
A Single Dose of Novel PSMA-Targeting Radiopharmaceutical Agent [177Lu]Ludotadipep for Patients with Metastatic Castration-Resistant Prostate Cancer: Phase I Clinical Trial
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
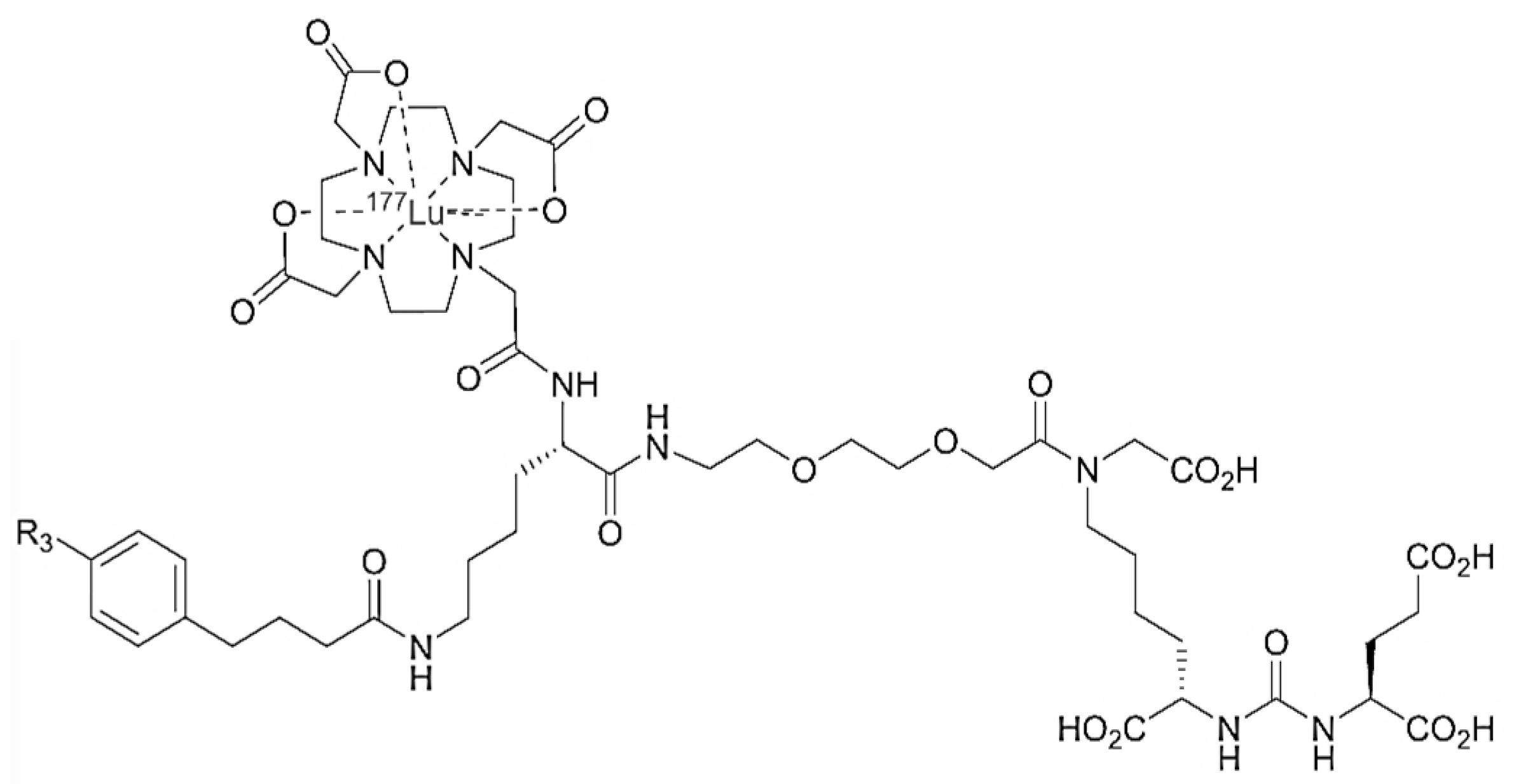
2.1. [177Lu]Ludotadipep
2.2. PSMA PET/CT
2.3. Study Method
2.4. Outcomes
2.5. Statistical Analysis
2.6. Ethical Statement
3. Results
3.1. Patient Characteristics
3.2. Treatment Related Toxicity
3.3. Laboratory Changes
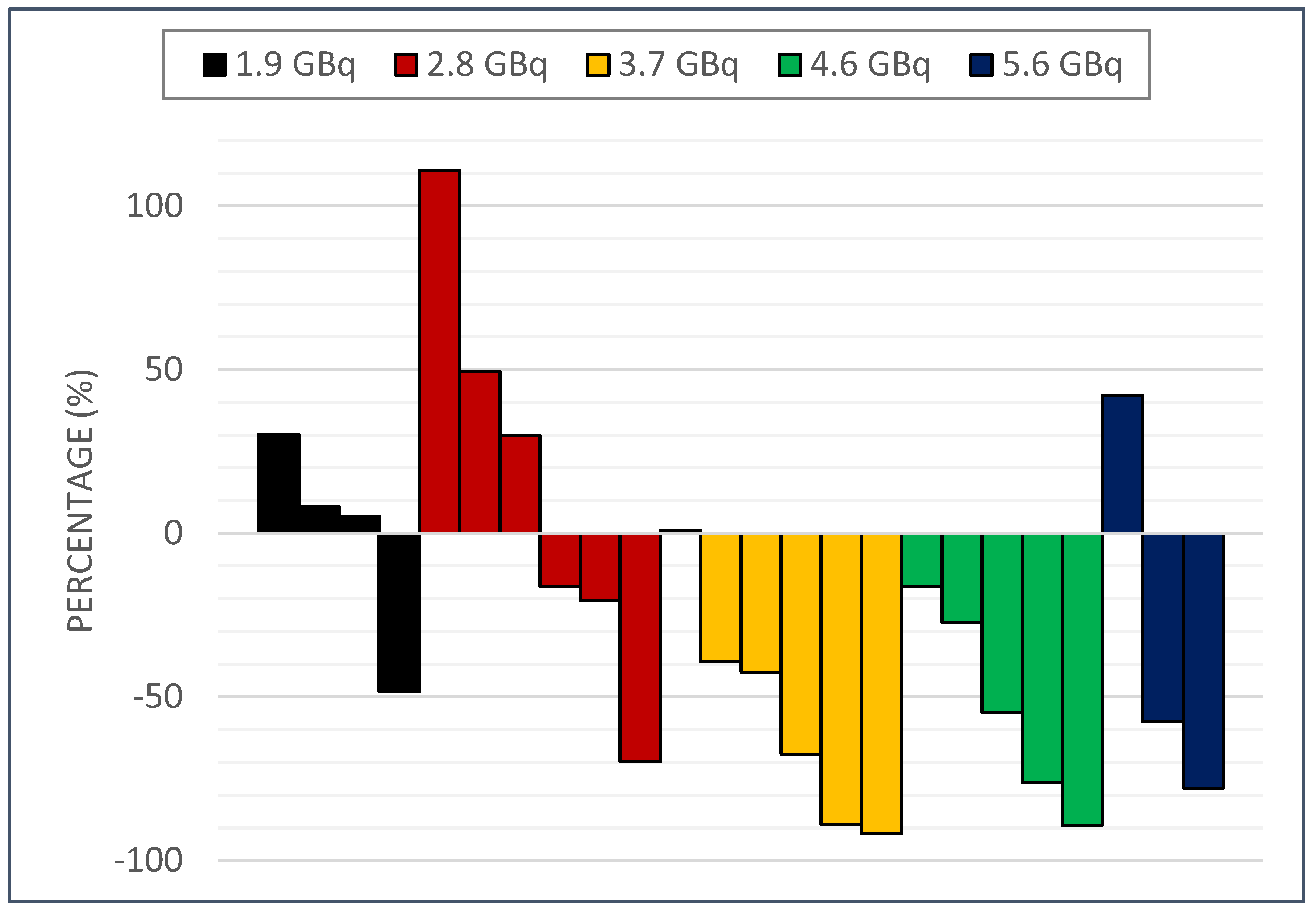
3.4. PSA Response
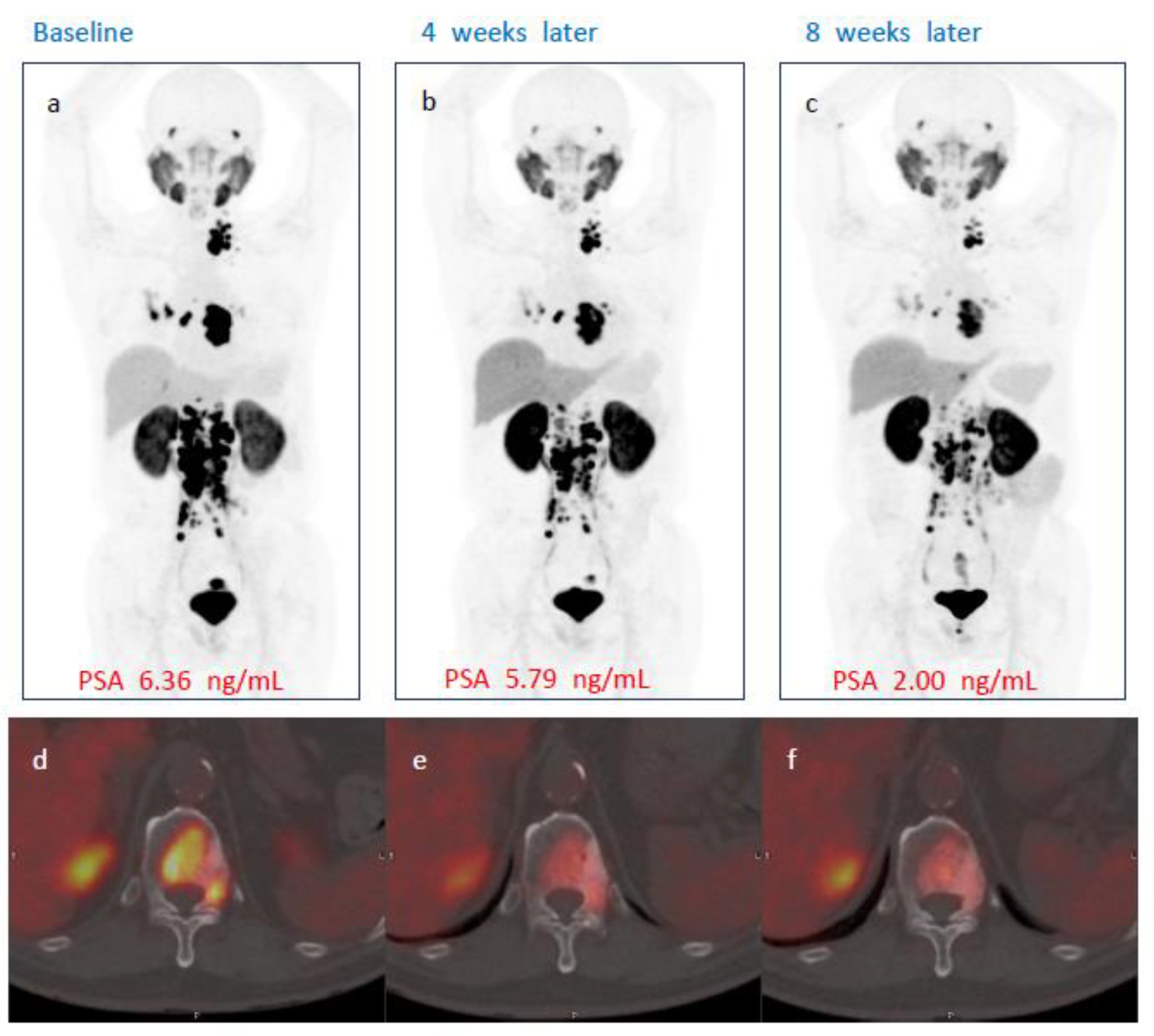
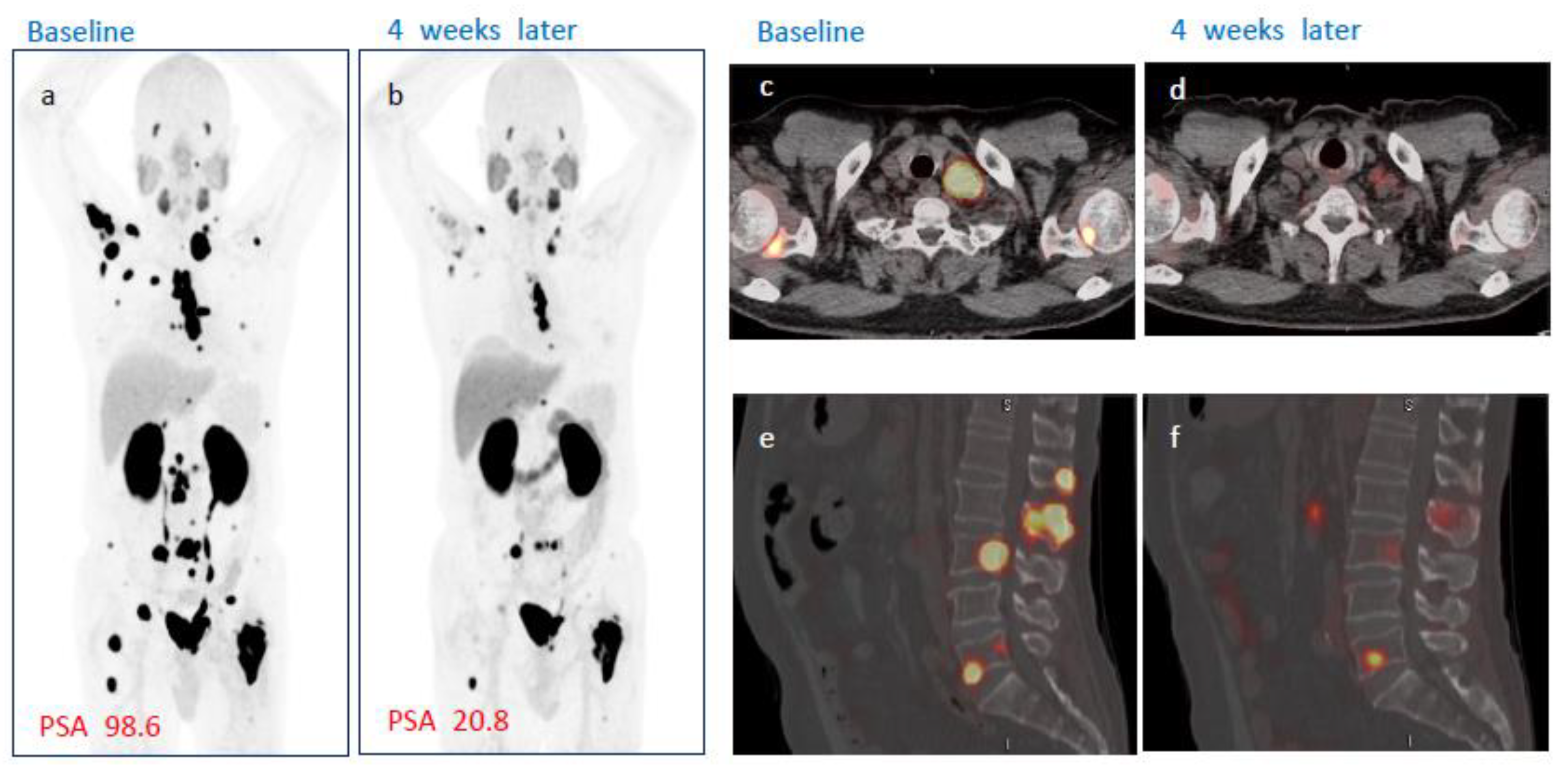
3.5. Radiological Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Broeck, T.; Van Den Bergh, R.C.N.; Arfi, N.; Gross, T.; Moris, L.; Briers, E.; Cumberbatch, M.; De Santis, M.; Tilki, D.; Fanti, S.; et al. Prognostic value of biochemical recurrence following treatment with curative intent for prostate cancer: A systematic review. Eur. Urol. 2019, 75, 967–987. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, W.P.; Mostaghel, E.A.; Nelson, P.S.; Montgomery, B. Androgen deprivation therapy: Progress in understanding mechanisms of resistance and optimizing androgen depletion. Nat. Clin. Pract. Urol. 2009, 6, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Sella, A.; Yarom, N.; Zisman, A.; Kovel, S. Paclitaxel, estramustine and carboplatin combination chemotherapy after initial docetaxel-based chemotherapy in castration-resistant prostate cancer. Oncology 2009, 76, 442–446. [Google Scholar] [CrossRef] [PubMed]
- Kirby, M.; Hirst, C.; Crawford, E.D. Characterising the castration-resistant prostate cancer population: A systematic review. Int. J. Clin. Pract. 2011, 65, 1180–1192. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Su, Y.; Zhu, Y.; Markowski, M.C.; Xin, M.; Gorin, M.A.; Dong, B.; Pan, J.; Pomper, M.G.; Liu, J.; et al. The European Association of Urology biochemical recurrence risk groups predict findings on PSMA PET in patients with biochemically recurrent prostate cancer after radical prostatectomy. J. Nucl. Med. 2022, 63, 248–252. [Google Scholar] [CrossRef]
- Neale, J.H.; Yamamoto, T. N-acetylaspartylglutamate (NAAG) and glutamate carboxypeptidase II: An abundant peptide neurotransmitter-enzyme system with multiple clinical applications. Prog. Neurobiol. 2020, 184, 101722. [Google Scholar] [CrossRef] [PubMed]
- Bakht, M.K.; Hayward, J.J.; Shahbazi-Raz, F.; Skubal, M.; Tamura, R.; Stringer, K.F.; Meister, D.; Venkadakrishnan, V.B.; Xue, H.; Pillon, A.; et al. Identification of alternative protein targets of glutamate-ureido-lysine associated with PSMA tracer uptake in prostate cancer cells. Proc. Natl. Acad. Sci. USA 2022, 119, e2025710119. [Google Scholar] [CrossRef]
- Ferdinandus, J.; Violet, J.; Sandhu, S.; Hofman, M.S. Prostate-specific membrane antigen theranostics: Therapy with lutetium-177. Curr. Opin. Urol. 2018, 28, 197–204. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S. [177Lu] Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Sartor, O.; De Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G. Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. New Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Lisney, A.R.; Leitsmann, C.; Strauß, A.; Meller, B.; Bucerius, J.A.; Sahlmann, C.-O. The Role of PSMA PET/CT in the Primary Diagnosis and Follow-Up of Prostate Cancer—A Practical Clinical Review. Cancers 2022, 14, 3638. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.W.; Suh, M.; Cheon, G.J. Current Status of PSMA-Targeted Radioligand Therapy in the Era of Radiopharmaceutical Therapy Acquiring Marketing Authorization. Nucl. Med. Mol. Imaging 2022, 56, 263–281. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.S.; Kim, M.H.; Chu, S.Y.; Jung, W.J.; Jeong, H.J.; Lee, K.; Kim, H.S.; Kim, M.H.; Kil, H.S.; Han, S.J.; et al. Improving Theranostic Gallium-68/Lutetium-177–Labeled PSMA Inhibitors with an Albumin Binder for Prostate CancerA Novel 177Lu-PSMA Ligand for Prostate Cancer Therapy. Mol. Cancer Ther. 2021, 20, 2410–2419. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.; Lim, I.; Byun, B.H.; Kim, B.I.; Choi, C.W.; Woo, S.-K.; Lee, K.C.; Kang, J.H.; Kil, H.S.; Park, C.; et al. A microdose clinical trial to evaluate [18F] Florastamin as a positron emission tomography imaging agent in patients with prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.P.; Pienta, K.J.; Pomper, M.G.; Gorin, M.A. PSMA-RADS version 1.0: A step towards standardizing the interpretation and reporting of PSMA-targeted PET imaging studies. Eur. Urol. 2018, 73, 485–487. [Google Scholar] [CrossRef]
- Tagawa, S.T.; Vallabhajosula, S.; Christos, P.J.; Jhanwar, Y.S.; Batra, J.S.; Lam, L.; Osborne, J.; Beltran, H.; Molina, A.M.; Goldsmith, S.J.; et al. Phase 1/2 study of fractionated dose lutetium-177–labeled anti–prostate-specific membrane antigen monoclonal antibody J591 (177Lu-J591) for metastatic castration-resistant prostate cancer. Cancer 2019, 125, 2561–2569. [Google Scholar] [CrossRef]
- Zang, J.; Fan, X.; Wang, H.; Liu, Q.; Wang, J.; Li, H.; Li, F.; Jacobson, O.; Niu, G.; Zhu, Z.; et al. First-in-human study of 177Lu-EB-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 148–158. [Google Scholar] [CrossRef]
- Kratochwil, C.; Giesel, F.L.; Stefanova, M.; Benešová, M.; Bronzel, M.; Afshar-Oromieh, A.; Mier, W.; Eder, M.; Kopka, K.; Haberkorn, U. PSMA-targeted radionuclide therapy of metastatic castration-resistant prostate cancer with 177Lu-labeled PSMA-617. J. Nucl. Med. 2016, 57, 1170–1176. [Google Scholar] [CrossRef] [Green Version]
- Bergsma, H.; Konijnenberg, M.W.; van der Zwan, W.A.; Kam, B.L.; Teunissen, J.J.; Kooij, P.P.; Mauff, K.A.; Krenning, E.P.; Kwekkeboom, D.J. Nephrotoxicity after PRRT with 177Lu-DOTA-octreotate. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1802–1811. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Francis, R.J. TheraP: 177Lu-PSMA-617 (LuPSMA) Versus Cabazitaxel in Metastatic Castration-Resistant Prostate Cancer (mCRPC) Progressing after Docetaxel—Overall Survival after Median Follow-Up of 3 Years (ANZUP 1603); American Society of Clinical Oncology: Chicago, IL, USA, 2022. [Google Scholar]
- Van Kalmthout, L.W.M.; van der Sar, E.C.A.; Braat, A.J.A.T.; de Keizer, B.; Lam, M.G.E.H. Lutetium-177-PSMA therapy for prostate cancer patients-a brief overview of the literature. Tijdschr. Voor Urol. 2020, 10, 141–146. [Google Scholar] [CrossRef]
- Baum, R.P.; Kulkarni, H.R.; Schuchardt, C.; Singh, A.; Wirtz, M.; Wiessalla, S.; Schottelius, M.; Mueller, D.; Klette, I.; Wester, H.-J. Lutetium-177 PSMA radioligand therapy of metastatic castration-resistant prostate cancer: Safety and efficacy. J. Nucl. Med. 2016, 57, 1006–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heynickx, N.; Herrmann, K.; Vermeulen, K.; Baatout, S.; Aerts, A. The salivary glands as a dose limiting organ of PSMA-targeted radionuclide therapy: A review of the lessons learnt so far. Nucl. Med. Biol. 2021, 98–99, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Van Kalmthout, L.W.M.; Lam, M.G.E.H.; de Keizer, B.; Krijger, G.C.; Ververs, T.F.T.; de Roos, R.; Braat, A.J.A.T. Impact of external cooling with icepacks on 68Ga-PSMA uptake in salivary glands. EJNMMI Res. 2018, 8, 56. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | N = 29 |
|---|---|
| Age (years) | 72.7 ± 8.1 |
| Time from prostate cancer diagnosis (months) | 67.0 ± 50.8 |
| ECOG Performance Status | |
| 0 | 26 (89.6%) |
| 1 | 3 (10.34%) |
| PSA (ng/mL) | 681.3 ± 1139.9 |
| Gleason Score | |
| 3 + 4 | 2 (6.9%) |
| 4 + 3 | 2 (6.9%) |
| 4 + 4 | 9 (31.0%) |
| 4 + 5 | 9 (31.0%) |
| 5 + 4 | 5 (17.2%) |
| 5 + 5 | 2 (6.9%) |
| Bone metastasis | 28 (96.6%) |
| Lymph node metastasis | 18 (62.1%) |
| Liver metastasis | 4 (13.8%) |
| Lung metastasis | 5 (17.2%) |
| Radical prostatectomy | 16 (55.2%) |
| Radiation Therapy | 7 (24.1%) |
| Prior Systemic Treatment | |
| Androgen deprivation therapy only | 7 (24.1%) |
| Docetaxel | 3 (10.3%) |
| Abiraterone | 7 (24.1%) |
| Enzalutamide | 1 (3.4%) |
| Docetaxel then enzalutamide | 4 (13.8%) |
| Docetaxel then abiraterone | 3 (10.3%) |
| Degarelix then androgen deprivation therapy | 1 (3.4%) |
| Abiraterone then docetaxel then enzalutamide | 3 (10.3%) |
| AEs/Dose | 1.9 GBq | 2.8 GBq | 3.7 GBq | 4.6 GBq | 5.6 GBq |
|---|---|---|---|---|---|
| (N = 6) | (N = 6) | (N = 6) | (N = 6) | (N = 5) | |
| Hematologic | |||||
| Neutropenia | 0 | 0 | 0 | 0 | 0 |
| Febrile neutropenia | 0 | 0 | 0 | 0 | 0 |
| Anemia | 1 (16.7%) | 0 | 1 (16.7%) | 0 | 1 (20.0%) |
| Thrombocytopenia | 0 | 0 | 0 | 0 | 0 |
| Non-hematologic | |||||
| Anorexia | 0 | 1 (16.7%) | 1 (16.7%) | 0 | 1 (20.0%) |
| Dyspnea | 0 | 0 | 0 | 0 | 0 |
| Fatigue | 0 | 0 | 0 | 0 | 0 |
| Nausea | 1 (16.7%) | 1 (16.7%) | 1 (16.7%) | 0 | 2 (40.0%) |
| Stomatitis | 0 | 0 | 0 | 0 | 0 |
| Vomiting | 0 | 0 | 0 | 0 | 0 |
| Weight loss | 0 | 0 | 0 | 0 | 0 |
| Constipation | 0 | 0 | 0 | 1 (16.7%) | 1 (16.7%) |
| Xerostomia | 1 (16.7%) | 1 (16.7%) | 1 (16.7%) | 1 (16.7%) | 2 (20.0%) |
| Total 29 Subjects | |
|---|---|
| Subjects with TEAEs, n(%) [number of events] | 17(58.6) [36] |
| Gastrointestinal disorders | 6(20.7) [8] |
| Nausea | 5(17.2) [5] |
| Constipation | 2(6.9) [2] |
| Hematochezia | 1(3.5) [1] |
| Blood and lymphatic system disorders | 3(10.3) [3] |
| Anemia | 3(10.3) [3] |
| Laboratory investigations | 3(10.3) [3] |
| Alanine aminotransferase increased | 1(3.5) [1] |
| Aspartate aminotransferase increased | 1(3.5) [1] |
| Platelet count decreased | 1(3.5) [1] |
| Metabolism and nutrition disorders | 3(10.3) [3] |
| Decreased appetite | 3(10.3) [3] |
| Nervous system disorders | 3(10.3) [3] |
| Headache | 2(6.9) [2] |
| Dizziness | 1(3.5) [1] |
| General disorders and administration site conditions | 2(6.9) [3] |
| Edema peripheral | 1(3.5) [2] |
| Asthenia | 1(3.5) [1] |
| Psychiatric disorders | 1(3.5) [2] |
| Insomnia | 1(3.5) [2] |
| Injury, poisoning and procedural complications | 1(3.5) [1] |
| Procedural pain | 1(3.5) [1] |
| Musculoskeletal and connective tissue disorders | 2(6.9) [1] |
| Bone pain | 1(3.5) [1] |
| Arthralgia | 1(3.5) [1] |
| Renal and urinary disorders | 1(3.5) [1] |
| Dysuria | 1(3.5) [1] |
| Reproductive system and breast disorders | 1(3.5) [1] |
| Scrotal pain | 1(3.5) [1] |
| Dry mouth | 6(20.7) [6] |
| Skin and subcutaneous tissue disorders | 1(3.5) [1] |
| Dermatitis | 1(3.5) [1] |
| Total 29 Subjects | |
|---|---|
| Subjects with ADRs, n(%) [number of events] | 3(10.3) [4] |
| Gastrointestinal disorders | |
| Nausea | 2(6.9) [2] |
| Metabolism and nutrition disorders | |
| Decreased appetite | 1(3.5) [1] |
| Skin and subcutaneous tissue disorders | |
| Dermatitis | 1(3.5) [1] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, D.; Ha, S.; O, J.H.; Rhew, S.a.; Yoon, C.E.; Kwon, H.J.; Moon, H.W.; Park, Y.H.; Park, S.Y.; Park, C.; et al. A Single Dose of Novel PSMA-Targeting Radiopharmaceutical Agent [177Lu]Ludotadipep for Patients with Metastatic Castration-Resistant Prostate Cancer: Phase I Clinical Trial. Cancers 2022, 14, 6225. https://doi.org/10.3390/cancers14246225
Shin D, Ha S, O JH, Rhew Sa, Yoon CE, Kwon HJ, Moon HW, Park YH, Park SY, Park C, et al. A Single Dose of Novel PSMA-Targeting Radiopharmaceutical Agent [177Lu]Ludotadipep for Patients with Metastatic Castration-Resistant Prostate Cancer: Phase I Clinical Trial. Cancers. 2022; 14(24):6225. https://doi.org/10.3390/cancers14246225
Chicago/Turabian StyleShin, Dongho, Seunggyun Ha, Joo Hyun O, Seung ah Rhew, Chang Eil Yoon, Hyeok Jae Kwon, Hyong Woo Moon, Yong Hyun Park, Sonya Youngju Park, Chansoo Park, and et al. 2022. "A Single Dose of Novel PSMA-Targeting Radiopharmaceutical Agent [177Lu]Ludotadipep for Patients with Metastatic Castration-Resistant Prostate Cancer: Phase I Clinical Trial" Cancers 14, no. 24: 6225. https://doi.org/10.3390/cancers14246225