
Modulation of the Tumor Microenvironment with Trastuzumab Enables Radiosensitization in HER2+ Breast Cancer


 , , , , and
, , , , and 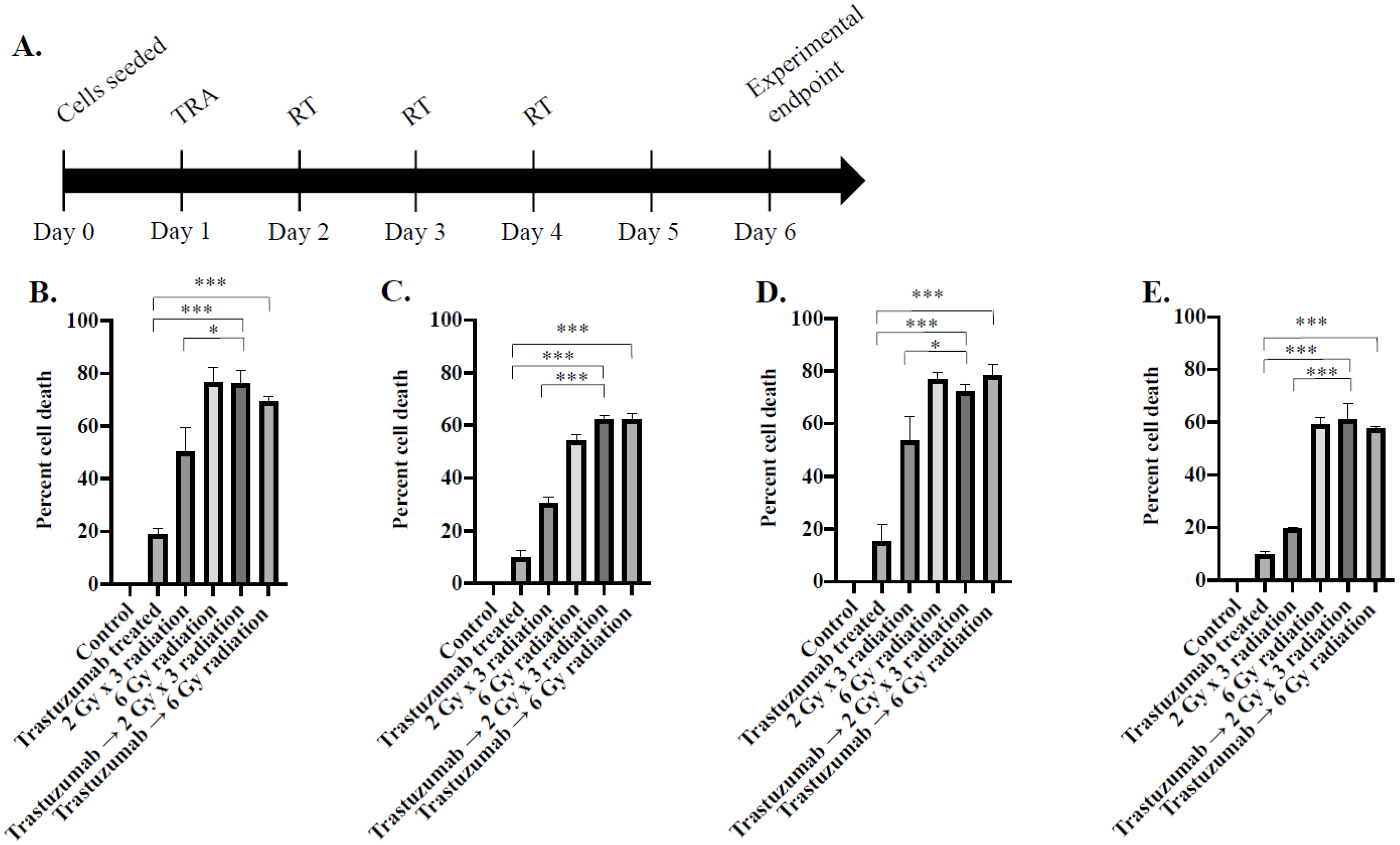{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Trastuzumab Prior to Fractionated Radiation Enhances In Vitro Cytotoxicity Compared to Single Agent Therapy
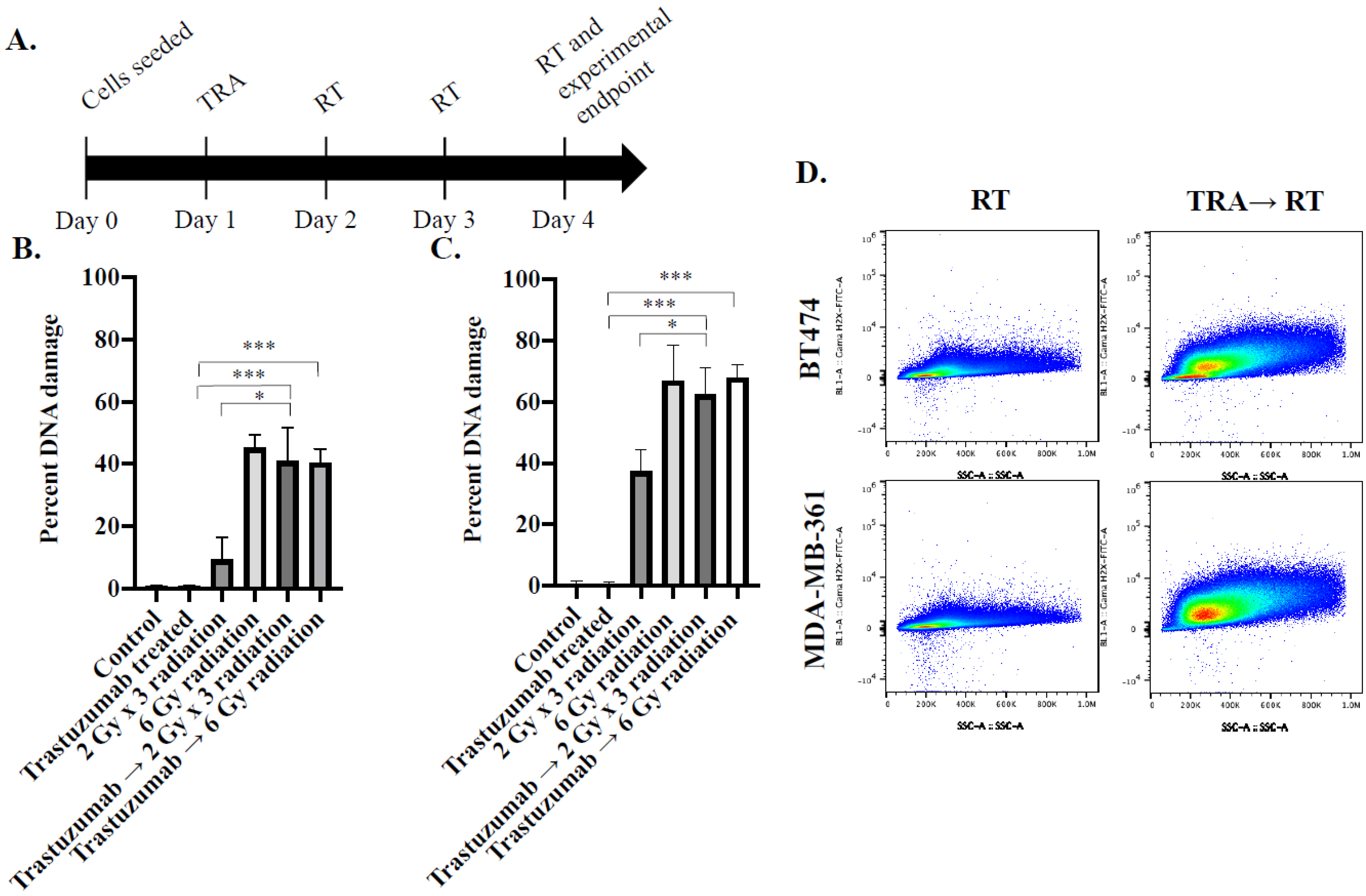
2.2. Phosphorylated γ-H2AX Analysis Reveals Significantly Increased DNA Damage in Trastuzumab-Pretreated HER2+ Cancer Cells Treated with Fractionated Radiation In Vitro
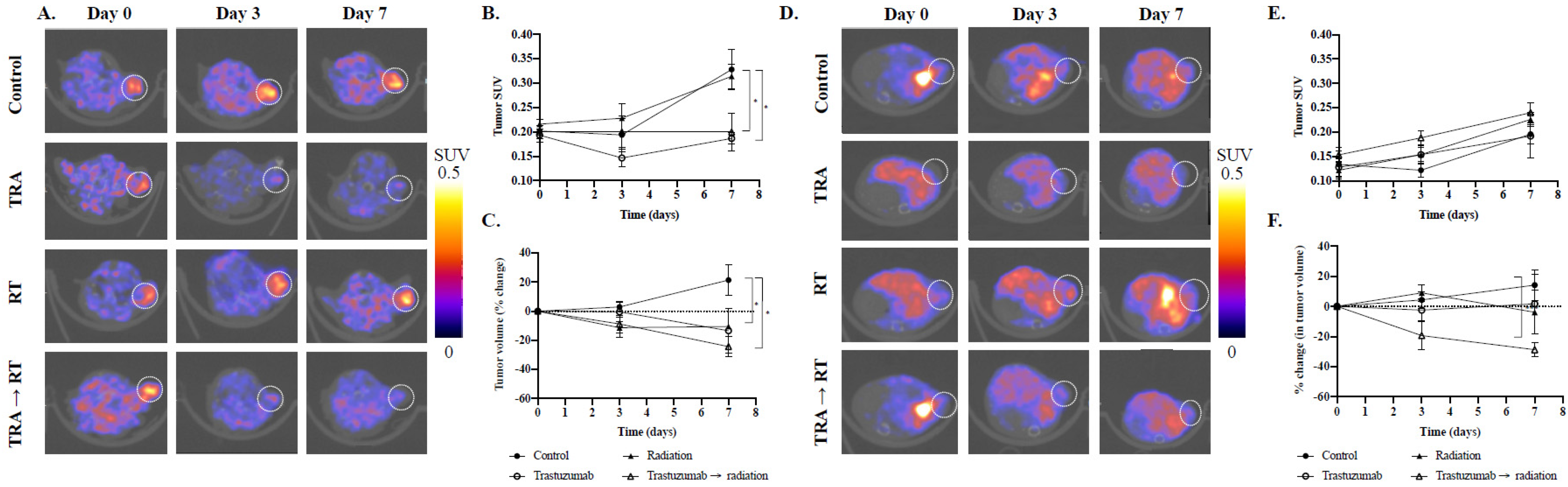
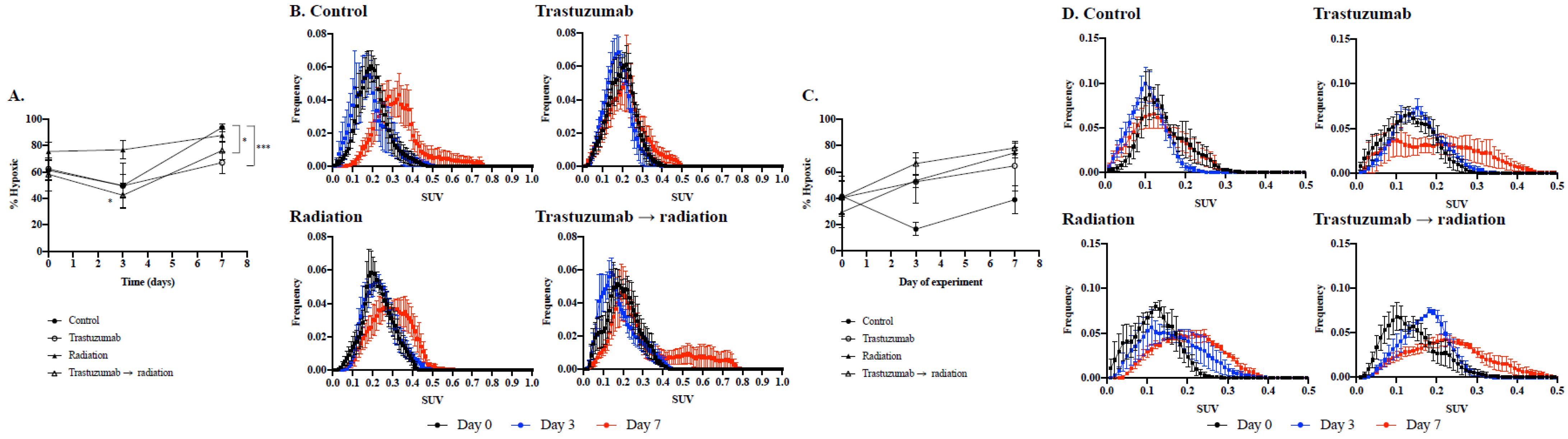
2.3. Changes in Tumor Hypoxia and Volume in Response to Treatment Synergy of Trastuzumab and Fractionated Radiation Monitored with [18F]-FMISO PET Imaging
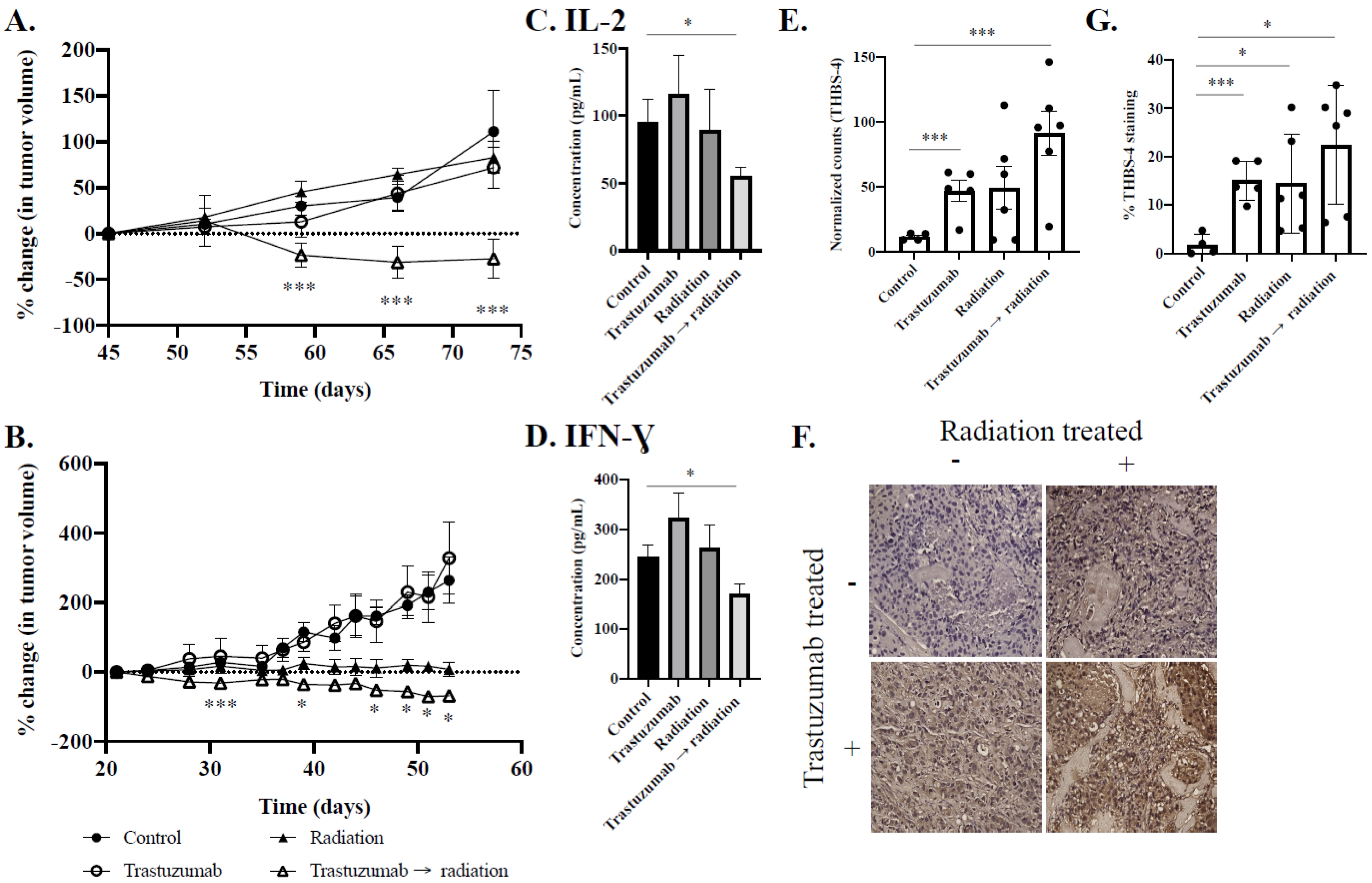
2.4. Trastuzumab Synergistically Improves the Efficacy of Fractionated Radiation over the Longitudinal Observation Period
2.5. Analyte Analysis Reveals Decreased Expression of IL-2 and IFN-Gamma in Cytotoxic Combination-Treated Tumors
2.6. Nanostring Analysis Reveals Increased Expression of Vascular and Immune Modulation in Combination-Treated Tumors
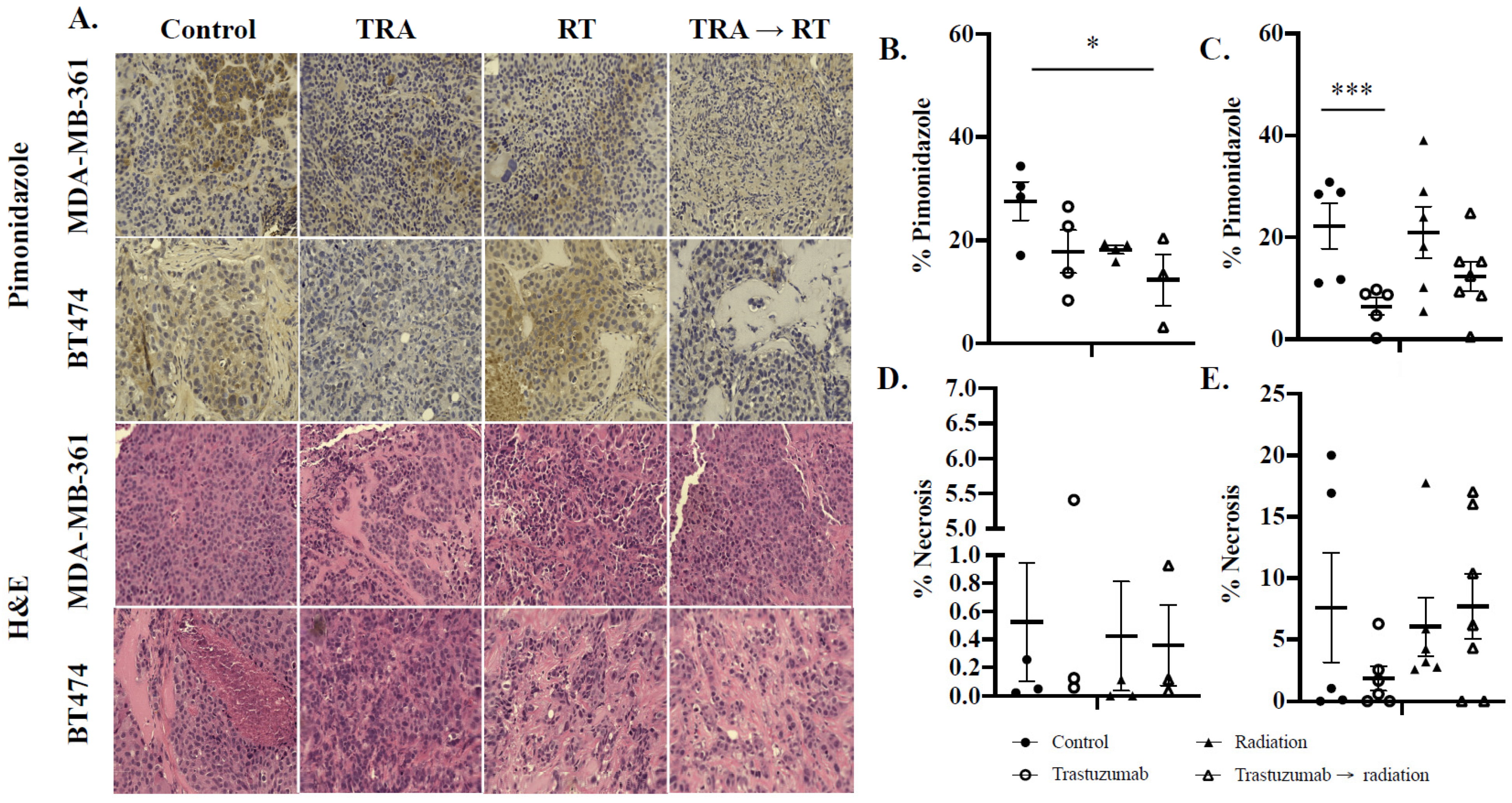
2.7. Immunohistochemical Analysis Reveals Decreased Oxygenation in Trastuzumab Monotherapy and Cytotoxic Combination-Treated Tumors
3. Discussion
4. Materials and Methods
4.1. HER2+ Cell Culture
4.2. Tumor Model
4.2.1. Evaluation of In Vitro Treatment Synergy between Trastuzumab and Fractionated Radiation
4.2.2. Evaluating In Vitro Treatment Synergy through Flow Cytometry against DNA Repair
4.2.3. Non-Invasive [18F]-FMISO PET Imaging Identifies Increases in Tumor Oxygenation That Can Be Exploited with Fractionated Radiation Therapy In Vivo
4.2.4. Longitudinal Monitoring of Changes in Tumor Viability in Response to Trastuzumab and Fractionated Radiation Therapy In Vivo
4.3. Cytokine Detection Assay
4.4. Nanostring RNA Analysis
4.5. Immunohistochemistry
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
| PET | Positron emission tomography |
| CT | Computed tomography |
| PDX | Patient derived xenograft |
| ROS | Reactive oxygen species |
| ROI | Region of interest |
| DSB | Double strand breaks |
| FMISO | [18F]-fluoromisonidazole |
| PBS | Phosphate-buffered saline |
| NSG | Nod Scid Gamma |
| SUV | Standard uptake value |
| HER2 | Human epidermal growth factor receptor 2 |
| MAPK | Mitogen activated protein kinase |
| IMEM | Improved Modified Eagle’s Media |
| DMEM | Dulbecco’s Minimal Essential Media |
| ATCC | American Type Culture Collective |
| Gy | Gray |
| RT | Radiation therapy |
| TRA | Trastuzumab |
References
- Sattler, U.G.A.; Mueller-Klieser, W. The anti-oxidant capacity of tumour glycolysis. Int. J. Radiat. Biol. 2009, 85, 963–971. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xu, B. Targeted therapeutic options and future perspectives for HER2-positive breast cancer. Signal Transduct. Target. Ther. 2019, 4, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, L.B.; Chadha, M.; Hill, R.J.; Hu, K.; Shasha, D. Impact of Tumor Hypoxia and Anemia on Radiation Therapy Outcomes. Oncologist 2002, 7, 492–508. [Google Scholar] [CrossRef] [PubMed]
- Jahanzeb, M. Adjuvant Trastuzumab Therapy for HER2-Positive Breast Cancer. Clin. Breast Cancer 2008, 8, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Muller, V.; Clemens, M.; Jassem, J.; Al-Sakaff, N.; Auclair, P.; Nuesch, E.; Holloway, D.; Shing, M.; Bang, Y.J. Long-term trastuzumab (Herceptin(R)) treatment in a continuation study of pa-tients with HER2-positive breast cancer or HER2-positive gastric cancer. BMC Cancer 2018, 18, 295. [Google Scholar] [CrossRef] [PubMed]
- Vu, T.; Claret, F.X. Trastuzumab: Updated Mechanisms of Action and Resistance in Breast Cancer. Front. Oncol. 2012, 2, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, J.; Zhou, Z.; Chen, X.; Zhao, R.; Yang, Z.; Wei, N.; Ni, Q.; Feng, Y.; Yu, X.; Ma, J.; et al. HER2 reduces breast cancer radiosensitivity by activating focal adhesion kinase in vitro and in vivo. Oncotarget 2016, 7, 45186–45198. [Google Scholar] [CrossRef] [Green Version]
- Jacob, J.; Belin, L.; Pierga, J.-Y.; Gobillion, A.; Vincent-Salomon, A.; Dendale, R.; Beuzeboc, P.; Campana, F.; Fourquet, A.; Kirova, Y.M. Concurrent administration of trastuzumab with locoregional breast radiotherapy: Long-term results of a prospective study. Breast Cancer Res. Treat. 2014, 148, 345–353. [Google Scholar] [CrossRef]
- Jongen, J.M.J.; Van Der Waals, L.M.; Trumpi, K.; Laoukili, J.; Peters, N.A.; Schelven, S.J.S.-V.; Govaert, K.M.; Rinkes, I.H.M.B.; Kranenburg, O. Downregulation of DNA repair proteins and increased DNA damage in hypoxic colon cancer cells is a therapeutically exploitable vulnerability. Oncotarget 2017, 8, 86296–86311. [Google Scholar] [CrossRef] [Green Version]
- Begg, K.; Tavassoli, M. Inside the hypoxic tumour: Reprogramming of the DDR and radiore-sistance. Cell Death Discov. 2020, 6, 77. [Google Scholar] [CrossRef]
- Liu, C.; Lin, Q.; Yun, Z. Cellular and molecular mechanisms underlying oxygen-dependent ra-diosensitivity. Radiat. Res. 2015, 183, 487–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourton, E.C.; Plowman, P.N.; Smith, D.; Arlett, C.F.; Parris, C.N. Prolonged expression of the gamma-H2AX DNA repair biomarker correlates with excess acute and chronic toxicity from radiotherapy treatment. Int. J. Cancer 2011, 129, 2928–2934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, J.; Milano, M.T.; Javaheri, A.; Garofalo, M.C.; Chmura, S.J.; Weichselbaum, R.T.; Kron, S.J. gamma-H2AX as a therapeutic target for improving the efficacy of radiation therapy. Curr. Cancer Drug Targets 2006, 6, 197–205. [Google Scholar] [CrossRef]
- Liang, K.; Lu, Y.; Jin, W.; Ang, K.K.; Milas, L.; Fan, Z. Sensitization of breast cancer cells to radiation by trastuzumab. Mol. Cancer Ther. 2003, 2, 1113–1120. [Google Scholar] [PubMed]
- Masaki, Y.; Shimizu, Y.; Yoshioka, T.; Tanaka, Y.; Nishijima, K.-I.; Zhao, S.; Higashino, K.; Sakamoto, S.; Numata, Y.; Yamaguchi, Y.; et al. The accumulation mechanism of the hypoxia imaging probe “FMISO” by imaging mass spectrometry: Possible involvement of low-molecular metabolites. Sci. Rep. 2015, 5, 16802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löck, S.; Linge, A.; Seidlitz, A.; Bandurska-Luque, A.; Nowak, A.; Gudziol, V.; Buchholz, F.; Aust, D.E.; Baretton, G.B.; Zöphel, K.; et al. Repeat FMISO-PET imaging weakly correlates with hypoxia-associated gene expressions for locally advanced HNSCC treated by primary radiochemotherapy. Radiother. Oncol. 2019, 135, 43–50. [Google Scholar] [CrossRef]
- Bekaert, L.; Valable, S.; Lechapt-Zalcman, E.; Ponte, K.; Collet, S.; Constans, J.-M.; Levallet, G.; Bordji, K.; Petit, E.; Branger, P.; et al. [18F]-FMISO PET study of hypoxia in gliomas before surgery: Correlation with molecular markers of hypoxia and angiogenesis. Eur. J. Pediatr. 2017, 44, 1383–1392. [Google Scholar] [CrossRef]
- Sorace, A.G.; Syed, A.K.; Barnes, S.L.; Quarles, C.C.; Sanchez, V.; Kang, H.; Yankeelov, T.E. Quantitative [18F]FMISO PET Imaging Shows Reduction of Hypoxia Fol-lowing Trastuzumab in a Murine Model of HER2+ Breast Cancer. Mol. Imaging Biol. 2017, 19, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Syed, A.K.; Woodall, R.; Whisenant, J.G.; Yankeelov, T.E.; Sorace, A.G. Characterizing Trastuzumab-Induced Alterations in Intratumoral Heterogeneity with Quantitative Imaging and Immunohistochemistry in HER2+ Breast Cancer. Neoplasia 2018, 21, 17–29. [Google Scholar] [CrossRef]
- Baylor College of Medicine. PDX Portal. 2022. Available online: https://pdxportal.research.bcm.edu/pdxportal/?dswid=-8886 (accessed on 28 January 2022).
- Wang, H.; Jiang, H.; Van De Gucht, M.; De Ridder, M. Hypoxic Radioresistance: Can ROS Be the Key to Overcome It? Cancers 2019, 11, 112. [Google Scholar] [CrossRef] [Green Version]
- Barnes, S.L.; Sorace, A.G.; Loveless, M.E.; Whisenant, J.G.; Yankeelov, T.E. Correlation of tumor characteristics derived from DCE-MRI and DW-MRI with histology in murine models of breast cancer. NMR Biomed. 2015, 28, 1345–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorace, A.G.; Quarles, C.C.; Whisenant, J.G.; Hanker, A.B.; McIntyre, J.O.; Sanchez, V.M.; Yankeelov, T.E. Trastuzumab improves tumor perfusion and vascular delivery of cytotoxic therapy in a murine model of HER2+ breast cancer: Preliminary results. Breast Cancer Res. Treat. 2016, 155, 273–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whisenant, J.G.; Sorace, A.G.; McIntyre, J.O.; Kang, H.; Sánchez, V.; Loveless, M.E.; Yankeelov, T.E. Evaluating treatment response using DW-MRI and DCE-MRI in trastuzumab responsive and resistant HER2-overexpressing human breast cancer xenografts. Transl. Oncol. 2014, 7, 768–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whisenant, J.G.; McIntyre, J.O.; Peterson, T.E.; Kang, H.; Sánchez, V.; Manning, H.C.; Arteaga, C.L.; Yankeelov, T.E. Utility of [18F]FLT-PET to assess treatment response in trastuzumab-resistant and trastuzumab-sensitive HER2-overexpressing human breast cancer xeno-grafts. Mol. Imaging Biol. 2015, 17, 119–128. [Google Scholar] [CrossRef] [Green Version]
- Shah, C.; Miller, T.W.; Wyatt, S.K.; McKinley, E.T.; Olivares, M.G.; Sanchez, V.; Nolting, D.D.; Buck, J.R.; Zhao, P.; Ansari, M.S.; et al. Imaging Biomarkers Predict Response to Anti-HER2 (ErbB2) Therapy in Preclinical Models of Breast Cancer. Clin. Cancer Res. 2009, 15, 4712–4721. [Google Scholar] [CrossRef] [Green Version]
- Jarrett, A.M.; Bloom, M.J.; Godfrey, W.; Syed, A.K.; A Ekrut, D.; I Ehrlich, L.; E Yankeelov, T.; Sorace, A.G. Mathematical modelling of trastuzumab-induced immune response in an in vivo murine model of HER2+ breast cancer. Math. Med. Biol. A J. IMA 2018, 36, 381–410. [Google Scholar] [CrossRef]
- Lu, Y.; Li, M.; Massicano, A.; Song, P.; Mansur, A.; Heinzman, K.; Larimer, B.; Lapi, S.; Sorace, A. [89Zr]-Pertuzumab PET Imaging Reveals Paclitaxel Treatment Efficacy Is Positively Correlated with HER2 Expression in Human Breast Cancer Xenograft Mouse Models. Molecules 2021, 26, 1568. [Google Scholar] [CrossRef]
- Syed, A.K.; Whisenant, J.G.; Barnes, S.L.; Sorace, A.G.; Yankeelov, T.E. Multiparametric Analysis of Longitudinal Quantitative MRI data to Identify Dis-tinct Tumor Habitats in Preclinical Models of Breast Cancer. Cancers 2020, 12, 1682. [Google Scholar] [CrossRef]
- Hanker, A.B.; Estrada, M.V.; Bianchini, G.; Moore, P.D.; Zhao, J.; Cheng, F.; Koch, J.P.; Gianni, L.; Tyson, D.R.; Sánchez, V.; et al. Extracellular Matrix/Integrin Signaling Promotes Resistance to Combined In-hibition of HER2 and PI3K in HER2(+) Breast Cancer. Cancer Res. 2017, 77, 3280–3292. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Claerhout, S.; Prat, A.; Dobrolecki, L.E.; Petrovic, I.; Lai, Q.; Landis, M.D.; Wiechmann, L.; Schiff, R.; Giuliano, M.; et al. A Renewable Tissue Resource of Phenotypically Stable, Biologically and Ethnically Diverse, Patient-Derived Human Breast Cancer Xenograft Models. Cancer Res. 2013, 73, 4885–4897. [Google Scholar] [CrossRef] [Green Version]
- Ewer, S.M.; Ewer, M.S. Cardiotoxicity Profile of Trastuzumab. Drug Saf. 2008, 31, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Mohan, N.; Jiang, J.; Dokmanovic, M.; Wu, W.J. Trastuzumab-mediated cardiotoxicity: Current understanding, challenges, and frontiers. Antib. Ther. 2018, 1, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Tian, Z.; Wei, H. Developmental and Functional Control of Natural Killer Cells by Cy-tokines. Front Immunol. 2017, 8, 930. [Google Scholar] [CrossRef] [PubMed]
- Benci, J.L.; Xu, B.; Qiu, Y.; Wu, T.J.; Dada, H.; Twyman-Saint Victor, C.; Cucolo, L.; Lee, D.S.M.; Pauken, K.E.; Huang, A.C.; et al. Tumor Interferon Signaling Regulates a Multigenic Resistance Program to Immune Checkpoint Blockade. Cell 2016, 167, 1540–1554. [Google Scholar] [CrossRef] [Green Version]
- Laky, K.; Kruisbeek, A.M. In vivo Depletion of T Lymphocytes. Curr. Protoc. Immunol. 2016, 113, 411–419. [Google Scholar] [CrossRef]
- Institute, T.B. Cancer Cell Line Encyclopedia. 2017. Available online: https://sites.broadinstitute.org/ccle/ (accessed on 28 January 2022).
- Lim, J.-L.; Berridge, M.S. An efficient radiosynthesis of [18F]fluoromisonidazole. Appl. Radiat. Isot. 1993, 44, 1085–1091. [Google Scholar] [CrossRef]
- Tang, G.; Wang, M.; Tang, X.; Gan, M.; Luo, L. Fully automated one-pot synthesis of [18F]fluoromisonidazole. Nucl. Med. Biol. 2005, 32, 553–558. [Google Scholar] [CrossRef]
- Kelada, O.J.; Rockwell, S.; Zheng, M.Q.; Huang, Y.; Liu, Y.; Booth, C.J.; Decker, R.H.; Oelfke, U.; Carson, R.E.; Carlson, D.J. Quantification of Tumor Hypoxic Fractions Using Positron Emission Tomog-raphy with [18F]Fluoromisonidazole ([18F]FMISO) Kinetic Analysis and Invasive Oxygen Measurements. Mol. Imaging Biol. 2017, 19, 893–902. [Google Scholar] [CrossRef] [Green Version]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, P.N.; Mansur, A.; Lu, Y.; Della Manna, D.; Burns, A.; Samuel, S.; Heinzman, K.; Lapi, S.E.; Yang, E.S.; Sorace, A.G. Modulation of the Tumor Microenvironment with Trastuzumab Enables Radiosensitization in HER2+ Breast Cancer. Cancers 2022, 14, 1015. https://doi.org/10.3390/cancers14041015
Song PN, Mansur A, Lu Y, Della Manna D, Burns A, Samuel S, Heinzman K, Lapi SE, Yang ES, Sorace AG. Modulation of the Tumor Microenvironment with Trastuzumab Enables Radiosensitization in HER2+ Breast Cancer. Cancers. 2022; 14(4):1015. https://doi.org/10.3390/cancers14041015
Chicago/Turabian StyleSong, Patrick N., Ameer Mansur, Yun Lu, Deborah Della Manna, Andrew Burns, Sharon Samuel, Katherine Heinzman, Suzanne E. Lapi, Eddy S. Yang, and Anna G. Sorace. 2022. "Modulation of the Tumor Microenvironment with Trastuzumab Enables Radiosensitization in HER2+ Breast Cancer" Cancers 14, no. 4: 1015. https://doi.org/10.3390/cancers14041015