
Intraoperative Extra Corporeal Membrane Oxygenator for Lung Cancer Resections Does Not Impact Circulating Tumor Cells

 ,
,  , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility, Patient Population, and Management
2.3. Clinical Evaluation and Procedures
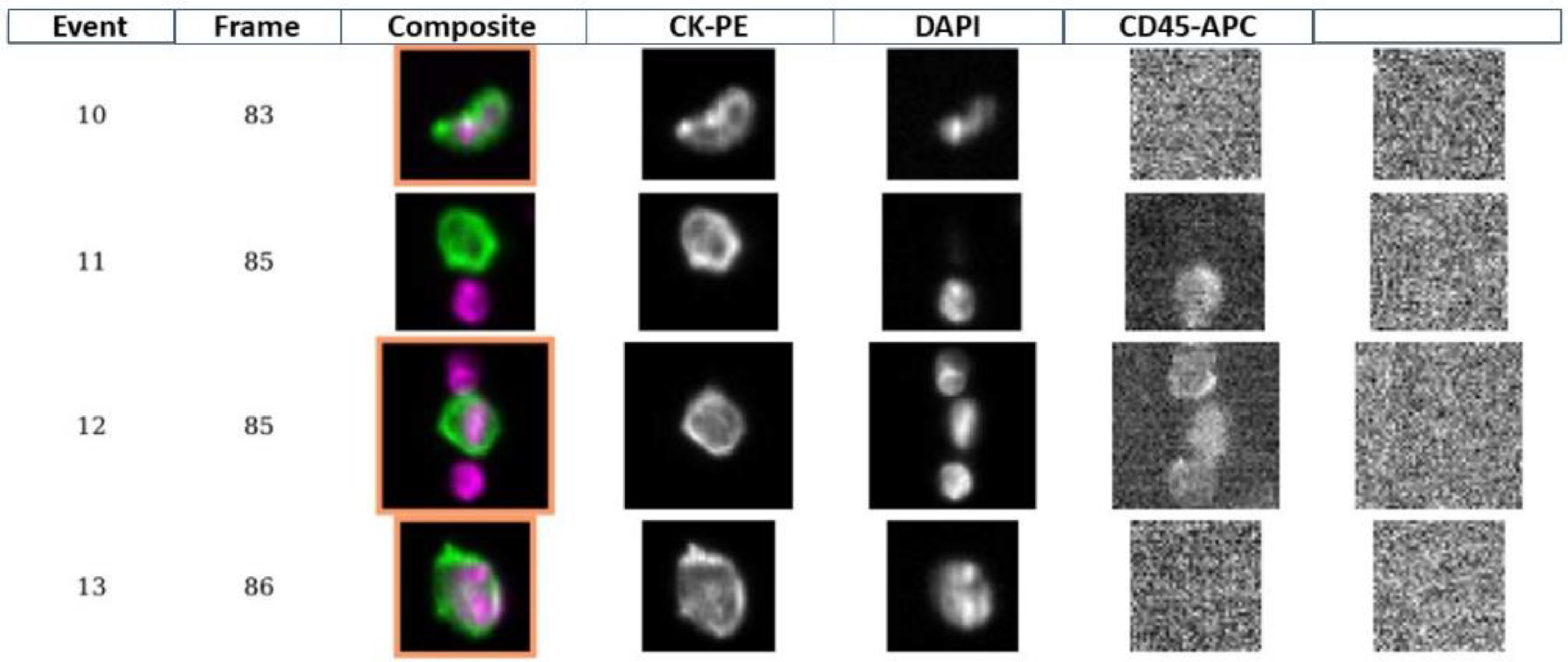
2.4. Circulating Tumor Cells Assessment
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kelly, B.; Carton, E. Extended Indications for Extracorporeal Membrane Oxygenation in the Operating Room. J. Intensive Care Med. 2019, 35, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Gow, K.W.; Lao, O.B.; Leong, T.; Fortenberry, J.D. Extracorporeal life support for adults with malignancy and respiratory or cardiac failure: The Extracorporeal Life Support experience. Am. J. Surg. 2010, 199, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Wohlfarth, P.; Ullrich, R.; Staudinger, T.; Bojic, A.; Robak, O.; Hermann, A.; Lubsczyk, B.; Worel, N.; Fuhrmann, V.; Schoder, M.; et al. Extracorporeal membrane oxygenation in adult patients with hematologic malignancies and severe acute respiratory failure. Crit. Care 2014, 18, R20–R28. [Google Scholar] [CrossRef] [Green Version]
- Allard, W.J.; Matera, J.; Miller, M.C.; Repollet, M.; Connelly, M.C.; Rao, C.; Tibbe, A.G.J.; Uhr, J.W.; Terstappen, L.W.M.M. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin. Cancer Res. 2004, 10, 6897–6904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fehm, T.; Sagalowsky, A.; Clifford, E.; Beitsch, P.; Saboorian, H.; Euhus, D.; Meng, S.; Morrison, L.; Tucker, T.; Lane, N.; et al. Cytogenetic evidence that circulating epithelial cells in patients with carcinoma are malignant. Clin. Cancer Res. 2002, 8, 2073–2084. [Google Scholar] [PubMed]
- Hayes, D.F.; Walker, T.M.; Singh, B.; Vitetta, E.S.; Uhr, J.W.; Gross, S.; Rao, C.; Doyle, G.V.; Terstappen, L. Monitoring expression of HER-2 on circulating epithelial cells in patients with advanced breast cancer. Int. J. Oncol. 2002, 21, 1111–1117. [Google Scholar] [CrossRef]
- O’Hara, S.M.; Moreno, J.G.; Zweitzig, D.R.; Gross, S.; Gomella, L.G.; Terstappen, L. Multigene Reverse Transcription-PCR Profiling of Circulating Tumor Cells in Hormone-Refractory Prostate Cancer. Clin. Chem. 2004, 50, 826–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Racila, E.; Euhus, D.; Weiss, A.J.; Rao, C.; McConnell, J.; Terstappen, L.W.M.M.; Uhr, J.W. Detection and characterization of carcinoma cells in the blood. Proc. Natl. Acad. Sci. USA 1998, 95, 4589–4594. [Google Scholar] [CrossRef] [Green Version]
- Ivanovic, J.; Al-Hussaini, A.; Al-Shehab, D.; Threader, J.; Villeneuve, P.J.; Ramsay, T.; Maziak, D.E.; Gilbert, S.; Shamji, F.M.; Sundaresan, R.S.; et al. Evaluating the Reliability and Reproducibility of the Ottawa Thoracic Morbidity and Mortality Classification System. Ann. Thorac. Surg. 2011, 91, 387–393. [Google Scholar] [CrossRef]
- Suzuki, Y.; Cass, S.; Carvalho, J.L.; DeAnda, A.; Radhakrishnan, R.S. Extracorporeal Membrane Oxygenation for Patients with Thoracic Neoplasms: An Extracorporeal Life Support Organization (ELSO) Registry Analysis. Ann. Thorac. Surg. 2022, in press. [CrossRef]
- ELSO International Summary. 2020. Available online: www.elso.org (accessed on 9 August 2022).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Blanc, K.; Dechartres, A.; Zaimi, R.; Lefebvre, A.; Janet-Vendroux, A.; Fournel, L.; Dermine, H.; Lorut, C.; Becanne, X.; Hamelin-Canny, E.; et al. Patients experiencing early acute respiratory failure have high postoperative mortality after pneumonectomy. J. Thorac. Cardiovasc. Surg. 2018, 156, 2368–2376. [Google Scholar] [CrossRef] [PubMed]
- Rosskopfova, P.; Perentes, J.Y.; Ris, H.-B.; Gronchi, F.; Krueger, T.; Gonzalez, M. Extracorporeal support for pulmonary resection: Current indications and results. World J. Surg. Oncol. 2016, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.; Ye, H.; Cheng, Z.; Liao, X.; Wang, L.; Li, B.; Liang, Y.; Jiang, H. Outcomes from the Use of Perioperative Extracorporeal Membrane Oxygenation in Patients Undergoing Thoracic Surgery: An 8-Year Single-Center Experience. Med. Sci. Monit. 2021, 27, e931842. [Google Scholar] [CrossRef] [PubMed]
- Haines, N.M.; Rycus, P.T.; Zwischenberger, J.B.; Bartlett, R.H.; Ündar, A. Extracorporeal Life Support Registry Report 2008: Neonatal and Pediatric Cardiac Cases. ASAIO J. 2009, 55, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Park, P.K.; Napolitano, L.M.; Bartlett, R.H. Extracorporeal Membrane Oxygenation in Adult Acute Respiratory Distress Syndrome. Crit. Care Clin. 2011, 27, 627–646. [Google Scholar] [CrossRef]
- Jin, Y.-J.; Liu, C.; Li, F. Advances in the application of extracorporeal membrane oxygenation in acute respiratory distress syn-drome. Chin. J. Lung Dis. 2015, 8, 478–481. [Google Scholar]
- Ried, M.; Bein, T.; Philipp, A.; Müller, T.; Graf, B.; Schmid, C.; Zonies, D.; Diez, C.; Hofmann, H.-S. Extracorporeal lung support in trauma patients with severe chest injury and acute lung failure: A 10-year institutional experience. Crit. Care 2013, 17, R110. [Google Scholar] [CrossRef] [Green Version]
- Gao, C.-L.; Rawal, S.K.; Sun, L.; Ali, A.; Connelly, R.R.; Bañez, L.L.; Sesterhenn, I.A.; McLeod, D.G.; Moul, J.W.; Srivastava, S. Diagnostic potential of prostate-specific antigen expressing epithelial cells in blood of prostate cancer patients. Clin. Cancer Res. 2003, 9, 2545–2550. [Google Scholar]
- Ellis, W.J.; Pfitzenmaier, J.; Colli, J.; Arfman, E.; Lange, P.H.; Vessella, R.L. Detection and isolation of prostate cancer cells from peripheral blood and bone marrow. Urology 2003, 61, 277–281. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.M.M.; et al. Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engell, H.C. Cancer cells in the circulating blood: A clinical study on the occurrence of cancer cells in the peripheral blood and in venous blood draining the tumour area at operation. Acta Chir. Scand. Suppl. 1955, 201, 1–70. [Google Scholar] [PubMed]
- Rodriguez-Salas, N.; Jimenez-Gordo, A.M.; Gonzalez, E.; Heras, B.D.L.; Zamora, P.; Espinosa, E.; De Castro, M.F.; Gonzalez-Baron, M. Circulating cancer cells in peripheral blood: A case report. Acta Cytol. 2000, 44, 237–241. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Level | ECMO (N = 8) | Non-ECMO (N = 12) | p-Value |
|---|---|---|---|---|
| Age (years), median (min–max) | 68 (38–75) | 65 (53–79) | 1.00 | |
| Sex, N (%) | Female | 2 (25) | 3 (25) | 1.00 |
| Male | 6 (75) | 9 (75) | ||
| BMI (kg/m2), median (min–max) | 24.0 (18.0–34.9) | 25.3 (17.7–34.1) | 0.44 | |
| ASA, N (%) | 2 | 4 (50) | 5 (45) | 1.00 |
| 3 | 4 (50) | 6 (55) | ||
| Tube, N (%) | Magill | 5 (63) | 0 (0) | 0.004 |
| Robert Shaw Right | 0 (0) | 4 (36) | ||
| Robert Shaw Left | 3 (38) | 7 (64) | ||
| Tube caliber, median (min–max) | 8 (7.5–39) | 39 (37–41) | 0.003 | |
| Side, N (%) | Right | 5 (63) | 6 (50) | 0.67 |
| Left | 3 (38) | 6 (50) | ||
| Histology, N (%) | Adenocarcinoma | 5 (63) | 5 (42) | 0.19 |
| Cystic adenoid carcinoma | 1 (13) | 0 (0) | ||
| Poorly differentiated carcinoma | 0 (0) | 1 (8) | ||
| Squamous cell carcinoma | 1 (13) | 6 (50) | ||
| Myofibroblastic inflammatory tumor | 1 (13) | 0 (0) | ||
| TNM, N (%) a | T1N0 | 0 (0) | 1 (9.1) | - |
| T2N0 | 1 (33) | 2 (18.2) | ||
| T2aN1M1 (single) | 1 (33) | 0 (0.0) | ||
| T3N2 | 0 (0) | 4 (36.4) | ||
| T4N0 | 1 (33) | 2 (18.2) | ||
| T4N1 | 0 (0) | 2 (18.2) | ||
| Stage, N (%) b | IB | 1 (33) | 3 (27) | - |
| IIIA | 1 (33) | 4 (36) | ||
| IIIB | 0 (0) | 4 (36) | ||
| IVA | 1 (33) | 0 (0) | ||
| Induction treatment, N (%) | No | 4 (50) | 7 (58) | 1.00 |
| Yes | 4 (50) | 5 (42) | ||
| Post-op treatment, N (%) | No | 6 (75) | 7 (58) | 0.64 |
| Yes | 2 (25) | 5 (42) |
| Variable | Median (Min–Max) N = 8 |
|---|---|
| ECMO duration (minutes) | 60 (39–132) |
| Ventilation arrest (minutes) | 46 (20–124) |
| Preoperative ACT (seconds) | 143 (108–157) |
| Preoperative ACT after heparinization (seconds) | 275 (246–355) |
| ECMO flow (mL) | |
| T0 | 963 (200–2000) |
| T10 | 2213 (2000–2700) |
| T20 | 2575 (2260–3000) |
| T30 | 2625 (2170–3080) |
| O2 saturation (%) | |
| T0 | 100 (97–100) |
| T10 | 98 (95–100) |
| T20 | 97 (95–100) |
| T30 | 96 (95–99) |
| Arterial pressure (diastolic, mmHg) | |
| T0 | 56 (51–76) |
| T10 | 58 (51–77) |
| T20 | 72 (59–88) |
| T30 | 60 (45–91) |
| Arterial pressure (systolic, mmHg) | |
| T0 | 87 (83–113) |
| T10 | 96 (90–152) |
| T20 | 127 (109–137) |
| T30 | 123 (70–140) |
| Variable | Level | ECMO (N = 8) | Non-ECMO (N = 12) | p-Value |
|---|---|---|---|---|
| Operative time (min), median (min–max) | 105 (32–242) | 176 (97–263) | 0.043 | |
| Post-op complications, N (%) | No | 4 (50) | 6 (50) | 1.00 |
| Yes | 4 (50) | 6 (50) | ||
| ICU stay (days), median (min–max) | 1 (1–4) | 1 (0–3) | 0.30 | |
| Hospital stay (days), median (min–max) | 15 (3–25) | 7 (4–10) | 0.23 | |
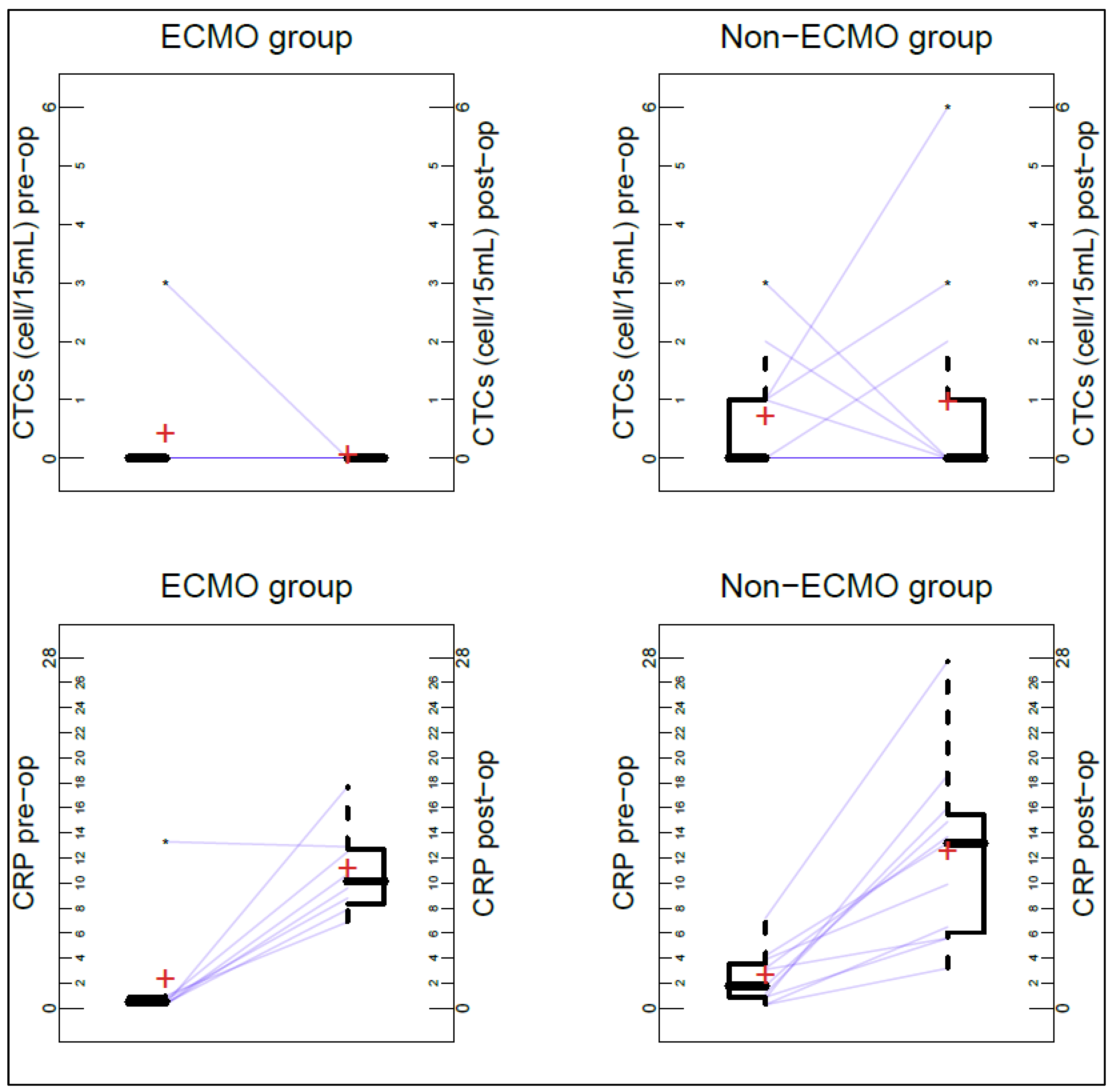
| CTCs post-op > CTCs pre-op, N (%) | No | 8 (100) | 9 (75) | 0.24 |
| Yes | 0 (0) | 3 (25) | ||
| CRP post-op–CRP pre-op, median (min–max) | 8.7 (−0.4–17.4) | 9.0 (2.5–20.5) | 0.80 | |
| Status at last FU, N (%) | NED | 5 (63) | 8 (67) | 1.00 |
| AWD | 2 (25) | 2 (17) | ||
| DOD | 1 (13) | 2 (17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrella, F.; Zorzino, L.; Frassoni, S.; Bagnardi, V.; Casiraghi, M.; Bardoni, C.; Mohamed, S.; Musso, V.; Simonini, E.; Rossi, F.; et al. Intraoperative Extra Corporeal Membrane Oxygenator for Lung Cancer Resections Does Not Impact Circulating Tumor Cells. Cancers 2022, 14, 5004. https://doi.org/10.3390/cancers14205004
Petrella F, Zorzino L, Frassoni S, Bagnardi V, Casiraghi M, Bardoni C, Mohamed S, Musso V, Simonini E, Rossi F, et al. Intraoperative Extra Corporeal Membrane Oxygenator for Lung Cancer Resections Does Not Impact Circulating Tumor Cells. Cancers. 2022; 14(20):5004. https://doi.org/10.3390/cancers14205004
Chicago/Turabian StylePetrella, Francesco, Laura Zorzino, Samuele Frassoni, Vincenzo Bagnardi, Monica Casiraghi, Claudia Bardoni, Shehab Mohamed, Valeria Musso, Emanuele Simonini, Fabiana Rossi, and et al. 2022. "Intraoperative Extra Corporeal Membrane Oxygenator for Lung Cancer Resections Does Not Impact Circulating Tumor Cells" Cancers 14, no. 20: 5004. https://doi.org/10.3390/cancers14205004