
FLT3-ITD Expression as a Potential Biomarker for the Assessment of Treatment Response in Patients with Acute Myeloid Leukemia

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
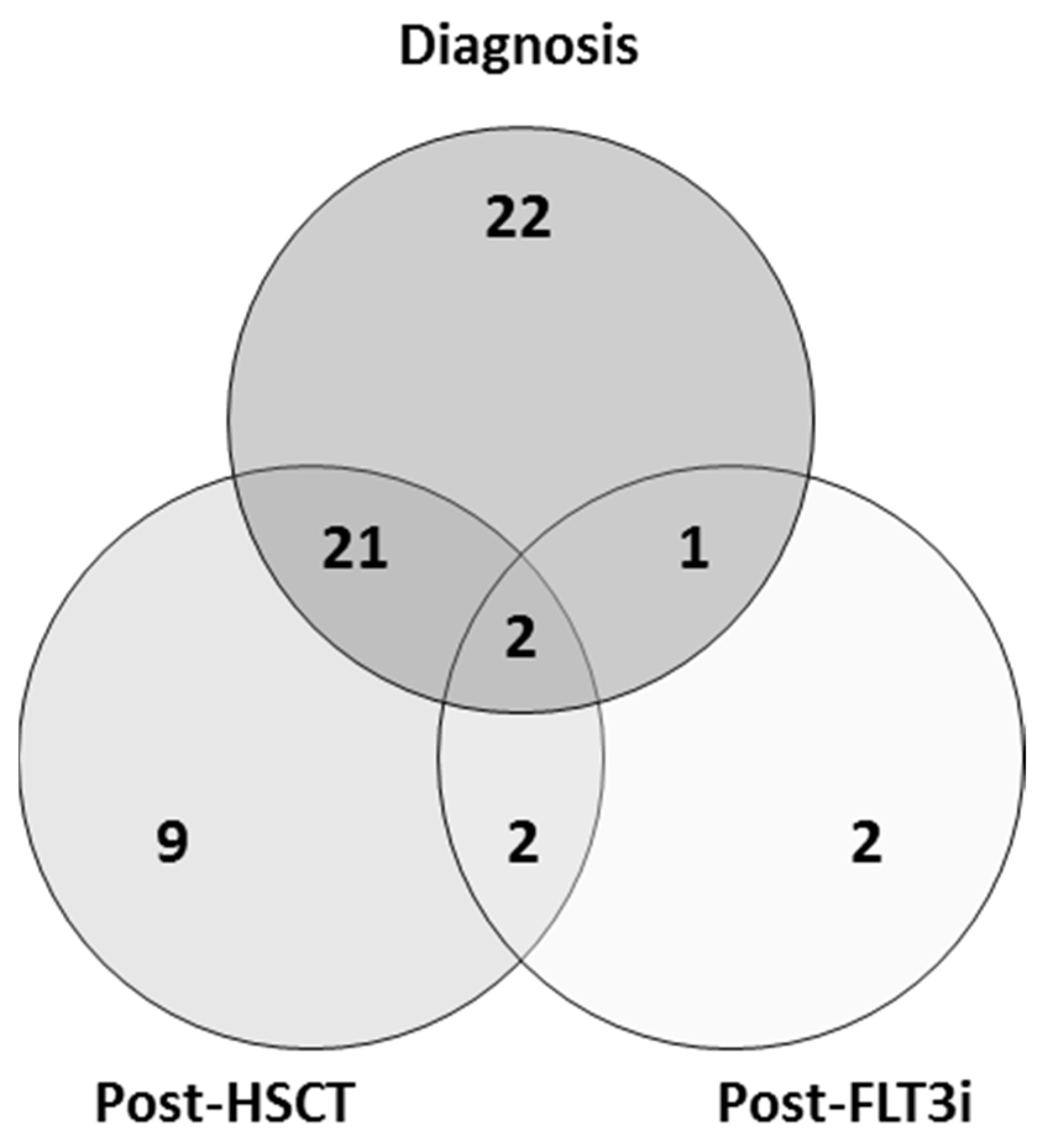
2.1. Patient Samples
2.2. Sample Processing
2.3. FLT3-ITD Mutation Analysis and Quantification
2.4. Measurable Residual Disease and Chimerism Analysis
2.5. Statistical Analysis
3. Results
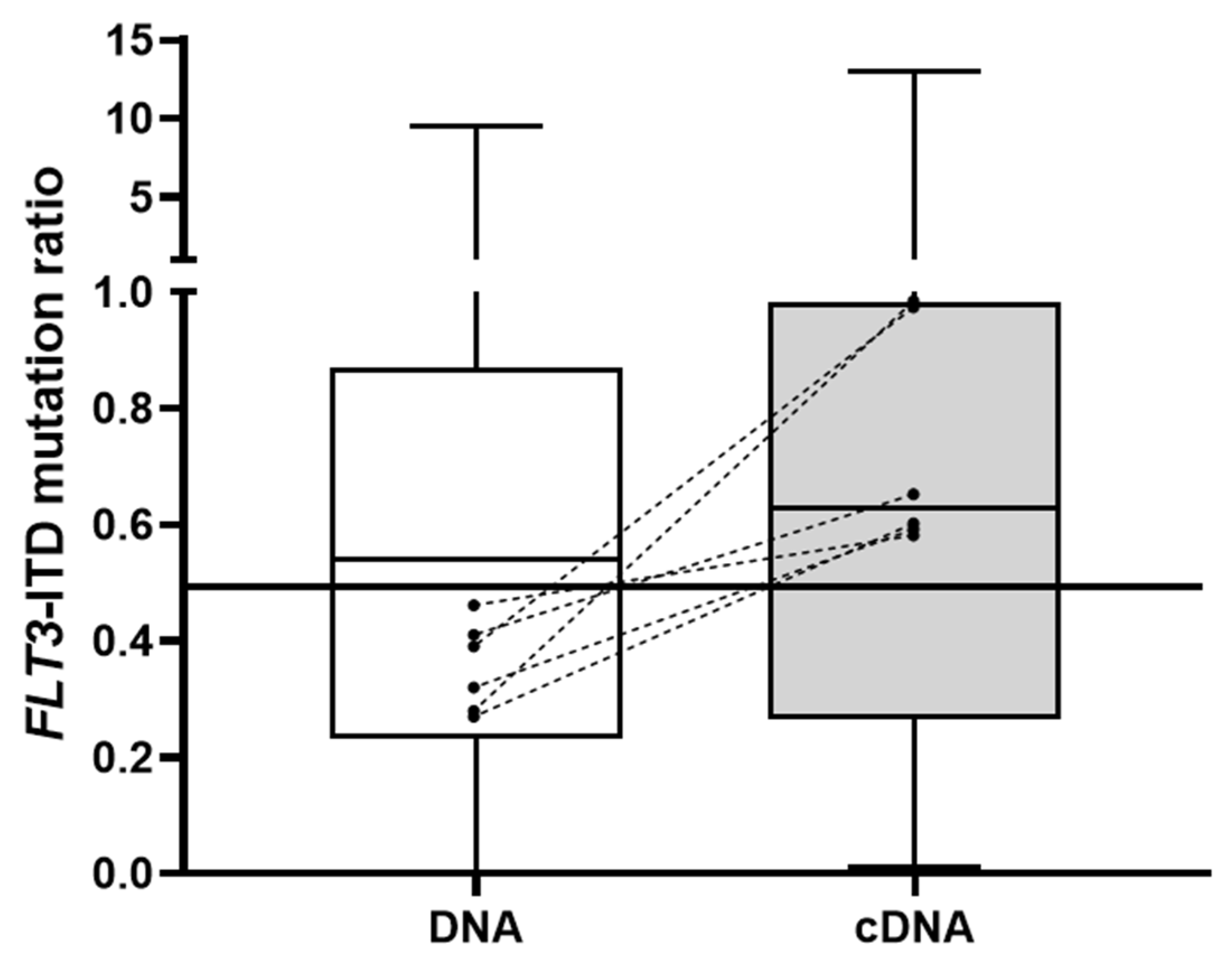
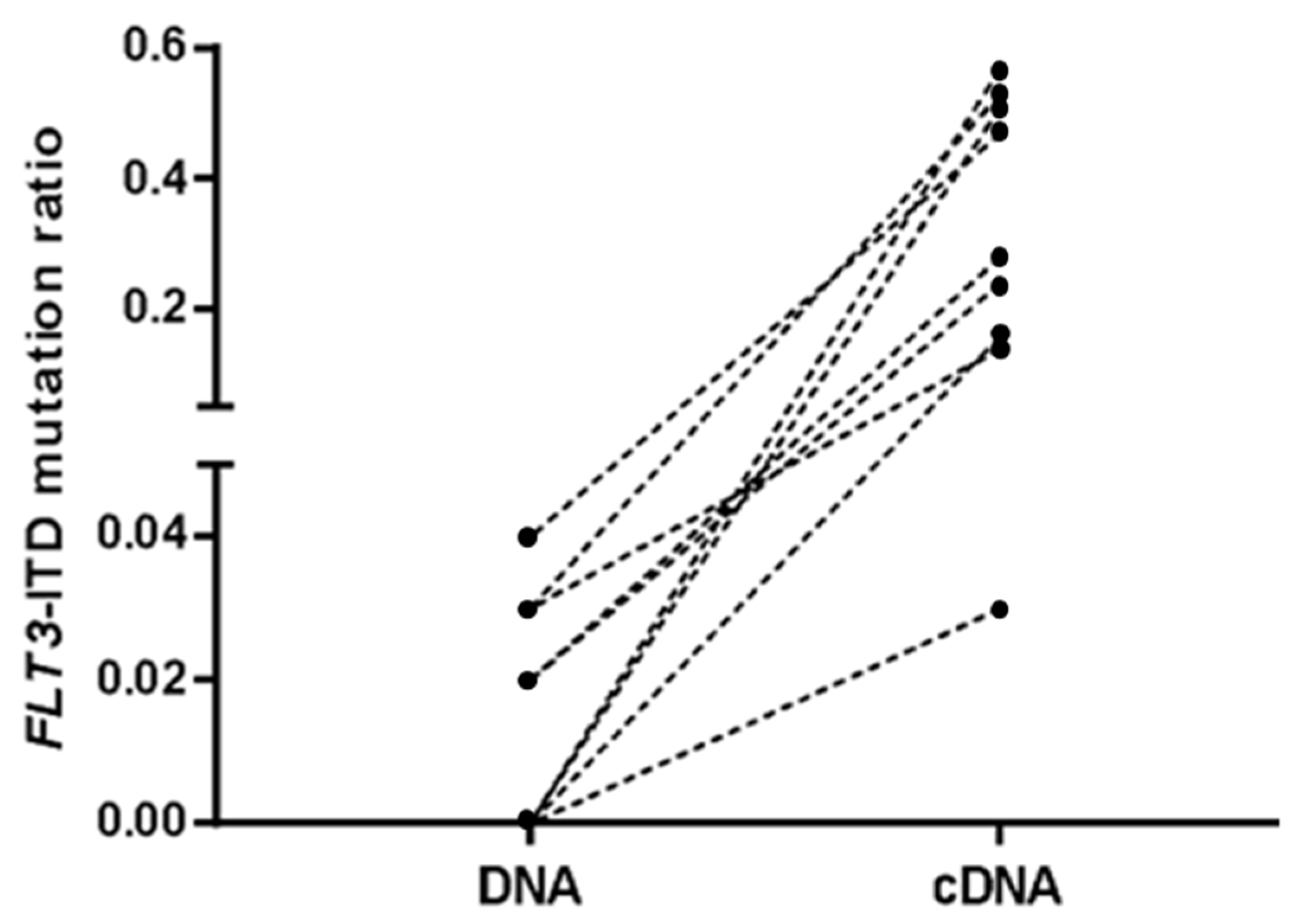
3.1. FLT3-ITD Mutation in DNA and cDNA in Diagnostic Samples (Allelic Ratio)
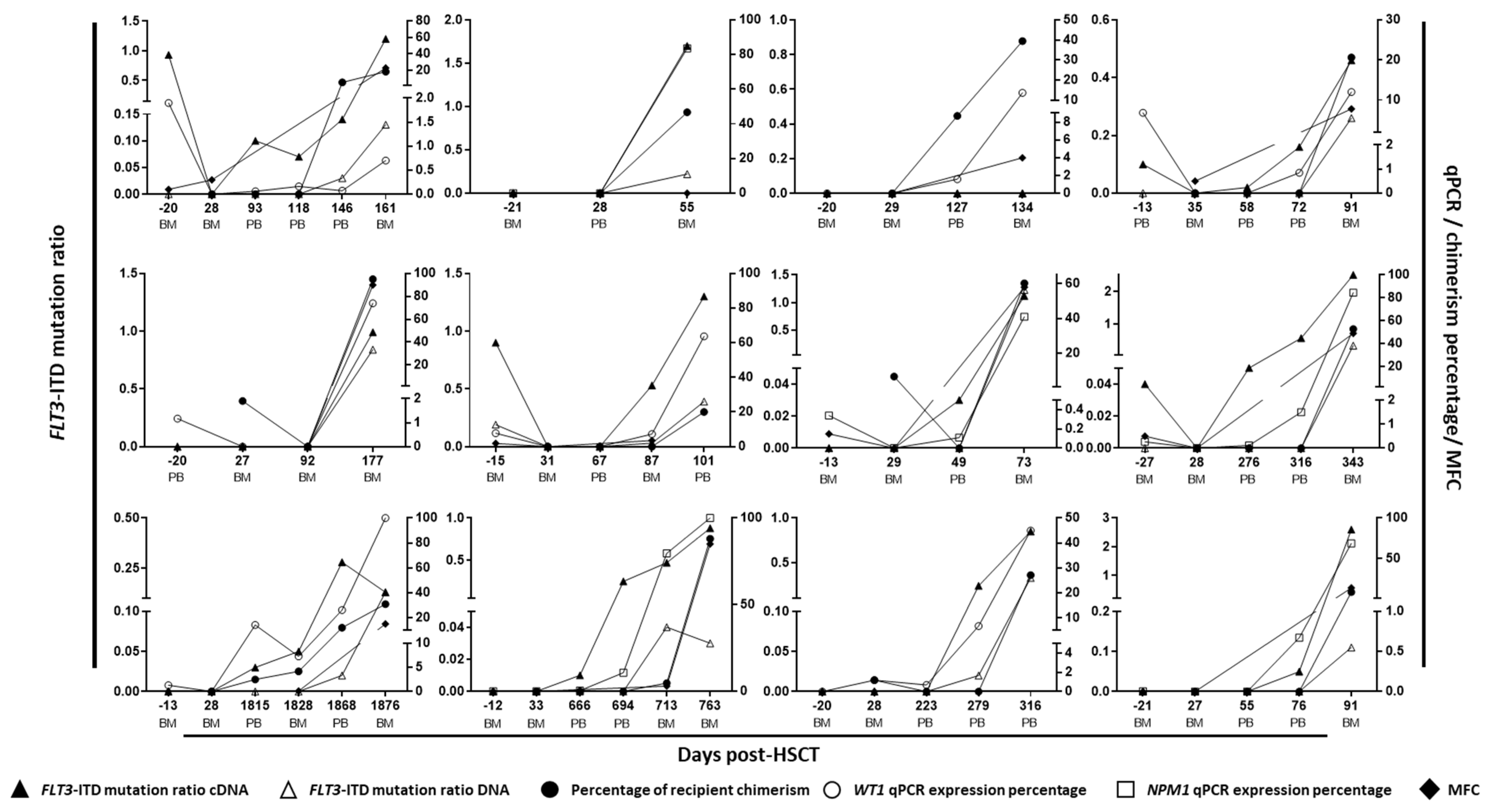
3.2. FLT3-ITD Mutations in DNA and cDNA for Post-Allo-HSCT Monitoring
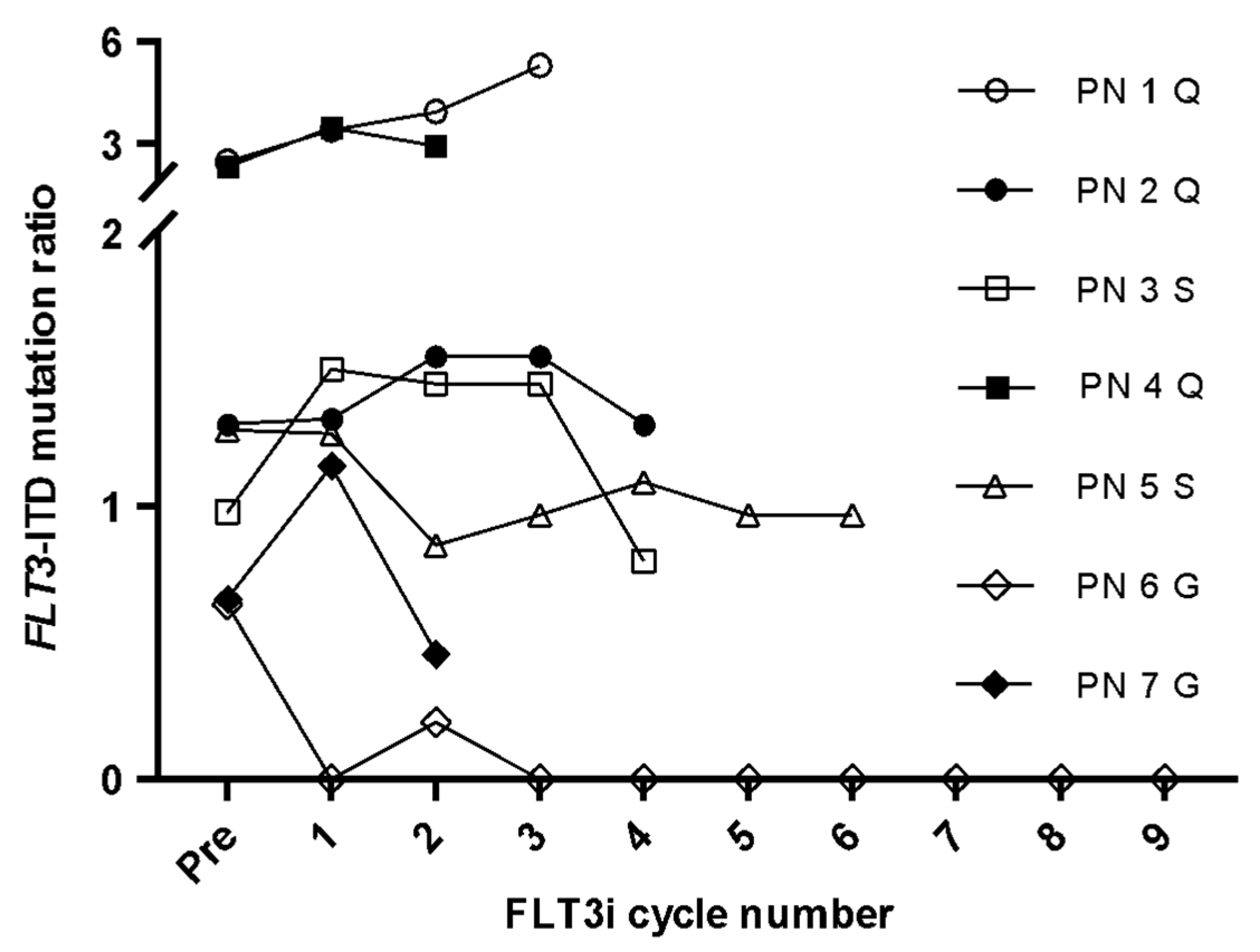
3.3. FLT3-ITD Expression for FLT3i Treatment Monitoring
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lagunas-Rangel, F.A.; Chávez-Valencia, V. FLT3–ITD and its current role in acute myeloid leukaemia. Med. Oncol. 2017, 34, 114. [Google Scholar] [CrossRef] [PubMed]
- Papaemmanuil, E.; Gerstung, M.; Bullinger, L.; Gaidzik, V.I.; Paschka, P.; Roberts, N.D.; Potter, N.E.; Heuser, M.; Thol, F.; Bolli, N.; et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N. Engl. J. Med. 2016, 374, 2209–2221. [Google Scholar] [CrossRef]
- Döhner, H.; Estey, E.; Grimwade, D.; Amadori, S.; Appelbaum, F.R.; Büchner, T.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Larson, R.A.; et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017, 129, 424–447. [Google Scholar] [CrossRef] [PubMed]
- Tallman, M.S.; Wang, E.S.; Altman, J.K.; Appelbaum, F.R.; Bhatt, V.R.; Bixby, D.; Coutre, S.E.; De Lima, M.; Fathi, A.T.; Fiorella, M.; et al. Acute Myeloid Leukemia, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2019, 17, 721–749. [Google Scholar] [CrossRef]
- Loke, J.; Buka, R.; Craddock, C. Allogeneic Stem Cell Transplantation for Acute Myeloid Leukemia: Who, When, and How? Front. Immunol. 2021, 12, 659595. [Google Scholar] [CrossRef] [PubMed]
- Daver, N.; Schlenk, R.F.; Russell, N.H.; Levis, M.J. Targeting FLT3 mutations in AML: Review of current knowledge and evidence. Leukemia 2019, 33, 299–312. [Google Scholar] [CrossRef]
- Short, N.; Kantarjian, H.; Ravandi, F.; Daver, N. Emerging treatment paradigms with FLT3 inhibitors in acute myeloid leukemia. Ther. Adv. Hematol. 2019, 10, 204062071982731. [Google Scholar] [CrossRef]
- Levis, M. Midostaurin approved for FLT3-mutated AML. Blood 2017, 129, 3403–3406. [Google Scholar] [CrossRef]
- Dhillon, S. Gilteritinib: First Global Approval. Drugs 2019, 79, 331–339. [Google Scholar] [CrossRef]
- Antar, A.; Otrock, Z.K.; El-Cheikh, J.; Kharfan-Dabaja, M.A.; Battipaglia, G.; Mahfouz, R.; Mohty, M.; Bazarbachi, A. Inhibition of FLT3 in AML: A focus on sorafenib. Bone Marrow Transpl. 2016, 52, 344–351. [Google Scholar] [CrossRef]
- Levis, M. Quizartinib for the treatment of FLT3/ITD acute myeloid leukemia. Future Oncol. Lond. Engl. 2014, 10, 1571–1579. [Google Scholar] [CrossRef] [PubMed]
- Kiyoi, H.; Kawashima, N.; Ishikawa, Y. FLT3 mutations in acute myeloid leukemia: Therapeutic paradigm beyond inhibitor development. Cancer Sci. 2020, 111, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.M.; Levis, M.; Hafez, M.J.; Geiger, T.; Cooper, L.C.; Smith, B.; Small, D.; Berg, K.D. Detection of FLT3 Internal Tandem Duplication and D835 Mutations by a Multiplex Polymerase Chain Reaction and Capillary Electrophoresis Assay. J. Mol. Diagn. 2003, 5, 96–102. [Google Scholar] [CrossRef]
- Cloos, J.; Goemans, B.F.; Hess, C.J.; Van Oostveen, J.W.; Waisfisz, Q.; Corthals, S.L.; De Lange, D.; Boeckx, N.; Hählen, K.; Reinhardt, D.; et al. Stability and prognostic influence of FLT3 mutations in paired initial and relapsed AML samples. Leukemia 2006, 20, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Gorello, P.; Cazzaniga, G.; Alberti, F.; Dell’Oro, M.G.; Gottardi, E.; Specchia, G.; Roti, G.; Rosati, R.; Martelli, M.F.; Diverio, D.; et al. Quantitative assessment of minimal residual disease in acute myeloid leukemia carrying nucleophosmin (NPM1) gene mutations. Leukemia 2006, 20, 1103–1108. [Google Scholar] [CrossRef]
- Kwon, M.; Martínez-Laperche, C.; Infante, M.; Carretero, F.; Balsalobre, P.; Serrano, D.; Gayoso, J.; Pérez-Corral, A.; Anguita, J.; Díez-Martín, J.L.; et al. Evaluation of Minimal Residual Disease by Real-Time Quantitative PCR of Wilms’ Tumor 1 Expression in Patients with Acute Myelogenous Leukemia after Allogeneic Stem Cell Transplantation: Correlation with Flow Cytometry and Chimerism. Biol. Blood Marrow Transpl. 2012, 18, 1235–1242. [Google Scholar] [CrossRef]
- Patnaik, M.M. The importance of FLT3 mutational analysis in acute myeloid leukemia. Leuk. Lymphoma 2017, 59, 2273–2286. [Google Scholar] [CrossRef]
- Kondo, M.; Horibe, K.; Takahashi, Y.; Matsumoto, A.; Fukuda, M.; Inaba, J.; Kato, K.; Kojima, S.; Matsuyama, T. Prognostic value of internal tandem duplication of the FLT3 gene in childhood acute myelogenous leukemia. Med. Pediatr. Oncol. 1999, 33, 525–529. [Google Scholar] [CrossRef]
- Cucchi, D.J.G.; Denys, B.; Kaspers, G.J.L.; Janssen, J.J.W.M.; Ossenkoppele, G.J.; De Haas, V.; Zwaan, C.M.; Heuvel-Eibrink, M.M.V.D.; Philippé, J.; Csikós, T.; et al. RNA-based FLT3-ITD allelic ratio is associated with outcome and ex vivo response to FLT3 inhibitors in pediatric AML. Blood 2018, 131, 2485–2489. [Google Scholar] [CrossRef]
- Cucchi, D.G.J.; Vonk, C.M.; Rijken, M.; Kavelaars, F.G.; Merle, P.A.; Verhoef, E.; Venniker-Punt, B.; Kwidama, Z.J.; Gradowska, P.; Löwenberg, B.; et al. DNA vs cDNA FLT3-ITD allelic ratio and length measurements in adult acute myeloid leukemia. Blood Adv. 2021, 5, 4476–4479. [Google Scholar] [CrossRef]
- Whitman, S.P.; Archer, K.; Feng, L.; Baldus, C.; Becknell, B.; Carlson, B.D.; Carroll, A.J.; Mrózek, K.; Vardiman, J.W.; George, S.L.; et al. Absence of the wild-type allele predicts poor prognosis in adult de novo acute myeloid leukemia with normal cytogenetics and the internal tandem duplication of FLT3: A cancer and leukemia group B study. Cancer Res. 2001, 61, 7233–7239. [Google Scholar] [PubMed]
- Nazha, A.; Cortes, J.; Faderl, S.; Pierce, S.; Daver, N.; Kadia, T.; Borthakur, G.; Luthra, R.; Kantarjian, H.; Ravandi, F. Activating internal tandem duplication mutations of the fms-like tyrosine kinase-3 (FLT3-ITD) at complete response and relapse in patients with acute myeloid leukemia. Haematologica 2012, 97, 1242–1245. [Google Scholar] [CrossRef] [PubMed]
- Ossenkoppele, G.; Schuurhuis, G.J. MRD in AML: Does it already guide therapy decision-making? Hematology 2016, 2016, 356–365. [Google Scholar] [CrossRef]
- Chou, W.-C.; Hou, H.-A.; Liu, C.-Y.; Chen, C.-Y.; Lin, L.-I.; Huang, Y.-N.; Chao, Y.-C.; Hsu, C.-A.; Huang, C.-F.; Tien, H.-F. Sensitive measurement of quantity dynamics of FLT3 internal tandem duplication at early time points provides prognostic information. Ann. Oncol. 2010, 22, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Schiller, J.; Praulich, I.; Rocha, C.K.; Kreuzer, K.-A. Patient-specific analysis of FLT3 internal tandem duplications for the prognostication and monitoring of acute myeloid leukemia. Eur. J. Haematol. 2012, 89, 53–62. [Google Scholar] [CrossRef]
- Grunwald, M.R.; Tseng, L.-H.; Lin, M.-T.; Pratz, K.W.; Eshleman, J.R.; Levis, M.J.; Gocke, C.D. Improved FLT3 Internal Tandem Duplication PCR Assay Predicts Outcome after Allogeneic Transplant for Acute Myeloid Leukemia. Biol. Blood Marrow Transpl. 2014, 20, 1989–1995. [Google Scholar] [CrossRef]
- Levis, M.J.; Perl, A.E.; Altman, J.K.; Gocke, C.D.; Bahceci, E.; Hill, J.; Liu, C.; Xie, Z.; Carson, A.R.; McClain, V.; et al. A next-generation sequencing–based assay for minimal residual disease assessment in AML patients with FLT3-ITD mutations. Blood Adv. 2018, 2, 825–831. [Google Scholar] [CrossRef]
- Perl, A.E. The role of targeted therapy in the management of patients with AML. Hematology 2017, 2017, 54–65. [Google Scholar] [CrossRef]
- Daver, N.; Venugopal, S.; Ravandi, F. FLT3 mutated acute myeloid leukemia: 2021 treatment algorithm. Blood Cancer J. 2021, 11, 104. [Google Scholar] [CrossRef]
- Altman, J.K.; Perl, A.E.; Hill, J.E.; Rosales, M.; Bahceci, E.; Levis, M.J. The impact of FLT3 mutation clearance and treatment response after gilteritinib therapy on overall survival in patients with FLT3 mutation–positive relapsed/refractory acute myeloid leukemia. Cancer Med. 2021, 10, 797–805. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort | Diagnosis | Post-HSCT | Post-FLT3i |
|---|---|---|---|
| n | 46 | 34 | 7 |
| Age, median (range), years | 63 (27–91) | 45 (27–65) | 52 (31–65) |
| Female sex, n (%) | 15 (32.6) | 14 (41.2) | 3 (42.9) |
| Induction therapy, n (%) | |||
| IA 3 × 7 | 27 (58.7) | 29 (85.3) | 5 (71.4) |
| IA 3 × 7 + FLT3i | 5 (10.9) | 2 (5.9) | 2 (28.6) |
| Hypomethylating | 3 (6.5) | 0 (0.0) | 0 (0.0) |
| Other | 1 (2.1) | 3 (8.8) | 0 (0.0) |
| Palliative care | 10 (21.8) | 0 (0.0) | 0 (0.0) |
| Allo-HSCT | |||
| HSCT type, n (%) | |||
| Haploidentical | - | 17 (50.0) | - |
| HLA-identical | - | 15 (44.1) | - |
| Haplo-cord | - | 2 (5.9) | - |
| Conditioning regimen, n (%) | |||
| Myeloablative | - | 26 (76.5) | - |
| Reduced intensity | - | 8 (23.5) | - |
| FLT3i in patients with R/R AML | |||
| Quizartinib | - | - | 3 (42.8) |
| Sorafenib | - | - | 2 (28.6) |
| Gilteritinib | - | - | 2 (28.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carbonell, D.; Chicano, M.; Cardero, A.J.; Gómez-Centurión, I.; Bailén, R.; Oarbeascoa, G.; Martínez-Señarís, D.; Franco, C.; Muñiz, P.; Anguita, J.; et al. FLT3-ITD Expression as a Potential Biomarker for the Assessment of Treatment Response in Patients with Acute Myeloid Leukemia. Cancers 2022, 14, 4006. https://doi.org/10.3390/cancers14164006
Carbonell D, Chicano M, Cardero AJ, Gómez-Centurión I, Bailén R, Oarbeascoa G, Martínez-Señarís D, Franco C, Muñiz P, Anguita J, et al. FLT3-ITD Expression as a Potential Biomarker for the Assessment of Treatment Response in Patients with Acute Myeloid Leukemia. Cancers. 2022; 14(16):4006. https://doi.org/10.3390/cancers14164006
Chicago/Turabian StyleCarbonell, Diego, María Chicano, Alfonso J. Cardero, Ignacio Gómez-Centurión, Rebeca Bailén, Gillen Oarbeascoa, Diana Martínez-Señarís, Carolina Franco, Paula Muñiz, Javier Anguita, and et al. 2022. "FLT3-ITD Expression as a Potential Biomarker for the Assessment of Treatment Response in Patients with Acute Myeloid Leukemia" Cancers 14, no. 16: 4006. https://doi.org/10.3390/cancers14164006