
Interleukin-6 Is a Circulating Prognostic Biomarker for Hepatocellular Carcinoma Patients Treated with Combined Immunotherapy

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Quantitative Measurement of Multiple Plasma Proteins Using a Multiplex Bead-Based Immunoassay
2.3. Quantitative Measurement of Plasma IL-6 Levels by Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Statistical Analysis
3. Results
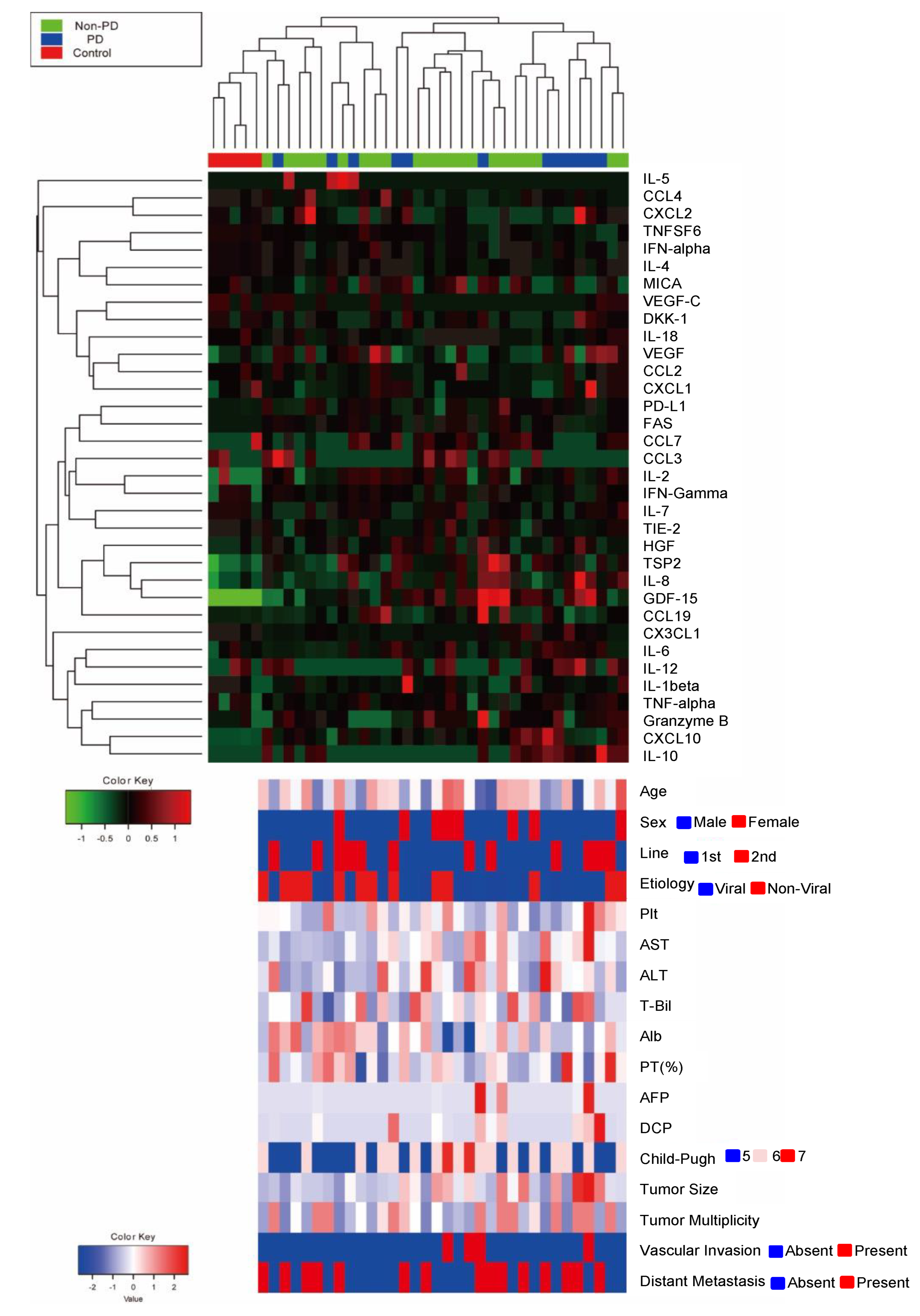
3.1. Quantitative Multiplex Measurement of Plasma Proteins Showed That High Baseline IL-6 Levels Were Associated with Poor Treatment Response in HCC Patients Who Underwent Atezo/Bev Therapy
3.1.1. Quantitative Multiplex Measurement of Plasma Proteins
3.1.2. Logistic Regression Analysis of Factors Related to Progressive Disease
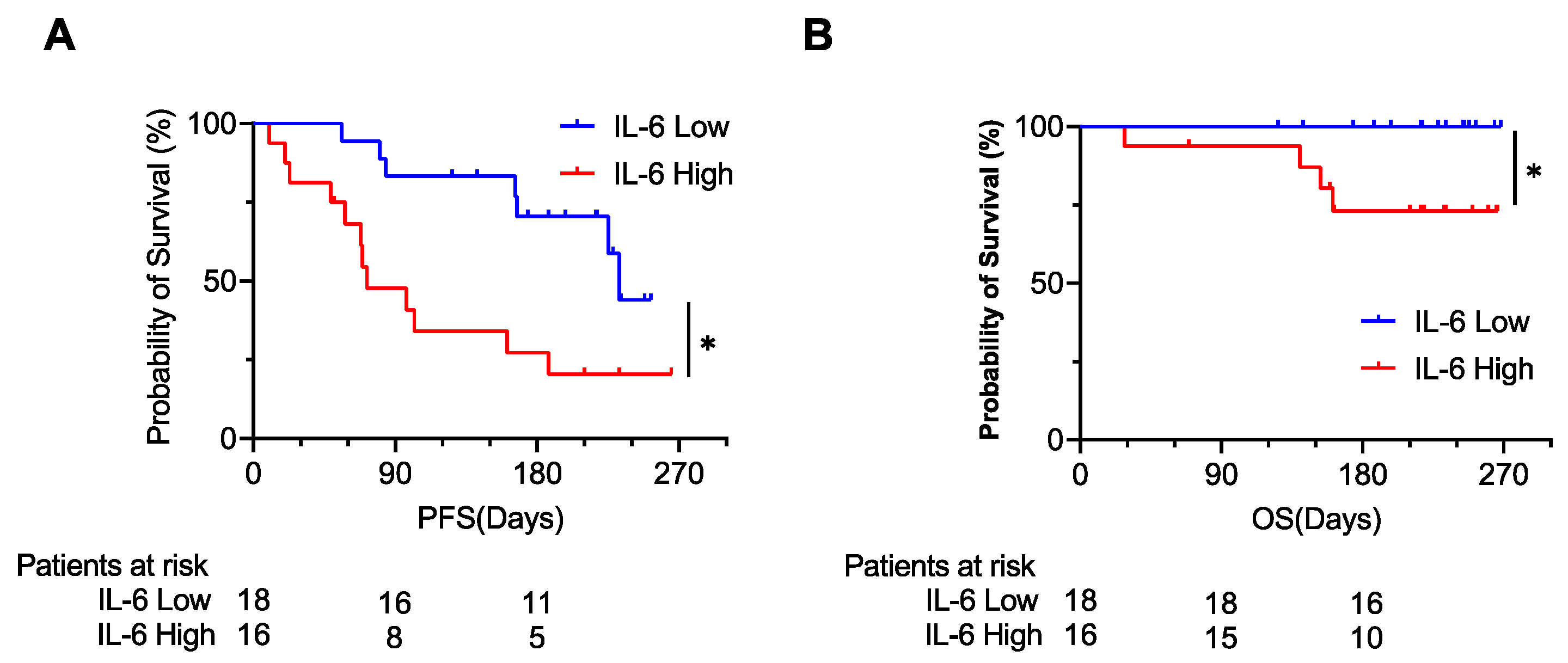
3.1.3. PFS and OS According to Plasma IL-6 Levels
3.2. High Baseline Plasma IL-6 Levels Were an Independent Predictor of Poor PFS in HCC Patients during Atezo/Bev Therapy
3.2.1. Patient Characteristics of the Validation Cohort
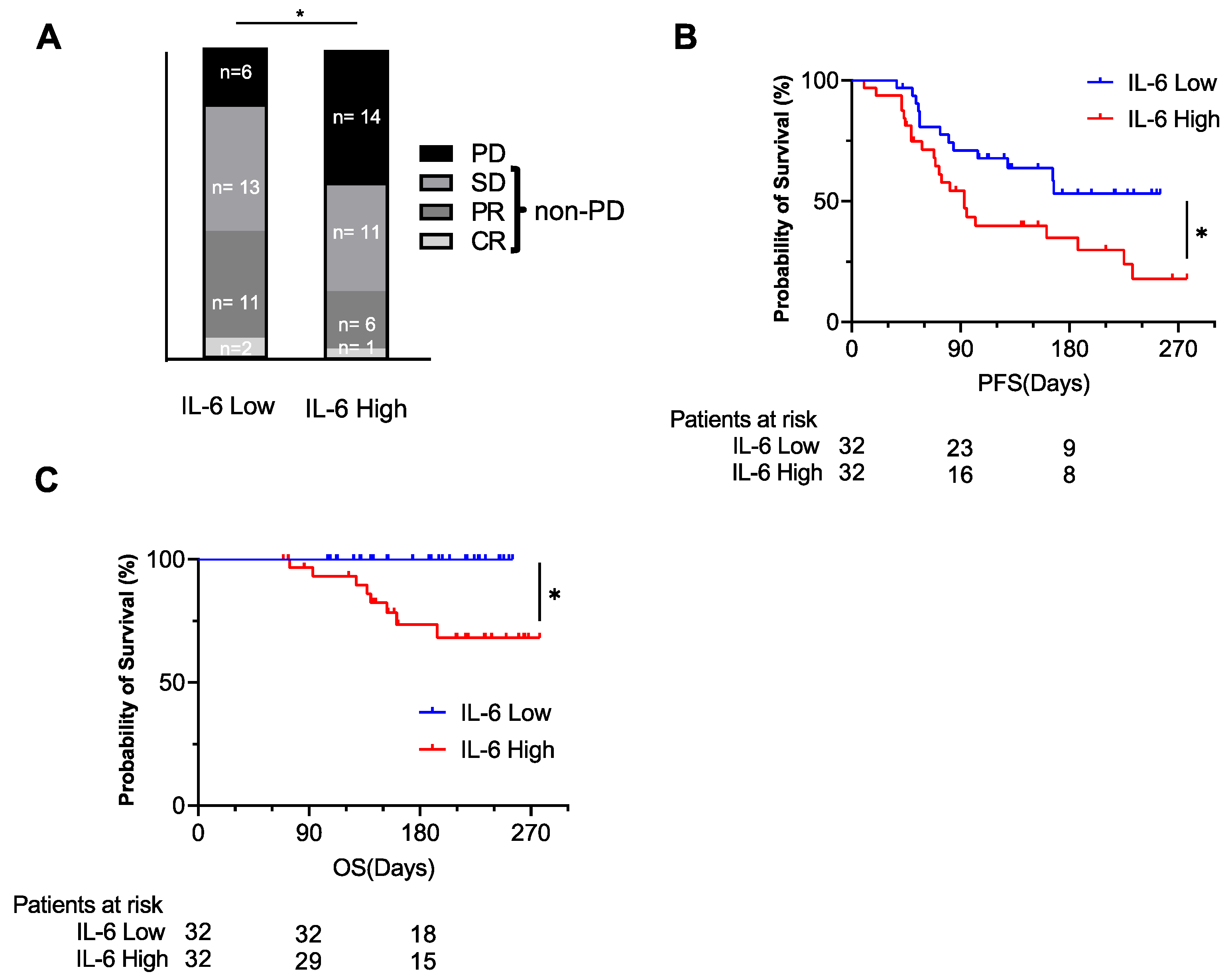
3.2.2. Treatment Response and Kaplan–Meier Curves of PFS and OS
3.2.3. Patient Characteristics According to the Plasma IL-6 Levels
3.2.4. Treatment Response and Kaplan–Meier Curves of PFS and OS According to Plasma IL-6 Levels
3.2.5. Univariate and Multivariate Cox Proportional Hazards Analysis of Factors Related to PFS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2021; in press. [Google Scholar] [CrossRef]
- Greten, T.F.; Abou-Alfa, G.K.; Cheng, A.L.; Duffy, A.G.; El-Khoueiry, A.B.; Finn, R.S.; Galle, P.R.; Goyal, L.; He, A.R.; Kaseb, A.O.; et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of hepatocellular carcinoma. J. Immunother. Cancer 2021, 9, e002794. [Google Scholar] [CrossRef]
- Kudo, M. Recent Advances in Systemic Therapy for Hepatocellular Carcinoma in an Aging Society: 2020 Update. Liver Cancer 2020, 9, 640–662. [Google Scholar] [CrossRef]
- Li, F.; Li, C.; Cai, X.; Xie, Z.; Zhou, L.; Cheng, B.; Zhong, R.; Xiong, S.; Li, J.; Chen, Z.; et al. The association between CD8+ tumor-infiltrating lymphocytes and the clinical outcome of cancer immunotherapy: A systematic review and meta-analysis. EClinicalMedicine 2021, 41, 101134. [Google Scholar] [CrossRef]
- Lu, S.; Stein, J.E.; Rimm, D.L.; Wang, D.W.; Bell, J.M.; Johnson, D.B.; Sosman, J.A.; Schalper, K.A.; Anders, R.A.; Wang, H.; et al. Comparison of Biomarker Modalities for Predicting Response to PD-1/PD-L1 Checkpoint Blockade: A Systematic Review and Meta-analysis. JAMA Oncol. 2019, 5, 1195–1204. [Google Scholar] [CrossRef]
- Llovet, J.M.; Lencioni, R. mRECIST for HCC: Performance and novel refinements. J. Hepatol. 2020, 72, 288–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demirtas, C.O.; D’Alessio, A.; Rimassa, L.; Sharma, R.; Pinato, D.J. ALBI grade: Evidence for an improved model for liver functional estimation in patients with hepatocellular carcinoma. JHEP Rep. 2021, 3, 100347. [Google Scholar] [CrossRef] [PubMed]
- Garbers, C.; Heink, S.; Korn, T.; Rose-John, S. Interleukin-6: Designing specific therapeutics for a complex cytokine. Nat. Rev. Drug Discov. 2018, 17, 395–412. [Google Scholar] [CrossRef] [PubMed]
- Giraldez, M.D.; Carneros, D.; Garbers, C.; Rose-John, S.; Bustos, M. New insights into IL-6 family cytokines in metabolism, hepatology and gastroenterology. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 787–803. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Arras, D.; Rose-John, S. IL-6 pathway in the liver: From physiopathology to therapy. J. Hepatol. 2016, 64, 1403–1415. [Google Scholar] [CrossRef] [Green Version]
- Park, E.J.; Lee, J.H.; Yu, G.Y.; He, G.; Ali, S.R.; Holzer, R.G.; Osterreicher, C.H.; Takahashi, H.; Karin, M. Dietary and genetic obesity promote liver inflammation and tumorigenesis by enhancing IL-6 and TNF expression. Cell 2010, 140, 197–208. [Google Scholar] [CrossRef] [Green Version]
- Shakiba, E.; Ramezani, M.; Sadeghi, M. Evaluation of serum interleukin-6 levels in hepatocellular carcinoma patients: A systematic review and meta-analysis. Clin. Exp. Hepatol. 2018, 4, 182–190. [Google Scholar] [CrossRef]
- Guo, Y.; Xu, F.; Lu, T.; Duan, Z.; Zhang, Z. Interleukin-6 signaling pathway in targeted therapy for cancer. Cancer Treat Rev. 2012, 38, 904–910. [Google Scholar] [CrossRef]
- Sheng, T.; Wang, B.; Wang, S.Y.; Deng, B.; Qu, L.; Qi, X.S.; Wang, X.L.; Deng, G.L.; Sun, X. The Relationship Between Serum Interleukin-6 and the Recurrence of Hepatitis B Virus Related Hepatocellular Carcinoma after Curative Resection. Medicine 2015, 94, e941. [Google Scholar] [CrossRef]
- McLoughlin, R.M.; Jenkins, B.J.; Grail, D.; Williams, A.S.; Fielding, C.A.; Parker, C.R.; Ernst, M.; Topley, N.; Jones, S.A. IL-6 trans-signaling via STAT3 directs T cell infiltration in acute inflammation. Proc. Natl. Acad. Sci. USA 2005, 102, 9589–9594. [Google Scholar] [CrossRef] [Green Version]
- Meyer, C.; Sevko, A.; Ramacher, M.; Bazhin, A.V.; Falk, C.S.; Osen, W.; Borrello, I.; Kato, M.; Schadendorf, D.; Baniyash, M.; et al. Chronic inflammation promotes myeloid-derived suppressor cell activation blocking antitumor immunity in transgenic mouse melanoma model. Proc. Natl. Acad. Sci. USA 2011, 108, 17111–17116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.F.; Kuan, F.C.; Yen, T.C.; Lu, M.S.; Lin, P.Y.; Chung, Y.H.; Chen, W.C.; Lee, K.D. IL-6-stimulated CD11b+ CD14+ HLA-DR- myeloid-derived suppressor cells, are associated with progression and poor prognosis in squamous cell carcinoma of the esophagus. Oncotarget 2014, 5, 8716–8728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.; Yang, X.; Liu, W.; Li, B.; Yin, W.; Shi, Y.; He, R. Chemerin has a protective role in hepatocellular carcinoma by inhibiting the expression of IL-6 and GM-CSF and MDSC accumulation. Oncogene 2017, 36, 3599–3608. [Google Scholar] [CrossRef] [PubMed]
- Weber, R.; Fleming, V.; Hu, X.; Nagibin, V.; Groth, C.; Altevogt, P.; Utikal, J.; Umansky, V. Myeloid-Derived Suppressor Cells Hinder the Anti-Cancer Activity of Immune Checkpoint Inhibitors. Front. Immunol. 2018, 9, 1310. [Google Scholar] [CrossRef] [Green Version]
- Bai, R.; Lv, Z.; Xu, D.; Cui, J. Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors. Biomark Res. 2020, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Myojin, Y.; Hikita, H.; Sugiyama, M.; Sasaki, Y.; Fukumoto, K.; Sakane, S.; Makino, Y.; Takemura, N.; Yamada, R.; Shigekawa, M.; et al. Hepatic Stellate Cells in Hepatocellular Carcinoma Promote Tumor Growth Via Growth Differentiation Factor 15 Production. Gastroenterology 2021, 160, 1741–1754.e1716. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhang, Y.; Shi, C.; Zhou, X.; Xu, K.; Jiao, D.; Sun, Z.; Han, X. A novel immune classification reveals distinct immune escape mechanism and genomic alterations: Implications for immunotherapy in hepatocellular carcinoma. J. Transl. Med. 2021, 19, 5. [Google Scholar] [CrossRef]
- Xiao, X.; Mo, H.; Tu, K. CTNNB1 mutation suppresses infiltration of immune cells in hepatocellular carcinoma through miRNA-mediated regulation of chemokine expression. Int. Immunopharmacol. 2020, 89, 107043. [Google Scholar] [CrossRef]
- Harding, J.J.; Nandakumar, S.; Armenia, J.; Khalil, D.N.; Albano, M.; Ly, M.; Shia, J.; Hechtman, J.F.; Kundra, R.; El Dika, I.; et al. Prospective Genotyping of Hepatocellular Carcinoma: Clinical Implications of Next-Generation Sequencing for Matching Patients to Targeted and Immune Therapies. Clin. Cancer Res. 2019, 25, 2116–2126. [Google Scholar] [CrossRef] [Green Version]
- Morita, M.; Nishida, N.; Sakai, K.; Aoki, T.; Chishina, H.; Takita, M.; Ida, H.; Hagiwara, S.; Minami, Y.; Ueshima, K.; et al. Immunological Microenvironment Predicts the Survival of the Patients with Hepatocellular Carcinoma Treated with Anti-PD-1 Antibody. Liver Cancer 2021, 10, 380–393. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Cut Off | ODDs Ratio | 95% CI | FDR p Value |
|---|---|---|---|---|
| CCL2 | >288/288 | 0.595 | 0.144–2.467 | 0.642 |
| CCL3 | Detected/Not detected | 0.200 | 0.035–1.132 | 0.405 |
| CCL4 | >220/220 | 0.595 | 0.144–2.467 | 0.642 |
| CCL7 | Detected/Not detected | 0.900 | 0.139–5.811 | 1.000 |
| CCL19 | >80/80 | 0.595 | 0.144–2.467 | 0.642 |
| CX3CL1 | >900/900 | 1.680 | 0.4054–6.962 | 0.642 |
| CXCL1 | >120/120 | 2.889 | 0.664–12.57 | 0.504 |
| CXCL2 | >145/145 | 0.595 | 0.144–2.467 | 0.642 |
| CXCL10 | >56/56 | 0.346 | 0.080–1.507 | 0.504 |
| DKK1 | >1000/1000 | 1.680 | 0.405–6.962 | 0.642 |
| Fas Ligand | >45/45 | 1.000 | 0.245–4.08 | 1.000 |
| Fas Receptor | >8400/8400 | 0.595 | 0.144–2.47 | 0.642 |
| GDF15 | >2400/2400 | 1.000 | 0.245–4.083 | 1.000 |
| Granzyme B | >9/9 | 1.000 | 0.245–4.083 | 1.000 |
| HGF | >100/100 | 1.000 | 0.245–4.083 | 1.000 |
| IFNα | >2.1/2.1 | 13.330 | 2.24–79.44 | 0.021 |
| IFNγ | >11.05/11.05 | 5.250 | 1.093–25.21 | 0.323 |
| IL1β | >3.06/3.06 | 2.889 | 0.663–12.57 | 0.504 |
| IL2 | >6.9/6.9 | 1.400 | 0.339–5.79 | 0.807 |
| IL4 | >49/49 | 3.500 | 0.795–15.40 | 0.502 |
| IL5 | Detected/Not detected | 2.000 | 0.244–16.36 | 0.681 |
| IL6 | >3.2/3.2 | 13.333 | 2.234–79.438 | 0.021 |
| IL7 | >2.4/2.4 | 0.595 | 0.144–2.467 | 0.642 |
| IL8 | >17/17 | 1.680 | 0.405–6.962 | 0.642 |
| IL10 | Detected/Not detected | 2.022 | 0.475–8.434 | 0.642 |
| IL12 | Detected/Not detected | 1.680 | 0.405–6.962 | 0.642 |
| IL18 | >260/260 | 1.680 | 0.405–6.962 | 0.642 |
| MICA | >55/55 | 1.000 | 0.245–4.08 | 1.000 |
| PD-L1 | >18/18 | 0.346 | 0.080–1.507 | 0.504 |
| TIE2 | >15,300/15,300 | 0.286 | 0.065–1.257 | 0.502 |
| TNFα | >5/5 | 0.595 | 0.137–2.445 | 0.642 |
| TSP2 | >43,000/43,000 | 1.679 | 0.405–6.962 | 0.642 |
| VEGF | >30/30 | 1.680 | 0.405–6.962 | 0.642 |
| VEGF-C | >480/480 | 1.000 | 0.245–4.08 | 1.000 |
| Characteristic | Unit | Value (Median, IQR) |
|---|---|---|
| Age | Years | 75 (63–79) |
| Sex | Male/Female | 50/14 |
| Etiology | Non-viral/Viral | 25/39 |
| Platelets | ×104/μL | 13.8 (16.1–11.1) |
| Total Bilirubin | mg/dL | 0.7 (0.5–1) |
| AST | U/L | 37 (24–51) |
| ALT | U/L | 26 (17–35) |
| PT | % | 93 (82–101) |
| Albumin | g/dL | 3.7 (3.3–4.0) |
| Child-Pugh Score | 5/6/7 | 34/26/4 |
| AFP | ng/mL | 11 (3.1–200) |
| DCP | mAU/mL | 276 (53–1544) |
| Distant Metastasis | Present/Absent | 31/33 |
| Vascular Invasion | Present/Absent | 7/57 |
| BCLC Stage | A,B/C | 30/34 |
| ALBI Score | −2.435 | |
| Tratment Line | 1st/2nd/3rd/4th- | 36/17/6/5 |
| Observation Time | Days | 104 (56–184) |
| Characteristic | Unit | Value (Median, IQR) | p value | |
|---|---|---|---|---|
| IL6 High (N=32) | IL6 Low (N = 32) | |||
| Age | Years Old | 75 (67–79) | 72 (61–81) | 0.819 |
| Sex | Male/Female | 21/11 | 29/3 | 0.032 |
| Etiology | Non-viral/Viral | 12/20 | 14/18 | 0.984 |
| Platelets | ×104/μL | 13.3 (9.0–17.8) | 14.5 (12.6–16.1) | 0.163 |
| Total Bilirubin | mg/dL | 0.7 (0.6–1.1) | 0.8 (0.5–0.9) | 0.995 |
| AST | U/L | 45 (29–57 ) | 29 (24–42) | 0.014 |
| ALT | U/L | 30 (19–47) | 22 (16–33) | 0.237 |
| PT | % | 93 (82–100) | 91 (82–103) | 0.767 |
| Albumin | g/dL | 3.6 (3.3–3.9) | 3.9 (3.5–4.1) | 0.077 |
| Child-Pugh Score | 5/6/7 | 14/14/4 | 20/12/0 | 0.041 |
| AFP | ng/mL | 57 (6.3–3718) | 6.6 (3–86) | 0.011 |
| DCP | mAU/mL | 440 (102–9982) | 108 (39–598) | 0.018 |
| Distant Metastasis | Present/Absent | 16/16 | 15/17 | 0.803 |
| Vascular Invasion | Present/Absent | 7/25 | 0/32 | 0.001 |
| BCLC Stage | A,B/C | 13/19 | 17/15 | 0.316 |
| Tratment Line | 1st/2nd/3rd/4th- | 16/9/4/3 | 20/8/2/2 | 0.709 |
| Observation Time | Days | 84 (49–160) | 130 (75–195) | 0.079 |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Characteristic | Unit | Hazard Ratio | 95% CI | p Value | Hazard Ratio | 95% CI | p Value |
| Age | >72/72 | 0.432 | 0.220–0.849 | 0.015 | 0.306 | 0.140–0.668 | 0.003 |
| Sex | Male/Femal | 1.284 | 0.571–2.887 | 0.545 | |||
| Etiology | Viral/Non-viral | 1.028 | 0.516–2.048 | 0.938 | |||
| Platelets | >12/12 | 1.134 | 0.578–2.230 | 0.712 | |||
| Total Bilirubin | >0.8/0.8 | 1.011 | 0.519–1.968 | 0.975 | |||
| AST | >40/40 | 2.58 | 1.289–5.163 | 0.008 | 1.655 | 0.785–3.488 | 0.186 |
| ALT | >27/27 | 1.77 | 0.894–3.524 | 0.101 | |||
| PT | >90/90 | 1.544 | 0.754–3.167 | 0.235 | |||
| Albumin | >3.6/3.6 | 1.148 | 0.583–2.260 | 0.689 | |||
| Child-Pugh Score | 6,7/5 | 0.76 | 0.386–1.497 | 0.428 | |||
| AFP | >11/11 | 1.953 | 0.998–3.820 | 0.051 | |||
| DCP | >276/276 | 1.478 | 0.742–2.941 | 0.266 | |||
| Distant Metastasis | Present/Absent | 1.349 | 0.693–2.627 | 0.378 | |||
| Vascular Invasion | Present/Absent | 1.924 | 0.792–4.67 | 0.148 | |||
| BCLC Stage | C/A,B | 1.241 | 0.636–2.426 | 0.526 | |||
| Treatment Line | 1st/later | 0.445 | 0.227–0.873 | 0.019 | 0.661 | 0.334–1.310 | 0.236 |
| IL6 | >4.77/4.77 | 2.197 | 1.104–4.372 | 0.025 | 2.785 | 1.216–6.380 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myojin, Y.; Kodama, T.; Sakamori, R.; Maesaka, K.; Matsumae, T.; Sawai, Y.; Imai, Y.; Ohkawa, K.; Miyazaki, M.; Tanaka, S.; et al. Interleukin-6 Is a Circulating Prognostic Biomarker for Hepatocellular Carcinoma Patients Treated with Combined Immunotherapy. Cancers 2022, 14, 883. https://doi.org/10.3390/cancers14040883
Myojin Y, Kodama T, Sakamori R, Maesaka K, Matsumae T, Sawai Y, Imai Y, Ohkawa K, Miyazaki M, Tanaka S, et al. Interleukin-6 Is a Circulating Prognostic Biomarker for Hepatocellular Carcinoma Patients Treated with Combined Immunotherapy. Cancers. 2022; 14(4):883. https://doi.org/10.3390/cancers14040883
Chicago/Turabian StyleMyojin, Yuta, Takahiro Kodama, Ryotaro Sakamori, Kazuki Maesaka, Takayuki Matsumae, Yoshiyuki Sawai, Yasuharu Imai, Kazuyoshi Ohkawa, Masanori Miyazaki, Satoshi Tanaka, and et al. 2022. "Interleukin-6 Is a Circulating Prognostic Biomarker for Hepatocellular Carcinoma Patients Treated with Combined Immunotherapy" Cancers 14, no. 4: 883. https://doi.org/10.3390/cancers14040883