
The Association between Peptic Ulcer Disease and Gastric Cancer: Results from the Stomach Cancer Pooling (StoP) Project Consortium
 , , , , , , , , , ,
, , , , , , , , , ,  , , , , ,
, , , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Statistical Analysis and Covariates
2.3. Sensitivity Analysis
3. Results
Sensitivity Analysis
4. Discussion
5. Conclusion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jung, K.-W.; Park, S.; Kong, H.-J.; Won, Y.-J.; Lee, J.Y.; Park, E.-C.; Lee, J.-S. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2008. Cancer Res. Treat. 2011, 43, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Peek, R.M.; Blaser, M.J. Helicobacter pylori and gastrointestinal tract adenocarcinomas. Nat. Rev. Cancer 2002, 2, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Asaka, M. Eradication of gastric cancer and more efficient gastric cancer surveillance in Japan: Two peas in a pod. J. Gastroenterol. 2010, 45, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Berger, H.; Marques, M.; Zietlow, R.; Meyer, T.F.; Machado, J.C.; Figueiredo, C. Gastric cancer pathogenesis. Helicobacter 2016, 21, 34–38. [Google Scholar] [CrossRef]
- Bauer, B.; Meyer, T.F. The human gastric pathogen Helicobacter pylori and its association with gastric cancer and ulcer disease. Ulcers 2011, 2011, 340157. [Google Scholar] [CrossRef] [Green Version]
- Hansson, L.-E.; Nyrén, O.; Hsing, A.W.; Bergström, R.; Josefsson, S.; Chow, W.-H.; Fraumeni, J.F.; Adami, H.-O. The Risk of Stomach Cancer in Patients with Gastric or Duodenal Ulcer Disease. N. Engl. J. Med. 1996, 335, 242–249. [Google Scholar] [CrossRef]
- Uemura, N.; Okamoto, S.; Yamamoto, S.; Matsumura, N.; Yamaguchi, S.; Yamakido, M.; Taniyama, K.; Sasaki, N.; Schlemper, R.J. Helicobacter pylori infection and the Development of Gastric Cancer. N. Engl. J. Med. 2001, 345, 784–789. [Google Scholar] [CrossRef]
- Take, S.; Mizuno, M.; Ishiki, K.; Nagahara, Y.; Yoshida, T.; Yokota, K.; Oguma, K.; Okada, H.; Shiratori, Y. The Effect of Eradicating Helicobacter Pylori on the Development of Gastric Cancer in Patients with Peptic Ulcer Disease. Am. J. Gastroenterol. 2005, 100, 1037–1042. [Google Scholar] [CrossRef]
- Molloy, R.M.; Sonnenberg, A. Relation between gastric cancer and previous peptic ulcer disease. Gut 1997, 40, 247–252. [Google Scholar] [CrossRef]
- Pelucchi, C.; Lunet, N.; Boccia, S.; Zhang, Z.F.; Praud, D.; Boffetta, P.; Negri, E.; Malekzadeh, R.; Zaridze, D.; Ye, W.; et al. The stomach cancer pooling (StoP) project: Study design and presentation. Eur. J. Cancer Prev. 2015, 24, 16–23. [Google Scholar] [CrossRef] [PubMed]
- La Vecchia, C.; Pelucchi, C.; Negri, E.; Bonzi, R.; Boffetta, P.; Camargo, M.C.; Curado, P.M.; Lunet, N.; Vioque, J.; Zhang, Z.F. The stomach cancer pooling (STOP) project: A global consortium of epidemiological studies of gastric cancer, updated to 2021. Eur. J. Cancer Prev. 2021, 31, S4–S5. [Google Scholar] [CrossRef]
- Buiatti, E.; Palli, D.; Decarli, A.; Amadori, D.; Avellini, C.; Bianchi, S.; Biserni, R.; Cipriani, F.; Cocco, P.; Giacosa, A.; et al. A case-control study of gastric cancer and diet in Italy. Int. J. Cancer 1989, 44, 611–616. [Google Scholar] [CrossRef] [PubMed]
- Vecchia, C.L.; D'Avanzo, B.; Negri, E.; Decarli, A.; Benichou, J. Attributable risks for stomach cancer in northern Italy. Int. J. Cancer 1995, 60, 748–752. [Google Scholar] [CrossRef]
- De Feo, E.; Simone, B.; Persiani, R.; Cananzi, F.; Biondi, A.; Arzani, D.; Amore, R.; D’Ugo, D.; Ricciardi, G.; Boccia, S. A case-control study on the effect of Apolipoprotein E genotypes on gastric cancer risk and progression. BMC Cancer 2012, 12, 494. [Google Scholar] [CrossRef] [Green Version]
- Zaridze, D.; Borisova, E.; Maximovitch, D.; Chkhikvadze, V. Alcohol consumption, smoking and risk of gastric cancer: Case-control study from Moscow, Russia. Cancer Causes Control. 2000, 11, 363–371. [Google Scholar] [CrossRef]
- Lagiou, P.; Samoli, E.; Lagiou, A.; Peterson, J.; Tzonou, A.; Dwyer, J.; Trichopoulos, D. Flavonoids, vitamin C and adenocarcinoma of the stomach. Cancer Causes Control. 2004, 15, 67–72. [Google Scholar] [CrossRef]
- Setiawan, V.W.; Yu, G.-P.; Lu, Q.-Y.; Lu, M.-L.; Yu, S.-Z.; Mu, L.; Zhang, J.-G.; Kurtz, R.C.; Cai, L.; Hsieh, C.-C.; et al. Allium vegetables and stomach cancer risk in China. Asian Pac. J. Cancer Prev. 2005, 6, 387–395. [Google Scholar]
- Deandrea, S.; Foschi, R.; Galeone, C.; La Vecchia, C.; Negri, E.; Hu, J. Is temperature an effect modifier of the association between green tea intake and gastric cancer risk? Eur. J. Cancer Prev. 2010, 19, 18–22. [Google Scholar] [CrossRef]
- Setiawan, V.W.; Zhang, Z.-F.; Yu, G.-P.; Lu, Q.-Y.; Li, Y.-L.; Lu, M.-L.; Wang, M.-R.; Guo, C.H.; Yu, S.-Z.; Kurtz, R.C.; et al. GSTP1 polymorphisms and gastric cancer in a high-risk Chinese population. Cancer Causes Control. 2001, 12, 673–681. [Google Scholar] [CrossRef]
- Mu, L.-N.; Lu, Q.-Y.; Yu, S.-Z.; Jiang, Q.-W.; Cao, W.; You, N.-C.; Setiawan, V.; Zhou, X.-F.; Ding, B.-G.; Wang, R.-H.; et al. Green tea drinking and multigenetic index on the risk of stomach cancer in a Chinese population. Int. J. Cancer 2005, 116, 972–983. [Google Scholar] [CrossRef] [PubMed]
- Machida-Montani, A.; Sasazuki, S.; Inoue, M.; Natsukawa, S.; Shaura, K.; Koizumi, Y.; Kasuga, Y.; Hanaoka, T.; Tsugane, S. Association of Helicobacter pylori infection and environmental factors in non-cardia gastric cancer in Japan. Gastric Cancer 2004, 7, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-Y. Some recent works on diagnosis and treatment of gastric cancer. World J. Gastroenterol. 1999, 5, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Firth, D. Bias reduction of maximum likelihood estimates. Biometrika 1993, 80, 27–38. [Google Scholar] [CrossRef]
- Liu, Y.; De, A. Multiple Imputation by Fully Conditional Specification for Dealing with Missing Data in a Large Epidemiologic Study. Int. J. Stat. Med Res. 2015, 4, 287–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 2004. [Google Scholar]
- Der Simonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- La Vecchia, C.; Braga, C.; Negri, E.; Franceschi, S. Risk of stomach cancer in patients with gastric or duodenal ulcer. Eur. J. Cancer Prev. 1997, 6, 20–23. [Google Scholar] [CrossRef]
- Tuan, V.P.; Yahara, K.; Dung, H.D.Q.; Binh, T.T.; Tung, P.H.; Tri, T.D.; Thuan, N.P.M.; van Khien, V.; Trang, T.T.H.; Phuc, B.H.; et al. Genome-wide association study of gastric cancer- and duodenal ulcer-derived Helicobacter pylori strains reveals discriminatory genetic variations and novel oncoprotein candidates. Microb. Genom. 2021, 7, 000680. [Google Scholar] [CrossRef]
- Moss, S.; Rodríguez, L.A.G.; Lagergren, J.; Lindblad, M. Gastric acid suppression and risk of oesophageal and gastric adenocarcinoma: A nested case control study in the UK. Gut 2006, 55, 1538–1544. [Google Scholar] [CrossRef]
- Basurto, O.X.; Rigau, C.D.; Urrutia, G. Opioids for acute pancreatitis pain. Cochrane Database Syst. Rev. 2013, CD009179. [Google Scholar] [CrossRef]
- Hosokawa, O.; Hattori, M.; Douden, K.; Hayashi, H.; Ohta, K.; Kaizaki, Y. Difference in accuracy between gastroscopy and colonoscopy for detection of cancer. Hepatogastroenterology 2007, 54, 442–444. [Google Scholar] [PubMed]
- Ikenoyama, Y.; Hirasawa, T.; Ishioka, M.; Namikawa, K.; Yoshimizu, S.; Horiuchi, Y.; Ishiyama, A.; Yoshio, T.; Tsuchida, T.; Takeuchi, Y.; et al. Detecting early gastric cancer: Comparison between the diagnostic ability of convolutional neural networks and endoscopists. Dig. Endosc. 2021, 33, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Feili, O.; Bakhti, S.Z.; Latifi-Navid, S.; Zahri, S.; Yazdanbod, A. Contrasting association of Helicobacter pylori oipA genotype with risk of peptic ulceration and gastric cancer. Infect. Genet. Evol. 2021, 89, 104720. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, N. Is Helicobacter pylori a cause of gastric cancer? An appraisal of the seroepidemiological evidence. Cancer Epidemiol. Prev. Biomark. 1994, 3, 445–451. [Google Scholar]
- Gupta, S.; Tao, L.; Murphy, J.D.; Camargo, M.C.; Oren, E.; Valasek, M.A.; Gomez, S.L.; Martinez, M.E. Race/Ethnicity-, Socioeconomic Status-, and Anatomic Subsite-Specific Risks for Gastric Cancer. Gastroenterology 2019, 156, 59–62e4. [Google Scholar] [CrossRef]
- Collatuzzo, G.; Alicandro, G.; Bertuccio, P.; Pelucchi, C.; Bonzi, R.; Palli, D.; Ferraroni, M.; Ye, W.; Plymoth, A.; Zaridze, D.; et al. Peptic ulcer as mediator of the association between risk of gastric cancer and socioeconomic status, tobacco smoking, alcohol drinking and salt intake. J. Epidemiol. Commun. Health 2022, 76, 861–866. [Google Scholar] [CrossRef]
- Merchant, S.J.; Li, L.; Kim, J. Racial and ethnic disparities in gastric cancer outcomes: More important than surgical technique? World J. Gastroenterol. 2014, 20, 11546–11551. [Google Scholar] [CrossRef]
- Fock, K.M.; Ang, T.L. Epidemiology of Helicobacter pylori infection and gastric cancer in Asia. J. Gastroenterol. Hepatol. 2010, 25, 479–486. [Google Scholar] [CrossRef]
- Theuer, C.P.; Al-Kuran, R.; Akiyama, Y.; Okumura, M.; Ziogas, A.; Carpenter, P.M. Increased epithelial cadherin expression among Japanese intestinal-type gastric cancers compared with specimens from American patients of European descent. Am. Surg. 2006, 72, 332–338. [Google Scholar] [CrossRef]
- Theuer, C.P.; Campbell, B.S.; Peel, D.J.; Lin, F.; Carpenter, P.; Ziogas, A.; Butler, J.A. Microsatellite Instability in Japanese vs European American Patients With Gastric Cancer. Arch. Surg. 2002, 137, 960–966. [Google Scholar] [CrossRef]
- Park, B.; Shin, A.; Park, S.K.; Ko, K.-P.; Ma, S.H.; Lee, E.-H.; Gwack, J.; Jung, E.-J.; Cho, L.Y.; Yang, J.J.; et al. Ecological study for refrigerator use, salt, vegetable, and fruit intakes, and gastric cancer. Cancer Causes Control 2011, 22, 1497–1502. [Google Scholar] [CrossRef]
- Lam, S.K. Pathogenesis and pathophysiology of duodenal ulcer. Clin. Gastroenterol. 1984, 13, 447–472. [Google Scholar] [CrossRef]
- World Cancer Research Fund; American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; American Institute for Cancer Research: Washington, DC, USA, 2007. [Google Scholar]



{kind=link}
{kind=link}
| Gastric Cancer Cases (n = 4106) | Controls (n = 6922) | p-Value | |
|---|---|---|---|
| Age (Mean ± SD) | 61.5 (10.7) | 57.0 (12.4) | <0.0001 |
| Age categories (years) | <0.0001 | ||
| ≤55 | 1080 (26.3) | 2881 (41.6) | |
| 55–65 | 1206 (29.4) | 1872 (27.0) | |
| ≥65 | 1820 (44.3) | 2169 (31.3) | |
| Sex | 0.003 | ||
| Male | 2590 (63.1) | 4171 (60.3) | |
| Female | 1516 (37.0) | 2751 (39.7) | |
| Race/ethnicity | 0.59 | ||
| White | 545 (13.3) | 683 (9.8) | |
| Black/African American | 4 (0.1) | 8 (0.1) | |
| Asian | 8 (0.2) | 5 (0.1) | |
| Hispanic/Latino | 6 (0.2) | 7 (0.1) | |
| Other | 0 (0.0) | 1 (0.01) | |
| Missing | 3543 (86.3) | 6218 (89.8) | |
| Education (completed) | <0.0001 | ||
| Less than high school | 1946 (47.4) | 2147 (31.0) | |
| High school | 812 (19.8) | 1436 (20.8) | |
| College graduate | 178 (4.3) | 348 (5.0) | |
| Missing | 1170 (28.5) | 2991 (43.2) | |
| Socioeconomic status | <0.0001 | ||
| Low | 2418 (58.9) | 3227 (46.6) | |
| Intermediate | 1244 (30.3) | 2360 (34.1) | |
| High | 337 (8.2) | 1004 (14.5) | |
| Missing | 107 (2.6) | 331 (4.8) | |
| Smoking | <0.0001 | ||
| Never | 1801 (43.9) | 3345 (48.3) | |
| Former | 871 (21.2) | 1261 (18.2) | |
| Current, Low * | 345 (8.4) | 688 (10.0) | |
| Current, Intermediate/High * | 1030 (25.1) | 1575 (22.8) | |
| Missing | 59 (1.4) | 53 (0.8) | |
| Alcohol Drinking | |||
| Never | 769 (18.7) | 1659 (24.0) | <0.0001 |
| Low ** | 464 (11.3) | 877 (12.7) | |
| Moderate/High ** | 1822 (44.4) | 2817 (40.7) | |
| Missing | 1051 (25.6) | 1569 (22.7) | |
| Body Mass Index (Kg/m2) | |||
| <18.5 | 239 (5.8) | 191 (2.8) | <0.0001 |
| 18.5–23 | 1249 (30.4) | 1917 (27.7) | |
| 23–25 | 689 (16.8) | 1272 (18.4) | |
| 25–27.5 | 543 (13.2) | 1137 (16.4) | |
| 27.5–30 | 330 (8.0) | 651 (9.4) | |
| >30 | 877 (21.4) | 1148 (16.6) | |
| Missing | 179 (4.4) | 606 (8.8) | |
| Vegetables/fruits intake | <0.001 | ||
| Low | 1268 (30.9) | 1845 (26.7) | |
| Intermediate | 1319 (32.1) | 2186 (31.6) | |
| High | 1363 (33.2) | 2379 (34.4) | |
| Missing | 156 (3.8) | 512 (7.4) | |
| History of diabetes | 0.30 | ||
| No | 3180 (77.5) | 5115 (73.9) | |
| Yes | 210 (5.1) | 307 (4.4) | |
| Missing | 716 (17.4) | 1500 (21.7) | |
| History of peptic ulcer | <0.0001 | ||
| No | 2,735 (66.6) | 5122 (74.0) | |
| Yes | 545 (13.3) | 475 (6.9) | |
| Missing | 826 (20.1) | 1325 (19.1) | |
| History of GU | |||
| No | 3381 (82.3) | 6386 (92.3) | <0.0001 |
| Yes | 487 (11.9) | 276 (4.0) | |
| Missing | 238 (5.8) | 260 (3.8) | |
| History of DU | 0.0003 | ||
| No | 3128 (76.2) | 5377 (77.7) | |
| Yes | 253 (6.2) | 318 (4.6) | |
| Missing | 725 (17.7) | 1227 (17.7) | |
| H. pylori serostatus | <0.0001 | ||
| Negative | 393 (9.6) | 612 (8.8) | |
| Positive | 470 (11.5) | 494 (7.1) | |
| Missing | 3243 (79.0) | 5816 (84.0) |
| Gastric Cancer | |||||
|---|---|---|---|---|---|
| Cases | Controls | ||||
| Gastric Ulcer (Yes) | Gastric Ulcer (Yes) | OR (95% CI) | Pbetween-study | Pinteraction | |
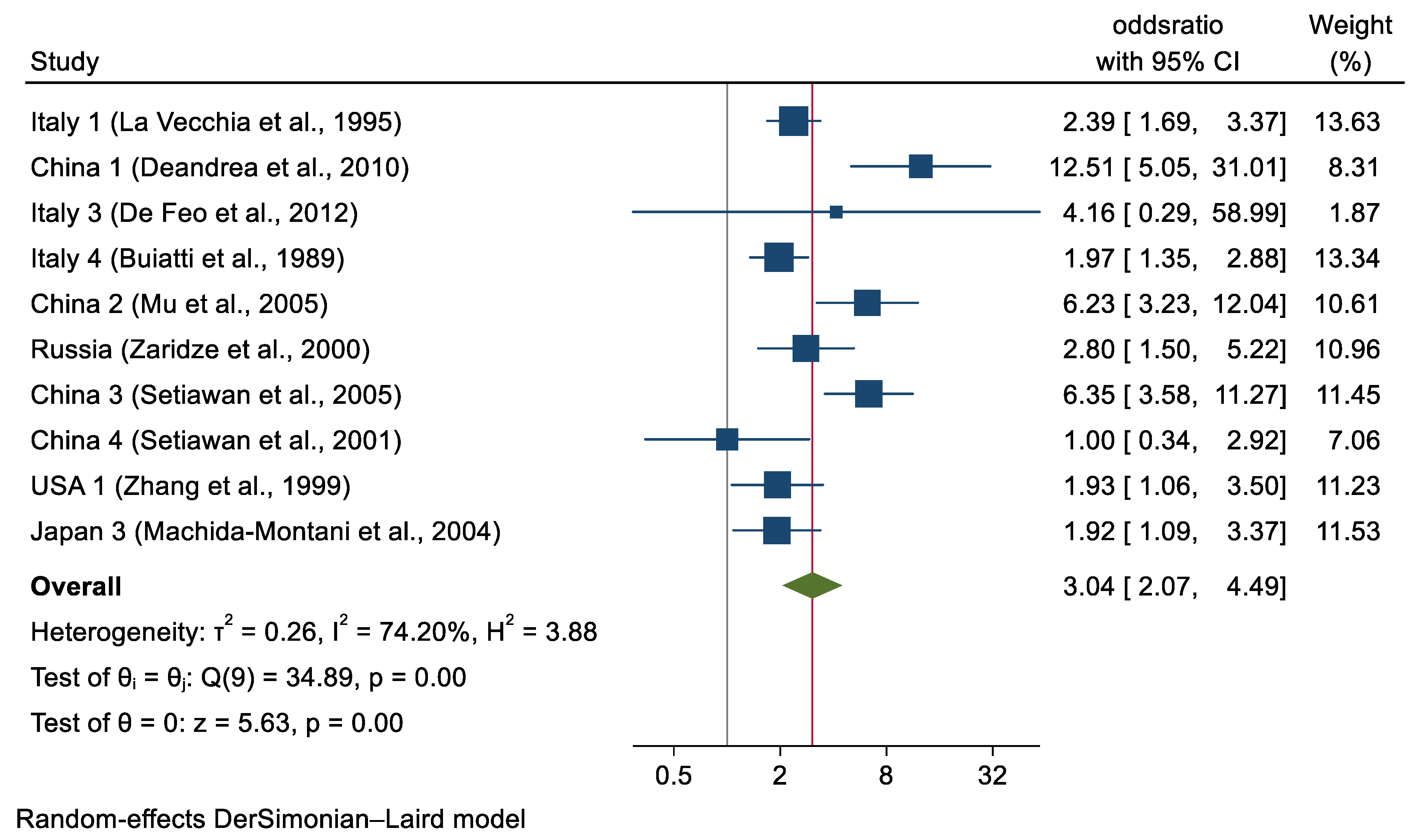
| Overall a | 487 | 276 | 3.04 (2.07–4.49) | 0.00 | N/A |
| Sex b | 0.37 | ||||
| Men | 136 (27.9) | 72 (27.6) | 2.72 (1.82–4.07) | 0.00 | |
| Women | 346 (72.1) | 189 (72.4) | 3.39 (1.98–5.63) | 0.11 | |
| Age (years) c | 0.15 | ||||
| ≤55 | 137 (30.6) | 84 (35.6) | 4.22 (2.64–6.74) | 0.08 | |
| >55–<65 | 131 (29.2) | 74 (31.3) | 2.36 (1.66–3.35) | 0.38 | |
| ≥65 | 180 (40.2) | 78 (33.1) | 2.89 (2.28–4.12) | 0.00 | |
| Education completed d | 0.97 | ||||
| Less than high school | 139 (58.6) | 51 (63.7) | 3.53 (1.36–7.34) | 0.03 | |
| High school | 76 (32.1) | 23 (28.7) | 3.64 (1.89–7.00) | 0.24 | |
| Graduate | 22 (9.3) | 6 (7.6) | 3.16 (1.30–9.59) | 0.74 | |
| Socioeconomic status e | 0.34 | ||||
| Low/Intermediate | 418 (87.4) | 219 (79.9) | 3.12 (2.03–4.78) | 0.01 | |
| High | 60 (12.6) | 55 (20.1) | 2.24 (1.32–3.79) | 0.96 | |
| BMI (Kg/m2) | 0.96 | ||||
| <25 | 291 (60.7) | 165 (62.0) | 2.99 (1.99–4.49) | 0.01 | |
| ≥25 | 188 (39.3) | 101 (38.0) | 3.04 (1.99–4.67) | 0.12 | |
| Smoking status f | 0.14 | ||||
| Never | 150 (34.1) | 79 (35.7) | 2.17 (2.07–3.46) | 0.01 | |
| Former | 118 (26.8) | 56 (25.4) | 2.02 (1.41–2.90) | 0.58 | |
| Current | 172 (39.1) | 86 (38.9) | 2.83 (2.29–4.21) | 0.28 | |
| Alcohol consumption g | 0.08 | ||||
| Never | 72 (24.7) | 51 (24.0) | 4.53 (2.56–8.00) | 0.05 | |
| Low | 65 (22.3) | 43 (20.3) | 2.71 (1.76–4.18) | 0.56 | |
| Moderate/high | 154 (53.0) | 118 (53.4) | 2.07 (1.43–2.99) | 0.14 | |
| Fruit/vegetable intake h | 0.61 | ||||
| Low | 129 (29.2) | 67 (30.3) | 3.36 (2.03–5.57) | 0.05 | |
| Intermediate | 160 (36.2) | 72 (32.6) | 2.93 (1.97–4.37) | 0.17 | |
| High | 153 (34.6) | 82 (37.1) | 2.50 (1.78–3.52) | 0.67 | |
| H. pylori serostatus i | 0.19 | ||||
| Positive | 65 (52.0) | 35 (55.6) | 2.61 (1.38–4.95) | 0.50 | |
| Negative | 60 (48.0) | 28 (44.4) | 4.58 (2.63–8.00) | 0.24 | |
| History of diabetes j | 0.98 | ||||
| Yes | 12 (4.6) | 12 (6.4) | 2.88 (1.29–6.29) | 0.42 | |
| No | 246 (95.4) | 174 (93.6) | 2.85 (1.94–4.28) | 0.02 | |
| Cancer subsite k | 0.05 | ||||
| Cardia | 36 (16.6) | 172 (50.0) | 1.43 (0.85–2.40) | 0.43 | |
| Non-cardia | 181 (83.4) | 172 (50.0) | 2.50 (1.94–3.23) | 0.76 | |
| Histological type l | 0.87 | ||||
| Intestinal | 90 (47.9) | 10 (33.3) | 2.39 (1.53–3.73) | 0.25 | |
| Diffuse | 40 (21.3) | 104 (33.3) | 2.04 (1.34–3.11) | 0.88 | |
| Other/unspecified | 58 (30.8) | 104 (33.3) | 2.12 (1.45–3.09) | 0.64 | |
| Geographic region | 0.30 | ||||
| Europe | 207 (42.5) | 90 (32.6) | 2.28 (1.80–2.88) | 0.74 | |
| Asia | 225 (46.2) | 150 (54.3) | 4.05 (1.87–8.74) | 0.00 | |
| Americas (USA only) | 55 (11.3) | 36 (13.0) | 1.93 (1.06–3.50) | N/A | |
| Source of study Controls | 0.84 | ||||
| Hospital | 253 (51.9) | 180 (65.2) | 2.86 (1.82–4.50) | 0.02 | |
| Population | 234 (48.1) | 96 (34.8) | 3.15 (1.43–6.94) | 0.00 | |
| Gastric Cancer | |||||
|---|---|---|---|---|---|
| Cases | Controls | ||||
| Duodenal Ulcer (Yes) | Duodenal Ulcer (Yes) | OR (95% CI) | Pbetween-study | Pinteraction | |
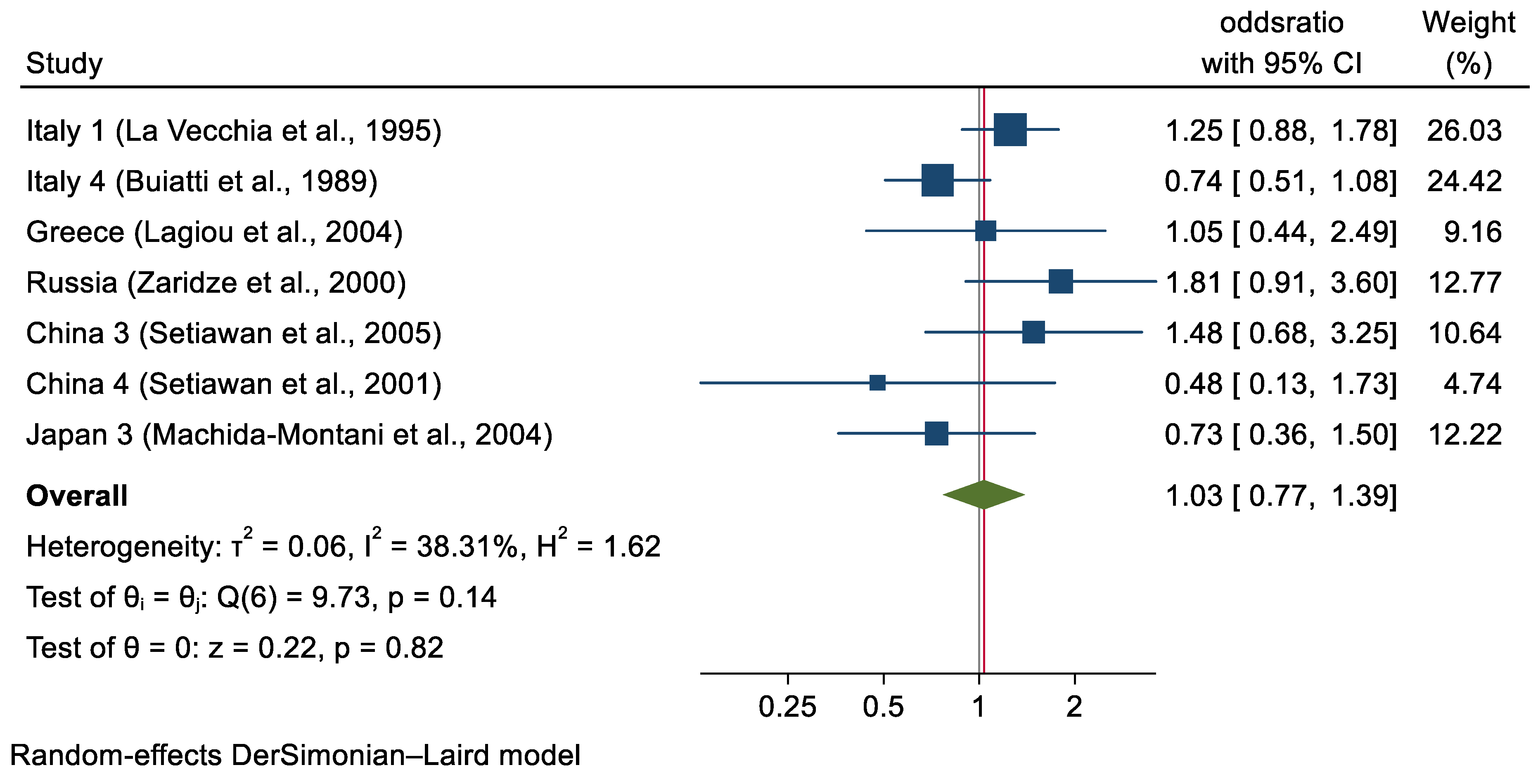
| Overall a | 252 | 318 | 1.03 (0.77–1.39) | 0.82 | N/A |
| Sex | 0.10 | ||||
| Men | 186 (73.8) | 237 (74.5) | 0.91 (0.70–1.18) | 0.37 | |
| Women | 66 (26.2) | 81 (25.5) | 1.43 (0.88–2.31) | 0.26 | |
| Age (years) | 0.20 | ||||
| ≤55 | 80 (31.7) | 119 (37.4) | 1.45 (0.96–2.21) | 0.38 | |
| >55–<65 | 74 (29.4) | 89 (28.0) | 1.05 (0.72–1.52) | 0.87 | |
| ≥65 | 98 (38.9) | 110 (34.6) | 0.88 (0.62–1.25) | 0.41 | |
| Education completed b | 0.31 | ||||
| Less than high school | 97 (61.0) | 96 (58.5) | 1.98 (0.71–5.51) | 0.36 | |
| High school | 48 (30.2) | 57 (34.8) | 1.07 (0.63–1.81) | 0.64 | |
| Graduate | 14 (8.8) | 11 (6.7) | 0.85 (0.56–1.29) | 0.36 | |
| SES c | 0.22 | ||||
| Low | 136 (58.4) | 173 (57.3) | 0.94 (0.72–1.23) | 0.56 | |
| Intermediate | 77 (33.0) | 98 (32.4) | 1.16 (0.71–1.87) | 0.23 | |
| High | 20 (8.6) | 31 (10.3) | 1.77 (0.89–3.51) | 0.89 | |
| Socioeconomic status c | 0.25 | ||||
| Low/intermediate | 213 (91.4) | 271 (89.7) | 1.70 (0.86–3.38) | 0.11 | |
| High | 20 (8.6) | 31 (10.3) | 1.08 (0.78–1.52) | 0.82 | |
| BMI (kg/m2) d | 0.95 | ||||
| <25 | 141 (67.8) | 183 (63.8) | 0.99 (0.60–1.66) | 0.02 | |
| ≥25 | 67 (32.2) | 104 (36.2) | 1.01 (0.70–1.47) | 0.93 | |
| Smoking status e | 0.52 | ||||
| Never | 64 (27.9) | 84 (30.3) | 1.08 (0.89–1.84) | 0.49 | |
| Former | 74 (32.3) | 67 (24.2) | 1.18 (0.76–1.81) | 0.82 | |
| Current | 91 (39.8) | 126 (45.5) | 1.14 (0.63–1.40) | 0.62 | |
| Alcohol consumption f | 0.51 | ||||
| Never | 33 (20.8) | 50 (20.7) | 1.02 (0.65–1.61) | 0.24 | |
| Low | 19 (11.9) | 25 (10.4) | 0.85 (0.59–1.23) | 0.26 | |
| Moderate/high | 107 (67.3) | 166 (68.9) | 1.41 (0.62–3.20) | 0.31 | |
| Fruit/vegetable intake g | 0.03 | ||||
| Low | 81 (41.8) | 74 (30.3) | 1.61 (0.87–2.97) | 0.11 | |
| Intermediate | 42 (21.7) | 93 (38.1) | 1.19 (0.75–1.88) | 0.33 | |
| High | 71 (36.5) | 77 (31.5) | 0.64 (0.41–0.99) | 0.39 | |
| H. pylori serostatus h | 0.86 | ||||
| Positive | 34 (75.6) | 29 (69.0) | 1.15 (0.48–2.74) | 0.13 | |
| Negative | 11 (24.4) | 13 (31.0) | 1.29 (0.46–3.63) | 0.65 | |
| History of diabetes i | 0.89 | ||||
| Yes | 11 (4.6) | 15 (5.2) | 1.03 (0.42–2.57) | 0.77 | |
| No | 227 (95.4) | 27 (94.8) | 1.11 (0.80–1.53) | 0.11 | |
| Cancer subsite j | 0.10 | ||||
| Cardia | 20 (10.5) | 258 (50.0) | 1.89 (1.03–3.47) | 0.84 | |
| Non-cardia | 171 (89.5) | 258 (50.0) | 0.10 (0.63–1.57) | 0.03 | |
| Histological type k | 0.83 | ||||
| Intestinal | 57 (48.7) | 120 (33.3) | 0.84 (0.55–1.29) | 0.00 | |
| Diffuse | 20 (17.1) | 120 (33.3) | 0.88 (0.28–2.71) | 0.45 | |
| Other/unspecified | 40 (34.2) | 120 (33.3) | 1.27 (0.36-4.48) | 0.70 | |
| Region | 0.56 | ||||
| Europe | 58 (23.0) | 74 (23.3) | 1.10 (0.75–1.61) | 0.09 | |
| Asia | 194 (77.0) | 244 (76.7) | 0.89 (0.49–1.62) | 0.25 | |
| Source of study Controls | 0.26 | ||||
| Hospital | 125 (49.6) | 170 (53.4) | 1.20 (0.89–1.62) | 0.34 | |
| Population | 127 (50.4) | 148 (46.6) | 0.85 (0.51–1.43) | 0.21 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paragomi, P.; Dabo, B.; Pelucchi, C.; Bonzi, R.; Bako, A.T.; Sanusi, N.M.; Nguyen, Q.H.; Zhang, Z.-F.; Palli, D.; Ferraroni, M.; et al. The Association between Peptic Ulcer Disease and Gastric Cancer: Results from the Stomach Cancer Pooling (StoP) Project Consortium. Cancers 2022, 14, 4905. https://doi.org/10.3390/cancers14194905
Paragomi P, Dabo B, Pelucchi C, Bonzi R, Bako AT, Sanusi NM, Nguyen QH, Zhang Z-F, Palli D, Ferraroni M, et al. The Association between Peptic Ulcer Disease and Gastric Cancer: Results from the Stomach Cancer Pooling (StoP) Project Consortium. Cancers. 2022; 14(19):4905. https://doi.org/10.3390/cancers14194905
Chicago/Turabian StyleParagomi, Pedram, Bashir Dabo, Claudio Pelucchi, Rossella Bonzi, Abdulaziz T. Bako, Nabila Muhammad Sanusi, Quan H. Nguyen, Zuo-Feng Zhang, Domenico Palli, Monica Ferraroni, and et al. 2022. "The Association between Peptic Ulcer Disease and Gastric Cancer: Results from the Stomach Cancer Pooling (StoP) Project Consortium" Cancers 14, no. 19: 4905. https://doi.org/10.3390/cancers14194905