
A Multi-Centre Study to Risk Stratify Colorectal Polyp Surveillance Patients Utilising Volatile Organic Compounds and Faecal Immunochemical Test
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methodology
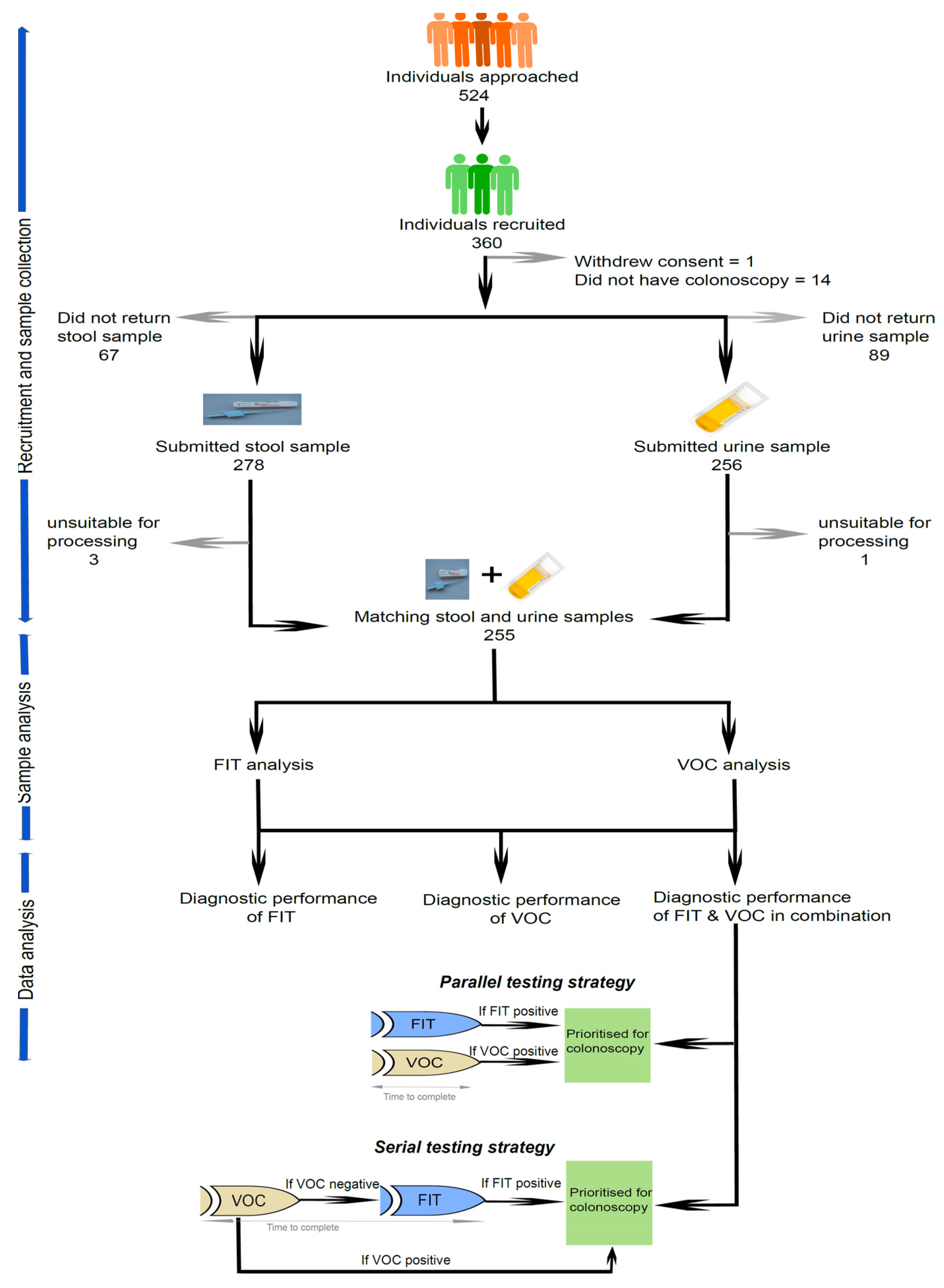
2.1. Study Design and Participant Recruitment
2.2. Stool Sample Collection and Analysis
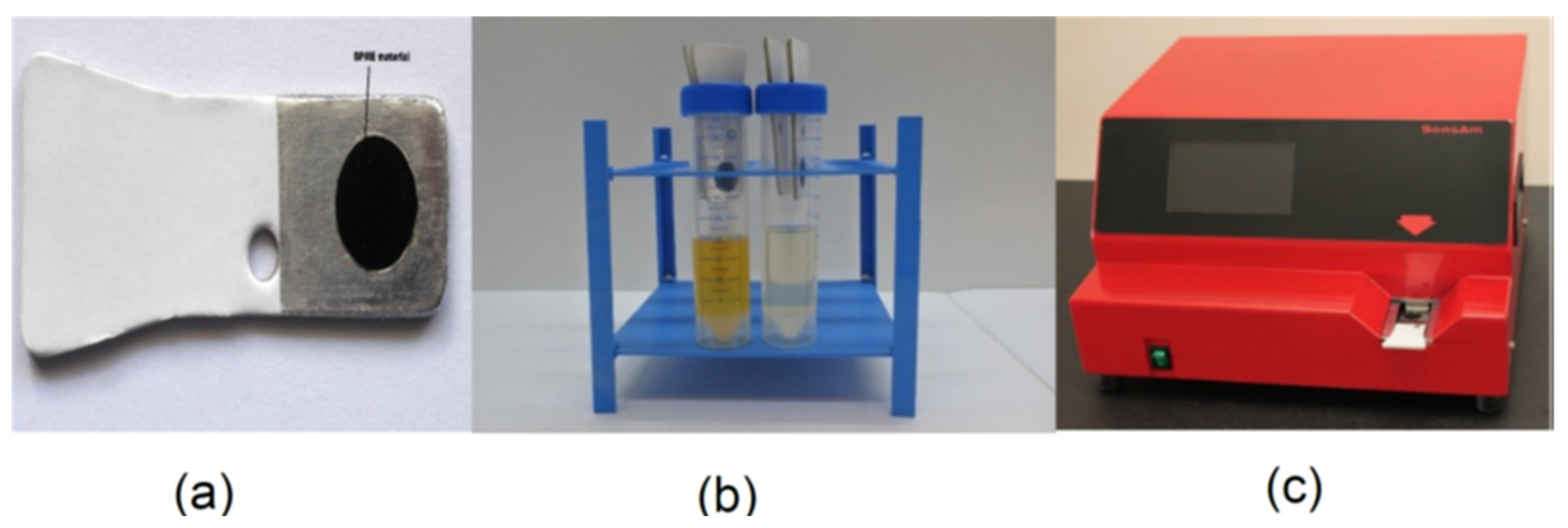
2.3. Urine Sample Collection
2.4. Urine Sample Analysis through E-Nose Technology
2.5. Identification of Chemical Compounds
2.6. Colonoscopy Examination
2.7. Data Collection and Management
2.8. Statistical Analysis
2.8.1. Sample Size Calculation
2.8.2. FIT
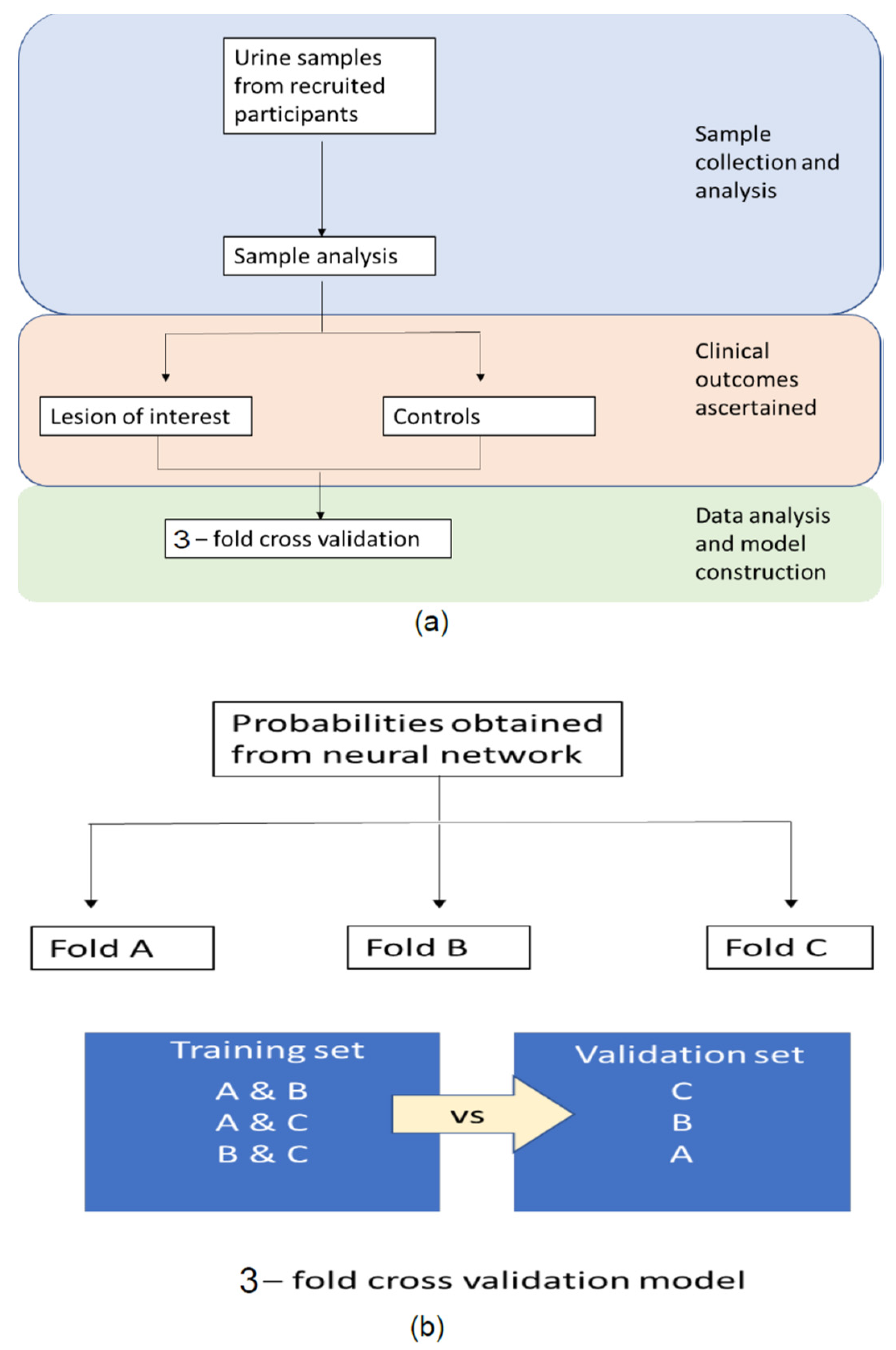
2.8.3. VOC
2.8.4. VOC and FIT Combined
2.9. Patient and Public Involvement
3. Results
3.1. Diagnostic Performance of FIT for the Detection of a High-Risk Finding (≥2 Premalignant Polyps including ≥1 Advanced Polyp or ≥5 Premalignant Polyps)
3.2. The Diagnostic Performance of VOC for the Detection of a High-Risk Finding
3.3. The Combined Diagnostic Performance of VOC and FIT in the Detection of a High-Risk Finding
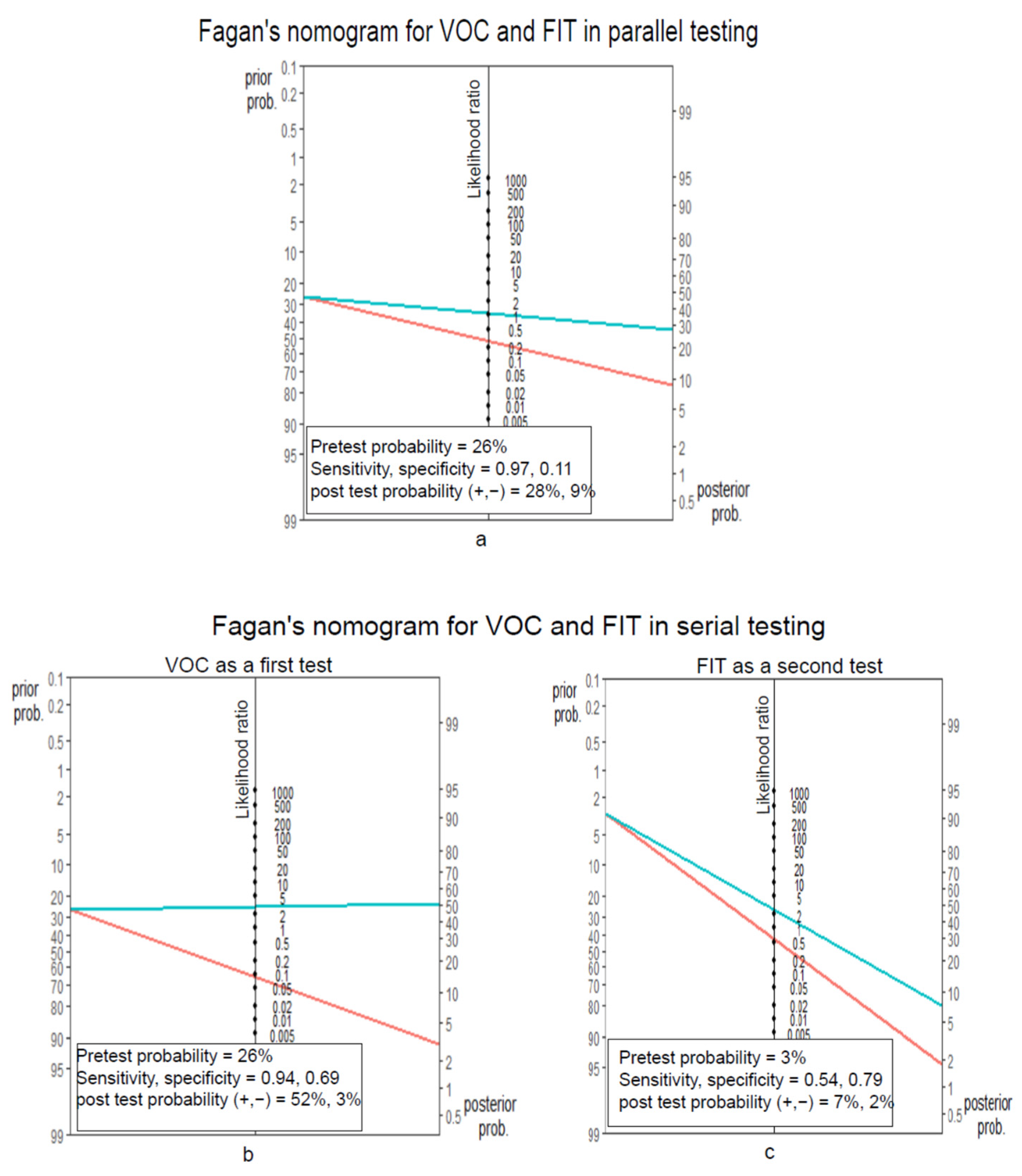
3.3.1. FIT and VOC in a Parallel Testing Manner
3.3.2. VOC then FIT in a Serial Testing Manner
3.4. Comparison of Parallel and Serial Testing in 1000 Polyp Surveillance Patients
3.5. Volatile Organic Compounds Identified in Patients with High-Risk Findings
4. Discussion
4.1. Strengths and Limitations
4.2. Future Research and Unanswered Questions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vatn, M.H.; Stalsberg, H. The prevalence of polyps of the large intestine in Oslo: An autopsy study. Cancer 1982, 49, 819–825. [Google Scholar] [CrossRef]
- Williams, A.R.; Balasooriya, B.A.W.; Day, D.W. Polyps and cancer of the large bowel: A necropsy study in Liverpool. Gut 1982, 23, 835–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conteduca, V.; Sansonno, D.; Russi, S.; Dammacco, F. Precancerous colorectal lesions. Int. J. Oncol. 2013, 43, 973–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkin, W.; Wooldrage, K.; Parkin, D.M.; Kralj-Hans, I.; MacRae, E.; Shah, U.; Duffy, S.; Cross, A.J. Long term effects of once-only flexible sigmoidoscopy screening after 17 years of follow-up: The UK Flexible Sigmoidoscopy Screening randomised controlled trial. Lancet 2017, 389, 1299–1311. [Google Scholar] [CrossRef] [Green Version]
- Schoen, R.E.; Pinsky, P.F.; Weissfeld, J.L.; Yokochi, L.A.; Church, T.; Laiyemo, A.O.; Bresalier, R.; Andriole, G.L.; Buys, S.S.; Crawford, E.D.; et al. Colorectal-cancer incidence and mortality with screening flexible sigmoidoscopy. N. Engl. J. Med. 2012, 366, 2345–2357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holme, Ø.; Løberg, M.; Kalager, M.; Bretthauer, M.; Hernán, M.A.; Aas, E.; Eide, T.J.; Skovlund, E.; Schneede, J.; Tveit, K.M.; et al. Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality: A randomized clinical trial. JAMA 2014, 312, 606–615. [Google Scholar] [CrossRef] [Green Version]
- Winawer, S.J.; Zauber, A.G.; Ho, M.N.; O’brien, M.J.; Gottlieb, L.S.; Sternberg, S.S.; Waye, J.D.; Schapiro, M.; Bond, J.H.; Panish, J.F.; et al. Prevention of Colorectal Cancer by Colonoscopic Polypectomy. N. Engl. J. Med. 1993, 329, 1977–1981. [Google Scholar] [CrossRef]
- Thiis-Evensen, E.; Hoff, G.S.; Sauar, J.; Langmark, F.; Majak, B.M.; Vatn, M.H. Population-based surveillance by colonoscopy: Effect on the incidence of colorectal cancer: Telemark Polyp Study, I. Scand. J. Gastroenterol. 1999, 34, 414–420. [Google Scholar] [CrossRef]
- Atkin, W.S.; Morson, B.C.; Cuzick, J. Long-Term Risk of Colorectal Cancer after Excision of Rectosigmoid Adenomas. N. Engl. J. Med. 1992, 326, 658–662. [Google Scholar] [CrossRef]
- Selby, J.V.; Friedman, G.D.; Quesenberry, C.P.; Weiss, N.S. A Case–Control Study of Screening Sigmoidoscopy and Mortality from Colorectal Cancer. N. Engl. J. Med. 1992, 326, 653–657. [Google Scholar] [CrossRef]
- Müller, A.D.; Sonnenberg, A. Protection by Endoscopy Against Death From Colorectal Cancer: A Case-Control Study Among Veterans. Arch. Intern. Med. 1995, 155, 1741–1748. [Google Scholar] [CrossRef] [PubMed]
- Müller, A.D.; Sonnenberg, A. Prevention of colorectal cancer by flexible endoscopy and polypectomy: A case-control study of 32 702 veterans. Ann. Intern. Med. 1995, 123, 904–910. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M.D.; East, J.; Rees, C.J.; Cripps, N.; Docherty, J.; Dolwani, S.; Kaye, P.V.; Monahan, K.J.; Novelli, M.R.; Plumb, A.; et al. British Society of Gastroenterology/Association of Coloproctology of Great Britain and Ireland/Public Health England post-polypectomy and post-colorectal cancer resection surveillance guidelines. Gut 2020, 69, 201–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkin, W.; Wooldrage, K.; Brenner, A.; Martin, J.; Shah, U.; Perera, S.; Lucas, F.; Brown, J.P.; Kralj-Hans, I.; Greliak, P.; et al. Adenoma surveillance and colorectal cancer incidence: A retrospective, multicentre, cohort study. Lancet Oncol. 2017, 18, 823–834. [Google Scholar] [CrossRef] [Green Version]
- Von Wagner, C.; Ghanouni, A.; Halligan, S.; Smith, S.; Dadswell, E.; Lilford, R.J.; Morton, D.; Atkin, W.; Wardle, J. Patient acceptability and psychologic consequences of CT colonography compared with those of colonoscopy: Results from a multicenter randomized controlled trial of symptomatic patients. Radiology 2012, 263, 723–731. [Google Scholar] [CrossRef] [Green Version]
- Atkin, W.; Dadswell, E.; Wooldrage, K.; Kralj-Hans, I.; Von Wagner, C.; Edwards, R.; Yao, G.; Kay, C.; Burling, D.; Faiz, O.; et al. Computed tomographic colonography versus colonoscopy for investigation of patients with symptoms suggestive of colorectal cancer (SIGGAR): A multicentre randomised trial. Lancet 2013, 381, 1194–1202. [Google Scholar] [CrossRef] [Green Version]
- Thakkar, K.; El-Serag, H.B.; Mattek, N.; Gilger, M. Complications of Pediatric Colonoscopy: A Five-Year Multicenter Experience. Clin. Gastroenterol. Hepatol. 2008, 6, 515. [Google Scholar] [CrossRef] [Green Version]
- Brown, H.; Wyatt, S.; Croft, S.; Gale, N.; Turner, A.; Mulla, A. Scoping the Future: An Evaluation of Endoscopy Capacity Across the NHS in England; Cancer Research UK: Glasgow, UK, 2015; pp. 16–17. [Google Scholar]
- NHS England. NHS England: National Tariff Payment System. 2021. Available online: https://www.england.nhs.uk/pay-syst/national-tariff/national-tariff-payment-system/ (accessed on 1 June 2022).
- Nwankwo, E.C.; Lines, J.; Trehan, S.; Marsh, M.; Trehan, A.; Banwait, K.; Pathapati, S.; Misra, S.; Obokhare, I. Improving Adenoma Detection Rates: The Role of the Fecal Immunochemical Test. Cureus 2021, 13, e14382. [Google Scholar] [CrossRef]
- Chandrapalan, S.; Hee, S.W.; Widlak, M.M.; Farrugia, A.; Alam, M.T.; Smith, S.; Arasaradnam, R.P. Performance of the faecal immunochemical test for the detection of colorectal neoplasms and the role of proton pump inhibitors in their diagnostic accuracy. Colorectal Dis. 2021, 23, 1649–1657. [Google Scholar] [CrossRef]
- Rozen, P.; Levi, Z.; Hazazi, R.; Waked, A.; Vilkin, A.; Maoz, E.; Birkenfeld, S.; Leshno, M.; Niv, Y. Identification of colorectal adenomas by a quantitative immunochemical faecal occult blood screening test depends on adenoma characteristics, development threshold used and number of tests performed. Aliment. Pharmacol. Ther. 2009, 29, 906–917. [Google Scholar] [CrossRef]
- Cross, A.J.; Wooldrage, K.; Robbins, E.C.; Kralj-Hans, I.; MacRae, E.; Piggott, C.; Stenson, I.; Prendergast, A.; Patel, B.; Pack, K.; et al. Faecal immunochemical tests (FIT) versus colonoscopy for surveillance after screening and polypectomy: A diagnostic accuracy and cost-effectiveness study. Gut 2019, 68, 1642–1652. [Google Scholar] [CrossRef] [PubMed]
- Widlak, M.M.; Neal, M.; Daulton, E.; Thomas, C.L.; Tomkins, C.; Singh, B.; Harmston, C.; Wicaksono, A.; Evans, C.; Smith, S.; et al. Risk stratification of symptomatic patients suspected of colorectal cancer using faecal and urinary markers. Colorectal Dis. 2018, 20, O335–O342. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Gatsonis, C.A.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; De Vet, H.C.W.; et al. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 61, 1446–1452. [Google Scholar]
- Chandrapalan, S.; Arasaradnam, R.P. Urine as a biological modality for colorectal cancer detection. Expert Review of Molecular Diagnostics. Expert Rev. Mol. Diagn. 2020, 20, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Arasaradnam, R.P.; Mcfarlane, M.J.; Ryan-Fisher, C.; Westenbrink, E.; Hodges, P.; Thomas, M.G.; Chambers, S.; O’Connell, N.; Bailey, C.; Harmston, C.; et al. Detection of colorectal cancer (CRC) by urinary volatile organic compound analysis. PLoS ONE 2014, 9, e108750. [Google Scholar] [CrossRef] [PubMed]
- Bannaga, A.S.; Kvasnik, F.; Persaud, K.; Arasaradnam, R.P. Differentiating cancer types using a urine test for volatile organic compounds. J. Breath Res. 2021, 15, 017102. [Google Scholar] [CrossRef]
- Thriumani, R.; Zakaria, A.; Hashim, Y.Z.H.Y.; Jeffree, A.I.; Helmy, K.M.; Kamarudin, L.M.; Omar, M.I.; Shakaff, A.Y.M.; Adom, A.H.; Persaud, K.C. A study on volatile organic compounds emitted by in-vitro lung cancer cultured cells using gas sensor array and SPME-GCMS. BMC Cancer 2018, 18, 362. [Google Scholar] [CrossRef]
- The R Foundation. R: The R Project for Statistical Computing. 2018. Available online: https://www.r-project.org/ (accessed on 1 January 2022).
- Sibieude, E.; Khandelwal, A.; Hesthaven, J.S.; Girard, P.; Terranova, N. Fast screening of covariates in population models empowered by machine learning. J. Pharm. Pharm. 2021, 48, 597–609. [Google Scholar] [CrossRef]
- Moody, J.; Darken, C.J. Fast Learning in Networks of Locally-Tuned Processing Units. Neural Comput. 1989, 1, 281–294. [Google Scholar] [CrossRef]
- Fagan, T. Nomogram for Bayes’s Theorem. N. Engl. J. Med. 1975, 293, 257. [Google Scholar]
- Caraguel, C.G.B.; Vanderstichel, R. The two-step Fagan’s nomogram: Ad hoc interpretation of a diagnostic test result without calculation. Evid. Based Med. 2013, 18, 125–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]
- Zhu, X.; Weiser, E.; Jacobson, D.J.; Griffin, J.M.; Limburg, P.J.; Finney Rutten, L.J. Patient preferences on general health and colorectal cancer screening decision-making: Results from a national survey. Patient Educ. Couns. 2021, 105, 1034–1040. [Google Scholar] [CrossRef]
- Markar, S.R.; Chin, S.T.; Romano, A.; Wiggins, T.; Antonowicz, S.; Paraskeva, P.; Ziprin, P.; Darzi, A.; Hanna, G.B. Breath Volatile Organic Compound Profiling of Colorectal Cancer Using Selected Ion Flow-tube Mass Spectrometry. Ann. Surg. 2019, 269, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Altomare, D.F.; Picciariello, A.; Rotelli, M.T.; De Fazio, M.; Aresta, A.; Zambonin, C.G.; Vincenti, L.; Trerotoli, P.; De Vietro, N. Chemical signature of colorectal cancer: Case–control study for profiling the breath print. BJS Open 2020, 4, 1189–1199. [Google Scholar] [CrossRef] [PubMed]
- De Vietro, N.; Aresta, A.; Rotelli, M.T.; Zambonin, C.; Lippolis, C.; Picciariello, A.; Altomare, D.F. Relationship between cancer tissue derived and exhaled volatile organic compound from colorectal cancer patients. Preliminary results. J. Pharm. Biomed. Anal. 2020, 180, 113055. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Value (n = 255) |
|---|---|
| Age, years | |
| Mean (standard deviation, SD) | 67.65 (10.11) |
| Median (interquartile range, IQR) | 69 (60.25 to 75.00) |
| Sex | |
| Female, n (%) | 113 (44) |
| Male, n (%) | 142 (55) |
| Body mass index | |
| Mean (SD) | 27.81 (5.38) |
| Median (IQR) | 27.32 (24.56 to 30.76) |
| FIT value, μg/g faeces | |
| Mean (SD) | 44.91 (124.13) |
| Concurrent medication | |
| Proton pump inhibitors, n (%) | 79 (30) |
| Anticoagulation therapy, n (%) | 25 (10) |
| Antiplatelet therapy, n (%) | 20 (8) |
| NSAID and aspirin, n (%) | 27 (10) |
| Current alcohol consumption, n (%) | 126 (49) |
| Smoking | |
| Current smoker, n (%) | 23 (9) |
| Former smoker, n (%) | 59 (23) |
| Never smoked, n (%) | 173 (67) |
| Colonoscopy findings | |
| Normal, n (%) | 73 (28) |
| All adenoma, n (%) | 162 (63) |
| High-risk finding (among all adenoma), n (%) | 68 (26) |
| Other pathologies (diverticulosis, microscopic colitis) | 15 (6) |
| CRC, n (%) | 5 (2) |
| Cut-Off Levels | True Positives | True Negatives | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|
| At 3 ugHb/g faeces | 42 | 123 | 0.62 (0.50, 0.73) | 0.66 (0.59, 0.72) | 0.39 (0.32, 0.45) | 0.83 (0.77, 0.89) |
| At 5 ugHb/g faeces | 38 | 136 | 0.56 (0.44, 0.68) | 0.73 (0.66, 0.79) | 0.42 (0.34, 0.49) | 0.83 (0.78, 0.86) |
| At 7 ugHb/g faeces | 37 | 140 | 0.54 (0.41, 0.65) | 0.75 (0.69, 0.81) | 0.43 (0.35, 0.51) | 0.82 (0.78, 0.86) |
| At 10 ugHb/g faeces | 37 | 148 | 0.54 (0.41, 0.65) | 0.79 (0.73, 0.84) | 0.47 (0.39, 0.56) | 0.83 (0.79, 0.86) |
| At 20 μg Hb/g faeces | 33 | 159 | 0.49 (0.37, 0.61) | 0.85 (0.79, 0.89) | 0.53 (0.42, 0.63) | 0.83 (0.78, 0.85) |
| At 80 μg Hb/g faeces | 17 | 170 | 0.25 (0.16, 0.37) | 0.91 (0.86, 0.95) | 0.50 (0.34, 0.64) | 0.78 (0.74, 0.79) |
| At 100 μg Hb/g faeces | 16 | 172 | 0.23 (0.13, 0.34) | 0.92 (0.88, 0.95) | 0.50 (0.35, 0.66) | 0.77 (0.74, 0.89) |
| At 120 μg Hb/g faeces | 14 | 172 | 0.20 (0.11, 0.31) | 0.92 (0.88, 0.95) | 0.47 (0.31, 0.63) | 0.77 (0.74, 0.78) |
| Cut-Off Levels | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|
| 0.78 | 0.99 (0.94, 0.99) | 0.48 (0.42, 0.54) | 0.66 | 0.98 |
| 0.81 | 0.98 (0.92, 0.99) | 0.54 (0.48, 0.60) | 0.68 | 0.96 |
| 0.88 | 0.94 (0.88, 0.98) | 0.69 (0.64, 0.75) | 0.75 | 0.92 |
| 0.94 | 0.66 (0.55, 0.75) | 0.76 (0.70, 0.80) | 0.73 | 0.69 |
| 0.95 | 0.43 (0.33, 0.53) | 0.77 (0.72, 0.82) | 0.66 | 0.57 |
| Sensitivity | Specificity | Test Positives | Test Negatives | High-Risk Findings Detected among Those Tested Positive | High-Risk Findings Detected among Those Tested Negative | Total Colonoscopies Needed | Number Needed to Scope to Detect One High-Risk Finding | |
|---|---|---|---|---|---|---|---|---|
| Colonoscopy for all of the patients on polyp surveillance programme (current practice) | N/A | N/A | N/A | N/A | 260 | N/A | 1000 | 4 |
| Parallel testing | 0.97 | 0.11 | 911 | 89 | 252 | 8 | 911 | 4 |
| Serial testing | ||||||||
| VOC as a first test | 0.94 | 0.69 | 474 | 526 | 244 | 16 | 474 | 2 |
| FIT as a second test | 0.54 | 0.79 | 116 | 410 | 9 | 7 | 116 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandrapalan, S.; Khasawneh, F.; Singh, B.; Lewis, S.; Turvill, J.; Persaud, K.; Arasaradnam, R.P. A Multi-Centre Study to Risk Stratify Colorectal Polyp Surveillance Patients Utilising Volatile Organic Compounds and Faecal Immunochemical Test. Cancers 2022, 14, 4951. https://doi.org/10.3390/cancers14194951
Chandrapalan S, Khasawneh F, Singh B, Lewis S, Turvill J, Persaud K, Arasaradnam RP. A Multi-Centre Study to Risk Stratify Colorectal Polyp Surveillance Patients Utilising Volatile Organic Compounds and Faecal Immunochemical Test. Cancers. 2022; 14(19):4951. https://doi.org/10.3390/cancers14194951
Chicago/Turabian StyleChandrapalan, Subashini, Farah Khasawneh, Baljit Singh, Stephen Lewis, James Turvill, Krishna Persaud, and Ramesh P. Arasaradnam. 2022. "A Multi-Centre Study to Risk Stratify Colorectal Polyp Surveillance Patients Utilising Volatile Organic Compounds and Faecal Immunochemical Test" Cancers 14, no. 19: 4951. https://doi.org/10.3390/cancers14194951