

Prostate-Specific Antigen Bounce after 125I Brachytherapy Using Stranded Seeds with Intraoperative Optimization for Prostate Cancer

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. LDR-Brachytherapy
2.3. Definitions of PSA Bounce
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
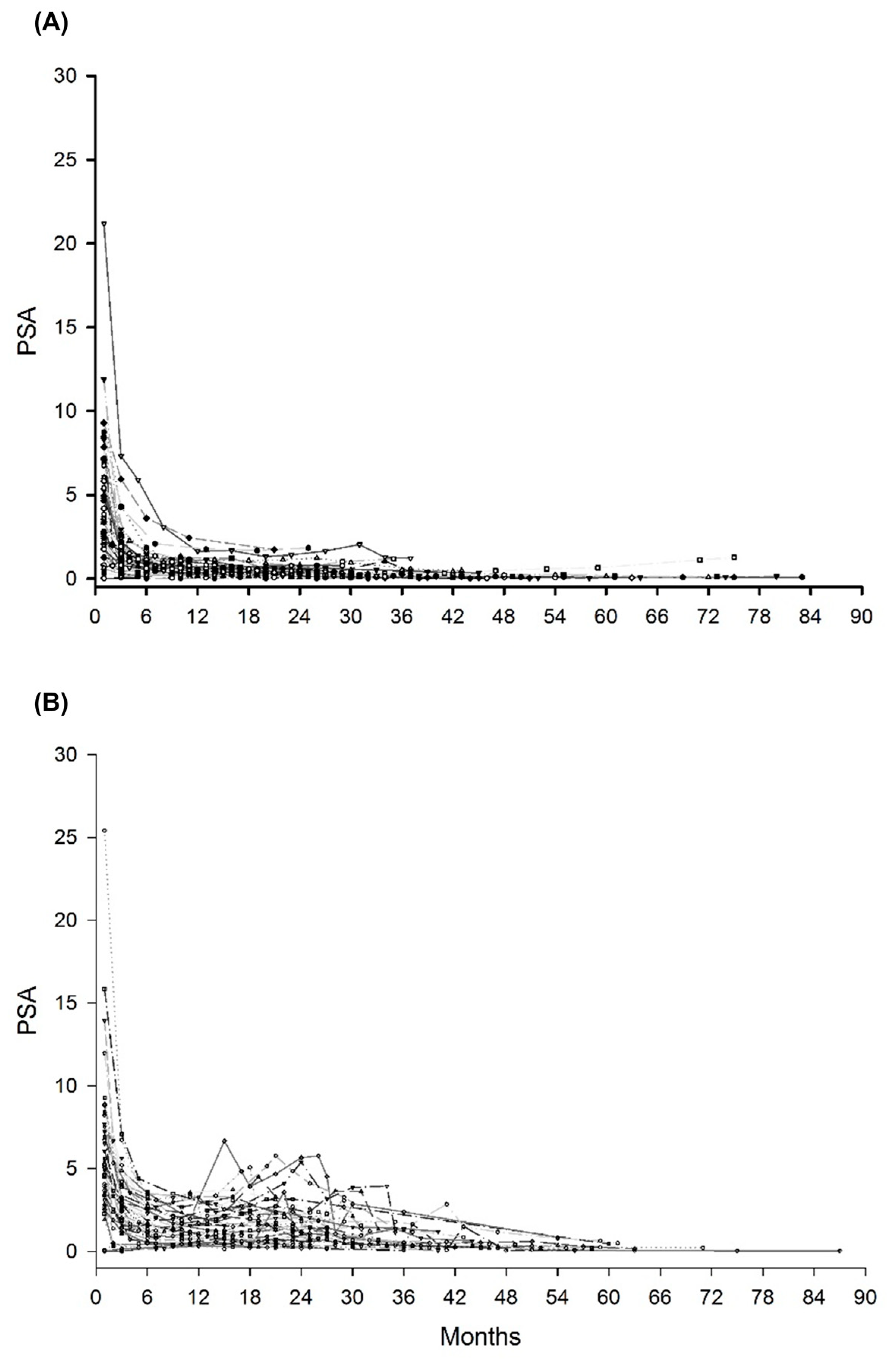
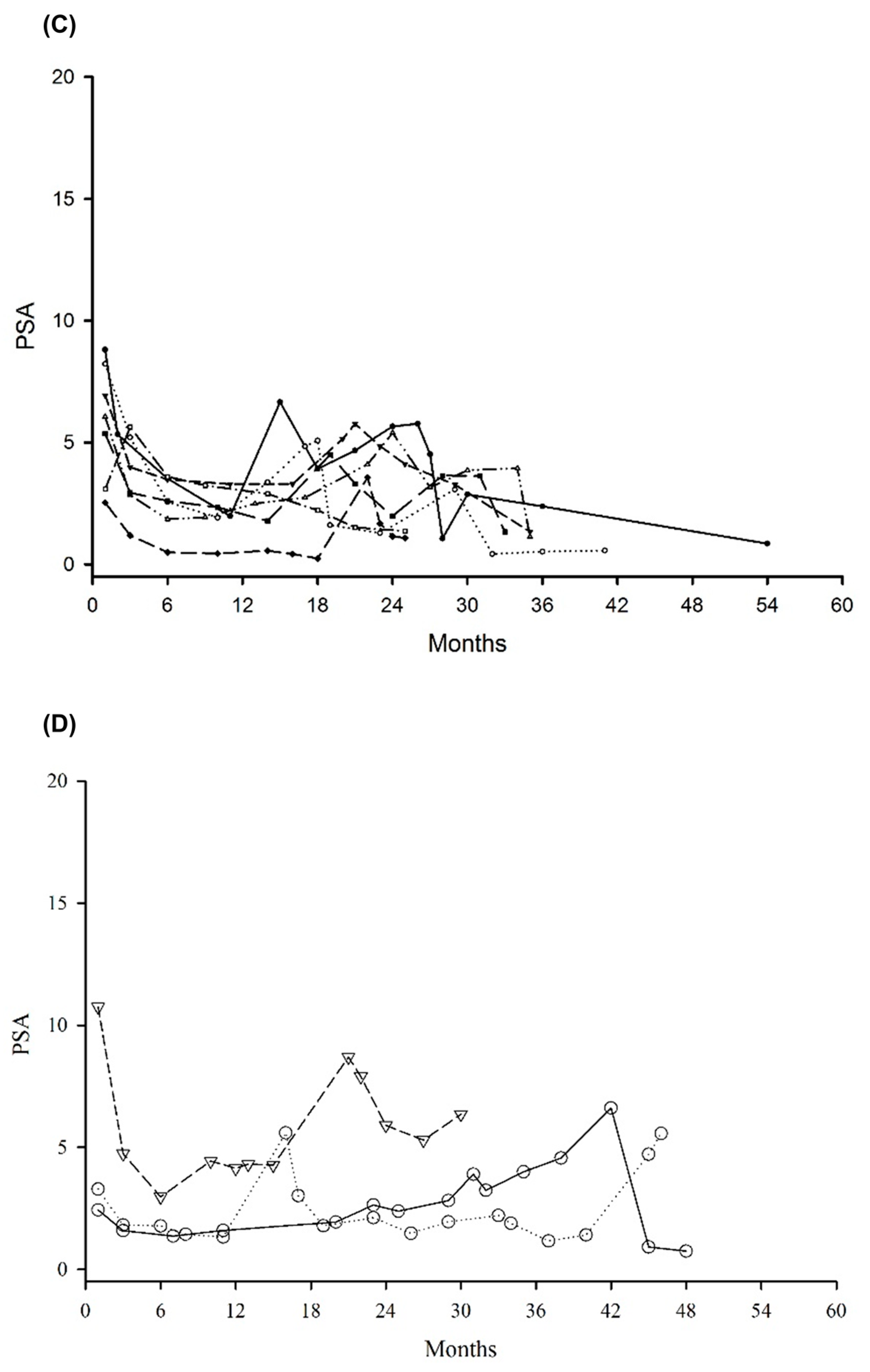
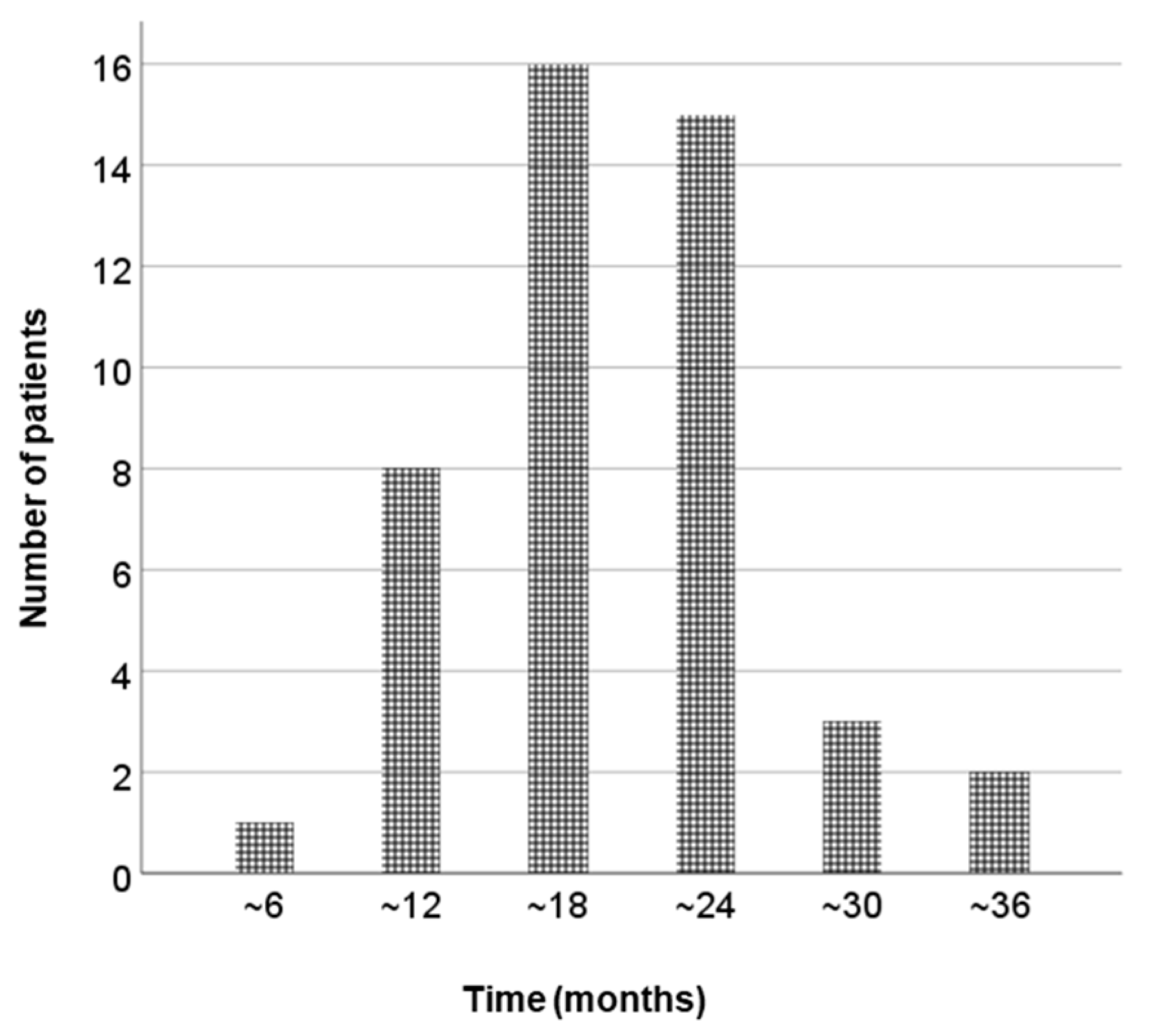
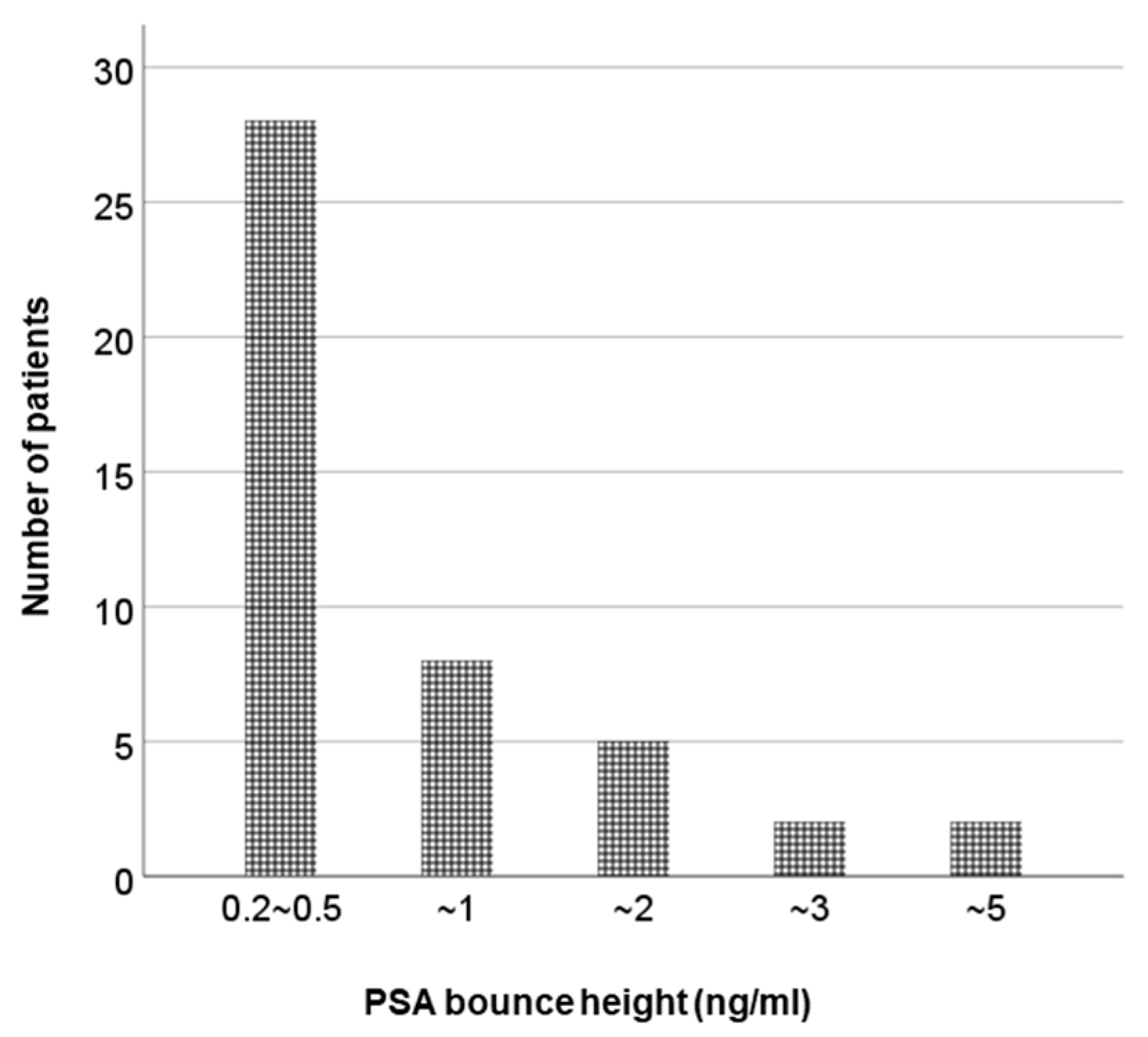
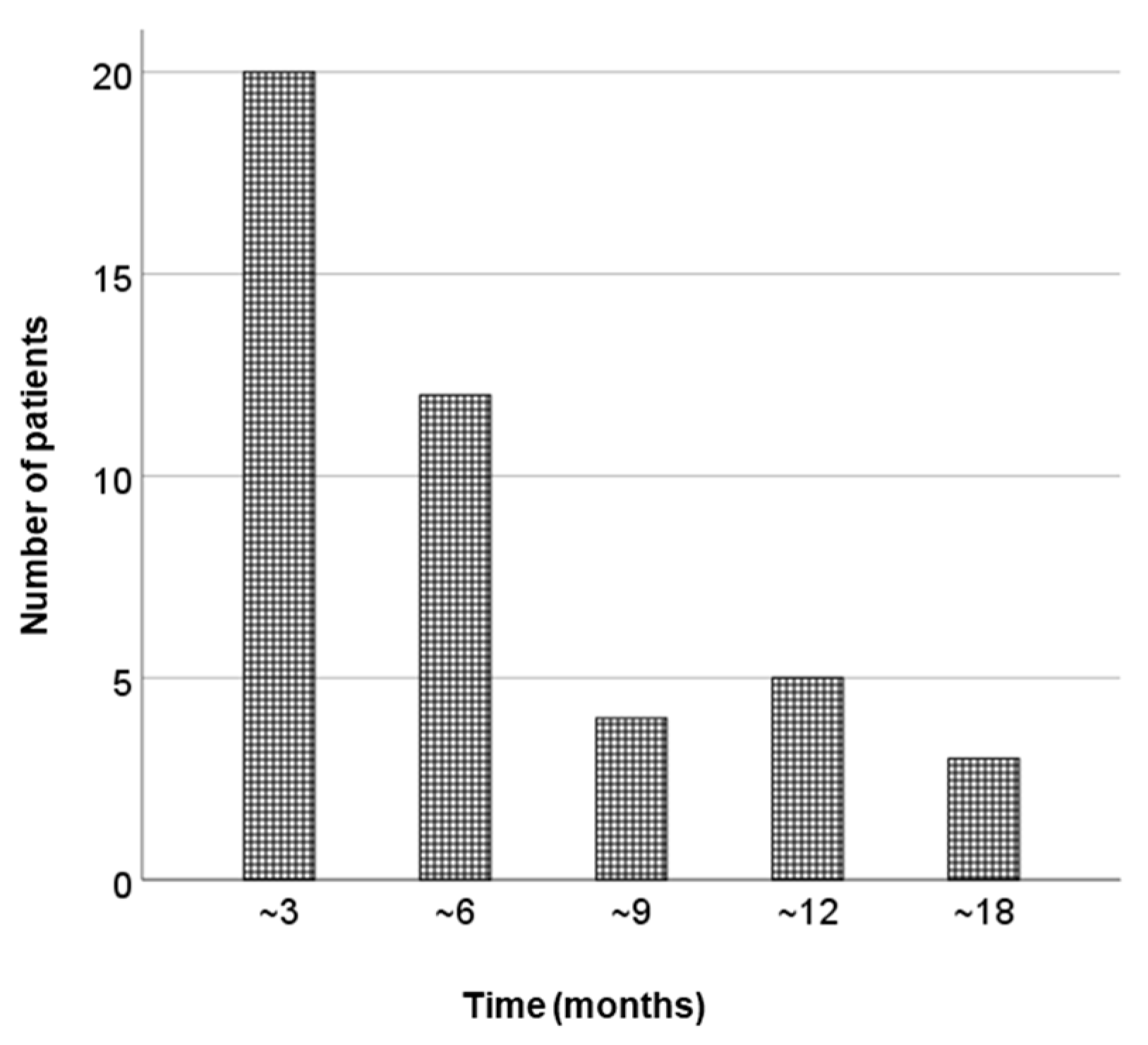
3.2. Analysis of Bounce Phenomenon
3.3. Analysis of Large Bounce Phenomenon
3.4. Early Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Routman, D.M.; Funk, R.K.; Stish, B.J.; Mynderse, L.A.; Wilson, T.M.; McLaren, R.; Harmsen, W.S.; Mara, K.; Deufel, C.L.; Furutani, K.M.; et al. Permanent prostate brachytherapy monotherapy with I-125 for low- and intermediate-risk prostate cancer: Outcomes in 974 patients. Brachytherapy 2018, 18, 1–7. [Google Scholar] [CrossRef]
- Crook, J.; Borg, J.; Evans, A.; Toi, A.; Saibishkumar, E.P.; Fung, S.; Ma, C. 10-year experience with i-125 prostate brachytherapy at the princess margaret hospital: Results for 1,100 patients. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Vuolukka, K.; Auvinen, P.; Palmgren, J.-E.; Voutilainen, T.; Aaltomaa, S.; Kataja, V. Long-term efficacy and urological toxicity of low-dose-rate brachytherapy (LDR-BT) as monotherapy in localized prostate cancer. Brachytherapy 2019, 18, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Kittel, J.A.; Reddy, C.A.; Smith, K.L.; Stephans, K.L.; Tendulkar, R.D.; Ulchaker, J.; Angermeier, K.; Campbell, S.; Stephenson, A.; Klein, E.A.; et al. Long-term efficacy and toxicity of low-dose-rate 125I prostate brachytherapy as monotherapy in low-, intermediate-, and high-risk prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Caloglu, M.; Ciezki, J.P.; Reddy, C.A.; Angermeier, K.; Ulchaker, J.; Chehade, N.; Altman, A.; Magi-Galuzzi, C.; Klein, E.A. PSA Bounce and Biochemical Failure After Brachytherapy for Prostate Cancer: A Study of 820 Patients With a Minimum of 3 Years of Follow-Up. Int. J. Radiat. Oncol. 2011, 80, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Hinnen, K.A.; Monninkhof, E.M.; Battermann, J.J.; van Roermund, J.; Frank, S.J.; van Vulpen, M. Prostate Specific Antigen Bounce Is Related to Overall Survival in Prostate Brachytherapy. Int. J. Radiat. Oncol. 2011, 82, 883–888. [Google Scholar] [CrossRef] [Green Version]
- Naghavi, A.O.; Strom, T.J.; Nethers, K.; Cruz, A.A.; Figura, N.B.; Shrinath, K.; Yue, B.; Kim, J.; Biagioli, M.C.; Fernandez, D.C.; et al. Clinical implications of a prostate-specific antigen bounce after radiation therapy for prostate cancer. Int. J. Clin. Oncol. 2014, 20, 598–604. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Souhami, L.; Mansure, J.J.; Duclos, M.; Aprikian, A.; Faria, S.; David, M.; Cury, F.L. Prostate-specific antigen bounce after high-dose-rate prostate brachytherapy and hypofractionated external beam radiotherapy. Brachytherapy 2014, 13, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Hackett, C.; Ghosh, S.; Sloboda, R.; Martell, K.; Lan, L.; Pervez, N.; Pedersen, J.; Yee, D.; Murtha, A.; Amanie, J.; et al. Distinguishing prostate-specific antigen bounces from biochemical failure after low-dose-rate prostate brachytherapy. J. Contemp. Brachytherapy 2014, 6, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Kanzaki, H.; Kataoka, M.; Nishikawa, A.; Uwatsu, K.; Nagasaki, K.; Nishijima, N.; Hashine, K. Kinetics differences between PSA bounce and biochemical failure in patients treated with 125I prostate brachytherapy. Jpn. J. Clin. Oncol. 2015, 45, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Kubo, K.; Wadasaki, K.; Kimura, T.; Murakami, Y.; Kajiwara, M.; Teishima, J.; Matsubara, A.; Nagata, Y. Clinical features of prostate-specific antigen bounce after 125I brachytherapy for prostate cancer. J. Radiat. Res. 2018, 59, 649–655. [Google Scholar] [CrossRef]
- E Sylvester, J.; Blasko, J.C.; Grimm, P.D.; Meier, R.; A Malmgren, J. Ten-year biochemical relapse-free survival after external beam radiation and brachytherapy for localized prostate cancer: The Seattle experience. Int. J. Radiat. Oncol. 2003, 57, 944–952. [Google Scholar] [CrossRef]
- Kim, H.; Kim, J.W.; Hong, S.J.; Rha, K.H.; Lee, C.-G.; Yang, S.C.; Choi, Y.D.; Suh, C.-O.; Cho, J. Treatment outcome of localized prostate cancer by 70 Gy hypofractionated intensity-modulated radiotherapy with a customized rectal balloon. Radiat. Oncol. J. 2014, 32, 187–197. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical Outcome After Radical Prostatectomy, External Beam Radiation Therapy, or Interstitial Radiation Therapy for Clinically Localized Prostate Cancer. JAMA J. Am. Med. Assoc. 1998, 280, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Charret, J.; Baumann, A.S.; Eschwege, P.; Moreau, J.L.; Bernier, V.; Falk, A.T.; Salleron, J.; Peiffert, D. Prostate-specific antigen bounce in patients treated before 60 years old by iodine 125 brachytherapy for prostate cancer is frequent and not a prognostic factor. Brachytherapy 2018, 17, 888–894. [Google Scholar] [CrossRef]
- Roach, M.T.; Hanks, G.; Thames, H.J.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the rtog-astro phoenix consensus conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef]
- Crook, J.; Gillan, C.; Yeung, I.; Austen, L.; McLean, M.; Lockwood, G. PSA Kinetics and PSA Bounce Following Permanent Seed Prostate Brachytherapy. Int. J. Radiat. Oncol. 2007, 69, 426–433. [Google Scholar] [CrossRef]
- Critz, F.A.; Williams, W.H.; Benton, J.B.; Levinson, A.K.; Holladay, C.T.; Holladay, D.A. Prostate specific antigen bounce after radioactive seed implantation followed by external beam radiation for prostate cancer. J. Urol. 2000, 163, 1085–1089. [Google Scholar] [CrossRef]
- Ciezki, J.P.; Reddy, C.A.; Garcia, J.; Angermeier, K.; Ulchaker, J.; Mahadevan, A.; Chehade, N.; Altman, A.; Klein, E.A. PSA kinetics after prostate brachytherapy: PSA bounce phenomenon and its implications for PSA doubling time. Int. J. Radiat. Oncol. 2005, 64, 512–517. [Google Scholar] [CrossRef]
- Stock, R.G.; Stone, N.N.; Cesaretti, J.A. Prostate-specific antigen bounce after prostate seed implantation for localized prostate cancer: Descriptions and implications. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 448–453. [Google Scholar] [CrossRef]
- Toledano, A.; Chauveinc, L.; Flam, T.; Thiounn, N.; Solignac, S.; Timbert, M.; Rosenwald, J.-C.; Cosset, J.-M. PSA bounce after permanent implant prostate brachytherapy may mimic a biochemical failure: A study of 295 patients with a minimum 3-year followup. Brachytherapy 2006, 5, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Reed, D.; Wallner, K.; Merrick, G.; Buskirk, S.; True, L. Clinical correlates to PSA spikes and positive repeat biopsies after prostate brachytherapy. Urology 2003, 62, 683–688. [Google Scholar] [CrossRef]
- Mitchell, D.M.; Swindell, R.; Elliott, T.; Wylie, J.P.; Taylor, C.; Logue, J.P. Analysis of prostate-specific antigen bounce after I125 permanent seed implant for localised prostate cancer. Radiother. Oncol. 2008, 88, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Das, P.; Chen, M.-H.; Valentine, K.; Lopes, L.; A Cormack, R.; A Renshaw, A.; Tempany, C.M.; Kumar, S.; D’Amico, A.V. Using the magnitude of PSA bounce after MRI-guided prostate brachytherapy to distinguish recurrence, benign precipitating factors, and idiopathic bounce. Int. J. Radiat. Oncol. 2002, 54, 698–702. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Offord, C.P.; Kimura, G.; Kuribayashi, S.; Takeda, H.; Tsuchiya, S.; Shimojo, H.; Kanno, H.; Bozic, I.; A Nowak, M.; et al. Tumour and immune cell dynamics explain the PSA bounce after prostate cancer brachytherapy. Br. J. Cancer 2016, 115, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Nakai, Y.; Tanaka, N.; Asakawa, I.; Anai, S.; Miyake, M.; Morizawa, Y.; Hori, S.; Owari, T.; Fujii, T.; Yamaki, K.; et al. Prostate-specific antigen bounce after 125I-brachytherapy for prostate cancer is a favorable prognosticator in patients who are biochemical recurrence-free at 4 years and correlates with testosterone. Jpn. J. Clin. Oncol. 2020, 50, 58–65. [Google Scholar] [CrossRef]
- Merrick, G.S.; Butler, W.M.; Wallner, K.E.; Lief, J.H.; Hinerman-Mulroy, A.; Galbreath, R.W. Prostate-specific antigen (PSA) velocity and benign prostate hypertrophy predict for PSA spikes following prostate brachytherapy. Brachytherapy 2003, 2, 181–188. [Google Scholar] [CrossRef]
- Thompson, A.; Keyes, M.; Pickles, T.; Palma, D.; Moravan, V.; Spadinger, I.; Lapointe, V.; Morris, W.J. Evaluating the phoenix definition of biochemical failure after (125)I prostate brachytherapy: Can psa kinetics distinguish psa failures from psa bounces? Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 415–421. [Google Scholar] [CrossRef]
- Engeler, D.S.; Schwab, C.; Thöni, A.F.; Hochreiter, W.; Prikler, L.; Suter, S.; Stucki, P.; Schiefer, J.; Plasswilm, L.; Schmid, H.-P.; et al. PSA bounce after 125I-brachytherapy for prostate cancer as a favorable prognosticator. Strahlenther. Onkol. 2015, 191, 787–791. [Google Scholar] [CrossRef]
- Hanlon, A.L.; Pinover, W.H.; Horwitz, E.M.; E Hanks, G. Patterns and fate of PSA bouncing following 3D-CRT. Int. J. Radiat. Oncol. 2001, 50, 845–849. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Total | No Bounce | PSA Bounce | p-Value |
|---|---|---|---|---|
| n = 100 | n = 55 | n = 45 | ||
| Age (years) | 0.005 | |||
| Range | 46–82 | 50–82 | 46–77 | |
| Median (Q1–Q3) | 64 (59–70) | 65 (61–73) | 60 (57.5–68) | |
| Gleason score | 0.411 | |||
| 6 (3 + 3) | 55 (55%) | 28 (50%) | 27 (60%) | |
| 7 (3 + 4) | 21 (21%) | 11 (20%) | 10 (22%) | |
| 7 (4 + 3) | 13 (13%) | 8 (15%) | 5 (11%) | |
| 8 (4 + 4) | 11 (11%) | 8 (15%) | 3 (7%) | |
| T stage | 0.512 | |||
| T1c-T2a | 79 (79%) | 43 (78%) | 36 (80%) | |
| T2b-T2c | 21 (21%) | 12 (22%) | 9 (20%) | |
| Pre-BT PSA value, ng/mL | 0.245 | |||
| Range | 2.8–32.9 | 3.0–20.6 | 2.8–32.9 | |
| Median (Q1–Q3) | 7.4 (5.5–9.7) | 7.4 (5.6–9.3) | 7.4 (5.4–11.9) | |
| Pre-BT PSA, n (%) | 0.440 | |||
| <10 | 77 (77%) | 44 (80%) | 33 (73%) | |
| 10–20 | 19 (19%) | 10 (18%) | 9 (20%) | |
| ≥20 | 4 (4%) | 1 (2%) | 3 (7%) | |
| MSKCC risk group [12] | 0.815 | |||
| Low | 45 (45%) | 25 (46%) | 20 (44%) | |
| Intermediate | 49 (49%) | 26 (47%) | 23 (51%) | |
| High | 6 (6%) | 4 (7%) | 2 (4%) | |
| D’Amico risk group [14] | 0.941 | |||
| Low | 37 (37%) | 20 (36%) | 17 (38%) | |
| Intermediate | 46 (46%) | 25 (46%) | 21 (47%) | |
| High | 17 (17%) | 10 (18%) | 7 (15%) | |
| ADT before BT | 0.728 | |||
| No | 83 (83%) | 45 (82%) | 38 (84%) | |
| Yes | 17 (17%) | 10 (18%) | 7 (16%) | |
| Pre-BT prostate volume, cc | 0.024 | |||
| Range | 14.0–48.0 | 16.7–44.7 | 14.0–48.0 | |
| Median (Q1, Q3) | 28.9 (23.8–35.7) | 27.1 (22.9–32.8) | 31.2 (24.3–39.3) | |
| Number of implanted seeds | 0.030 | |||
| Median (Range) | 76 (52–102) | 74 (52–100) | 80 (55–102) | |
| D90, Gy, median (range) | 149.9 (131.0–174.9) | 151.1 (131.1–173.5) | 149.5 (131.0–174.9) | 0.501 |
| PSA, prostate-specific antigen; BT, brachytherapy; ADT, androgen deprivation therapy; MSKCC, Memorial Sloan Kettering Cancer Center | ||||
| Characteristic | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (≤60 vs. >60 years) | 0.296 | 0.126–0.895 | 0.005 | 0.455 | 0.175–1.183 | 0.106 |
| Gleason score (6 vs. >6) | 0.691 | 0.312–1.534 | 0.364 | |||
| T stage (T1c and T2a vs. T2b and T2c) | 0.896 | 0.339–2.366 | 0.824 | |||
| Pretreatment PSA value | 1.052 | 0.968–1.143 | 0.230 | |||
| PSA nadir value at 2 years | 3.873 | 1.817–8.254 | <0.001 | 2.657 | 1.194–5.914 | 0.017 |
| MSKCC risk group [12] (low vs. intermediate and high) | 1.042 | 0.472–2.300 | 0.920 | |||
| D’Amico risk group [14] (low vs. intermediate and high) | 0.941 | 0.416–2.127 | 0.884 | |||
| Hormone therapy (no vs. yes) | 0.829 | 0.288–2.388 | 0.728 | |||
| Prostate volume (cc) (≤30 vs. >30) | 3.083 | 1.358–7.003 | 0.007 | 1.940 | 0.772–4.875 | 0.106 |
| PSA, Prostate-specific antigen; MSKCC, Memorial Sloan Kettering Cancer Center | ||||||
| Characteristic | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (≤60 vs. >60 years) | 0.058 | 0.007–0.506 | 0.010 | 0.055 | 0.005–0.666 | 0.023 |
| Gleason score (6 vs. >6) | 0.465 | 0.084–2.520 | 0.375 | |||
| T stage (T1c and T2a vs. T2b and T2c) | 1.558 | 0.280–8.661 | 0.613 | |||
| Pretreatment PSA value | 1.076 | 0.956–1.212 | 0.224 | |||
| PSA nadir value at 2 years | 4.008 | 1.640–9.797 | 0.002 | 4.961 | 1.448–16.998 | 0.011 |
| MSKCC Risk group [12] (low vs. intermediate and high) | 0.302 | 0.056–1.637 | 0.165 | |||
| D’Amico Risk group [14] (low vs. intermediate and high) | 1.509 | 0.278–8.198 | 0.634 | |||
| Hormone therapy (no vs. yes) | 2.080 | 0.369–11.738 | 0.407 | |||
| Prostate volume (cc) (≤30 vs. >30) | 3.312 | 0.611–17.960 | 0.165 | |||
| PSA, prostate-specific antigen; MSKCC, Memorial Sloan Kettering Cancer Center | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, T.H.; Lee, J.J.B.; Cho, J. Prostate-Specific Antigen Bounce after 125I Brachytherapy Using Stranded Seeds with Intraoperative Optimization for Prostate Cancer. Cancers 2022, 14, 4907. https://doi.org/10.3390/cancers14194907
Kim TH, Lee JJB, Cho J. Prostate-Specific Antigen Bounce after 125I Brachytherapy Using Stranded Seeds with Intraoperative Optimization for Prostate Cancer. Cancers. 2022; 14(19):4907. https://doi.org/10.3390/cancers14194907
Chicago/Turabian StyleKim, Tae Hyung, Jason Joon Bock Lee, and Jaeho Cho. 2022. "Prostate-Specific Antigen Bounce after 125I Brachytherapy Using Stranded Seeds with Intraoperative Optimization for Prostate Cancer" Cancers 14, no. 19: 4907. https://doi.org/10.3390/cancers14194907