
Analysis of the Risk of Oral Squamous Cell Carcinoma in Patients with and without Recurrent Aphthous Stomatitis: A Retrospective Evaluation of Real-World Data of about 150,000 Patients

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
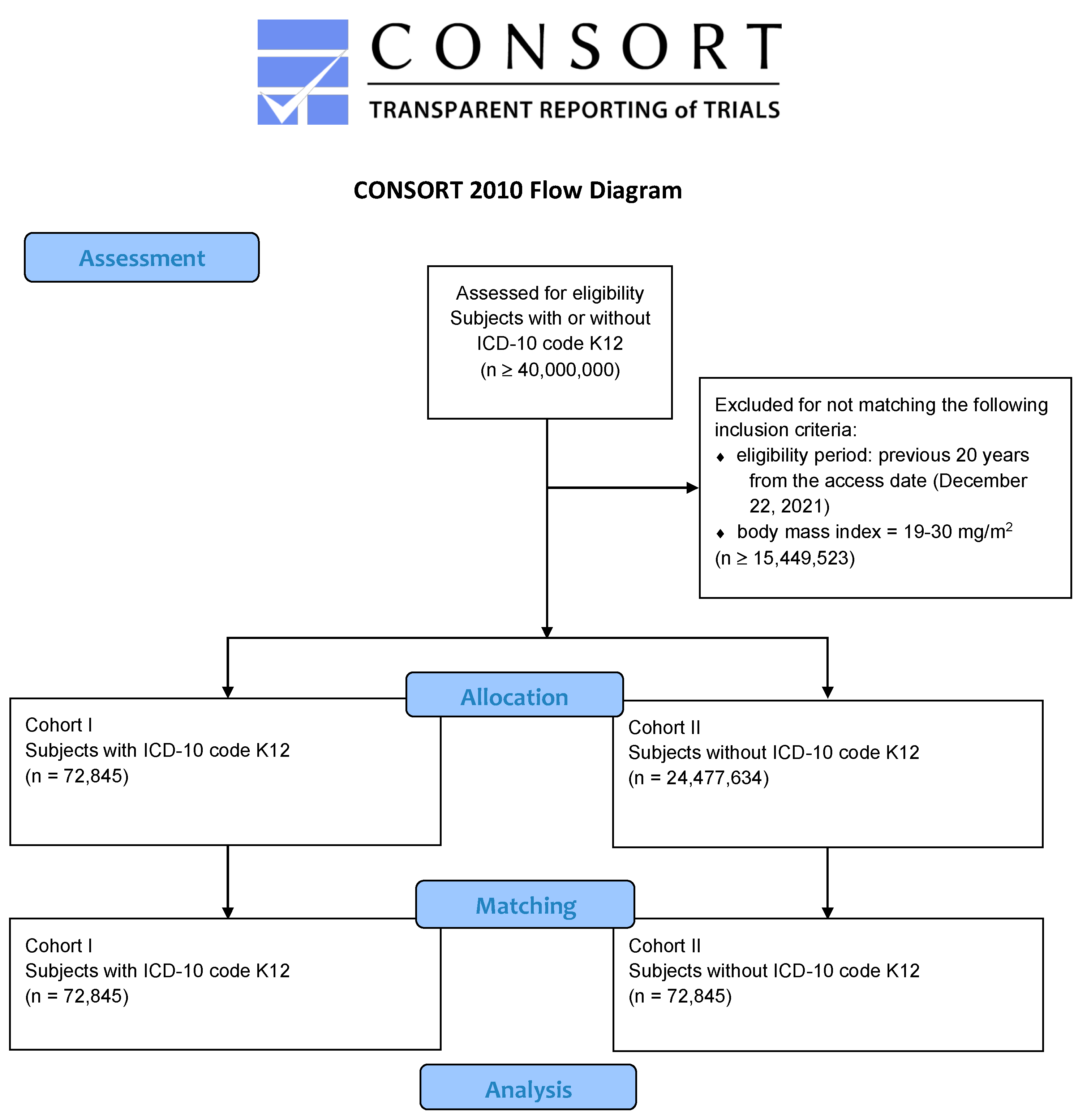
2.1. Data Acquisition, Allocation, and Matching
2.2. Data Analysis
3. Results
3.1. Assessment, Allocation, and Matching
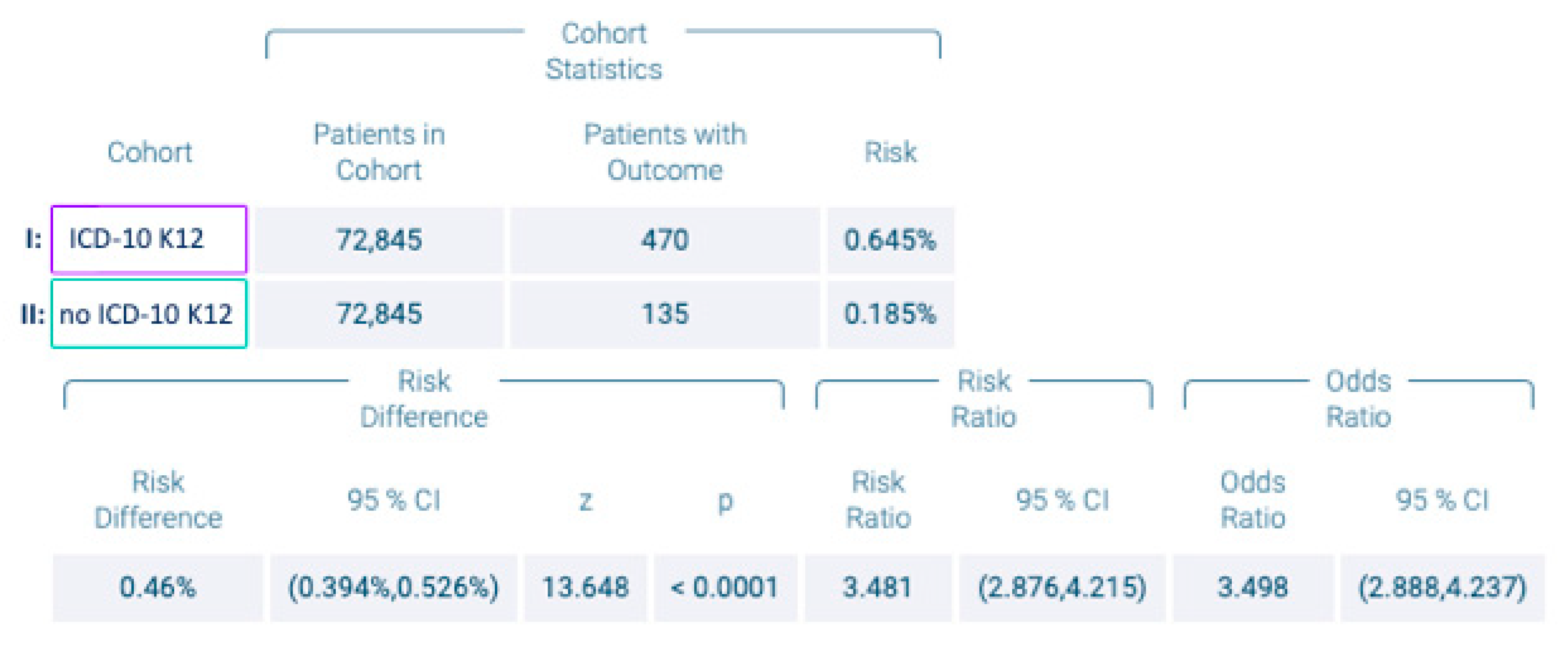
3.2. Diagnosis of OSCC
3.3. Human Immunodeficiency Virus (HIV)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AIDS | acquired immunodeficiency syndrome |
| BMI | body mass index |
| HCO | healthcare organization |
| HIV | human immunodeficiency virus |
| HPV | human papillomavirus |
| ICD | International Classification of Diseases |
| IL | interleukin |
| OLP | oral lichen planus |
| OPMD | oral potentially malignant disorder |
| OR | odds ratio |
| OSCC | oral squamous cell carcinoma |
| PFAPA | periodic fever, aphthous stomatitis, pharyngitis, and adenitis syndrome |
| RR | risk ratio |
| RAS | recurrent aphthous stomatitis |
| SIR | standardized incidence ratio |
| UICC | Union Internationale Contre le Cancer |
| WHO | World Health Organization |
References
- Rivera, C. Essentials of oral cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 11884–11894. [Google Scholar] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Sasahira, T.; Kirita, T. Hallmarks of Cancer-Related Newly Prognostic Factors of Oral Squamous Cell Carcinoma. Int. J. Mol. Sci. 2018, 19, 2413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; Gonzalez-Moles, M.A.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral. Dis. 2021, 27, 1862–1880. [Google Scholar] [CrossRef]
- Warnakulasuriya, S.; Johnson, N.W.; van der Waal, I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J. Oral. Pathol. Med. 2007, 36, 575–580. [Google Scholar] [CrossRef]
- Chattopadhyay, A.; Chatterjee, S. Risk indicators for recurrent aphthous ulcers among adults in the US. Community Dent. Oral. Epidemiol. 2007, 35, 152–159. [Google Scholar] [CrossRef]
- Bulur, I.; Onder, M. Behcet disease: New aspects. Clin. Dermatol. 2017, 35, 421–434. [Google Scholar] [CrossRef]
- Nieto, I.G.; Alabau, J.L.C. Immunopathogenesis of Behcet Disease. Curr. Rheumatol. Rev. 2020, 16, 12–20. [Google Scholar] [CrossRef]
- Porter, S.R.; Scully Cbe, C. Aphthous ulcers (recurrent). BMJ Clin. Evid. 2007, 2007, 1303. [Google Scholar]
- Mura, C.; Preissner, S.; Nahles, S.; Heiland, M.; Bourne, P.E.; Preissner, R. Real-world evidence for improved outcomes with histamine antagonists and aspirin in 22,560 COVID-19 patients. Signal. Transduct. Target. Ther. 2021, 6, 267. [Google Scholar] [CrossRef]
- Seeland, U.; Coluzzi, F.; Simmaco, M.; Mura, C.; Bourne, P.E.; Heiland, M.; Preissner, R.; Preissner, S. Evidence for treatment with estradiol for women with SARS-CoV-2 infection. BMC Med. 2020, 18, 369. [Google Scholar] [CrossRef] [PubMed]
- Geldof, T.; Popovic, D.; Van Damme, N.; Huys, I.; Van Dyck, W. Nearest Neighbour Propensity Score Matching and Bootstrapping for Estimating Binary Patient Response in Oncology: A Monte Carlo Simulation. Sci. Rep. 2020, 10, 964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, R.J.; Wyss, R.; Abdia, Y.; Toh, S.; Johnson, M.; Lee, H.; Karami, S.; Major, J.M.; Nguyen, M.; Wang, S.V.; et al. Evaluating the use of bootstrapping in cohort studies conducted with 1:1 propensity score matching-A plasmode simulation study. Pharmacoepidemiol. Drug Saf. 2019, 28, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Small, D.S. The use of bootstrapping when using propensity-score matching without replacement: A simulation study. Stat. Med. 2014, 33, 4306–4319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiels, M.S.; Cole, S.R.; Kirk, G.D.; Poole, C. A meta-analysis of the incidence of non-AIDS cancers in HIV-infected individuals. J. Acquir. Immune Defic. Syndr. 2009, 52, 611–622. [Google Scholar] [CrossRef] [Green Version]
- Shiels, M.S.; Engels, E.A. Evolving epidemiology of HIV-associated malignancies. Curr. Opin. HIV AIDS 2017, 12, 6–11. [Google Scholar] [CrossRef]
- Hernandez-Ramirez, R.U.; Shiels, M.S.; Dubrow, R.; Engels, E.A. Cancer risk in HIV-infected people in the USA from 1996 to 2012: A population-based, registry-linkage study. Lancet HIV 2017, 4, e495–e504. [Google Scholar] [CrossRef]
- Qin, L.; Kao, Y.W.; Lin, Y.L.; Peng, B.Y.; Deng, W.P.; Chen, T.M.; Lin, K.C.; Yuan, K.S.; Wu, A.T.; Shia, B.C.; et al. Combination of recurrent oral aphthae and dry eye syndrome may constitute an independent risk factor for oral cavity cancer in elderly women. Cancer Manag. Res. 2018, 10, 3273–3281. [Google Scholar] [CrossRef] [Green Version]
- Sardaro, N.; Della Vella, F.; Incalza, M.A.; Di Stasio, D.L.A.; Lucchese, A.; Contaldo, M.; Laudadio, C.; Petruzzi, M. Oxidative Stress and Oral Mucosal Diseases: An Overview. In Vivo 2019, 33, 289–296. [Google Scholar] [CrossRef] [Green Version]
- Di Gioia, S.A.; Bedoni, N.; von Scheven-Gete, A.; Vanoni, F.; Superti-Furga, A.; Hofer, M.; Rivolta, C. Analysis of the genetic basis of periodic fever with aphthous stomatitis, pharyngitis, and cervical adenitis (PFAPA) syndrome. Sci. Rep. 2015, 5, 10200. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Zhang, N.; Wu, C. LncRNA CASC 2 is upregulated in aphthous stomatitis and predicts the recurrence. BMC Oral. Health 2020, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Wu, W. Downregulation of lncRNA CASC2 promotes the postoperative local recurrence of early oral squamous cell carcinoma. Eur. Arch. Otorhinolaryngol. 2019, 276, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Xing, H.B.; Qiu, H.M.; Li, Y.; Dong, P.F.; Zhu, X.M. Long noncoding RNA CASC2 alleviates the growth, migration and invasion of oral squamous cell carcinoma via downregulating CDK1. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4777–4783. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.G.; Cohen, D.M.; Clark, A.N. Ulcerated Lesions of the Oral Mucosa: Clinical and Histologic Review. Head Neck Pathol. 2019, 13, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Hertel, M.; Matter, D.; Schmidt-Westhausen, A.M.; Bornstein, M.M. Oral syphilis: A series of 5 cases. J. Oral. Maxillofac. Surg. 2014, 72, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Mabey, D.; Kamb, M.L.; Chen, X.S.; Radolf, J.D.; Benzaken, A.S. Syphilis. Nat. Rev. Dis. Primers 2017, 3, 17073. [Google Scholar] [CrossRef]
- Ghanem, K.G.; Ram, S.; Rice, P.A. The Modern Epidemic of Syphilis. N. Engl. J. Med. 2020, 382, 845–854. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Nanavati, R.; Modi, T.G.; Dobariya, C. Oral cancer: Etiology and risk factors: A review. J. Cancer Res. Ther. 2016, 12, 458–463. [Google Scholar] [CrossRef]
- Baccaglini, L.; Lalla, R.V.; Bruce, A.J.; Sartori-Valinotti, J.C.; Latortue, M.C.; Carrozzo, M.; Rogers, R.S., III. Urban legends: Recurrent aphthous stomatitis. Oral. Dis. 2011, 17, 755–770. [Google Scholar] [CrossRef] [Green Version]
- Marafini, I.; Monteleone, G.; Stolfi, C. Association Between Celiac Disease and Cancer. Int. J. Mol. Sci. 2020, 21, 4155. [Google Scholar] [CrossRef]
- Loftus, C.G.; Loftus, E.V., Jr. Cancer risk in celiac disease. Gastroenterology 2002, 123, 1726–1729. [Google Scholar] [CrossRef] [PubMed]
- Ryan-Harshman, M.; Aldoori, W. Vitamin B12 and health. Can. Fam. Physician 2008, 54, 536–541. [Google Scholar] [PubMed]
- Wu, D.; Xin, J.; Liu, J.; Zhou, P. The association between interleukin polymorphism and recurrent aphthous stomatitis: A meta-analysis. Arch. Oral. Biol. 2018, 93, 3–11. [Google Scholar] [CrossRef]
- Bhat, I.A.; Naykoo, N.A.; Qasim, I.; Ganie, F.A.; Yousuf, Q.; Bhat, B.A.; Rasool, R.; Aziz, S.A.; Shah, Z.A. Association of interleukin 1 beta (IL-1beta) polymorphism with mRNA expression and risk of non small cell lung cancer. Meta Gene 2014, 2, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Sobti, R.C.; Kordi Tamandani, D.M.; Shekari, M.; Kaur, P.; Malekzadeh, K.; Suri, V. Interleukin 1 beta gene polymorphism and risk of cervical cancer. Int. J. Gynaecol. Obstet. 2008, 101, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.H.; Chen, W.C.; Tsai, C.H.; Hang, L.W.; Tsai, F.J. Interleukin-4 gene, but not the interleukin-1 beta gene polymorphism, is associated with oral cancer. J. Clin. Lab. Anal. 2005, 19, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Allison, P.; Franco, E.; Black, M.; Feine, J. The role of professional diagnostic delays in the prognosis of upper aerodigestive tract carcinoma. Oral. Oncol. 1998, 34, 147–153. [Google Scholar] [CrossRef]
- Kowalski, L.P.; Carvalho, A.L. Influence of time delay and clinical upstaging in the prognosis of head and neck cancer. Oral Oncol 2001, 37, 94–98. [Google Scholar] [CrossRef]
- Trinetx Database. Available online: https://trinetx.com/trinetx-publication-guidelines/ (accessed on 19 December 2021).




{kind=link}
{kind=link}
{kind=link}
| Patients (n) | Before Matching | After Matching | ||||||
|---|---|---|---|---|---|---|---|---|
| Cohort I | Cohort II | p-Value | Standardized Mean Difference | Cohort I | Cohort II | p-Value | Standardized Mean Difference | |
| Total | 72,845 | 24,477,634 | 72,845 | 72,845 | ||||
| Males | 28,814 (39.56%) | 11,213,208 (46.0%) | 28,814 (39.66%) | 28,813 (39.55%) | ||||
| Females | 44,031 (60.44%) | 13,264,426 (54.0%) | <0.0001 | 0.1267 | 44,031 (60.44%) | 44,032 (60.45%) | 1.0 | 0.0 |
| Mean age at Index | 35.51 | 38.15 | <0.0001 | 0.1109 | 35.51 | 35.51 | 0.99 | 0.0 |
| Standard deviation | 23.55 | 24.02 | 23.55 | 23.56 | ||||
| Minimum | 0 | 0 | 0 | 0 | ||||
| Maximum | 90 | 90 | 90 | 90 | ||||
| Nicotine abuse | 4089 (5.61%) | 189,264 (0.77%) | <0.0001 | 0.2779306 | 4089 (5.61%) | 4092 (5.61%) | 0.97 | 0.0002 |
| Alcohol abuse | 578 (0.79%) | 24,620 (0.10%) | <0.0001 | 0.10400509 | 578 (0.79%) | 575 (0.79%) | 0.93 | 0.0005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hertel, M.; Birinci, S.; Heiland, M.; Preissner, R.; Nahles, S.; Schmidt-Westhausen, A.-M.; Preissner, S. Analysis of the Risk of Oral Squamous Cell Carcinoma in Patients with and without Recurrent Aphthous Stomatitis: A Retrospective Evaluation of Real-World Data of about 150,000 Patients. Cancers 2022, 14, 6011. https://doi.org/10.3390/cancers14236011
Hertel M, Birinci S, Heiland M, Preissner R, Nahles S, Schmidt-Westhausen A-M, Preissner S. Analysis of the Risk of Oral Squamous Cell Carcinoma in Patients with and without Recurrent Aphthous Stomatitis: A Retrospective Evaluation of Real-World Data of about 150,000 Patients. Cancers. 2022; 14(23):6011. https://doi.org/10.3390/cancers14236011
Chicago/Turabian StyleHertel, Moritz, Senem Birinci, Max Heiland, Robert Preissner, Susanne Nahles, Andrea-Maria Schmidt-Westhausen, and Saskia Preissner. 2022. "Analysis of the Risk of Oral Squamous Cell Carcinoma in Patients with and without Recurrent Aphthous Stomatitis: A Retrospective Evaluation of Real-World Data of about 150,000 Patients" Cancers 14, no. 23: 6011. https://doi.org/10.3390/cancers14236011