
Factors Associated with Nodal Upstaging in Clinical T1a-bN0M0 Non-Small Cell Lung Cancers


Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
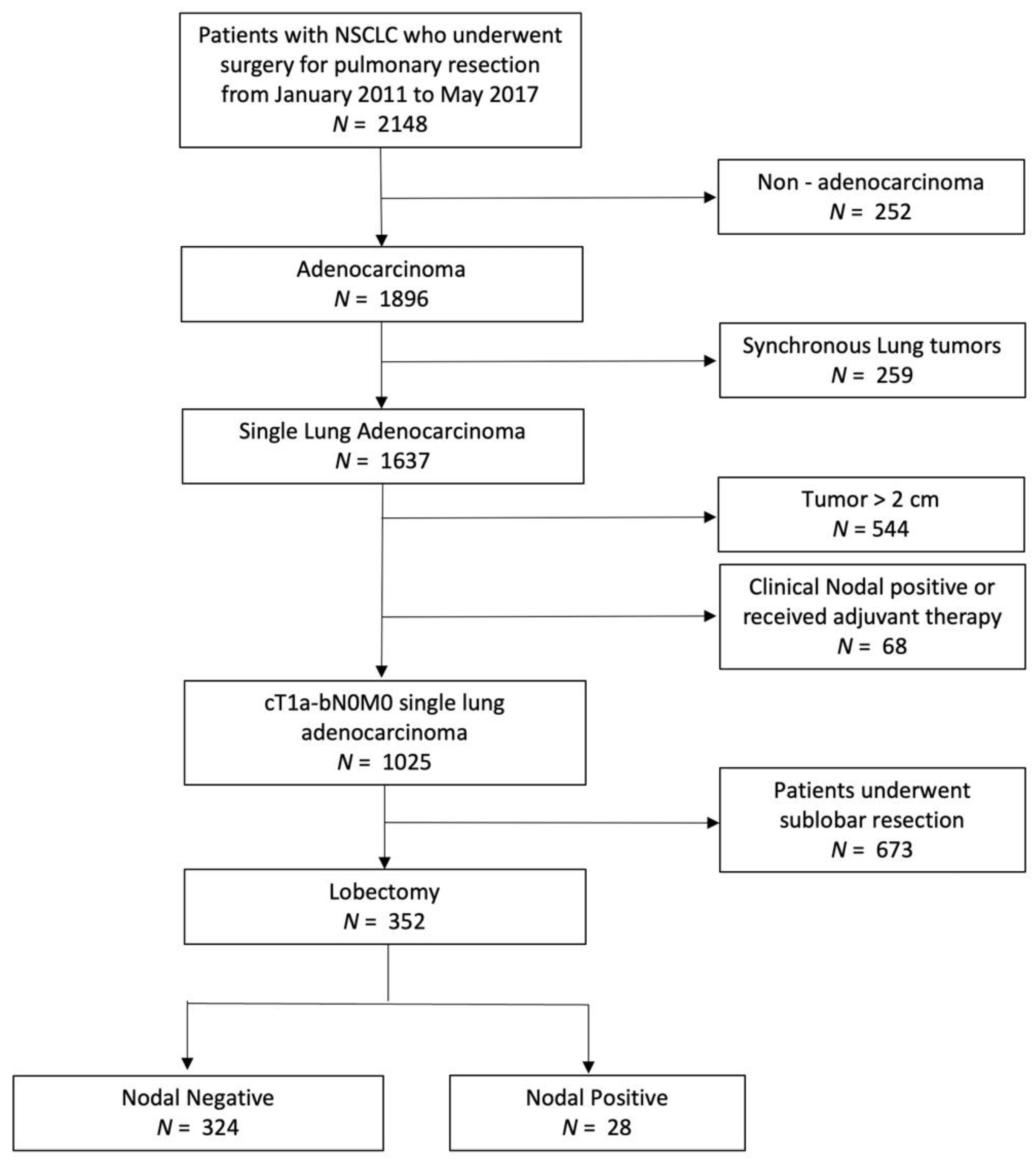
2.1. Study Population
2.2. Preoperative Assessments
2.3. Surgical Techniques and Follow-Ups
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics and Radiological Findings
3.2. Histopathological Findings
3.3. Selecting Cut-Off Values to Discriminate Patients with Lymph Nodal Upstaging
3.4. Univariate and Multivariate Analyses for Predictors of Lymph Nodal Upstaging
3.5. Correlation between Nodal Upstaging and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| NSCLC | Non-small cell lung cancer |
| CT | Computed tomography |
| LND | Lymph node dissection |
| MRI | Magnetic resonance imaging |
| PET | Positron emission tomography |
| GGO | Ground-glass opacity |
| CEA | Carcinoembryonic antigen |
| C/T ratio | consolidation-tumor ratio |
| ROC curve | Receiver operating characteristic curve |
| IQR | Interquartile range |
References
- Wood, A.J.J.; Spira, A.; Ettinger, D.S. Multidisciplinary management of lung cancer. N. Engl. J. Med. 2004, 350, 379–392. [Google Scholar]
- Wisnivesky, J.P.; Henschke, C.I.; Swanson, S.; Yankelevitz, D.F.; Zulueta, J.; Marcus, S.; Halm, E.A. Limited resection for the treatment of patients with stage IA lung cancer. Ann. Surg. 2010, 251, 550–554. [Google Scholar] [CrossRef]
- Vansteenkiste, J.; Crinò, L.; Dooms, C.; Douillard, J.Y.; Faivre-Finn, C.; Lim, E.; Rocco, G.; Senan, S.; Van Schil, P.; Veronesi, G.; et al. 2nd ESMO consensus conference on lung cancer: Early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, 1462–1474. [Google Scholar] [CrossRef]
- Boffa, D.J.; Kosinski, A.S.; Paul, S.; Mitchell, J.D.; Onaitis, M. Lymph Node Evaluation by Open or Video-Assisted Approaches in 11,500 Anatomic Lung Cancer Resections. Ann. Thorac. Surg. 2012, 94, 347–353. [Google Scholar] [CrossRef]
- Licht, P.B.; Jørgensen, O.D.; Ladegaard, L.; Jakobsen, E. A national study of nodal upstaging after thoracoscopic versus open lobectomy for clinical stage i lung cancer. Ann. Thorac. Surg. 2013, 96, 943–950. [Google Scholar] [CrossRef]
- Wilson, J.L.; Louie, B.E.; Cerfolio, R.J.; Park, B.J.; Vallières, E.; Aye, R.W.; Abdel-Razek, A.; Bryant, A.; Farivar, A.S. The prevalence of nodal upstaging during robotic lung resection in early stage non-small cell lung cancer. Ann. Thorac. Surg. 2014, 97, 1901–1907. [Google Scholar] [CrossRef]
- Toker, A.; Özyurtkan, M.O.; Kaba, E. Nodal upstaging: Effects of instrumentation and three-dimensional view in clinical stage I lung cancer. J. Vis. Surg. 2017, 3, 76. [Google Scholar] [CrossRef] [Green Version]
- Moon, Y.; Choi, S.Y.; Park, J.K.; Lee, K.Y. Risk Factors for Occult Lymph Node Metastasis in Peripheral Non-Small Cell Lung Cancer with Invasive Component Size 3 cm or Less. World J. Surg. 2020, 44, 1658–1665. [Google Scholar] [CrossRef]
- Ho, C.; Tong, K.M.; Ramsden, K.; Ionescu, D.N.; Laskin, J. Histologic classification of non-small-cell lung cancer over time: Reducing the rates of not-otherwise-specified. Curr. Oncol. 2015, 22, 164–170. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.C.; Port, J.L.; Korst, R.J.; Liss, Y.; Meherally, D.N.; Altorki, N.K. Risk Factors for Occult Mediastinal Metastases in Clinical Stage I Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2007, 84, 177–181. [Google Scholar] [CrossRef]
- Suzuki, K.; Nagai, K.; Yoshida, J.; Nishimura, M.; Takahashi, K.; Nishiwaki, Y. Clinical predictors of N2 disease in the setting of a negative computed tomographic scan in patients with lung cancer. J. Thorac. Cardiovasc. Surg. 1999, 117, 593–598. [Google Scholar] [CrossRef] [Green Version]
- De Leyn, P.; Vansteenkiste, J.; Cuypers, P.; Deneffe, G.; Van Raemdonck, D.; Coosemans, W.; Verschakelen, J.; Lerut, T. Role of cervical mediastinoscopy in staging of non-small cell lung cancer without enlarged mediastinal lymph nodes on CT scan. Eur. J. Cardio-Thorac. Surg. 1997, 12, 706–712. [Google Scholar] [CrossRef] [Green Version]
- Asamura, H.; Nakayama, H.; Kondo, H.; Tsuchiya, R.; Shimosato, Y.; Naruke, T. Lymph node involvement, recurrence, and prognosis in resected small, peripheral, non-small-cell lung carcinomas: Are these carcinomas candidates for video-assisted lobectomy? J. Thorac. Cardiovasc. Surg. 1996, 111, 1125–1134. [Google Scholar] [CrossRef] [Green Version]
- Shimamatsu, S.; Takenoyama, M.; Shimokawa, M.; Takada, K.; Edagawa, M.; Toyozawa, R.; Nosaki, K.; Oba, T.; Tagawa, T.; Yamaguchi, M.; et al. The Influence of Clinical T Factor on Predicting Pathologic N Factor in Resected Lung Cancer. Ann. Thorac. Surg. 2019, 108, 1080–1086. [Google Scholar] [CrossRef]
- Koike, T.T.; Koike, T.T.; Yamato, Y.; Yoshiya, K.; Toyabe, S. Predictive Risk Factors for Mediastinal Lymph Node Metastasis in Clinical Stage IA Non–Small-Cell Lung Cancer Patients. J. Thorac. Oncol. 2012, 7, 1246–1251. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, K.; Koike, T.; Asakawa, T.; Kusumoto, M.; Asamura, H.; Nagai, K.; Nosaki, K.; Oba, T.; Tagawa, T.; Yamaguchi, M.; et al. A prospective radiological study of thin-section computed tomography to predict pathological noninvasiveness in peripheral clinical IA lung cancer (Japan Clinical Oncology Group 0201). J. Thorac. Oncol. 2011, 6, 751–756. [Google Scholar] [CrossRef] [Green Version]
- Rami-Porta, R.; Asamura, H.; Travis, W.D.; Rusch, V.W. Lung cancer—major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 138–155. [Google Scholar] [CrossRef] [Green Version]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [Green Version]
- Jiang, T.; Li, M.; Lin, M.; Zhao, M.; Zhan, C.; Feng, M. Meta-analysis of comparing part-solid and pure-solid tumors in patients with clinical stage IA non-small-cell lung cancer in the eighth edition TNM classification. Cancer Manag. Res. 2019, 11, 2951–2961. [Google Scholar] [CrossRef] [Green Version]
- Hwang, E.J.; Park, C.M.; Ryu, Y.; Lee, S.M.; Kim, Y.T.; Kim, Y.W.; Goo, J.M. Pulmonary adenocarcinomas appearing as part-solid ground-glass nodules: Is measuring solid component size a better prognostic indicator? Eur. Radiol. 2015, 25, 558–567. [Google Scholar] [CrossRef]
- Ito, H.; Suzuki, K.; Mizutani, T.; Aokage, K.; Wakabayashi, M.; Fukuda, H.; Watanabe, S.; Koike, T.; Tsutani, Y.; Saji, H.; et al. Long-term survival outcome after lobectomy in patients with clinical T1 N0 lung cancer. J. Thorac. Cardiovasc. Surg. 2021, 161, 281–290. [Google Scholar] [CrossRef]
- Hattori, A.; Matsunaga, T.; Takamochi, K.; Oh, S.; Suzuki, K. Neither Maximum Tumor Size nor Solid Component Size Is Prognostic in Part-Solid Lung Cancer: Impact of Tumor Size Should Be Applied Exclusively to Solid Lung Cancer. Ann. Thorac. Surg. 2016, 102, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Hattori, A.; Matsunaga, T.; Takamochi, K.; Oh, S.; Suzuki, K. Significance of Lymphadenectomy in Part-Solid Lung Adenocarcinoma: Propensity Score Matched Analysis. Ann. Thorac. Surg. 2018, 106, 989–997. [Google Scholar] [CrossRef] [Green Version]
- Ketchedjian, A.; Daly, B.D.T.; Fernando, H.C.; Florin, L.; Hunter, C.J.; Morelli, D.M.; Shemin, R.J. Location as an important predictor of lymph node involvement for pulmonary adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2006, 132, 544–548. [Google Scholar] [CrossRef] [Green Version]
- De Leyn, P.; Dooms, C.; Kuzdzal, J.; Lardinois, D.; Passlick, B.; Rami-Porta, R.; Turna, A.; Van Schil, P.; Venuta, F.; Waller, D.; et al. Revised ESTS guidelines for preoperative mediastinal lymph node staging for non-small-cell lung cancer. Eur. J. Cardio-Thorac. Surg. 2014, 45, 787–798. [Google Scholar] [CrossRef]
- Silvestri, G.A.; Gonzalez, A.V.; Jantz, M.A.; Margolis, M.L.; Gould, M.K.; Tanoue, L.T.; Harris, L.J.; Detterbeck, F.C. Methods for staging non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 2013, 143, e211S–e250S. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.-H.; Chen, C.-K.; Hsieh, C.-C.; Hsu, W.-H.; Wu, Y.-C.; Hung, J.-J.; Hsu, P.-K.; Hsu, H.-S. Lymphadenectomy is Unnecessary for Pure Ground-Glass Opacity Pulmonary Nodules. J. Clin. Med. 2020, 9, 672. [Google Scholar] [CrossRef] [Green Version]
- Haruki, T.; Aokage, K.; Miyoshi, T.; Hishida, T.; Ishii, G.; Yoshida, J.; Tsuboi, M.; Nakamura, H.; Nagai, K. Mediastinal nodal involvement in patients with clinical Stage I non-small-cell lung cancer: Possibility of rational lymph node dissection. J. Thorac. Oncol. 2015, 10, 930–936. [Google Scholar] [CrossRef] [Green Version]
- Patel, V.K.; Naik, S.K.; Naidich, D.P.; Travis, W.D.; Weingarten, J.A.; Lazzaro, R.; Gutterman, D.D.; Wentowski, C.; Grosu, H.B.; Raoof, S. A practical algorithmic approach to the diagnosis and management of solitary pulmonary nodules: Part 1: Radiologic characteristics and imaging modalities. Chest 2013, 143, 825–839. [Google Scholar] [CrossRef] [Green Version]
- Chiang, X.-H.; Hsu, H.-H.; Hsieh, M.-S.; Chang, C.-H.; Tsai, T.-M.; Liao, H.-C.; Tsou, K.-C.; Lin, M.-W.; Chen, J.-S. Propensity-Matched Analysis Comparing Survival After Sublobar Resection and Lobectomy for cT1N0 Lung Adenocarcinoma. Ann. Surg. Oncol. 2020, 27, 703–715. [Google Scholar] [CrossRef]


{kind=link}
| Variable a | pN+ (n = 28) | pN− (n = 324) | p Value |
|---|---|---|---|
| Age | 59.5 (49–67.75) | 60 (52–65) | 0.828 |
| Gender (female) | 17 (60.7) | 210 (64.8) | 0.684 |
| Smoking | 4 (14.3) | 47 (14.5) | >0.999 |
| Familial lung cancer | 6 (21.7) | 64 (19.8) | 0.807 |
| Other malignancy | 5 (17.9) | 33 (10.2) | 0.206 |
| CEA (ng/mL) | 2.04 (1.28–5.67) | 1.54 (1.42–2.48) | 0.28 |
| CEA > 5 ng/mL (n) | 6 (21.7) | 12 (3.7) | 0.001 |
| Image Findings | |||
| Tumor Site | 0.872 | ||
| Right upper lobe | 10 (35.7) | 123 (38.0) | |
| Right middle lobe | 5 (17.9) | 40 (12.3) | |
| Right lower lobe | 4 (14.3) | 63 (19.4) | |
| Left upper lobe | 6 (21.4) | 58 (17.9) | |
| Left lower lobe | 3 (10.7) | 40 (12.3) | |
| Tumor Location | 0.003 | ||
| Central | 13 (46.4) | 64 (19.8) | |
| Peripheral | 15 (53.6) | 260 (80.2) | |
| Total size (cm) | 2.10 (1.79–2.69) | 1.93 (1.42–2.48) | 0.049 |
| 0–1 | 0 (0) | 33 (10.2) | 0.499 |
| 1–2 | 28 (100) | 291 (89.8) | 0.499 |
| Solid size (cm) | 1.60 (1.40–1.81) | 0.85 (0.00–1.38) | <0.001 |
| 0–1 | 0 (0) | 181 (55.9) | <0.001 |
| 1–2 | 28 (100) | 143 (44.1) | <0.001 |
| C/T ratio | 0.75 (0.59–0.87) | 0.43 (0.00–0.66) | <0.001 |
| <0.50 | 3 (10.7) | 197 (60.8) | <0.001 |
| ≥0.50 | 25 (89.3) | 127 (39.2) | |
| <0.75 | 14 (50) | 275 (84.9) | <0.001 |
| ≥0.75 | 14 (50) | 49 (15.1) | |
| Pathological features | |||
| Tumor size (cm) | 2.2 (1.73–2.5) | 1.6 (1.2–2.1) | <0.001 |
| LN op numbers | 13.5 (7–20.75) | 13 (8–18) | 0.852 |
| N1 op numbers | 4 (2–7) | 4 (2–7) | 0.592 |
| N2 op numbers | 7 (3–16.5) | 7 (4–12) | 0.907 |
| LN postive numbers | 2 (1–3) | 0 | <0.001 |
| N1 positive numbers | 1 (0–2) | 0 | <0.001 |
| N2 positive numbers | 1 (0–2.75) | 0 | <0.001 |
| Differentiation | <0.001 | ||
| Well | 0 (0) | 107 (33) | |
| Not well | 28 (100) | 217 (67) | |
| VPI | 7 (25) | 51 (15.7) | 0.005 |
| LVI | 20 (71.4) | 20 (8) | <0.001 |
| Lepidic predominant | 0 (0) | 31 (9.5) | 0.154 |
| Genetic Mutation a | n | pN+ | pN− | p Value |
|---|---|---|---|---|
| EGFR | 124 b | 4 (44.4) | 79 (68.7) | 0.155 |
| BRAF | 109 c | 0 (0) | 0 (0) | |
| KRAS | 109 c | 0 (0) | 3 (2.9) | |
| HER2 | 109 c | 0 (0) | 22 (21.8) | |
| ALK | 42 d | 1 (25) | 1 (2.6) |
| Univariate Predictors | Multivariate Predictors | ||||
|---|---|---|---|---|---|
| Independent Variables | n | OR (95% CI) | p Value | OR (95% CI) | p Value |
| Gender | |||||
| Male | 125 | 1.19 (0.54–2.63) | 0.664 | ||
| Female | 227 | 1.00 | |||
| Smoking | |||||
| Smoker | 51 | 0.98 (0.33–2.85) | 0.975 | ||
| Never Smoker | 301 | 1.00 | |||
| CEA (ng/dL) | |||||
| ≧5 | 18 | 7.09 (0.43–20.70) | <0.001 | 6.80 (1.89–24.40) | 0.003 |
| <5 | 334 | 1.00 | 1.00 | ||
| Total tumor diameter (cm) | |||||
| ≧1.7 | 229 | 2.64 (0.98–7.11) | 0.056 | ||
| <1.7 | 123 | 1.00 | |||
| Solid part diameter (cm) | |||||
| ≧1.3 | 115 | 11.6 (4.28–31.43) | <0.001 | 4.36 (1.39–13.68) | 0.012 |
| <1.3 | 237 | 1.00 | 1.00 | ||
| C/T ratio | |||||
| ≧0.50 | 152 | 12.93 (3.82–43.70) | <0.001 | 4.93 (1.16–21.02) | 0.031 |
| <0.50 | 200 | 1.00 | 1.00 | ||
| C/T ratio | |||||
| ≧0.75 | 63 | 5.61 (2.52–12.50) | <0.001 | 1.38 (0.53–3.57) | 0.51 |
| <0.75 | 289 | 1.00 | 1.00 | ||
| Tumor location | |||||
| Central | 77 | 3.52 (1.60–7.77) | 0.002 | 4.64 (1.84–11.70) | 0.001 |
| Peripheral | 275 | 1.00 | 1.00 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, T.-M.; Liu, C.-Y.; Lin, M.-W.; Hsu, H.-H.; Chen, J.-S. Factors Associated with Nodal Upstaging in Clinical T1a-bN0M0 Non-Small Cell Lung Cancers. Cancers 2022, 14, 1277. https://doi.org/10.3390/cancers14051277
Tsai T-M, Liu C-Y, Lin M-W, Hsu H-H, Chen J-S. Factors Associated with Nodal Upstaging in Clinical T1a-bN0M0 Non-Small Cell Lung Cancers. Cancers. 2022; 14(5):1277. https://doi.org/10.3390/cancers14051277
Chicago/Turabian StyleTsai, Tung-Ming, Chao-Yu Liu, Mong-Wei Lin, Hsao-Hsun Hsu, and Jin-Shing Chen. 2022. "Factors Associated with Nodal Upstaging in Clinical T1a-bN0M0 Non-Small Cell Lung Cancers" Cancers 14, no. 5: 1277. https://doi.org/10.3390/cancers14051277