sensitivity | 0.84 | 0.91 | 0.42 | 0.81 |
| Specificity | 0.67 | 0.65 | 1.00 | 0.88 |
| PPV | 0.83 | 0.9 | 1.00 | 0.78 |
| NPV | 0.69 | 0.68 | 0.86 | 0.89 |
| Accuracy | 0.79 | 0.86 | 0.88 | 0.85 |
| Cut-off | 0.13 | 215.32 | 20.34 | 0.99 |
| Linear Regression of Significant Features | AUC | Sensitivity | Specificity | PPV | NPV | Accuracy | Cut-Off |
|---|---|---|---|---|---|---|---|
| Linear regression of the textural features with respect to the lesion front | 0.74 | 0.91 | 0.70 | 0.85 | 0.81 | 0.84 | 1.51 |
| Linear regression of the textural features with respect to tumor budding | 0.91 | 0.82 | 1.00 | 1.00 | 0.63 | 0.86 | 1.43 |
| Linear regression of the textural features with respect to the mucinous type | 0.87 | 0.89 | 0.86 | 0.63 | 0.97 | 0.86 | 0.31 |
| Linear regression of the textural features with respect to recurrence | 0.95 | 0.94 | 0.98 | 0.97 | 0.97 | 0.97 | 0.44 |
| Pattern recognition analysis with significant features | Dataset | AUC with 95% of confidence interval | Accuracy | Sensitivity | Specificity | Training time [sec] | Model type and parameters |
| KNN | Training set | 0.95 (0.92–0.97) | 96.60 | 90.00 | 100.00 | 8.70 | Weighted KNN; number of neighbors: 10; distance metric: Euclidean; distance weight: squared inverse |
| Validation set | 0.88 (0.85–0.90) | 86.40 | 75.00 | 93.00 | |||
| Training set | 0.87 (0.82–0.91) | 93.20 | 75.00 | 99.00 | 8.90 | ||
| Validation set | 0.80 (0.78–0.84) | 90.90 | 75.00 | 100.00 | |||
| Training set | 0.94 (0.92–0.97) | 93.20 | 100.00 | 68.00 | 9.10 | ||
| Validation set | 0.95 (0.91–0.96) | 90.90 | 100.00 | 60.00 | |||
| Training set | 0.89 (0.85–0.92) | 90.90 | 96.00 | 81.00 | 7.80 | ||
| Validation set | 0.95 (0.91–0.98) | 86.40 | 87.00 | 86.00 |
| Linear regression of the textural features with respect to the front of tumor growth | Coefficients | p-value | p-value |
| Intercept | 0.34 | 0.81 | 0.00 |
| original_firstorder_RootMeanSquared | 0.00 | 0.12 | |
| wavelet_LLH_firstorder_Skewness | 0.09 | 0.00 | |
| wavelet_HHH_glcm_JointEntropy | 2.87 | 0.06 | |
| wavelet_HHH_glcm_Imc2 | −2.23 | 0.10 | |
| wavelet_HHH_glcm_Imc2 | −9.22 | 0.12 | |
| wavelet_HHL_glcm_MCC | −0.70 | 0.16 | |
| wavelet_HHL_glcm_Imc2 | 2.54 | 0.07 | |
| Linear regression of the textural features with respect to tumor budding | Coefficients | p-value | p-value |
| Intercept | −0.21 | 0.86 | 0.00 |
| original_firstorder_Median | 0.20 | 0.04 | |
| original_firstorder_RootMeanSquared | 0.58 | 0.00 | |
| original_firstorder_10Percentile | 0.09 | 0.03 | |
| original_firstorder_Mean | −0.82 | 0.00 | |
| wavelet_LHL_glcm_Imc2 | 6.70 | 0.00 | |
| wavelet_LLH_glcm_ClusterShade | 0.00 | 0.58 | |
| wavelet_HHH_gldm_SmallDependenceHighGrayLevelEmphasis | −0.20 | 0.01 | |
| wavelet_HHL_glcm_MCC | −0.55 | 0.54 | |
| wavelet_HHL_glcm_Imc2 | 4.69 | 0.04 | |
| wavelet_HHL_ngtdm_Strength | −5.58 | 0.22 | |
| wavelet_LLL_firstorder_Uniformity | 34.99 | 0.08 | |
| wavelet_LLL_firstorder_Median | −0.04 | 0.25 | |
| wavelet_LLL_firstorder_RootMeanSquared | −0.22 | 0.00 | |
| wavelet_LLL_firstorder_10Percentile | −0.03 | 0.04 | |
| wavelet_LLL_firstorder_Mean | 0.27 | 0.00 | |
| wavelet_LLL_glrlm_GrayLevelNonUniformityNormalized | −44.55 | 0.06 | |
| Linear regression of the textural features respect to the mucinous type | Coefficients | p-value | p-value |
| Intercept | 0.35 | 0.42 | 0.00 |
| original_firstorder_Median | −0.02 | 0.75 | |
| original_firstorder_RobustMeanAbsoluteDeviation | 0.02 | 0.46 | |
| original_firstorder_RootMeanSquared | 0.15 | 0.07 | |
| original_firstorder_10Percentile | 0.01 | 0.80 | |
| original_firstorder_Mean | 0.00 | 1.00 | |
| wavelet_LLH_glcm_Imc2 | 0.33 | 0.52 | |
| wavelet_LLH_ngtdm_Strength | −0.03 | 0.48 | |
| wavelet_HLH_ngtdm_Strength | −1.13 | 0.29 | |
| wavelet_HLH_ngtdm_Busyness | 0.00 | 0.02 | |
| wavelet_HHH_glcm_Imc2 | 0.69 | 0.60 | |
| wavelet_HHH_ngtdm_Strength | 3.47 | 0.14 | |
| wavelet_LLL_firstorder_Median | 0.01 | 0.75 | |
| wavelet_LLL_firstorder_RootMeanSquared | −0.06 | 0.07 | |
| wavelet_LLL_firstorder_10Percentile | 0.00 | 0.99 | |
| wavelet_LLL_firstorder_Mean | 0.00 | 0.95 | |
| Linear regression of the textural features with respect to recurrences | Coefficients | p-value | p-value |
| Intercept | −0.70 | 0.77 | 0.00 |
| wavelet_LHH_gldm_DependenceVariance | 0.01 | 0.59 | |
| wavelet_HLH_gldm_LargeDependenceHighGrayLevelEmphasis | 0.00 | 0.01 | |
| wavelet_HLH_glcm_ClusterShade | −1.60 | 0.02 | |
| wavelet_HLH_glcm_Idmn | −26.27 | 0.00 | |
| wavelet_HLH_glcm_Idn | 29.13 | 0.00 | |
| wavelet_HLH_glcm_ClusterProminence | 0.06 | 0.04 | |
| wavelet_HLH_firstorder_Skewness | 0.29 | 0.01 | |
| wavelet_HLH_firstorder_Maximum | 0.00 | 0.17 | |
| wavelet_HLH_firstorder_Range | −0.01 | 0.01 | |
| wavelet_HLH_firstorder_Kurtosis | 0.01 | 0.01 | |
| wavelet_HLH_glrlm_LongRunHighGrayLevelEmphasis | 0.01 | 0.17 | |
| wavelet_HLH_glszm_GrayLevelVariance | 0.14 | 0.13 | |
| wavelet_HLH_glszm_HighGrayLevelZoneEmphasis | 0.04 | 0.00 | |
| wavelet_HLH_ngtdm_Complexity | 0.01 | 0.34 | |
| wavelet_LLL_glszm_SizeZoneNonUniformityNormalized | 5.74 | 0.03 | |
| wavelet_LLL_glszm_SmallAreaEmphasis | −2.23 | 0.30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Granata, V.; Fusco, R.; Setola, S.V.; De Muzio, F.; Dell’ Aversana, F.; Cutolo, C.; Faggioni, L.; Miele, V.; Izzo, F.; Petrillo, A. CT-Based Radiomics Analysis to Predict Histopathological Outcomes Following Liver Resection in Colorectal Liver Metastases. Cancers 2022, 14, 1648. https://doi.org/10.3390/cancers14071648
Granata V, Fusco R, Setola SV, De Muzio F, Dell’ Aversana F, Cutolo C, Faggioni L, Miele V, Izzo F, Petrillo A. CT-Based Radiomics Analysis to Predict Histopathological Outcomes Following Liver Resection in Colorectal Liver Metastases. Cancers. 2022; 14(7):1648. https://doi.org/10.3390/cancers14071648
Chicago/Turabian StyleGranata, Vincenza, Roberta Fusco, Sergio Venanzio Setola, Federica De Muzio, Federica Dell’ Aversana, Carmen Cutolo, Lorenzo Faggioni, Vittorio Miele, Francesco Izzo, and Antonella Petrillo. 2022. "CT-Based Radiomics Analysis to Predict Histopathological Outcomes Following Liver Resection in Colorectal Liver Metastases" Cancers 14, no. 7: 1648. https://doi.org/10.3390/cancers14071648