
TP53 Co-Mutation Status Association with Clinical Outcomes in Patients with EGFR-Mutant Non-Small Cell Lung Cancer

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
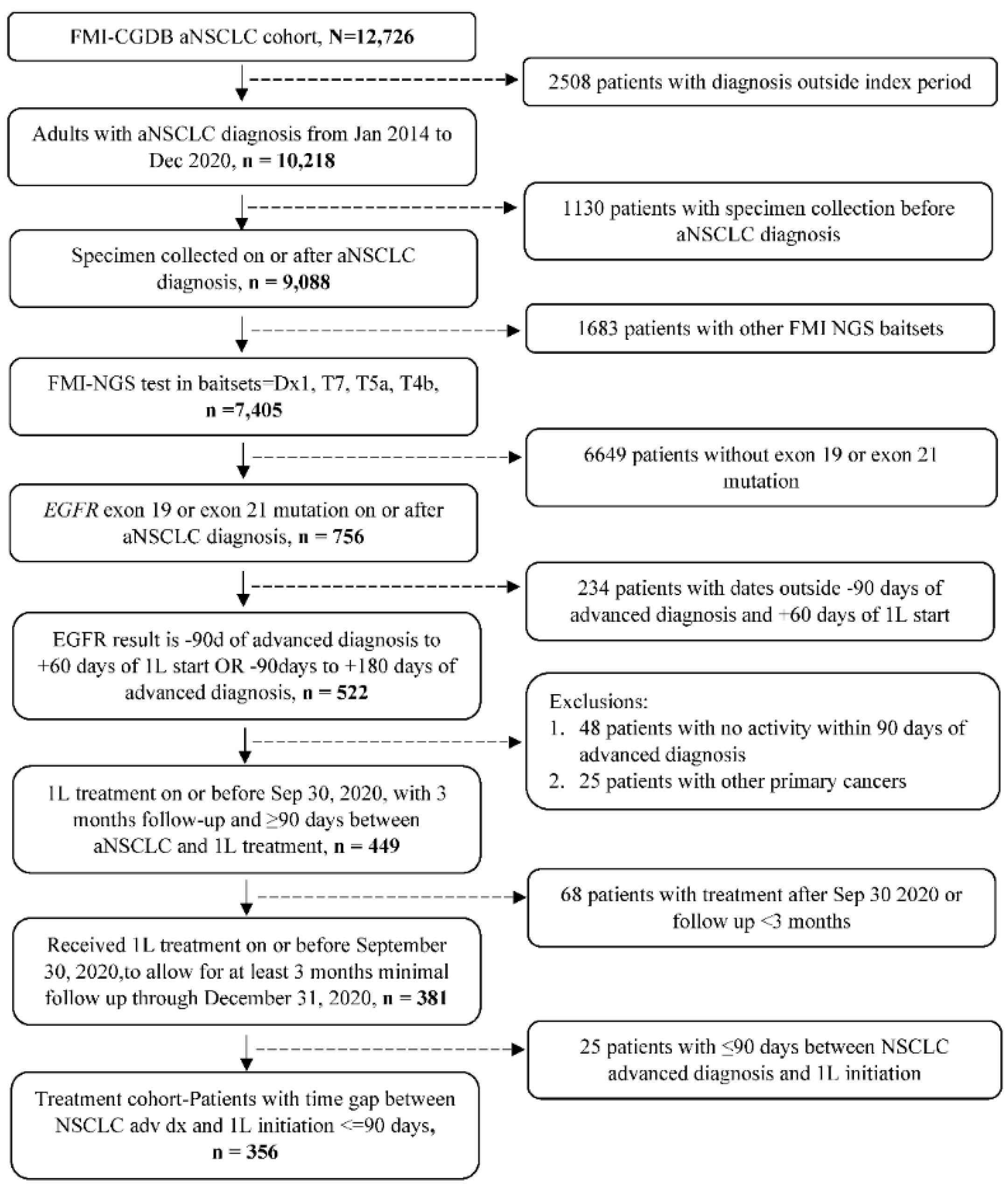
2.1. Study Design and Patients
2.2. End Points
2.3. Statistical Analysis
3. Results
3.1. Baseline Demographics and Clinical Characteristics
3.2. Treatments Received
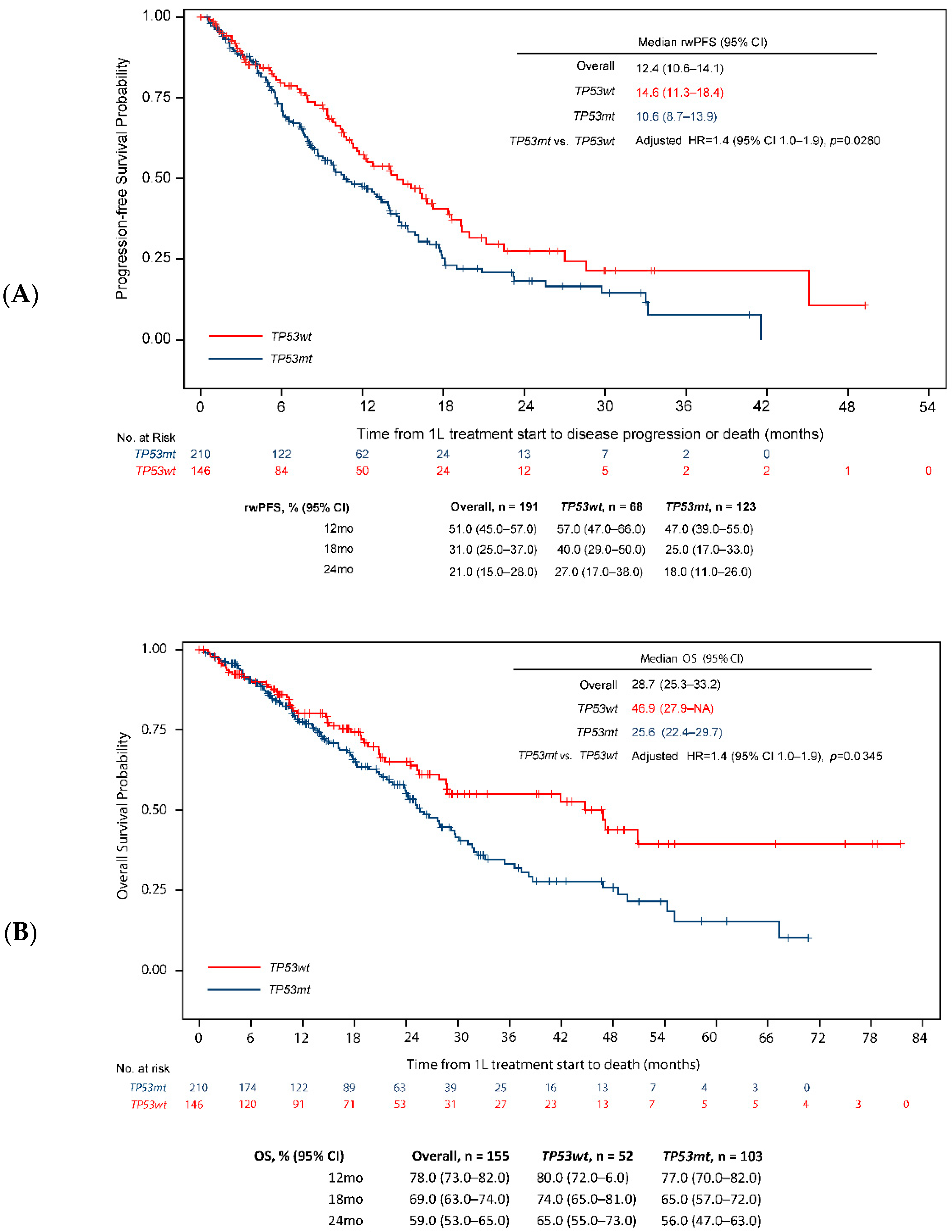
3.3. Survival End Points
3.4. Tumor Response
3.5. Subgroup Analysis
3.5.1. EGFR Mutation Subtype
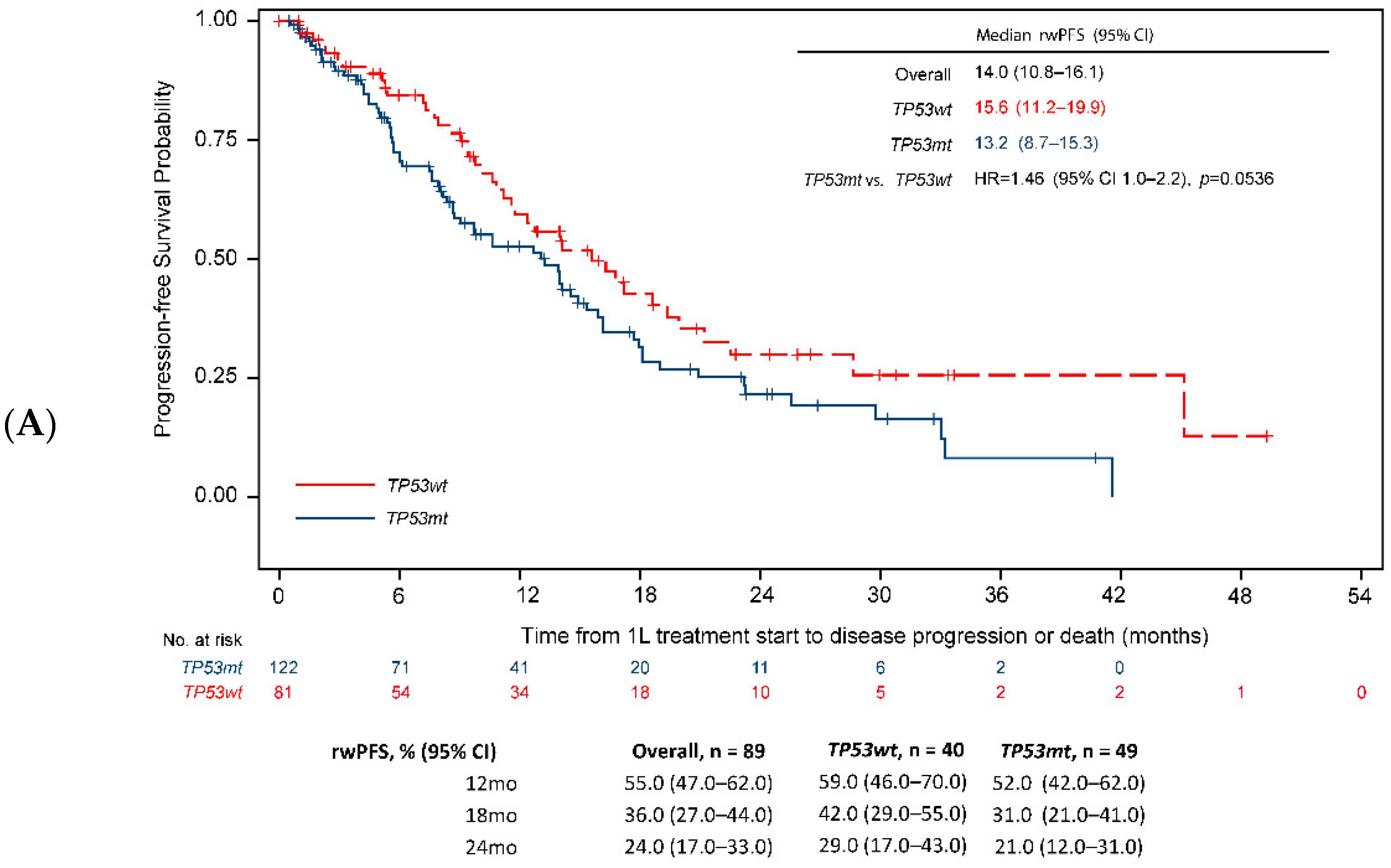
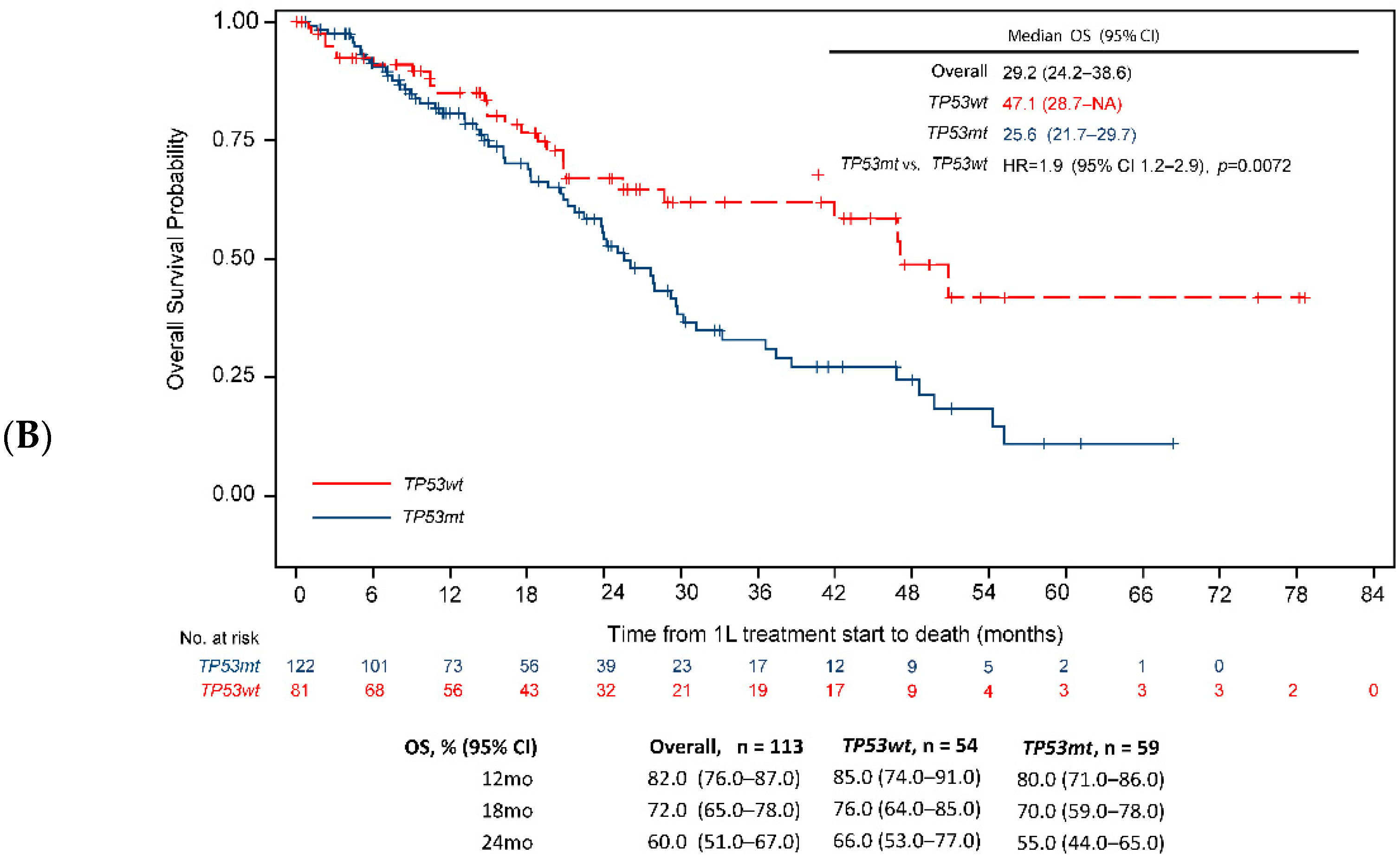
3.5.2. EGFR-TKI Monotherapy
3.5.3. EGFR-TKI Generation
3.5.4. Non-EGFR-TKI Monotherapy Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dearden, S.; Stevens, J.; Wu, Y.L.; Blowers, D. Mutation incidence and coincidence in non small-cell lung cancer: Meta-analyses by ethnicity and histology (mutMap). Ann. Oncol. 2013, 24, 2371–2376. [Google Scholar] [CrossRef] [PubMed]
- Midha, A.; Dearden, S.; McCormack, R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Harrison, P.T.; Vyse, S.; Huang, P.H. Rare epidermal growth factor receptor (EGFR) mutations in non-small cell lung cancer. Semin. Cancer Biol. 2020, 61, 167–179. [Google Scholar] [CrossRef]
- Robichaux, J.P.; Le, X.; Vijayan, R.S.K.; Hicks, J.K.; Heeke, S.; Elamin, Y.Y.; Lin, H.Y.; Udagawa, H.; Skoulidis, F.; Tran, H.; et al. Structure-based classification predicts drug response in EGFR-mutant NSCLC. Nature 2021, 597, 732–737. [Google Scholar] [CrossRef]
- Langer, C.J. Epidermal growth factor receptor inhibition in mutation-positive non-small-cell lung cancer: Is afatinib better or simply newer? J. Clin. Oncol. 2013, 31, 3303–3306. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Non-Small Cell Lung Cancer (Version 3.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (accessed on 3 May 2022).
- Hanna, N.H.; Robinson, A.G.; Temin, S.; Baker, S., Jr.; Brahmer, J.R.; Ellis, P.M.; Gaspar, L.E.; Haddad, R.Y.; Hesketh, P.J.; Jain, D.; et al. Therapy for Stage IV Non-Small-Cell Lung Cancer With Driver Alterations: ASCO and OH (CCO) Joint Guideline Update. J. Clin. Oncol. 2021, 39, 1040–1091. [Google Scholar] [CrossRef]
- Nakagawa, K.; Garon, E.B.; Seto, T.; Nishio, M.; Aix, S.P.; Paz-Ares, L.; Chiu, C.H.; Park, K.; Novello, S.; Nadal, E.; et al. Ramucirumab plus erlotinib in patients with untreated, EGFR-mutated, advanced non-small-cell lung cancer (RELAY): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 1655–1669. [Google Scholar] [CrossRef] [Green Version]
- Passaro, A.; Janne, P.A.; Mok, T.; Peters, S. Overcoming therapy resistance in EGFR-mutant lung cancer. Nat. Cancer 2021, 2, 377–391. [Google Scholar] [CrossRef]
- Yu, H.A.; Arcila, M.E.; Rekhtman, N.; Sima, C.S.; Zakowski, M.F.; Pao, W.; Kris, M.G.; Miller, V.A.; Ladanyi, M.; Riely, G.J. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin. Cancer Res. 2013, 19, 2240–2247. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.; Wu, Y.L.; Schuler, M.; Sebastian, M.; Popat, S.; Yamamoto, N.; Zhou, C.; Hu, C.P.; O’Byrne, K.; Feng, J.; et al. Afatinib versus cisplatin-based chemotherapy for EGFR mutation-positive lung adenocarcinoma (LUX-Lung 3 and LUX-Lung 6): Analysis of overall survival data from two randomised, phase 3 trials. Lancet Oncol. 2015, 16, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Jackman, D.; Pao, W.; Riely, G.J.; Engelman, J.A.; Kris, M.G.; Janne, P.A.; Lynch, T.; Johnson, B.E.; Miller, V.A. Clinical definition of acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 357–360. [Google Scholar] [CrossRef] [PubMed]
- Takezawa, K.; Pirazzoli, V.; Arcila, M.E.; Nebhan, C.A.; Song, X.; De Stanchina, E.; Ohashi, K.; Janjigian, Y.Y.; Spitzler, P.J.; Melnick, M.A.; et al. HER2 amplification: A potential mechanism of acquired resistance to EGFR inhibition in EGFR-mutant lung cancers that lack the second-site EGFRT790M mutation. Cancer Discov. 2012, 2, 922–933. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Loriot, Y.; Andre, F.; Gobert, A.; Auger, N.; Lacroix, L.; Soria, J.C. EGFR-independent mechanisms of acquired resistance to AZD9291 in EGFR T790M-positive NSCLC patients. Ann. Oncol. 2015, 26, 2073–2078. [Google Scholar] [CrossRef]
- Papadimitrakopoulou, V.A.; Mok, T.S.; Han, J.Y.; Ahn, M.J.; Delmonte, A.; Ramalingam, S.S.; Kim, S.W.; Shepherd, F.A.; Laskin, J.; He, Y.; et al. Osimertinib versus platinum-pemetrexed for patients with EGFR T790M advanced NSCLC and progression on a prior EGFR-tyrosine kinase inhibitor: AURA3 overall survival analysis. Ann. Oncol. 2020, 31, 1536–1544. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Le, X.; Puri, S.; Negrao, M.V.; Nilsson, M.B.; Robichaux, J.; Boyle, T.; Hicks, J.K.; Lovinger, K.L.; Roarty, E.; Rinsurongkawong, W.; et al. Landscape of EGFR-Dependent and -Independent Resistance Mechanisms to Osimertinib and Continuation Therapy Beyond Progression in EGFR-Mutant NSCLC. Clin. Cancer Res. 2018, 24, 6195–6203. [Google Scholar] [CrossRef] [PubMed]
- Teodoro, J.G.; Evans, S.K.; Green, M.R. Inhibition of tumor angiogenesis by p53: A new role for the guardian of the genome. J. Mol. Med. 2007, 85, 1175–1186. [Google Scholar] [CrossRef] [PubMed]
- Boutelle, A.M.; Attardi, L.D. p53 and Tumor Suppression: It Takes a Network. Trends Cell Biol. 2021, 31, 298–310. [Google Scholar] [CrossRef] [PubMed]
- Poeta, M.L.; Manola, J.; Goldwasser, M.A.; Forastiere, A.; Benoit, N.; Califano, J.A.; Ridge, J.A.; Goodwin, J.; Kenady, D.; Saunders, J.; et al. TP53 mutations and survival in squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2007, 357, 2552–2561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamid, A.B.; Petreaca, R.C. Secondary Resistant Mutations to Small Molecule Inhibitors in Cancer Cells. Cancers 2020, 12, 927. [Google Scholar] [CrossRef] [Green Version]
- Jao, K.; Tomasini, P.; Kamel-Reid, S.; Korpanty, G.J.; Mascaux, C.; Sakashita, S.; Labbe, C.; Leighl, N.B.; Liu, G.; Feld, R.; et al. The prognostic effect of single and multiple cancer-related somatic mutations in resected non-small-cell lung cancer. Lung Cancer 2018, 123, 22–29. [Google Scholar] [CrossRef]
- Hafner, A.; Bulyk, M.L.; Jambhekar, A.; Lahav, G. The multiple mechanisms that regulate p53 activity and cell fate. Nat. Rev. Mol. Cell. Biol. 2019, 20, 199–210. [Google Scholar] [CrossRef]
- Qin, K.; Hou, H.; Liang, Y.; Zhang, X. Prognostic value of TP53 concurrent mutations for EGFR- TKIs and ALK-TKIs based targeted therapy in advanced non-small cell lung cancer: A meta-analysis. BMC Cancer 2020, 20, 328. [Google Scholar] [CrossRef]
- Zhou, G.; Liu, Z.; Myers, J.N. TP53 Mutations in Head and Neck Squamous Cell Carcinoma and Their Impact on Disease Progression and Treatment Response. J. Cell. Biochem. 2016, 117, 2682–2692. [Google Scholar] [CrossRef] [Green Version]
- Molina-Vila, M.A.; Bertran-Alamillo, J.; Gasco, A.; Mayo-de-las-Casas, C.; Sanchez-Ronco, M.; Pujantell-Pastor, L.; Bonanno, L.; Favaretto, A.G.; Cardona, A.F.; Vergnenegre, A.; et al. Nondisruptive p53 mutations are associated with shorter survival in patients with advanced non-small cell lung cancer. Clin. Cancer Res. 2014, 20, 4647–4659. [Google Scholar] [CrossRef] [Green Version]
- Canale, M.; Petracci, E.; Delmonte, A.; Chiadini, E.; Dazzi, C.; Papi, M.; Capelli, L.; Casanova, C.; De Luigi, N.; Mariotti, M.; et al. Impact of TP53 Mutations on Outcome in EGFR-Mutated Patients Treated with First-Line Tyrosine Kinase Inhibitors. Clin. Cancer Res. 2017, 23, 2195–2202. [Google Scholar] [CrossRef]
- Canale, M.; Petracci, E.; Delmonte, A.; Bronte, G.; Chiadini, E.; Ludovini, V.; Dubini, A.; Papi, M.; Baglivo, S.; De Luigi, N.; et al. Concomitant TP53 Mutation Confers Worse Prognosis in EGFR-Mutated Non-Small Cell Lung Cancer Patients Treated with TKIs. J. Clin. Med. 2020, 9, 1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aggarwal, C.; Davis, C.W.; Mick, R.; Thompson, J.C.; Ahmed, S.; Jeffries, S.; Bagley, S.; Gabriel, P.; Evans, T.L.; Bauml, J.M.; et al. Influence of TP53 Mutation on Survival in Patients with Advanced EGFR-Mutant Non-Small-Cell Lung Cancer. JCO Precis Oncol. 2018, 2, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Scoccianti, C.; Vesin, A.; Martel, G.; Olivier, M.; Brambilla, E.; Timsit, J.F.; Tavecchio, L.; Brambilla, C.; Field, J.K.; Hainaut, P.; et al. Prognostic value of TP53, KRAS and EGFR mutations in nonsmall cell lung cancer: The EUELC cohort. Eur. Respir. J. 2012, 40, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Le Teuff, G.; Lacas, B.; Tsao, M.S.; Graziano, S.; Pignon, J.P.; Douillard, J.Y.; Le Chevalier, T.; Seymour, L.; Filipits, M.; et al. Prognostic and Predictive Effect of TP53 Mutations in Patients with Non-Small Cell Lung Cancer from Adjuvant Cisplatin-Based Therapy Randomized Trials: A LACE-Bio Pooled Analysis. J. Thorac. Oncol. 2016, 11, 850–861. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Rousseau, V.; Sun, H.; Lantuejoul, S.; Filipits, M.; Pirker, R.; Popper, H.; Mendiboure, J.; Vataire, A.L.; Le Chevalier, T.; et al. Significance of TP53 mutations as predictive markers of adjuvant cisplatin-based chemotherapy in completely resected non-small-cell lung cancer. Mol. Oncol. 2014, 8, 555–564. [Google Scholar] [CrossRef]
- Shepherd, F.A.; Lacas, B.; Le Teuff, G.; Hainaut, P.; Janne, P.A.; Pignon, J.P.; Le Chevalier, T.; Seymour, L.; Douillard, J.Y.; Graziano, S.; et al. Pooled Analysis of the Prognostic and Predictive Effects of TP53 Comutation Status Combined With KRAS or EGFR Mutation in Early-Stage Resected Non-Small-Cell Lung Cancer in Four Trials of Adjuvant Chemotherapy. J. Clin. Oncol. 2017, 35, 2018–2027. [Google Scholar] [CrossRef] [PubMed]
- Labbe, C.; Cabanero, M.; Korpanty, G.J.; Tomasini, P.; Doherty, M.K.; Mascaux, C.; Jao, K.; Pitcher, B.; Wang, R.; Pintilie, M.; et al. Prognostic and predictive effects of TP53 co-mutation in patients with EGFR-mutated non-small cell lung cancer (NSCLC). Lung Cancer 2017, 111, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Singal, G.; Miller, P.G.; Agarwala, V.; Li, G.; Kaushik, G.; Backenroth, D.; Gossai, A.; Frampton, G.M.; Torres, A.Z.; Lehnert, E.M.; et al. Association of Patient Characteristics and Tumor Genomics with Clinical Outcomes among Patients with Non-Small Cell Lung Cancer Using a Clinicogenomic Database. JAMA 2019, 321, 1391–1399. [Google Scholar] [CrossRef] [Green Version]
- Flatiron. About US. Available online: https://flatiron.com/about-us/ (accessed on 5 May 2022).
- Paesmans, M.; Sculier, J.P.; Libert, P.; Bureau, G.; Dabouis, G.; Thiriaux, J.; Michel, J.; Van Cutsem, O.; Sergysels, R.; Mommen, P.; et al. Prognostic factors for survival in advanced non-small-cell lung cancer: Univariate and multivariate analyses including recursive partitioning and amalgamation algorithms in 1,052 patients. The European Lung Cancer Working Party. J. Clin. Oncol. 1995, 13, 1221–1230. [Google Scholar] [CrossRef]
- O’Connell, J.P.; Kris, M.G.; Gralla, R.J.; Groshen, S.; Trust, A.; Fiore, J.J.; Kelsen, D.P.; Heelan, R.T.; Golbey, R.B. Frequency and prognostic importance of pretreatment clinical characteristics in patients with advanced non-small-cell lung cancer treated with combination chemotherapy. J. Clin. Oncol. 1986, 4, 1604–1614. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; McDonnell, K.; Kris, M.G.; Shen, R.; Sima, C.S.; Bach, P.B.; Rizvi, N.A.; Riely, G.J. Pack-years of cigarette smoking as a prognostic factor in patients with stage IIIB/IV nonsmall cell lung cancer. Cancer 2010, 116, 670–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergqvist, M.; Christensen, H.N.; Wiklund, F.; Bergstrom, S. Real world utilization of EGFR TKIs and prognostic factors for survival in NSCLC during 2010-2016 in Sweden: A nationwide observational study. Int. J. Cancer 2020, 146, 2510–2517. [Google Scholar] [CrossRef]
- Yu, X.; Sheng, J.; Pan, G.; Fan, Y. Real-world utilization of EGFR TKIs and prognostic factors for survival in EGFR-mutated non-small cell lung cancer patients with brain metastases. Int. J. Cancer 2021, 149, 1121–1128. [Google Scholar] [CrossRef] [PubMed]
- Cuyun Carter, G.; Barrett, A.M.; Kaye, J.A.; Liepa, A.M.; Winfree, K.B.; John, W.J. A comprehensive review of nongenetic prognostic and predictive factors influencing the heterogeneity of outcomes in advanced non-small-cell lung cancer. Cancer Manag. Res. 2014, 6, 437–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawaguchi, T.; Takada, M.; Kubo, A.; Matsumura, A.; Fukai, S.; Tamura, A.; Saito, R.; Maruyama, Y.; Kawahara, M.; Ou, S.H.I. Performance status and smoking status are independent favorable prognostic factors for survival in non-small cell lung cancer: A comprehensive analysis of 26,957 patients with NSCLC. J. Thorac. Oncol. 2010, 5, 620–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roeper, J.; Falk, M.; Chalaris-Rissmann, A.; Lueers, A.C.; Ramdani, H.; Wedeken, K.; Stropiep, U.; Diehl, L.; Tiemann, M.; Heukamp, L.C.; et al. TP53 co-mutations in EGFR mutated patients in NSCLC stage IV: A strong predictive factor of ORR, PFS and OS in EGFR mt+ NSCLC. Oncotarget 2020, 11, 250–264. [Google Scholar] [CrossRef] [Green Version]
- Vokes, N.I.; Chambers, E.; Nguyen, T.; Coolidge, A.; Lydon, C.A.; Le, X.; Sholl, L.; Heymach, J.V.; Nishino, M.; Van Allen, E.M.; et al. Concurrent TP53 Mutations Facilitate Resistance Evolution in EGFR-Mutant Lung Adenocarcinoma. J. Thorac. Oncol. 2022, 17, 779–792. [Google Scholar] [CrossRef]
- Ma, X.; Long, L.; Moon, S.; Adamson, B.J.S.; Baxi, S.S. Comparison of population characteristics in real-world clinical oncology databases in the US: Flatiron Health, SEER, and NPCR. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Berger, M.L.; Curtis, M.D.; Smith, G.; Harnett, J.; Abernethy, A.P. Opportunities and challenges in leveraging electronic health record data in oncology. Future Oncol. 2016, 12, 1261–1274. [Google Scholar] [CrossRef]
- Stewart, M.; Norden, A.D.; Dreyer, N.; Henk, H.J.; Abernethy, A.P.; Chrischilles, E.; Kushi, L.; Mansfield, A.S.; Khozin, S.; Sharon, E.; et al. An Exploratory Analysis of Real-World End Points for Assessing Outcomes Among Immunotherapy-Treated Patients With Advanced Non-Small-Cell Lung Cancer. JCO Clin. Cancer Inform. 2019, 3, 1–15. [Google Scholar] [CrossRef]
- Winfree, K.B.; Molife, C.; Peterson, P.M.; Chen, Y.; Visseren-Grul, C.M.; Leusch, M.S.; Beyrer, J.; Dimou, A. Real-world characteristics and outcomes of advanced non-small-cell lung cancer patients with EGFR exon 19 deletions or exon 21 mutations. Future Oncol. 2021, 17, 2867–2881. [Google Scholar] [CrossRef] [PubMed]
- Sheng, M.; Wang, F.; Zhao, Y.; Li, S.; Wang, X.; Shou, T.; Luo, Y.; Tang, W. Comparison of clinical outcomes of patients with non-small-cell lung cancer harbouring epidermal growth factor receptor exon 19 or exon 21 mutations after tyrosine kinase inhibitors treatment: A meta-analysis. Eur. J. Clin. Pharmacol. 2016, 72, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Human Services, US Food and Drug Administration. 2018. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-osimertinib-first-line-treatment-metastatic-nsclc-most-common-egfr-mutations (accessed on 5 May 2022).
- Sheinson, D.M.; Wong, W.B.; Meyer, C.S.; Stergiopoulos, S.; Lofgren, K.T.; Flores, C.; Adams, D.V.; Fleury, M.E. Trends in Use of Next-Generation Sequencing in Patients With Solid Tumors by Race and Ethnicity After Implementation of the Medicare National Coverage Determination. JAMA Netw. Open 2021, 4, e2138219. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, K.; Nadal, E.; Garon, E.B.; Nishio, M.; Seto, T.; Yamamoto, N.; Park, K.; Shih, J.Y.; Paz-Ares, L.; Frimodt-Moller, B.; et al. RELAY Subgroup Analyses by EGFR Ex19del and Ex21L858R Mutations for Ramucirumab Plus Erlotinib in Metastatic Non-Small Cell Lung Cancer. Clin. Cancer Res. 2021, 27, 5258–5271. [Google Scholar] [CrossRef]
- Zhang, L.; Zhao, H.; Zhang, Z.; Yao, W.; Min, X.; Gu, K.; Yu, G.; Cheng, C.; Cui, J.; Miao, L.; et al. ACTIVE: Apatinib Plus Gefitinib versus Placebo Plus Gefitinib as First-Line Treatment for Advanced Epidermal Growth Factor Receptor-Mutant (EGFRm) Non-Small-Cell Lung Cancer (NSCLC): A Multicentered, Randomized, Double-Blind, Placebo-Controlled Phase III Trial (CTONG1706). Available online: https://www.annalsofoncology.org/article/S0923-7534(20)42365-8/pdf (accessed on 14 September 2022).
- Li, A.M.; Boichard, A.; Kurzrock, R. Mutated TP53 is a marker of increased VEGF expression: Analysis of 7525 pan-cancer tissues. Cancer Biol. Ther. 2020, 21, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.K.; Wang, L.; Han, B.H.; Li, W.; Yu, P.; Liu, Y.P.; Ding, C.M.; Song, X.; Ma, Z.Y.; Ren, X.L.; et al. First-line icotinib versus cisplatin/pemetrexed plus pemetrexed maintenance therapy for patients with advanced EGFR mutation-positive lung adenocarcinoma (CONVINCE): A phase 3, open-label, randomized study. Ann. Oncol. 2017, 28, 2443–2450. [Google Scholar] [CrossRef]
- Sabapathy, K.; Lane, D.P. Therapeutic targeting of p53: All mutants are equal, but some mutants are more equal than others. Nat. Rev. Clin. Oncol. 2018, 15, 13–30. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 356) | TP53wt (n = 146) | TP53mt (n = 210) |
|---|---|---|---|
| Follow-up in months from 1 L start, mean (SD) | 19.9 (15.8) | 21.5 (17.5) | 18.8 (14.4) |
| Age at adv. Dx, median (IQR) | 68.0 (60.5–76.1) | 69.6 (63.5–77.7) | 66.7 (58.2–75.2) |
| Age group, n (%) | |||
| <65 years | 137 (38.5) | 46 (31.5) | 91 (43.3) |
| 65–74 years | 115 (32.3) | 51 (34.9) | 64 (30.5) |
| 75+ years | 104 (29.2) | 49 (33.6) | 55 (26.2) |
| Sex, n (%) | |||
| Female | 244 (68.5) | 103 (70.5) | 141 (67.1) |
| Male | 112 (31.5) | 43 (29.5) | 69 (32.9) |
| Race, n (%) | |||
| Missing | 26 (7.3) | 9 (6.2) | 17 (8.1) |
| Asian | 41 (11.5) | 22 (15.1) | 19 (9.0) |
| Black or African American | 15 (4.2) | 5 (3.4) | 10 (4.8) |
| Other Race | 59 (16.6) | 26 (17.8) | 33 (15.7) |
| White | 215 (60.4) | 84 (57.5) | 131 (62.4) |
| Smoking history, yes, n (%) | 154 (43.3) | 61 (41.8) | 93 (44.3) |
| NSCLC stage at initial diagnosis, n (%) | |||
| I–II | 20 (5.6) | 11 (7.5) | 9 (4.3) |
| III | 29 (8.1) | 11 (7.5) | 18 (8.6) |
| IV | 307 (86.2) | 124 (84.9) | 183 (87.1) |
| ECOG performance status, n (%) | |||
| 0 | 107 (30.1) | 43 (29.5) | 64 (30.5) |
| 1+ | 145 (40.7) | 59 (40.4) | 86 (41.0) |
| Missing | 104 (29.2) | 44 (30.1) | 60 (28.6) |
| EGFR mutation type, n (%) | |||
| Exon19 | 203 (57.0) | 81 (55.5) | 122 (58.1) |
| Exon21 | 153 (43.0) | 65 (44.5) | 88 (41.9) |
| Metastatic site, n (%) | |||
| Brain | 77 (21.6) | 28 (19.2) | 49 (23.3) |
| Bone | 97 (27.2) | 34 (23.3) | 63 (30.0) |
| Liver | 14 (3.9) | 8 (5.5) | 6 (2.9) |
| Lung | 51 (14.3) | 17 (11.6) | 34 (16.2) |
| Lymph Node | 23 (6.5) | 13 (8.9) | 10 (4.8) |
| Adrenal | 21 (5.9) | 7 (4.8) | 14 (6.7) |
| Other | 5 (1.4) | 3 (2.1) | 2 (1.0) |
| Practice type, n (%) | |||
| Academic | 41 (11.5) | 18 (12.3) | 23 (11.0) |
| Community | 315 (88.5) | 128 (87.7) | 187 (89.0) |
| 1 L | 2 L | ||||||
|---|---|---|---|---|---|---|---|
| Drug Class | Overall | TP53wt | TP53mt | Drug Class | Overall | TP53wt | TP53mt |
| n = 356 | n = 146 | n = 210 | n = 169 | n = 61 | n = 108 | ||
| EGFR-TKI monotherapy | 267 (75.0) | 107 (73.6) | 160 (76.2) | EGFR-TKI monotherapy | 114 (67.5) | 43 (70.5) | 71 (70.3) |
| Chemotherapy alone | 37 (10.0) | 19 (13.1) | 18 (8.6) | Chemotherapy + Immune Checkpoint Inhibitor | 13 (7.3) | 4 (6.6) | 9 (7.4) |
| Chemotherapy + Immune Checkpoint Inhibitor | 20 (5.6) | 7 (4.3) | 13 (6.2) | Chemotherapy alone | 8 (4.7) | 2 (2.9) | 6 (5.9) |
| Other | 8 (2.5) | 3 (2.1) | 5 (2.4) | Immune Checkpoint Inhibitor monotherapy | 7 (4.1) | 5 (8.2) | 2 (1.9) |
| Chemotherapy + VEGF Inhibitor | 8 (2.2) | 3 (2.1) | 5 (2.4) | EGFR-TKI + Chemotherapy + Immune Checkpoint Inhibitor | 4 (2.4) | 0 (0) | 4 (3.9) |
| EGFR-TKI + VEGF Inhibitor | 6 (1.7) | 2 (1.4) | 4 (1.9) | Other + Chemotherapy | 3 (1.8) | 2 (2.9) | 1 (0.9) |
| EGFR-TKI + Chemotherapy | 3 (0.9) | 1 (0.7) | 2 (0.9) | EGFR-TKI + Immune Checkpoint Inhibitor | 3 (1.8) | 0 (0) | 3 (3.0) |
| Immune Checkpoint Inhibitor monotherapy | 3 (0.9) | 2 (1.4) | 1 (0.5) | Chemotherapy + VEGF Inhibitor | 3 (1.7) | 0 (0) | 3 (2.8) |
| EGFR-TKI + Chemotherapy + VEGF Inhibitor | 1 (0.3) | 0 (0) | 1 (0.5) | EGFR-TKI + Chemotherapy | 2 (1.2) | 2 (3.3) | 0 (0) |
| EGFR-TKI + Chemotherapy + Immune Checkpoint Inhibitor | 1 (0.3) | 1 (0.7) | 0 (0) | EGFR-TKI + Chemotherapy + VEGF Inhibitor | 2 (1.2) | 0 (0) | 2 (1.9) |
| EGFR-TKI + Immune Checkpoint Inhibitor | 1 (0.3) | 0 (0) | 1 (0.5) | EGFR-TKI + VEGF Inhibitor | 2 (1.2) | 1 (1.64) | 1 (0.9) |
| Other + EGFR-TKI | 1 (0.3) | 1 (0.7) | 0 (0) | Hormone receptor therapy | 1 (0.6) | 0 (0) | 1 (0.9) |
| Immunosuppressant | 1 (0.6) | 0 (0) | 1 (0.9) | ||||
| Other + EGFR-TKI | 1 (0.6) | 0 (0) | 1 (0.9) | ||||
| Variable | Category | rwPFS, HR (95% CI) | OS, HR (95% CI) |
|---|---|---|---|
| Overall | |||
| Age at adv dx | ≥75 vs. <75 | 1.2 (0.9–1.6) | 2.0 (1.4–2.7) d |
| Sex | Male vs. Female | 1.1 (0.8–1.5) | 1.4 (1.0–2.0) a |
| ECOG PS | 1+ vs. 0 | 1.5 (1.1–2.2) a | 1.7 (1.1–2.5) b |
| Unknown vs. 0 | 1.5 (1.0–2.2) a | 0.9 (0.6–1.5) | |
| Smoking history | Yes vs. No | 1.6 (1.2–2.1) b | 1.4 (0.99–1.87) |
| TP53 status | mt vs. wt | 1.4 (1.1–1.9) a | 1.6 (1.1–2.2) b |
| TP53 status/EGFR mutation type | TP53mt/Exon19 vs. TP53wt/Exon19 | 1.5 (1.0–2.2) | 1.9 (1.2–2.9) b |
| TP53mt/Exon21 vs. TP53wt/Exon19 | 1.9 (1.3–2.9) b | 1.8 (1.1–3.0) a | |
| TP53wt/Exon21 vs. TP53wt/Exon19 | 1.4 (0.9–2.3) | 1.44 (0.8–2.5) | |
| Bone mets | Yes vs. No | 1.0 (0.7–1.4) | 1.4 (1.0–1.9) |
| Brain mets | Yes vs. No | 1.8 (1.3–2.5) c | 1.7 (1.2–2.4) b |
| Exon group | Exon21 vs. Exon19 | 1.3 (1.0–1.8) a | 1.1 (0.8–1.5) |
| TKI Monotherapy | |||
| Age at adv dx | ≥75 vs. <75 | 1.1 (0.8–1.6) | 1.7 (1.1–2.5) b |
| Sex | Male vs. Female | 1.2 (0.8–1.7) | 1.5 (1.0–2.3) a |
| ECOG PS | 1+ vs. 0 | 2.1 (1.3–3.3) b | 2.4 (1.4–4.1) b |
| Unknown vs. 0 | 2.2 (1.4–3.5) b | 1.3 (0.7–2.3) | |
| Smoking history | Yes vs. No | 1.6 (1.2–2.2) b | 1.6 (1.1–2.3) a |
| TP53 | mt vs. wt | 1.6 (1.1–2.3) b | 1.7 (1.1–2.6) a |
| TP53 status/EGFR mutation type | TP53mt/Exon19 vs. TP53wt/Exon19 | 1.6 (1.0–2.4) a | 2.2 (1.3–3.7) b |
| TP53mt/Exon21 vs. TP53wt/Exon19 | 2.0 (1.2–3.2) b | 2.1 (1.1–3.9) a | |
| TP53wt/Exon21 vs. TP53wt/Exon19 | 1.2 (0.6–2.1) | 1.9 (0.9–3.7) | |
| Bone mets | Yes vs. No | 1.1 (0.8–1.6) | 1.4 (0.9–2.1) |
| Brain mets | Yes vs. No | 1.8 (1.2–2.6) b | 1.7 (1.1–2.6) b |
| Exon group | Exon21 vs. Exon19 | 1.2 (0.9–1.7) | 1.2 (0.8–1.8) |
| Other Monotherapy | |||
| Age at adv dx | ≥75 vs. <75 | 1.6 (0.8–3.0) | 3.1 (1.7–5.6) c |
| Sex | Male vs. Female | 0.7 (0.4–1.4) | 1.1 (0.6–2.1) |
| ECOG PS | 1+ vs. 0 | 0.8 (0.4–1.6) | 1.1 (0.6–2.0) |
| Unknown vs. 0 | 0.6 (0.3–1.3) | 0.5 (0.2–1.3) | |
| Smoking history | Yes vs. No | 1.4 (0.8–2.6) | 1.0 (0.6–1.8) |
| TP53 | mt vs. wt | 0.9 (0.5–1.6) | 1.3 (0.7–2.3) |
| TP53 status/EGFR mutation type | TP53mt/Exon19 vs. TP53wt/Exon19 | 0.9 (0.4–2.3) | 1.2 (0.5–2.9) |
| TP53mt/Exon21 vs. TP53wt/Exon19 | 1.2 (0.5–3.0) | 1.2 (0.5–2.7) | |
| TP53wt/Exon21 vs. TP53wt/Exon19 | 1.5 (0.6–3.7) | 0.9 (0.4–2.1) | |
| Bone mets | Yes vs. No | 0.9 (0.3–2.3) | 1.5 (0.8–2.9) |
| Brain mets | Yes vs. No | 3.5 (1.7–7.3) c | 1.8 (0.9–3.5) |
| Exon group | Exon21 vs. Exon19 | 1.4 (0.8–2.6) | 0.9 (0.5–1.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, X.; Molife, C.; Leusch, M.S.; Rizzo, M.T.; Peterson, P.M.; Caria, N.; Chen, Y.; Gugel, E.G.; Visseren-Grul, C. TP53 Co-Mutation Status Association with Clinical Outcomes in Patients with EGFR-Mutant Non-Small Cell Lung Cancer. Cancers 2022, 14, 6127. https://doi.org/10.3390/cancers14246127
Le X, Molife C, Leusch MS, Rizzo MT, Peterson PM, Caria N, Chen Y, Gugel EG, Visseren-Grul C. TP53 Co-Mutation Status Association with Clinical Outcomes in Patients with EGFR-Mutant Non-Small Cell Lung Cancer. Cancers. 2022; 14(24):6127. https://doi.org/10.3390/cancers14246127
Chicago/Turabian StyleLe, Xiuning, Cliff Molife, Mark S. Leusch, Maria Teresa Rizzo, Patrick M. Peterson, Nicola Caria, Yongmei Chen, Elena Gonzalez Gugel, and Carla Visseren-Grul. 2022. "TP53 Co-Mutation Status Association with Clinical Outcomes in Patients with EGFR-Mutant Non-Small Cell Lung Cancer" Cancers 14, no. 24: 6127. https://doi.org/10.3390/cancers14246127