
Prediction Model for Pancreatic Cancer—A Population-Based Study from NHIRD

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Data Processing
2.3. Model Training
2.3.1. Logistic Regression, LR
2.3.2. Deep Neural Networks (DNN)
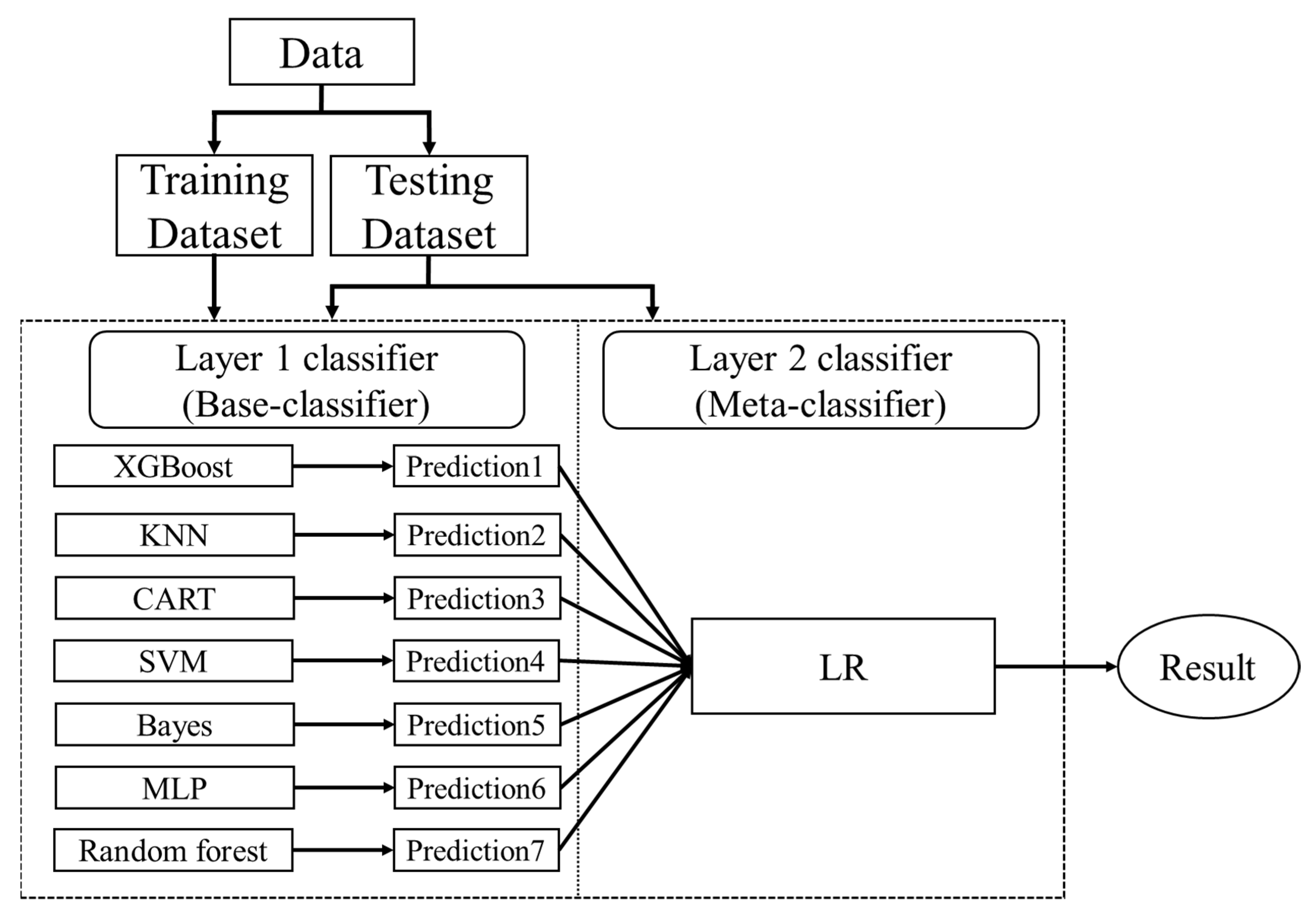
2.3.3. Ensemble Learning
- (1)
- Split the data into a training set and a testing set
- (2)
- Split the training set by k-fold
- (3)
- Train and predict until a prediction is available for each fold
- (4)
- Combine a base model on the complete training set
- (5)
- Use the model to make predictions on the testing set
- (6)
- Repeat the above steps for the other base models
- (7)
- Use all predictions from the base model as the learning features for the new model (meta-learners)
- (8)
- Use the new model to make final predictions on the testing set
2.3.4. Voting Ensemble
2.4. Model Development Environment
3. Results
3.1. Model Performance Comparison
3.1.1. First Factor Combinations (32 Factors)
3.1.2. Second Factor Combinations (19 Factors)
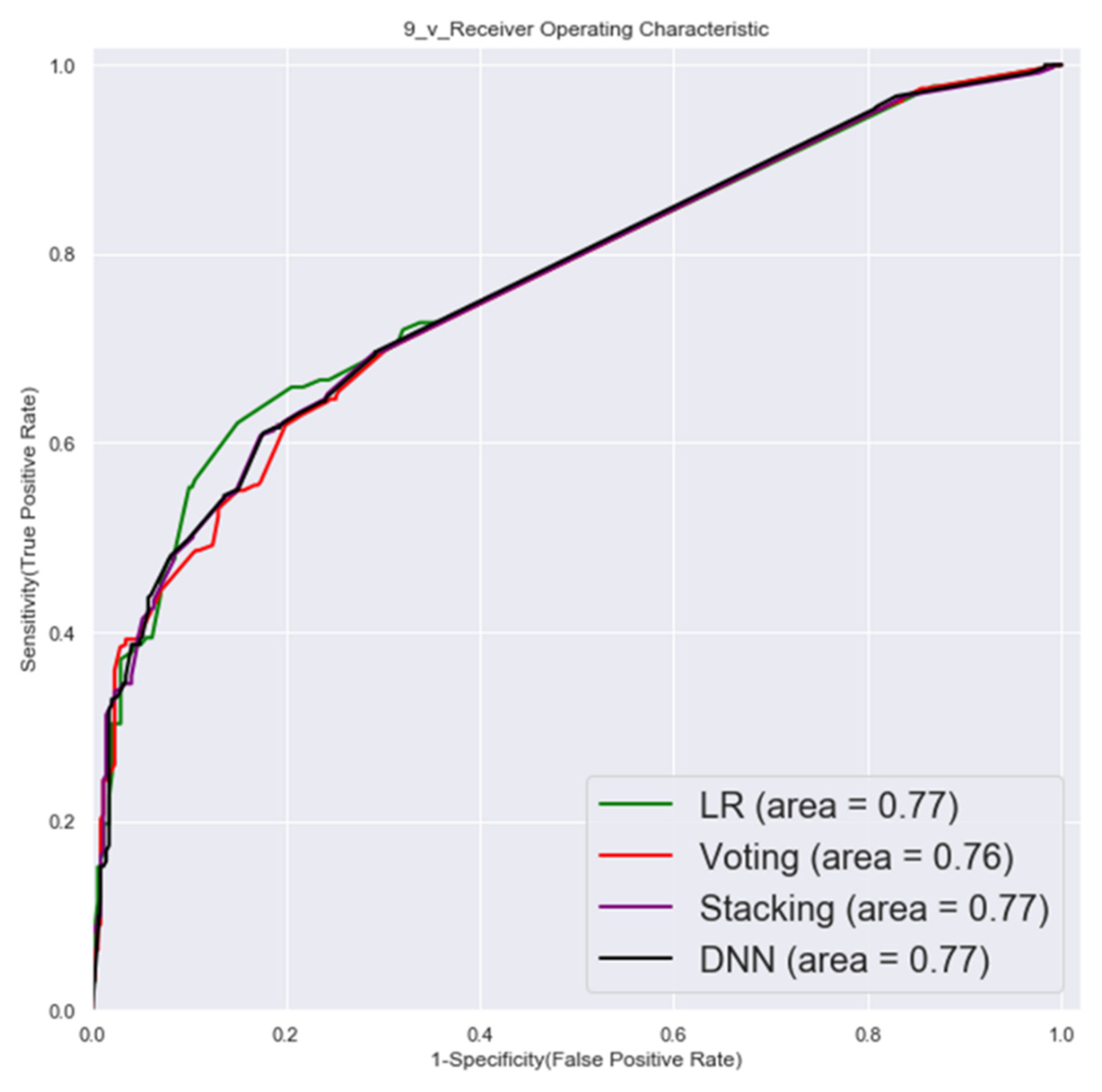
3.1.3. Third Factor Combinations (9 Factors)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chang, C.-L.; Hsu, M.-Y. The study that applies artificial intelligence and logistic regression for assistance in differential diagnostic of pancreatic cancer. Expert Syst. Appl. 2009, 36, 10663–10672. [Google Scholar] [CrossRef]
- Statistics, Ministry of Health and Welfare. National Death Cause Statistics Results (2020). 2021. Available online: https://www.hpa.gov.tw/Pages/ashx/File.ashx?FilePath=~/File/Attach/13498/File_15611.pdf (accessed on 31 December 2021).
- Chang, J.S.; Chen, L.T.; Shan, Y.S.; Chu, P.Y.; Tsai, C.R.; Tsai, H.J. The incidence and survival of pancreatic cancer by histology, including rare subtypes: A nation-wide cancer registry-based study from Taiwan. Cancer Med. 2018, 7, 5775–5788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Research Institutes, Taiwan, ROC. Pancreatic Cancer Treatment Shows Promise. 2020. Available online: https://enews.nhri.org.tw/archives/3525 (accessed on 31 December 2021).
- American Cancer Society. Cancer Facts & Figures. 2020. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2020/cancer-facts-and-figures-2020.pdf (accessed on 31 December 2021).
- Pourshams, A.; Sepanlou, S.G.; Ikuta, K.S.; Bisignano, C.; Safiri, S.; Roshandel, G.; Sharif, M.; Khatibian, M.; Fitzmaurice, C.; Nixon, M.R.; et al. The global, regional, and national burden of pancreatic cancer and its attributable risk factors in 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol. Hepatol. 2019, 4, 934–947. [Google Scholar] [CrossRef] [Green Version]
- Kamisawa, T.; Wood, L.D.; Itoi, T.; Takaori, K. Pancreatic cancer. Lancet 2016, 388, 73–85. [Google Scholar] [CrossRef]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846. [Google Scholar] [CrossRef]
- Bockhorn, M.; Uzunoglu, F.G.; Adham, M.; Imrie, C.; Milicevic, M.; Sandberg, A.A.; Asbun, H.J.; Bassi, C.; Büchler, M.; Charnley, R.M.; et al. Borderline resectable pancreatic cancer: A consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2014, 155, 977–988. [Google Scholar] [CrossRef]
- US Preventive Services Task Force. Screening for Pancreatic Cancer: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA 2019, 322, 438–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henrikson, N.B.; Bowles EJ, A.; Blasi, P.R.; Morrison, C.C.; Nguyen, M.; Pillarisetty, V.G.; Lin, J.S. Screening for Pancreatic Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2019, 322, 445–454. [Google Scholar] [CrossRef] [Green Version]
- Kim, V.M.; Ahuja, N. Early detection of pancreatic cancer. Chin. J. Cancer Res. 2015, 27, 321–331. [Google Scholar]
- Canto, M.I.; Harinck, F.; Hruban, R.H.; Offerhaus, G.J.; Poley, J.-W.; Kamel, I.; Nio, Y.; Schulick, R.S.; Bassi, C.; Kluijt, I.; et al. International Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut 2013, 62, 339. [Google Scholar] [CrossRef]
- Chari, S.T.; Mohan, V.; Pitchumoni, C.S.; Viswanathan, M.; Madanagopalan, N.; Lowenfels, A.B. Risk of pancreatic carcinoma in tropical calcifying pancreatitis: An epidemiologic study. Pancreas 1994, 9, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Lowenfels, A.B.; Maisonneuve, P.; Cavallini, G.; Ammann, R.W.; Lankisch, P.G.; Andersen, J.R.; DiMagno, E.P.; Andren-Sandberg, A.; Domellof, L. Pancreatitis and the Risk of Pancreatic Cancer. N. Engl. J. Med. 1993, 328, 1433–1437. [Google Scholar] [CrossRef] [PubMed]
- Midha, S.; Chawla, S.; Garg, P.K. Modifiable and non-modifiable risk factors for pancreatic cancer: A review. Cancer Lett. 2016, 381, 269–277. [Google Scholar] [CrossRef]
- Maisonneuve, P.; Lowenfels, A.B. Risk factors for pancreatic cancer: A summary review of meta-analytical studies. Int. J. Epidemiol. 2015, 44, 186–198. [Google Scholar] [CrossRef]
- Risch, H.A.; Yu, H.; Lu, L.; Kidd, M.S. Detectable Symptomatology Preceding the Diagnosis of Pancreatic Cancer and Absolute Risk of Pancreatic Cancer Diagnosis. Am. J. Epidemiol. 2015, 182, 26–34. [Google Scholar] [CrossRef]
- Andersen, D.K. Diabetes and cancer: Placing the association in perspective. Curr. Opin. Endocrinol. Diabetes Obes. 2013, 20, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, A.; Ekbom, A.; Olsson, R.; Kornfeldt, D.; Lööf, L.; Danielsson, Å.; Hultcrantz, R.; Lindgren, S.; Prytz, H.; Sandberg-Gertzén, H.; et al. Hepatic and extrahepatic malignancies in primary sclerosing cholangitis. J. Hepatol. 2002, 36, 321–327. [Google Scholar] [CrossRef]
- Krejs, G.J. Pancreatic Cancer: Epidemiology and Risk Factors. Dig. Dis. 2010, 28, 355–358. [Google Scholar] [CrossRef]
- Ertz-Archambault, N.; Keim, P.; Von Hoff, D. Microbiome and pancreatic cancer: A comprehensive topic review of literature. World J. Gastroenterol. 2017, 23, 1899–1908. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.-Y.; Shi, S.; Liang, C.; Meng, Q.C.; Hua, J.; Zhang, Y.-Y.; Liu, J.; Bo, Z.; Xu, J.; Yu, X.J. The microbiota and microbiome in pancreatic cancer: More influential than expected. Mol. Cancer 2019, 18, 97. [Google Scholar] [CrossRef]
- Ahn, J.; Segers, S.; Hayes, R.B. Periodontal disease, Porphyromonas gingivalis serum antibody levels and orodigestive cancer mortality. Carcinogenesis 2012, 33, 1055–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hujoel, P.P.; Drangsholt, M.; Spiekerman, C.; Weiss, N.S. An Exploration of the Periodontitis–Cancer Association. Ann. Epidemiol. 2003, 13, 312–316. [Google Scholar] [CrossRef]
- Michaud, D.S.; Joshipura, K.; Giovannucci, E.; Fuchs, C.S. A Prospective Study of Periodontal Disease and Pancreatic Cancer in US Male Health Professionals. JNCI J. Natl. Cancer Inst. 2007, 99, 171–175. [Google Scholar] [CrossRef]
- Lowenfels, A.B.; Maisonneuve, P. Epidemiology and risk factors for pancreatic cancer. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 197–209. [Google Scholar] [CrossRef]
- Appelbaum, L.; Cambronero, J.P.; Stevens, J.P.; Horng, S.; Pollick, K.; Silva, G.; Haneuse, S.; Piatkowski, G.; Benhaga, N.; Duey, S.; et al. Development and validation of a pancreatic cancer risk model for the general population using electronic health records: An observational study. Eur. J. Cancer 2021, 143, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Baecker, A.; Kim, S.; Risch, H.A.; Nuckols, T.K.; Wu, B.U.; Hendifar, A.E.; Pandol, S.J.; Pisegna, J.R.; Jeon, C.Y. Do changes in health reveal the possibility of undiagnosed pancreatic cancer? Development of a risk-prediction model based on healthcare claims data. PLoS ONE 2019, 14, e0218580. [Google Scholar] [CrossRef]
- Klein, A.P.; Lindstroem, S.; Mendelsohn, J.B.; Steplowski, E.; Arslan, A.; Bueno-De-Mesquita, H.B.; Fuchs, C.S.; Gallinger, S.; Gross, M.; Helzlsouer, K.; et al. An Absolute Risk Model to Identify Individuals at Elevated Risk for Pancreatic Cancer in the General Population. PLoS ONE 2013, 8, e72311. [Google Scholar] [CrossRef]
- Lien, H. How to Use National Health Insurance Data to Conduct Health Economics Research. Taiwan Econ. Rev. 2008, 36, 115–143. [Google Scholar]
- Grimes, D.A.; Schulz, K.F. Compared to what? Finding controls for case-control studies. Lancet 2005, 365, 1429–1433. [Google Scholar] [CrossRef]
- Moreo, A.; Esuli, A.; Sebastiani, F. Distributional Random Oversampling for Imbalanced Text Classification. In Proceedings of the 39th International ACM SIGIR Conference on Research and Development in Information Retrieval, Pisa, Italy, 17–21 July 2016; Association for Computing Machinery: New York, NY, USA, 2016; pp. 805–808. [Google Scholar]
- Ben, Q.; Xu, M.; Ning, X.; Liu, J.; Hong, S.; Huang, W.; Zhang, H.; Li, Z. Diabetes mellitus and risk of pancreatic cancer: A meta-analysis of cohort studies. Eur. J. Cancer 2011, 47, 1928–1937. [Google Scholar] [CrossRef]
- Bengio, Y.; Courville, A.; Vincent, P. Representation Learning: A Review and New Perspectives. IEEE Trans. Pattern Anal. Mach. Intell. 2013, 35, 1798–1828. [Google Scholar] [CrossRef]
- Wolpert, D.H. Stacked generalization. Neural Netw. 1992, 5, 241–259. [Google Scholar] [CrossRef]
- Polikar, D.R. Ensemble learning. Scholarpedia 2009, 4, 2776. [Google Scholar] [CrossRef]
- Yu, J.; Blackford, A.L.; Molin, M.D.; Wolfgang, C.L.; Goggins, M. Time to progression of pancreatic ductal adenocarcinoma from low-to-high tumour stages. Gut 2015, 64, 1783–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Experimental Group | Control Group | Chi-Square |
|---|---|---|---|
| (With Pancreatic Cancer) | (No Cancer) | p-Value | |
| N | 738 | 2214 | |
| Gender | 0.517 | ||
| Male | 398 (53.9%) | 1194 (53.9%) | |
| Female | 340 (46.1%) | 1020 (46.1%) | |
| Age | 1 | ||
| 0~17 | 1 (0.1%) | 1 (<0.1%) | |
| 18~24 | 14 (1.9%) | 28 (1.3%) | |
| 25~34 | 21 (2.8%) | 64 (2.9%) | |
| 35~44 | 55 (7.5%) | 141 (6.4%) | |
| 45~54 | 95 (12.9%) | 234 (10.6%) | |
| 55~64 | 144 (19.5%) | 421 (19.0%) | |
| 65 and above | 408 (55.3%) | 1325 (59.8%) | |
| Short-term historical medical information within one year before diagnosis date | |||
| Peptic ulcer, site unspecified (ICD-9 = 533) | <0.001 | ||
| 138 (18.7%) | 126 (5.7%) | ||
| Symptoms involving digestive system (ICD-9 = 787) | <0.001 | ||
| 51 (6.9%) | 63 (2.8%) | ||
| Pancreatitis (ICD-9 = 577) | <0.001 | ||
| 54 (7.3%) | 15 (0.7%) | ||
| Gastritis and duodenitis (ICD-9 = 535) | <0.001 | ||
| 220 (29.8%) | 395 (17.8%) | ||
| Disorders of function of stomach (ICD-9 = 536) | <0.001 | ||
| 169 (22.9%) | 281 (12.7%) | ||
| Functional digestive disorders, not elsewhere classified (ICD-9 = 564) | <0.001 | ||
| 154 (20.9%) | 312 (14.1%) | ||
| Chronic liver disease and cirrhosis (ICD-9 = 571) | <0.001 | ||
| 120 (16.3%) | 134 (6.1%) | ||
| Gastric ulcer (ICD-9 = 531) | <0.001 | ||
| 51 (6.9%) | 63 (2.8%) | ||
| Cholangitis (ICD-9 = 576) | <0.001 | ||
| 44 (6.0%) | 5 (0.2%) | ||
| Duodenal ulcer (ICD-9 = 532) | <0.001 | ||
| 34 (4.6%) | 31 (1.4%) | ||
| Symptoms involving respiratory system and other chest symptoms (ICD-9 = 786) | <0.001 | ||
| 75 (10.0%) | 126 (5.7%) | ||
| Acute and subacute necrosis of liver (ICD-9 = 570) | <0.001 | ||
| 11 (1.5%) | 3 (0.1%) | ||
| Abdominal pain (ICD-9 = 789) | <0.001 | ||
| 229 (31.0%) | 294 (13.3%) | ||
| Symptoms involving head and neck (ICD-9 = 784) | 0.001 | ||
| 72 (9.8%) | 325 (14.7%) | ||
| Essential hypertension (ICD-9 = 401) | 0.001 | ||
| 164 (22.2%) | 631 (28.5%) | ||
| Acute bronchitis and bronchiolitis (ICD-9 = 466) | 0.003 | ||
| 184 (25%) | 403 (18.2%) | ||
| Other and unspecified disorders of the back (ICD-9 = 724) | 0.003 | ||
| 144 (19.5%) | 547 (24.7%) | ||
| Heart failure (ICD-9 = 428) | 0.004 | ||
| 9 (1.2%) | 60 (2.7%) | ||
| Urticaria (ICD-9 = 708) | 0.006 | ||
| 26 (3.5%) | 143 (6.5%) | ||
| Calculus of kidney and ureter (ICD-9 = 592) | 0.01 | ||
| 25 (3.4%) | 37 (1.7%) | ||
| Cardiac dysrhythmias (ICD-9 = 427) | 0.011 | ||
| 13 (1.8%) | 82 (3.7%) | ||
| Gout (ICD-9 = 274) | 0.012 | ||
| 28 (3.8%) | 145 (6.5%) | ||
| Hypertensive heart disease (ICD-9 = 402) | 0.013 | ||
| 66 (8.9%) | 279 (12.6%) | ||
| Acute nasopharyngitis (ICD-9 = 460) | 0.016 | ||
| 132 (17.9%) | 483 (21.8%) | ||
| Other cellulitis and abscess (ICD-9 = 682) | 0.019 | ||
| 3 (0.4%) | 25 (1.1%) | ||
| General symptoms (ICD-9 = 780) | 0.022 | ||
| 159 (21.5%) | 422 (19.1%) | ||
| Neurotic disorders (ICD-9 = 300) | 0.033 | ||
| 23 (3.1%) | 117 (5.3%) | ||
| Other disorders of pancreatic internal secretion (ICD-9 = 251) | 0.034 | ||
| 6 (0.8%) | 5 (0.2%) | ||
| Osteoarthrosis and allied disorders (ICD-9 = 715) | 0.034 | ||
| 76 (10.3%) | 298 (13.5%) | ||
| Diabetes mellitus (ICD-9 = 250) | 0.035 | ||
| 155 (21.0%) | 368 (16.6%) | ||
| Other forms of chronic ischemic heart disease (ICD-9 = 414) | 0.044 | ||
| 44 (6.0%) | 200 (9.0%) | ||
| Acute laryngitis and tracheitis (ICD-9 = 464) | 0.045 | ||
| 64 (8.7%) | 264 (11.9%) | ||
| Spondylosis and allied disorders (ICD-9 = 723) | 0.054 | ||
| 46 (6.2%) | 182 (8.2%) | ||
| Acute upper respiratory infections of multiple or unspecified (ICD-9 = 465) | 0.058 | ||
| 383 (51.9%) | 1248 (56.4%) | ||
| Other disorders of bone and cartilage (ICD-9 = 733) | 0.065 | ||
| 13 (1.8%) | 61 (2.8%) | ||
| Other and unspecified disorder of joints (ICD-9 = 719) | 0.092 | ||
| 49 (6.6%) | 201 (9.1%) | ||
| Diseases of hard tissues of teeth (ICD-9 = 521) | 0.109 | ||
| 186 (25.2%) | 509 (23.0%) | ||
| Urinary tract infection (ICD-9 = 599) | 0.133 | ||
| 51 (6.9%) | 195 (8.8%) | ||
| Noninfectious gastroenteritis (ICD-9 = 558) | 0.143 | ||
| 145 (19.6%) | 368 (16.6%) | ||
| Diseases of pulp and periapical tissues (ICD-9 = 522) | 0.172 | ||
| 57 (7.7%) | 211 (9.5%) | ||
| Allergic rhinitis (ICD-9 = 477) | 0.178 | ||
| 40 (5.4%) | 101 (4.6%) | ||
| Acute sinusitis (ICD-9 = 461) | 0.184 | ||
| 76 (10.3%) | 221 (10.0%) | ||
| Contact dermatitis and other eczema (ICD-9 = 692) | 0.194 | ||
| 101 (13.7%) | 358 (16.2%) | ||
| Cataract (ICD-9 = 366) | 0.225 | ||
| 76 (10.3%) | 202 (9.1%) | ||
| Sprains and strains (ICD-9 = 848) | 0.234 | ||
| 40 (5.4%) | 153 (6.9%) | ||
| Vertiginous syndromes and other disorders of vestibular system (ICD-9 = 386) | 0.234 | ||
| 9 (1.2%) | 41 (1.9%) | ||
| Influenza (ICD-9 = 487) | 0.235 | ||
| 44 (6.0%) | 173 (7.8%) | ||
| Disorders of conjunctiva (ICD-9 = 372) | 0.257 | ||
| 144 (19.5%) | 539 (24.3%) | ||
| Other disorders of soft tissues (ICD-9 = 729) | 0.257 | ||
| 126 (17.1%) | 400 (18.1%) | ||
| Chronic bronchitis (ICD-9 = 491) | 0.26 | ||
| 28 (3.8%) | 83 (3.7%) | ||
| Cystitis (ICD-9 = 595) | 0.276 | ||
| 23 (3.1%) | 79 (3.6%) | ||
| Other and unspecified arthropathies (ICD-9 = 716) | 0.289 | ||
| 28 (3.8%) | 106 (4.8%) | ||
| Cholelithiasis (ICD-9 = 574) | 0.312 | ||
| 16 (2.2%) | 24 (1.1%) | ||
| Benign prostatic hyperplasia (ICD-9 = 600) | 0.315 | ||
| 55 (7.5%) | 213 (9.6%) | ||
| Bronchitis, not specified as acute or chronic (ICD-9 = 490) | 0.343 | ||
| 17 (2.3%) | 72 (3.3%) | ||
| Other disorders of synovium, tendon, and bursa (ICD-9 = 727) | 0.387 | ||
| 37 (5.0%) | 134 (6.1%) | ||
| Chronic airways obstruction, not elsewhere classified (ICD-9 = 496) | 0.416 | ||
| 29 (3.9%) | 105 (4.7%) | ||
| Pneumonia, organism unspecified (ICD-9 = 486) | 0.445 | ||
| 19 (2.6%) | 77 (3.5%) | ||
| Menopausal and postmenopausal disorders (ICD-9 = 627) | 0.511 | ||
| 5 (0.7%) | 15 (0.7%) | ||
| Infections of kidney(s) (ICD-9 = 590) | 0.518 | ||
| 3 (0.4%) | 10 (0.5%) | ||
| Gingival and periodontal diseases (ICD-9 = 523) | 0.628 | ||
| 224 (30.4%) | 667 (30.1%) | ||
| Tooth restoration root (ICD-9 = 525) | 0.651 | ||
| 35 (4.7%) | 125 (5.6%) | ||
| Acute tonsillitis (ICD-9 = 463) | 0.693 | ||
| 75 (10.2%) | 285 (12.9%) | ||
| Acute appendicitis (ICD-9 = 540) | 0.705 | ||
| 1 (0.1%) | 5 (0.2%) | ||
| Other acquired deformity (ICD-9 = 738) | 0.748 | ||
| 6 (0.8%) | 16 (0.7%) | ||
| Diseases of the oral soft tissues, excluding lesions specific (ICD-9 = 528) | 0.784 | ||
| 64 (8.7%) | 223 (10.1%) | ||
| Acute myocardial infarction (ICD-9 = 410) | 0.802 | ||
| 2 (0.3%) | 2 (0.1%) | ||
| Other disorders of cervical region (ICD-9 = 723) | 0.909 | ||
| 21 (2.8%) | 55 (2.5%) | ||
| Occlusion of cerebral arteries (ICD-9 = 434) | 0.946 | ||
| 11 (1.5%) | 38 (1.7%) | ||
| Acute pharyngitis (ICD-9 = 462) | 0.954 | ||
| 76 (10.3%) | 246 (11.1%) | ||
| Angina pectoris (ICD-9 = 413) | 0.956 | ||
| 22 (3.0%) | 65 (2.9%) | ||
| Pruritus and related conditions (ICD-9 = 698) | 0.958 | ||
| 27 (3.7%) | 74 (3.3%) | ||
| Disorders of lipoid metabolism (ICD-9 = 272) | 0.96 | ||
| 24 (3.3%) | 81 (3.7%) | ||
| Fracture of clavicle (ICD-9 = 810) | 1 | ||
| 2 (0.3%) | 4 (0.2%) | ||
| Backward Elimination | |||
|---|---|---|---|
| Disease | p-Value | Disease | p-Value |
| Abdominal pain | 1.16 × 10−7 *** | Gout | 0.038517 * |
| Peptic ulcer, site unspecified | 2.06 × 10−14 *** | Functional digestive disorders, not elsewhere classified | 0.019337 * |
| Symptoms involving digestive system | 3.35 × 10−5 *** | Neurotic disorders | 0.069057 |
| Gastritis and duodenitis | 0.000162 *** | Disorders of conjunctiva | 0.090836 |
| Disorders of function of stomach | 3.88 × 10−5 *** | Heart failure | 0.090678 |
| Chronic liver disease and cirrhosis | 2.51 × 10−12 *** | Essential hypertension | 0. 054,498 |
| General symptoms | 0.000860 *** | Other forms of chronic ischemic heart disease | 0.068356 |
| Cholangitis | 1.03 × 10−14 *** | Other and unspecified disorders of the back | 0.082334 |
| Pancreatitis | 4.14 × 10−9 *** | Duodenal ulcer | 0.059147 |
| Symptoms involving head and neck | 0.005121 ** | Calculus of kidney and ureter | 0.067626 |
| Symptoms involving respiratory system and other chest symptoms | 0.007710 ** | Acute nasopharyngitis | 0.136144 |
| Urticaria | 0.002506 ** | Acute laryngitis and tracheitis | 0.123336 |
| Other cellulitis and abscess | 0.003819 ** | Gastric ulcer | 0.141536 |
| Acute bronchitis and bronchiolitis | 0.021931 * | * Hypertensive heart disease | 0.153331 |
| Cardiac dysrhythmias | 0.032659 * | Osteoarthrosis and allied disorders | 0.13224 |
| Acute and subacute necrosis of liver | 0.010382 * | Other disorders of pancreatic internal secretion | 0.132718 |
| Diabetes mellitus | 0.017619 * | Significant codes: <0.001 ‘***’ 0.001 ‘**’ 0.01 ‘*’ | |
| First Combination (32 Factors) | Validation Set | Testing Set (External Set) | ||||||
|---|---|---|---|---|---|---|---|---|
| AUC | Accuracy | Sensitivity | Specificity | AUC | Accuracy | Sensitivity | Specificity | |
| LR | 0.78 | 0.73 | 0.7 | 0.74 | 0.76 | 0.73 | 0.7 | 0.74 |
| Voting | 0.87 | 0.77 | 0.76 | 0.77 | 0.75 | 0.7 | 0.7 | 0.71 |
| Stacking | 0.85 | 0.77 | 0.71 | 0.82 | 0.74 | 0.7 | 0.74 | 0.7 |
| DNN | 0.89 | 0.82 | 0.78 | 0.86 | 0.73 | 0.65 | 0.65 | 0.66 |
| Second Combination (19 Factors) | Validation Set | Testing Set (External Set) | ||||||
| AUC | Accuracy | Sensitivity | Specificity | AUC | Accuracy | Sensitivity | Specificity | |
| LR | 0.78 | 0.7 | 0.7 | 0.7 | 0.77 | 0.7 | 0.7 | 0.7 |
| Voting | 0.83 | 0.73 | 0.74 | 0.72 | 0.76 | 0.71 | 0.71 | 0.71 |
| Stacking | 0.82 | 0.73 | 0.74 | 0.73 | 0.73 | 0.7 | 0.7 | 0.72 |
| DNN | 0.82 | 0.73 | 0.72 | 0.74 | 0.71 | 0.7 | 0.64 | 0.76 |
| Third Combination (9 Factors) | Validation Set | Testing Set (External Set) | ||||||
| AUC | Accuracy | Sensitivity | Specificity | AUC | Accuracy | Sensitivity | Specificity | |
| LR | 0.77 | 0.7 | 0.7 | 0.7 | 0.74 | 0.68 | 0.7 | 0.67 |
| Voting | 0.76 | 0.7 | 0.7 | 0.7 | 0.73 | 0.67 | 0.7 | 0.66 |
| Stacking | 0.77 | 0.7 | 0.7 | 0.7 | 0.72 | 0.68 | 0.68 | 0.68 |
| DNN | 0.77 | 0.7 | 0.7 | 0.71 | 0.71 | 0.68 | 0.7 | 0.67 |
| Research Team | Factor | Algorithm | Data Resource | Data Period | Performance |
|---|---|---|---|---|---|
| This study | Abdominal pain, peptic ulcers, flatulence, gastritis, abnormal gastric function, hepatitis, sleep disorders, cholangitis, pancreatitis (9 factors) | Logistic regression | NHIRD | Before diagnosis, within 12 months | Validation Set: 0.77 Testing Set: 0.74 |
| Limor Appelbaum 2021 [28] | Abdominal pain, angina pectoris, asthma, atherosclerotic heart disease, gallbladder stones, chest pain, chronic pancreatitis, coronary heart disease, diabetes mellitus, emphysema, primary hypertension, family history of pancreatic cancer, jaundice, stroke, ulcers (15 factors) | Logistic regression | Electronic health record at Boston Hospital | Before diagnosis, 6–12 months | 0.68–0.75 |
| Aileen Baecker 2019 [29] | Acute pancreatitis, chronic pancreatitis, diabetes mellitus, dyspepsia, gastritis/peptic ulcer/gallbladder disease, acute cholecystitis, depression, abdominal pain, chest pain, gastrointestinal symptoms, esophageal reflux, jaundice, weight loss/anorexia, nausea/vomiting, fatigue, tickling disorder (16 factors) | Logistic regression | SEER database | Before diagnosis, within 15 months | 0.68 |
| Alison P Klein 2013 [30] | Smoking, alcohol consumption, diabetes, obesity, family history of pancreatic cancer, non-O ABO genotype (6 factors) | Absolute risk regression | PanScan consortium | 0.58–0.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.-A.; Chen, K.-W.; Hsu, C.-Y. Prediction Model for Pancreatic Cancer—A Population-Based Study from NHIRD. Cancers 2022, 14, 882. https://doi.org/10.3390/cancers14040882
Lee H-A, Chen K-W, Hsu C-Y. Prediction Model for Pancreatic Cancer—A Population-Based Study from NHIRD. Cancers. 2022; 14(4):882. https://doi.org/10.3390/cancers14040882
Chicago/Turabian StyleLee, Hsiu-An, Kuan-Wen Chen, and Chien-Yeh Hsu. 2022. "Prediction Model for Pancreatic Cancer—A Population-Based Study from NHIRD" Cancers 14, no. 4: 882. https://doi.org/10.3390/cancers14040882