
Sex-Related Differences in Metastatic Melanoma Patients Treated with Immune Checkpoint Inhibition

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
- (a).
- The patient had a histopathologically confirmed metastatic melanoma;
- (b).
- The patient was treated either with a single checkpoint-inhibition (anti-PD-1) or dual checkpoint-inhibition (anti-PD-1/anti-CTLA-4);
- (c).
- The patient was treated in the Department of Dermatology of the University Hospital Zurich in Switzerland between 2013 and 2019;
2.2. Baseline Characteristics
2.2.1. Inflammatory Response to ICI in Peripheral Blood
2.2.2. Toxicity of ICI
2.2.3. Patient Response to ICI
- Short-term response to ICI
- A Long-term response to ICI
2.3. Statistical Analysis
3. Results
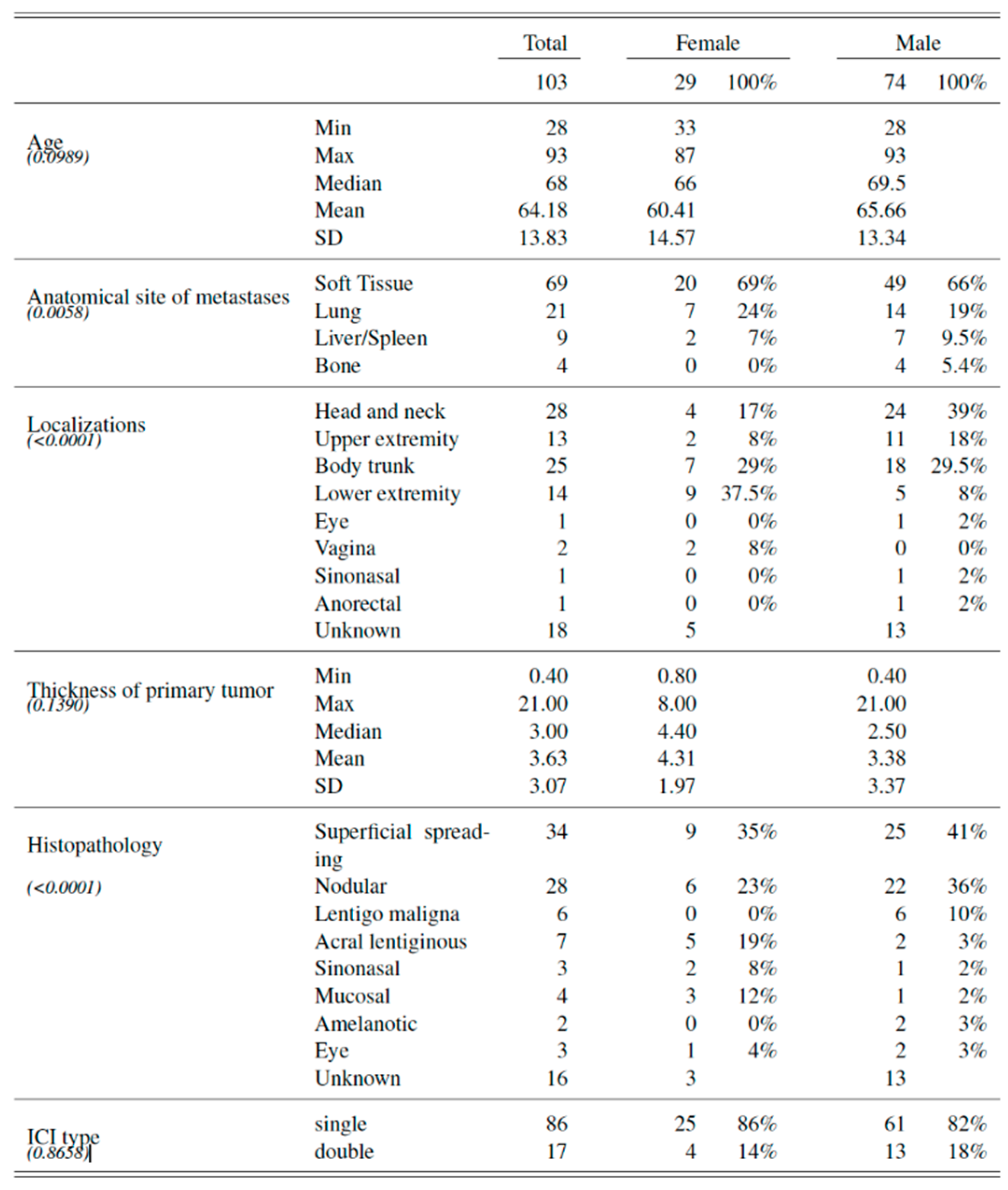
3.1. Baseline Characteristics
3.2. Inflammatory Response to ICI in Peripheral Blood
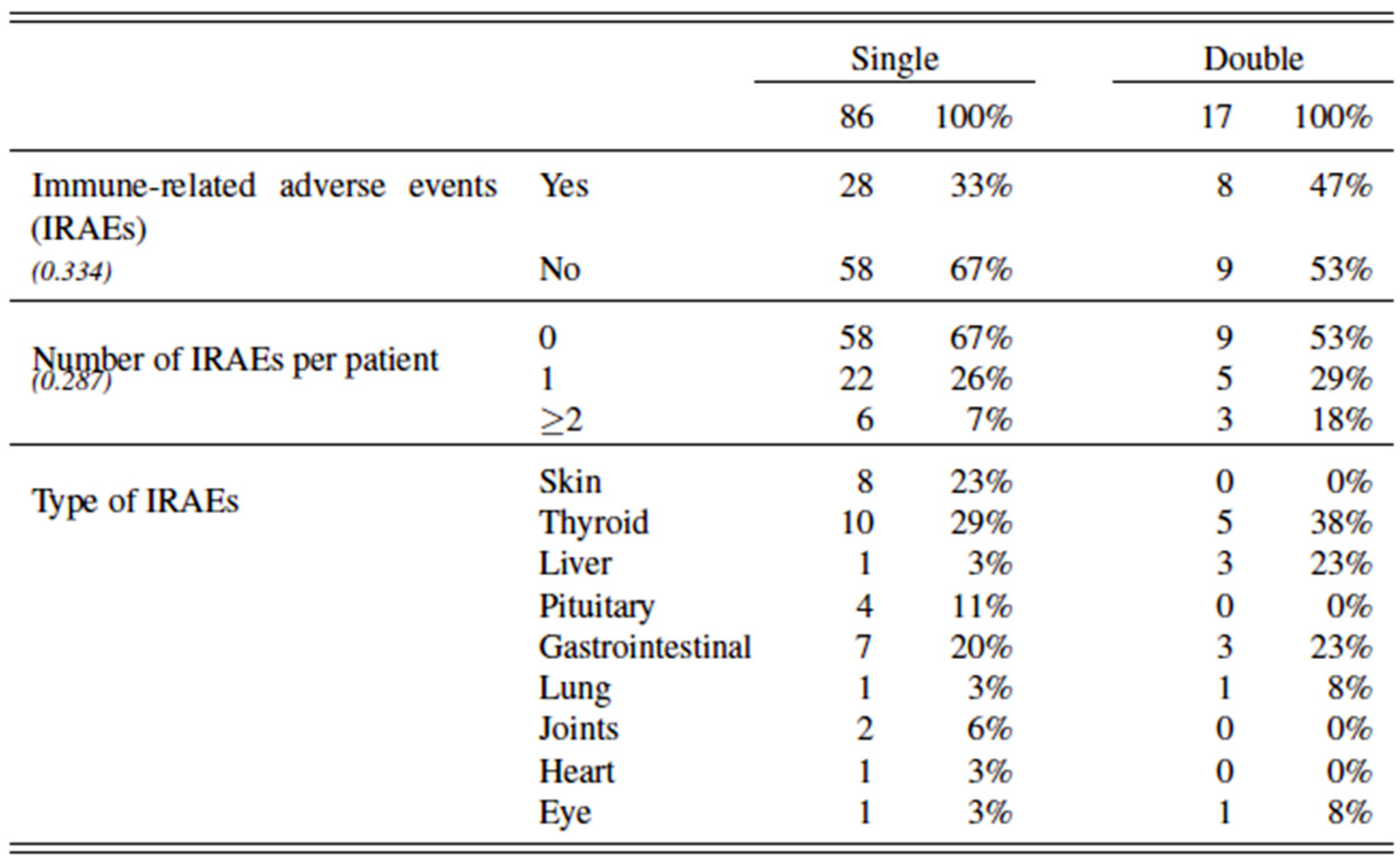
3.3. Treatment Toxicity
3.4. Patient Response to ICI
3.4.1. Short-Term Response to ICI
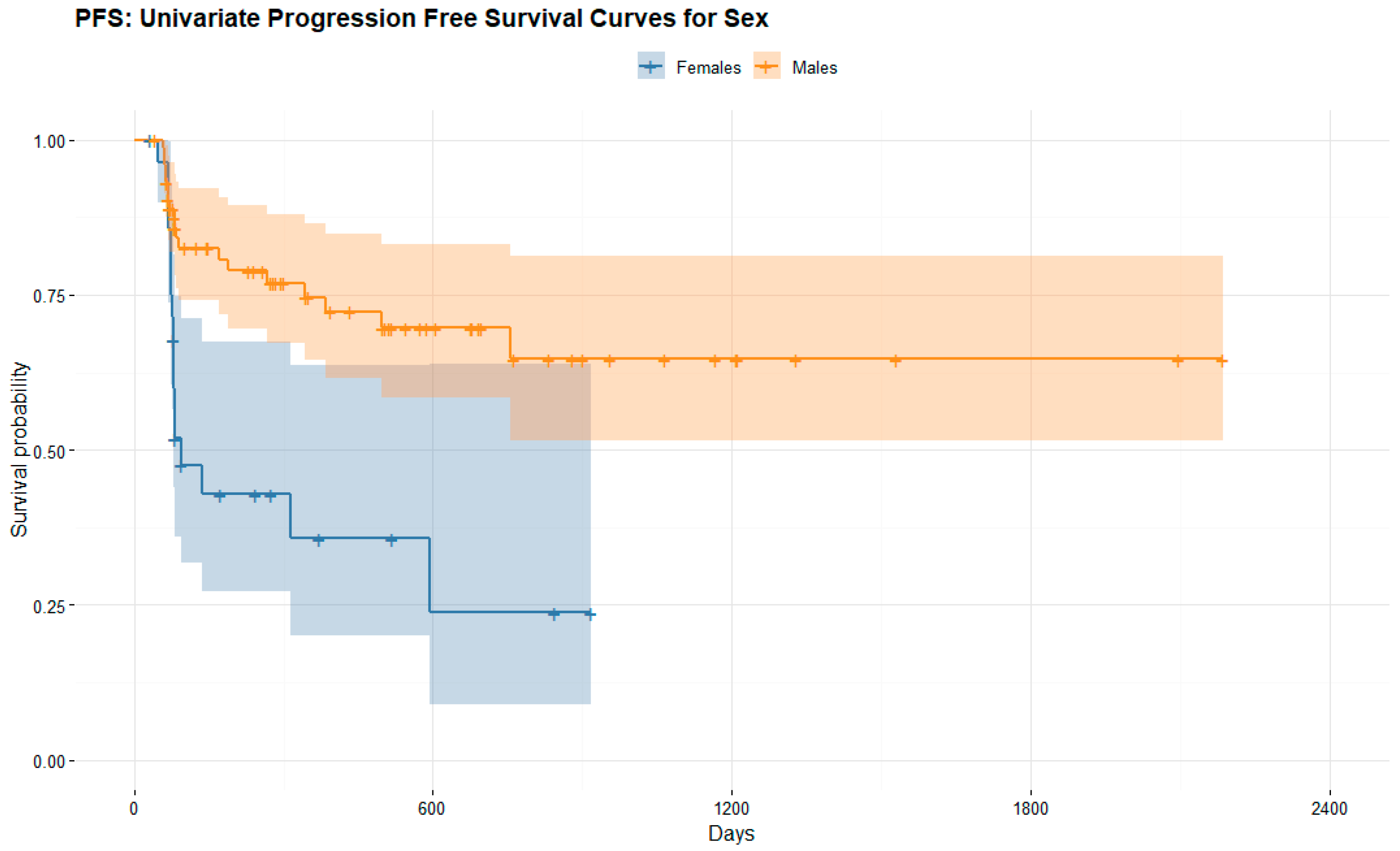
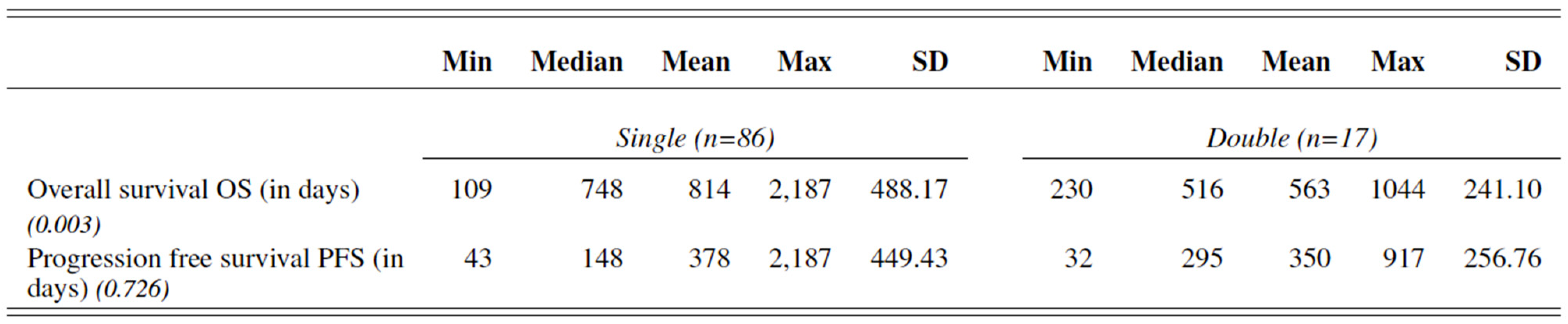
3.4.2. Long-Term Response to ICI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ICI | Immune Checkpoint Inhibitor |
| CTLA-4 | Cytotoxic T-Lymphocyte-associated Antigen-4 |
| PD-1 | Programmed cell death protein-1 |
| IRAEs | Immune-Related Adverse Events |
| GCP | Good Clinical Practice |
| AJCC | American Joint Committee on Cancer |
| NLR | Neutrophils-to-Lymphocytes Ratio |
| FDG-PET/CT18F-2-Fluor-2-desoxy-D-glucose Positron Emission Tomography/Computed Tomography | |
| RECIST 1.1. | Response Evaluation Criteria in Solid Tumors version 1.1. |
| PD | Progressive Disease |
| CB | Clinical Benefit |
| CR | Complete Response |
| PR | Partial Response |
| SD | Stable Disease |
| OS | Overall Survival |
| PFS | Progression-free survival PFS |
| MTV | Metabolic Tumor Volume |
| TLG | Total Lesion Glycolysis |
References
- Kudura, K.; Dimitriou, F.; Mihic-Probst, D.; Muehlematter, U.; Kutzker, T.; Basler, L.; Förster, R.; Dummer, R.; Mangana, J.; Husmann, L.; et al. Malignancy Rate of Indeterminate Findings on FDG-PET/CT in Cutaneous Melanoma Patients. Diagnostics 2021, 11, 883. [Google Scholar] [CrossRef] [PubMed]
- Buja, A.; Rugge, M.; Damiani, G.; Zorzi, M.; De Toni, C.; Vecchiato, A.; Del Fiore, P.; Spina, R.; Baldo, V.; Brazzale, A.R.; et al. Sex Differences in Cutaneous Melanoma: Incidence, Clinicopathological Profile, Survival, and Costs. J. Women’s Health 2022, 31, 1012–1019. [Google Scholar] [CrossRef] [PubMed]
- Kudura, K.; Dimitriou, F.; Basler, L.; Förster, R.; Mihic-Probst, D.; Kutzker, T.; Dummer, R.; Mangana, J.; Burger, I.A.; Kreissl, M.C. Prediction of Early Response to Immune Checkpoint Inhibition Using FDG-PET/CT in Melanoma Patients. Cancers 2021, 15, 3830. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, S.; Suppa, M.; Gandini, S. Melanoma Epidemiology and Sun Exposure. Acta Derm. Venereol. 2020, 100, adv00136. [Google Scholar] [CrossRef] [PubMed]
- Olsen, C.M.; Thompson, J.; Pandeya, N.; Whiteman, D.C. Evaluation of Sex-Specific Incidence of Melanoma. JAMA Dermatol. 2020, 156, 553–560. [Google Scholar] [CrossRef]
- Abbott, C.W.; Boyle, S.M.; Pyke, R.M.; McDaniel, L.D.; Levy, E.; Navarro, F.C.; Mellacheruvu, D.; Zhang, S.V.; Tan, M.; Santiago, R.; et al. Prediction of Immunotherapy Response in Melanoma through Combined Modeling of Neoantigen Burden and Immune-Related Resistance Mechanisms. Clin. Cancer Res. 2021, 27, 4265–4276. [Google Scholar] [CrossRef]
- Balatoni, T.; Ladányi, A.; Fröhlich, G.; Czirbesz, K.; Kovács, P.; Pánczél, G.; Bence, E.; Plótár, V.; Liszkay, G. Biomarkers Associated with Clinical Outcome of Advanced Melanoma Patients Treated with Ipilimumab. Pathol. Oncol. Res. 2020, 26, 317–325. [Google Scholar] [CrossRef]
- Wang, S.; Cowley, L.A.; Liu, X.-S. Sex Differences in Cancer Immunotherapy Efficacy, Biomarkers, and Therapeutic Strategy. Molecules 2019, 24, 3214. [Google Scholar] [CrossRef] [Green Version]
- Pala, L.; Conforti, F. The Effect of Patient Sex on the Efficacy and Safety of Anticancer Immunotherapy. Expert Opin. Drug Saf. 2021, 20, 1535–1544. [Google Scholar] [CrossRef]
- Bellenghi, M.; Puglisi, R.; Pontecorvi, G.; De De Feo, A.; Carè, A.; Mattia, G. Sex and Gender Disparities in Melanoma. Cancers 2020, 12, 1819. [Google Scholar] [CrossRef]
- Botticelli, A.; Onesti, C.E.; Zizzari, I.; Cerbelli, B.; Sciattella, P.; Occhipinti, M.; Roberto, M.; Di Pietro, F.; Bonifacino, A.; Ghidini, M.; et al. The Sexist Behaviour of Immune Checkpoint Inhibitors in Cancer Therapy? Oncotarget 2017, 8, 99336–99346. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; Bagnardi, V.; De Pas, T.; Martinetti, M.; Viale, G.; Gelber, R.D.; Goldhirsch, A. Cancer Immunotherapy Efficacy and Patients’ Sex: A Systematic Review and Meta-Analysis. Lancet Oncol. 2018, 19, 737–746. [Google Scholar] [CrossRef]
- Klein, S.L.; Morgan, R. The impact of sex and gender on immunotherapy outcomes. Biol. Sex Differ. 2020, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex Differences in Immune Responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- van der Kooij, M.K.; Dekkers, O.M.; Aarts, M.J.B.; Berkmortel, F.W.P.J.V.D.; Boers-Sonderen, M.J.; de Groot, J.W.B.; Hospers, G.A.P.; Piersma, D.; van Rijn, R.S.; Suijkerbuijk, K.P.M.; et al. Sex-Based Differences in Treatment with Immune Checkpoint Inhibition and Targeted Therapy for Advanced Melanoma: A Nationwide Cohort Study. Cancers 2021, 13, 4639. [Google Scholar] [CrossRef] [PubMed]
- Lai, L.-T.; Gu, W.-G.; Hu, M.-B.; Wang, W.-J.; Wang, S.-S.; Huai, Y.-J.; Mei, J.-H.; Wang, C.-L. Sex-Related Differences in the Efficacy of Immune Checkpoint Inhibitors in Malignancy: A Systematic Review and Meta-Analysis. Aging 2021, 13, 15413–15432. [Google Scholar] [CrossRef]
- Ye, Y.; Jing, Y.; Li, L.; Mills, G.B.; Diao, L.; Liu, H.; Han, L. Sex-Associated Molecular Differences for Cancer Immunotherapy. Nat. Commun. 2020, 11, 1779. [Google Scholar] [CrossRef] [Green Version]
- Dimitriou, F.; Staeger, R.; Ak, M.; Maissen, M.; Kudura, K.; Barysch, M.; Levesque, M.; Cheng, P.; Dummer, R.; Mangana, J. Frequency, Treatment and Outcome of Immune-Related Toxicities in Patients with Immune-Checkpoint Inhibitors for Advanced Melanoma: Results from an Institutional Database Analysis. Cancers 2021, 13, 2931. [Google Scholar] [CrossRef]
- Schweizer, C.; Schubert, P.; Rutzner, S.; Eckstein, M.; Haderlein, M.; Lettmaier, S.; Semrau, S.; Gostian, A.-O.; Frey, B.; Gaipl, U.S.; et al. Prospective Evaluation of the Prognostic Value of Immune-Related Adverse Events in Patients with Non-Melanoma Solid Tumour Treated with PD-1/PD-L1 Inhibitors Alone and in Combination with Radiotherapy. Eur. J. Cancer 2020, 140, 55–62. [Google Scholar] [CrossRef]
- Li, Y.; Meng, Y.; Sun, H.; Ye, L.; Zeng, F.; Chen, X.; Deng, G. The Prognostic Significance of Baseline Neutrophil-to-Lymphocyte Ratio in Melanoma Patients Receiving Immunotherapy. J. Immunother. 2022, 45, 43–50. [Google Scholar] [CrossRef]
- Maillet, D.; Corbaux, P.; Stelmes, J.-J.; Dalle, S.; Locatelli-Sanchez, M.; Perier-Muzet, M.; Duruisseaux, M.; Kiakouama-Maleka, L.; Freyer, G.; Boespflug, A.; et al. Association between Immune-Related Adverse Events and Long-Term Survival Outcomes in Patients Treated with Immune Checkpoint Inhibitors. Eur. J. Cancer 2020, 132, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Michailidou, D.; Khaki, A.R.; Morelli, M.P.; Diamantopoulos, L.; Singh, N.; Grivas, P. Association of Blood Biomarkers and Autoimmunity with Immune Related Adverse Events in Patients with Cancer Treated with Immune Checkpoint Inhibitors. Sci. Rep. 2021, 11, 9029. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Kitano, S.; Takahashi, A.; Tsutsumida, A.; Namikawa, K.; Tanese, K.; Abe, T.; Funakoshi, T.; Yamamoto, N.; Amagai, M.; et al. Nivolumab for Advanced Melanoma: Pretreatment Prognostic Factors and Early Outcome Markers during Therapy. Oncotarget 2016, 7, 77404–77415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, Y.; Tanaka, R.; Maruyama, H.; Ishitsuka, Y.; Okiyama, N.; Watanabe, R.; Fujimoto, M.; Fujisawa, Y. Correlation between Blood Cell Count and Outcome of Melanoma Patients Treated with Anti-PD-1 Antibodies. Jpn. J. Clin. Oncol. 2019, 49, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Ohashi, H.; Takeuchi, S.; Miyagaki, T.; Kadono, T. Increase of Lymphocytes and Eosinophils, and Decrease of Neutrophils at an Early Stage of Anti-PD-1 Antibody Treatment Is a Favorable Sign for Advanced Malignant Melanoma. Drug Discov. Ther. 2020, 14, 117–121. [Google Scholar] [CrossRef]
- Pavan, A.; Calvetti, L.; Maso, A.D.; Attili, I.; Del Bianco, P.; Pasello, G.; Guarneri, V.; Aprile, G.; Conte, P.; Bonanno, L. Peripheral Blood Markers Identify Risk of Immune-Related Toxicity in Advanced Non-Small Cell Lung Cancer Treated with Immune-Checkpoint Inhibitors. Oncologist 2019, 24, 1128–1136. [Google Scholar] [CrossRef] [Green Version]
- Basler, L.; Gabryś, H.S.; Hogan, S.A.; Pavic, M.; Bogowicz, M.; Vuong, D.; Tanadini-Lang, S.; Foerster, R.; Kudura, K.; Huellner, M.W.; et al. Radiomics, Tumor Volume, and Blood Biomarkers for Early Prediction of Pseudoprogression in Patients with Metastatic Melanoma Treated with Immune Checkpoint Inhibition. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2020, 26, 4414–4425. [Google Scholar] [CrossRef] [Green Version]
- Souza, B.D.C.E.; Silva, D.H.M.; Valente, N.Y.S.; Kakizaki, P.; Luce, M.C.A.; Bandeira, L.G. Cutaneous melanoma: A retrospective study of 18 years. Are there gender differences? An. Bras. Dermatol. 2021, 96, 619–623. [Google Scholar] [CrossRef]
- Pala, L.; Conforti, F.; Pagan, E.; Bagnardi, V.; De Pas, T.M.; Mazzarol, G.; Barberis, M.; Pennacchioli, E.; Orsolini, G.; Prestianni, P.; et al. Different Response to Immunotherapy According to Melanoma Histologic Subtype. J. Immunother. 2022, 45, 119–124. [Google Scholar] [CrossRef]
- Pontes, F.; de Souza, L.; de Abreu, M.; Fernandes, L.; Rodrigues, A.; Nascimento, D.D.; Vasconcelos, V.; Soares, C.; Corrêa, D.; Fonseca, F.; et al. Sinonasal Melanoma: A Systematic Review of the Prognostic Factors. Int. J. Oral Maxillofac. Surg. 2020, 49, 549–557. [Google Scholar] [CrossRef]
- Thuaire, A.; Nicot, R.; Boileau, M.; Raoul, G.; Descarpentries, C.; Mouawad, F.; Germain, N.; Mortier, L.; Schlund, M. Oral Mucosal Melanoma—A Systematic Review. J. Stomatol. Oral Maxillofac. Surg. 2022, 5, e425–e432. [Google Scholar] [CrossRef] [PubMed]










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kudura, K.; Basler, L.; Nussbaumer, L.; Foerster, R. Sex-Related Differences in Metastatic Melanoma Patients Treated with Immune Checkpoint Inhibition. Cancers 2022, 14, 5145. https://doi.org/10.3390/cancers14205145
Kudura K, Basler L, Nussbaumer L, Foerster R. Sex-Related Differences in Metastatic Melanoma Patients Treated with Immune Checkpoint Inhibition. Cancers. 2022; 14(20):5145. https://doi.org/10.3390/cancers14205145
Chicago/Turabian StyleKudura, Ken, Lucas Basler, Lukas Nussbaumer, and Robert Foerster. 2022. "Sex-Related Differences in Metastatic Melanoma Patients Treated with Immune Checkpoint Inhibition" Cancers 14, no. 20: 5145. https://doi.org/10.3390/cancers14205145