
Identification of Leukemia-Associated Immunophenotypes by Databaseguided Flow Cytometry Provides a Highly Sensitive and Reproducible Strategy for the Study of Measurable Residual Disease in Acute Myeloblastic Leukemia

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
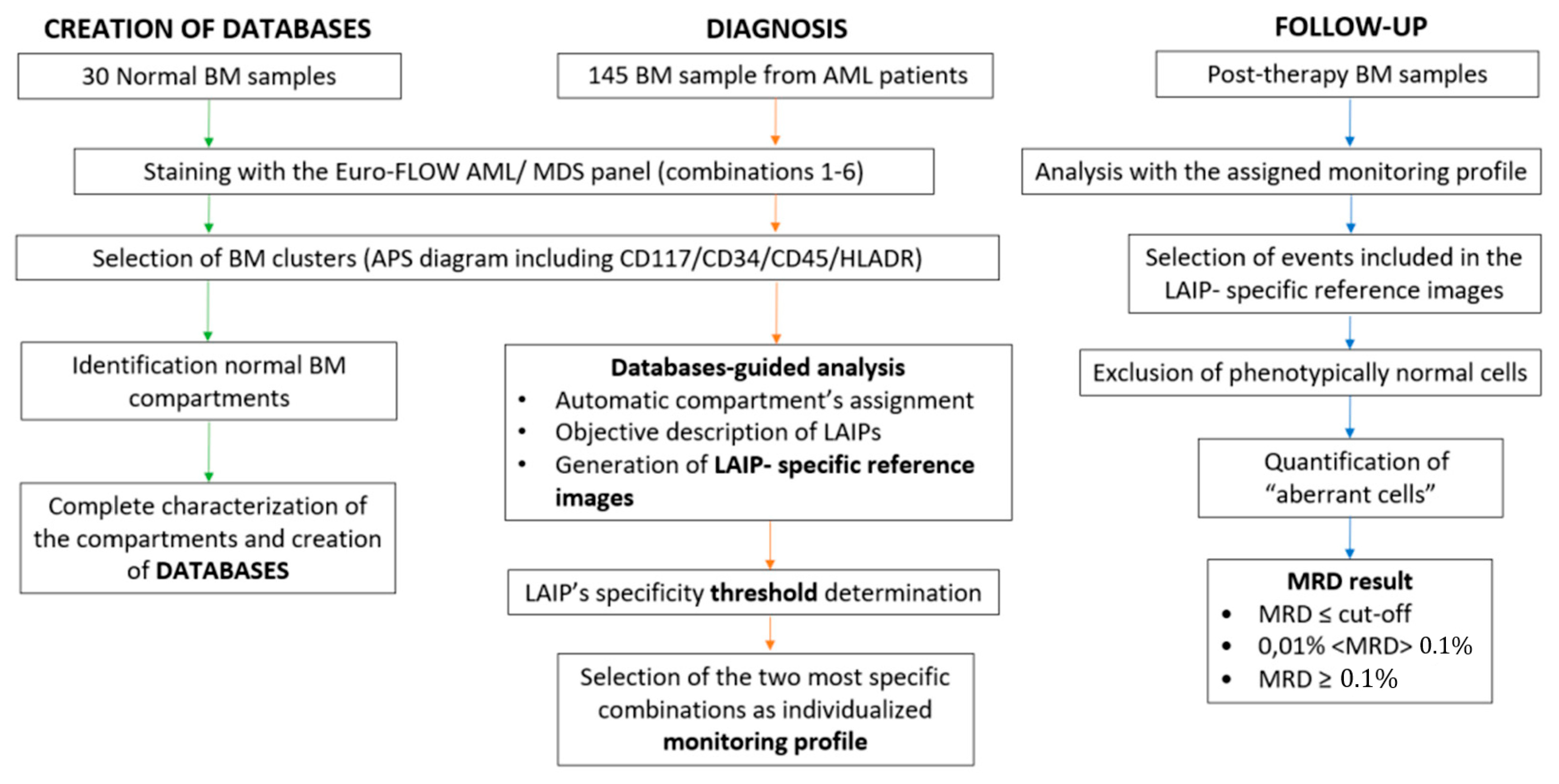
2.1. General Study Strategy
2.2. Patients and Samples
2.3. Flow Cytometry
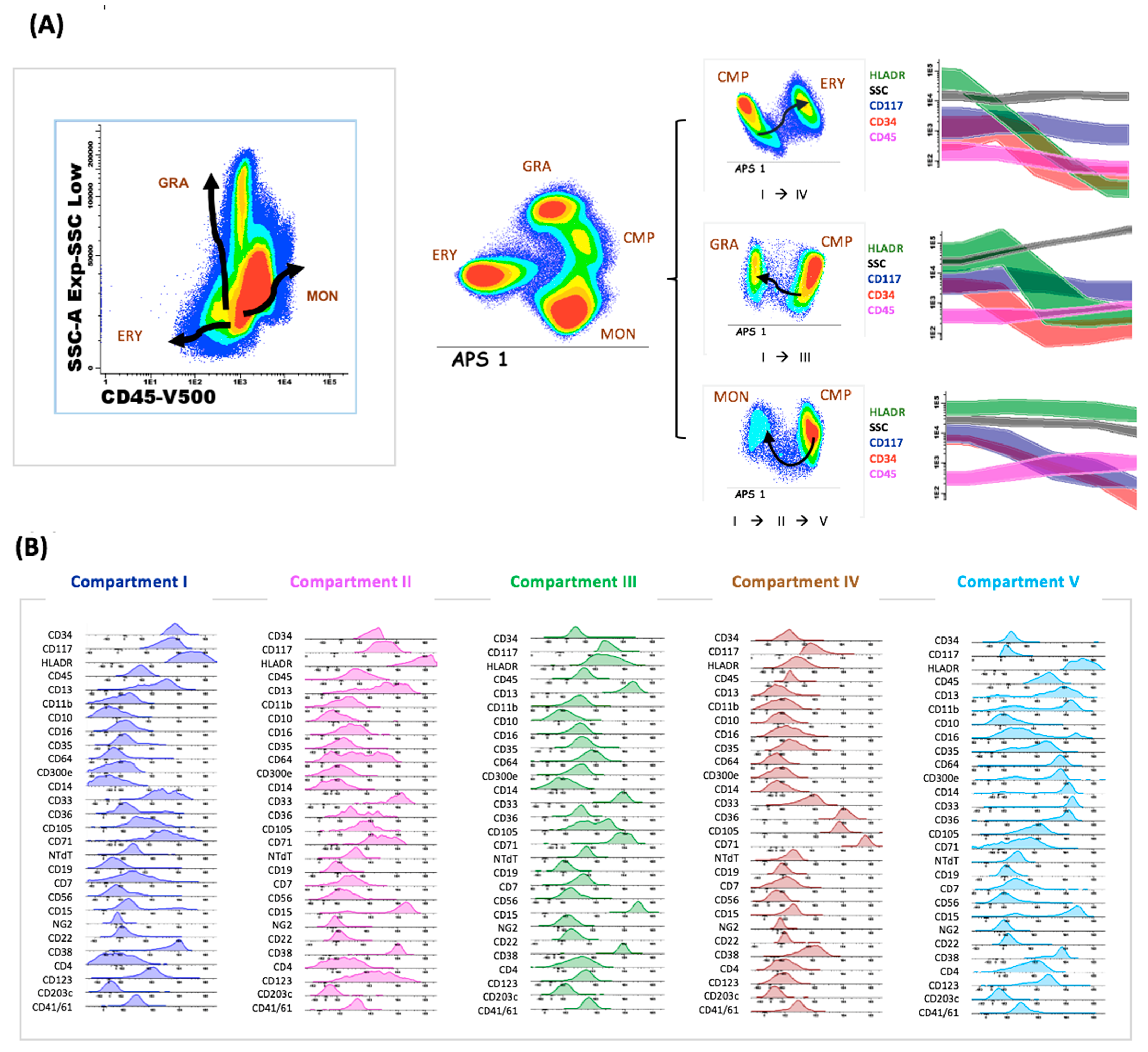
2.4. Normal Databases
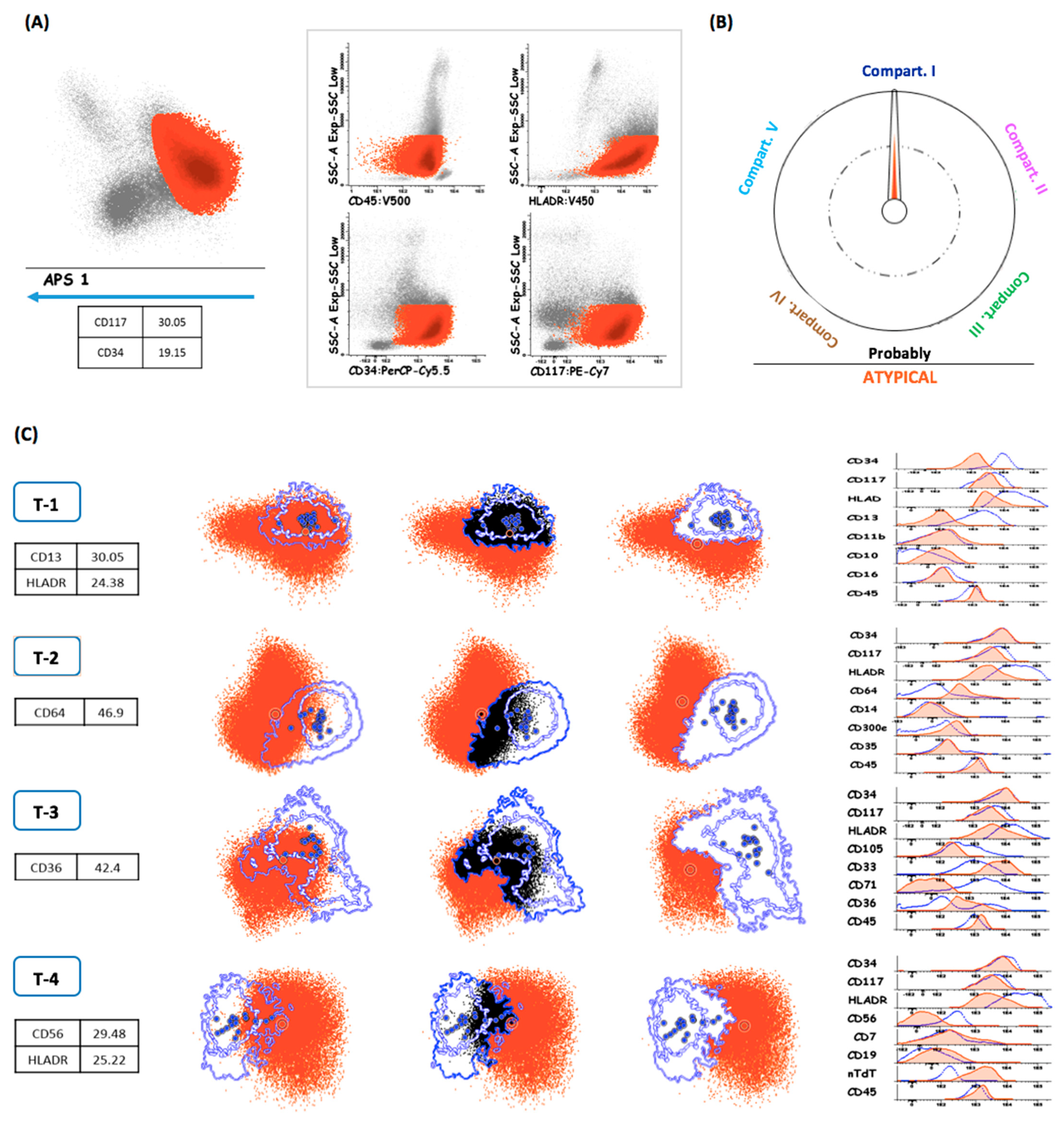
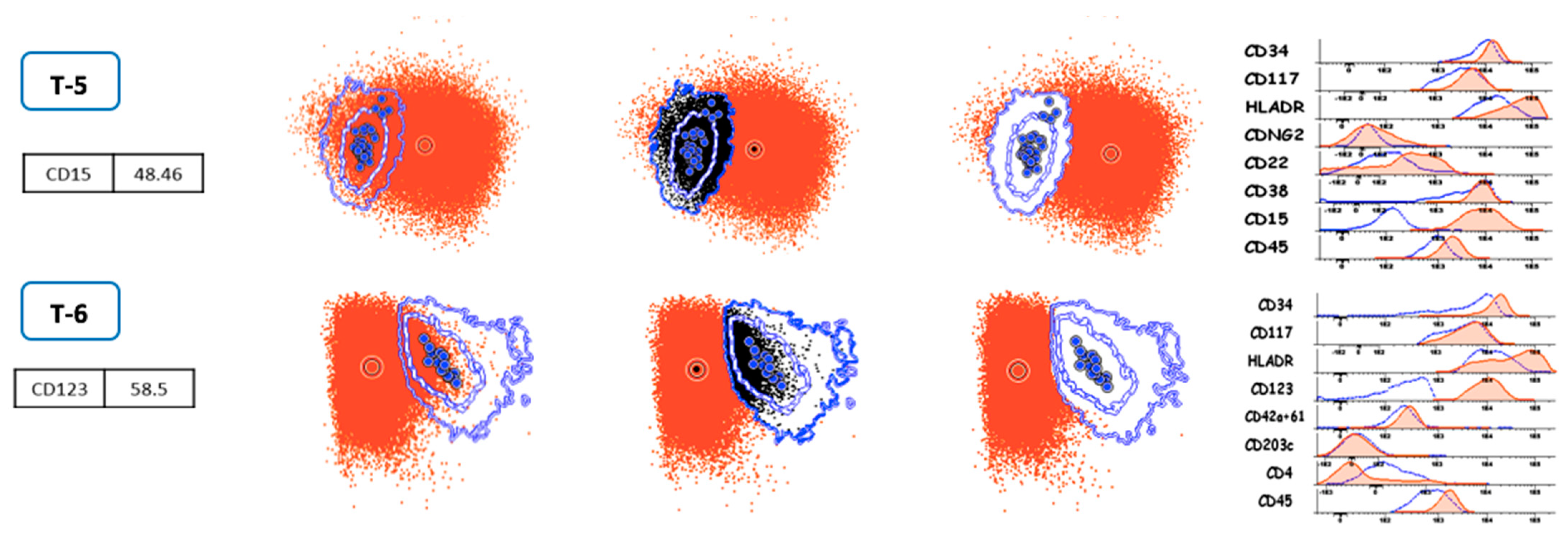
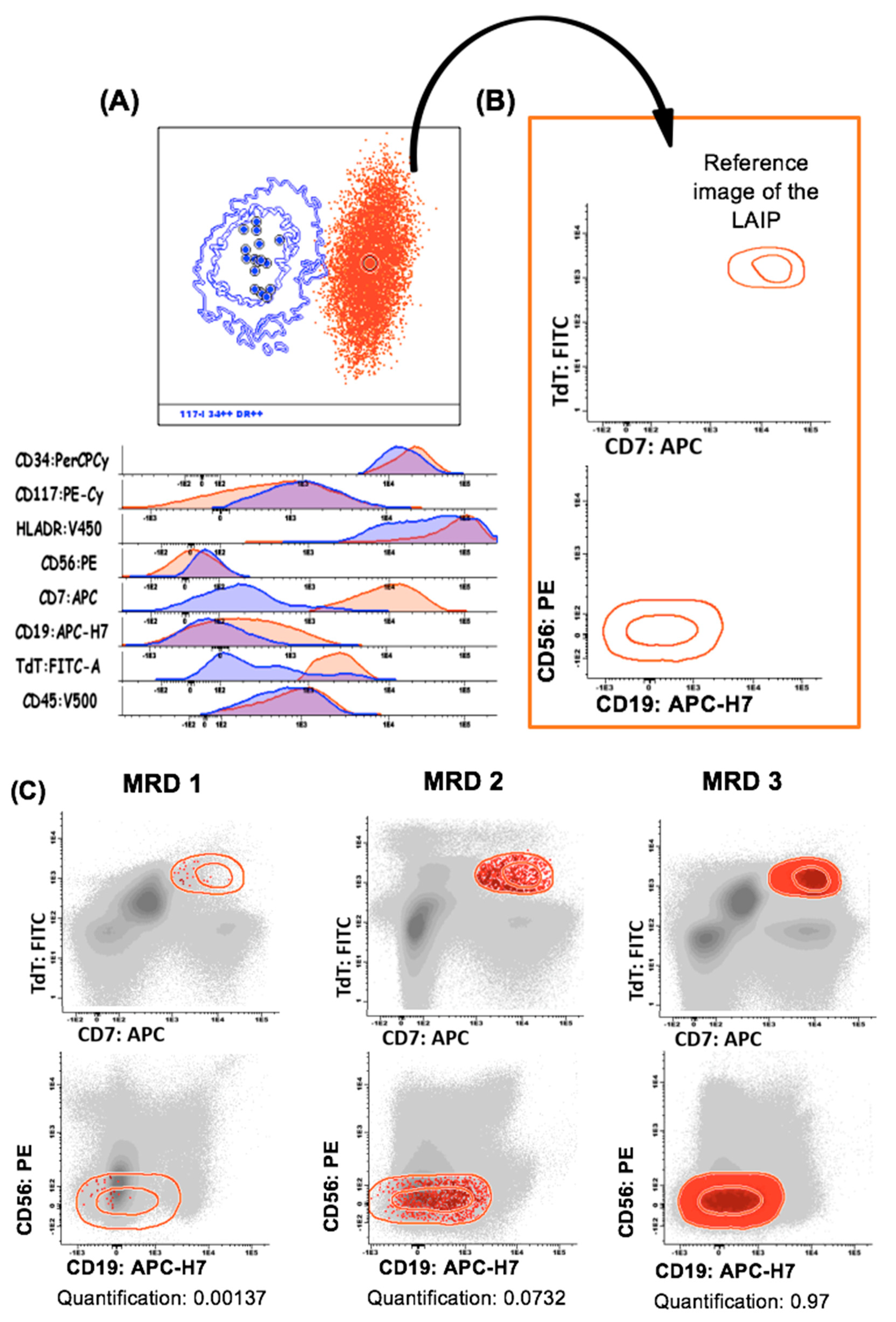
2.5. LAIP Characterization and Description and MFC-MRD Analysis
2.6. Generation of Individualized Monitoring Profiles
2.7. Specificity of LAIPs in Regenerative Bone Marrow Samples
2.8. MFC-MRD Analysis
2.9. PCR-Based MRD Analysis
2.10. Next-Generation Sequencing
2.11. Statistical Methods
3. Results
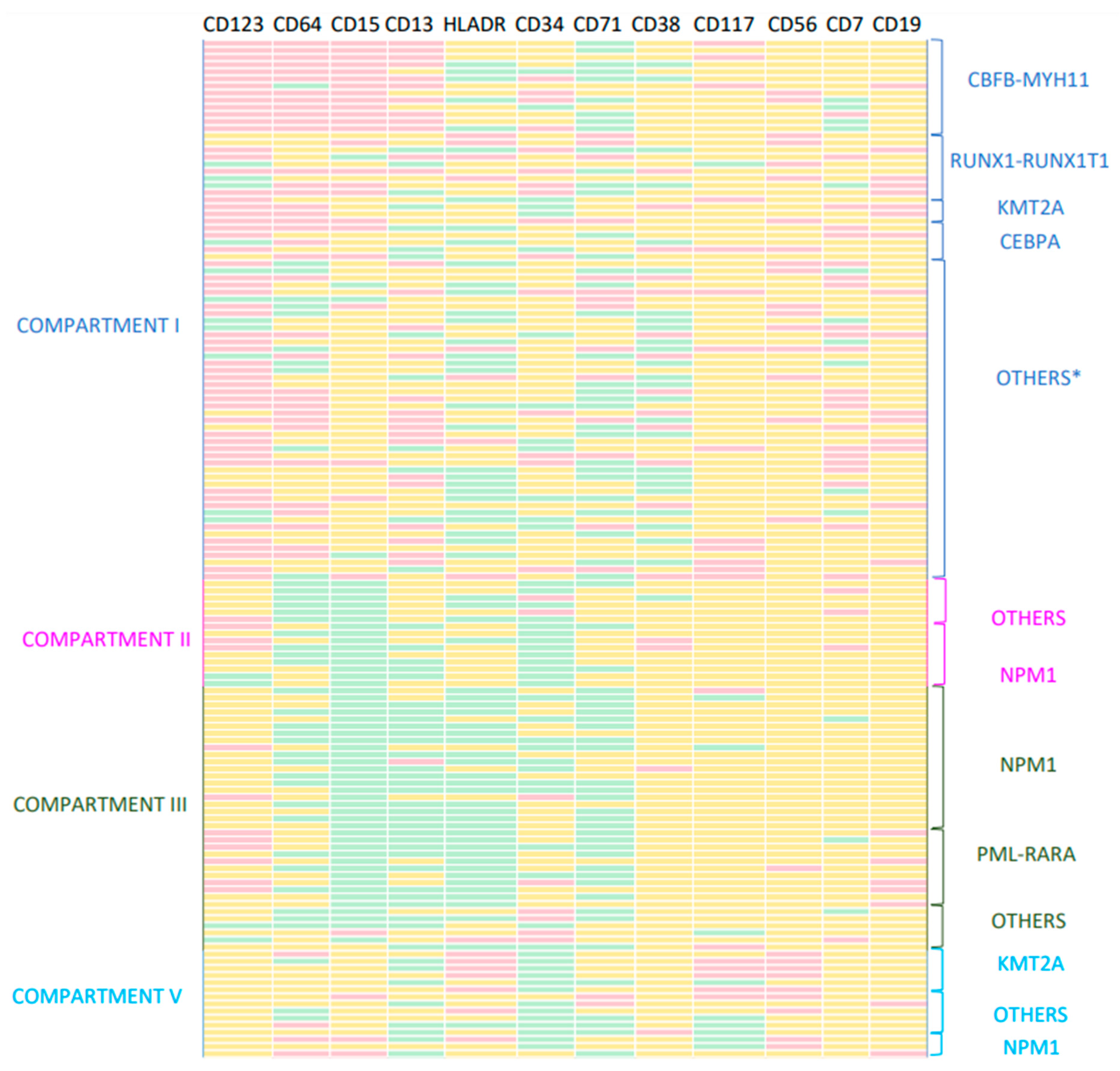
3.1. Classification and Characteristics of LAIPs
3.2. LAIPs and AML World Health Organization (WHO) Molecular Subtypes
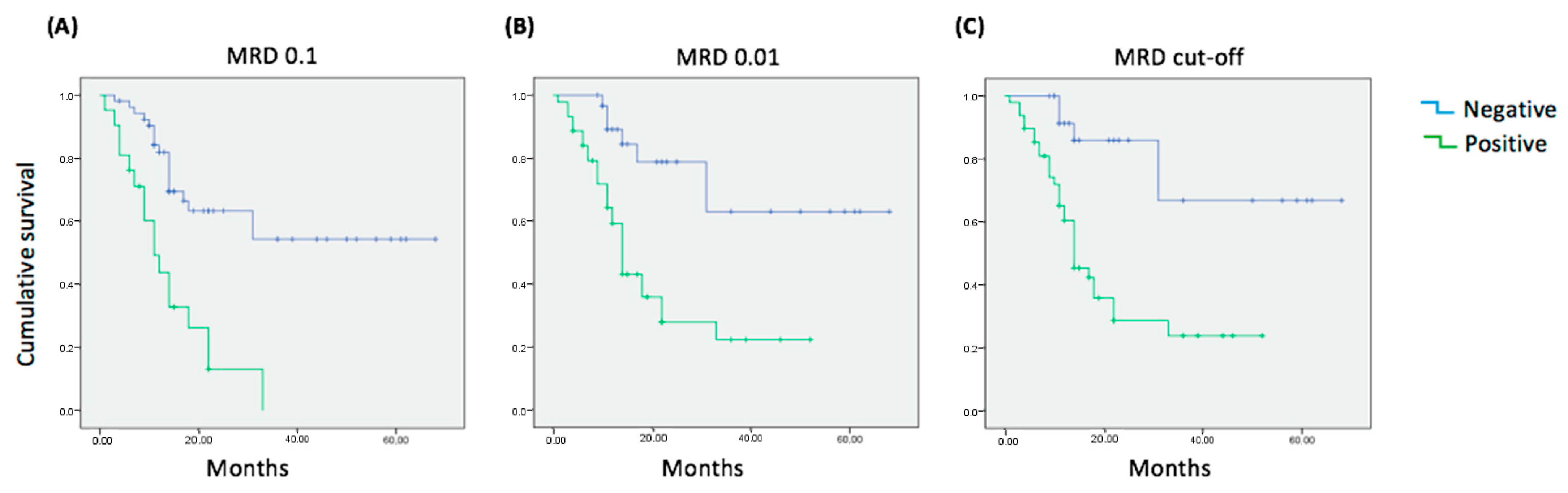
3.3. MFC-MRD Study and Progression-Free Survival
3.4. MFC-MRD and qPCR-MRD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bewersdorf, J.P.; Carraway, H.; Prebet, T. Emerging treatment options for patients with high-risk myelodysplastic syndrome. Ther. Adv. Hematol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Buccisano, F.; Dillon, R.; Freeman, S.D.; Venditti, A. Role of Minimal (Measurable) Residual Disease Assessment in Older Patients with Acute Myeloid Leukemia. Cancers 2018, 10, 215. [Google Scholar] [CrossRef] [PubMed]
- Short, N.J.; Zhou, S.; Fu, C.; Berry, D.A.; Walter, R.B.; Freeman, S.D.; Hourigan, C.S.; Huang, X.; Gonzalez, G.N.; Hwang, H.; et al. Association of Measurable Residual Disease with Survival Outcomes in Patients With Acute Myeloid Leukemia: A Systematic Review and Meta-analysis. JAMA Oncol. 2020, 6, 1890–1899. [Google Scholar] [CrossRef] [PubMed]
- Rossi, G.; Giambra, V.; Minervini, M.M.; de Waure, C.; Mancinelli, S.; Ciavarella, M.; Sinisi, N.P.; Scalzulli, P.R.; Carella, A.M.; Cascavilla, N. Leukemia-associated immunophenotypes subdivided in “categories of specificity” improve the sensitivity of minimal residual disease in predicting relapse in acute myeloid leukemia. Cytom. Part B Clin. Cytom. 2019, 98, 216–225. [Google Scholar] [CrossRef]
- Maiti, A.; Qiao, W.; Sasaki, K.; Ravandi, F.; Kadia, T.M.; Jabbour, E.J.; Daver, N.G.; Borthakur, G.; Garcia-Manero, G.; Pierce, S.A.; et al. Venetoclax with decitabine vs intensive chemotherapy in acute myeloid leukemia: A propensity score matched analysis stratified by risk of treatment-related mortality. Am. J. Hematol. 2020, 96, 282–291. [Google Scholar] [CrossRef]
- Ossenkoppele, G.; Schuurhuis, G.J.; van de Loosdrecht, A.; Cloos, J. Can we incorporate MRD assessment into clinical practice in AML? Best Pract. Res. Clin. Haematol. 2019, 32, 186–191. [Google Scholar] [CrossRef]
- Klyuchnikov, E.; Christopeit, M.; Badbaran, A.; Bacher, U.; Fritzsche-Friedland, U.; von Pein, U.; Wolschke, C.; Kröger, N. Role of pre-transplant MRD level detected by flow cytometry in recipients of allogeneic stem cell transplantation with AML. Eur. J. Haematol. 2020, 106, 606–615. [Google Scholar] [CrossRef]
- Schuurhuis, G.J.; Heuser, M.; Freeman, S.; Béné, M.-C.; Buccisano, F.; Cloos, J.; Grimwade, D.; Haferlach, T.; Hills, R.K.; Hourigan, C.S.; et al. Minimal/measurable residual disease in AML: A consensus document from the European LeukemiaNet MRD Working Party. Blood 2018, 131, 1275–1291. [Google Scholar] [CrossRef]
- Paterno, G.; Del Principe, M.I.; Venditti, A. Detection and management of acute myeloid leukemia measurable residual disease: Is it standard of care? Curr. Opin. Hematol. 2020, 27, 81–87. [Google Scholar] [CrossRef]
- Shang, L.; Cai, X.; Sun, W.; Cheng, Q.; Mi, Y. Time point-dependent concordance and prognostic significance of flow cytometry and real time quantitative PCR for measurable/minimal residual disease detection in acute myeloid leukemia with t(8;21)(q22;q22.1). Cytom. Part B Clin. Cytom. 2021, 102, 34–43. [Google Scholar] [CrossRef]
- Camburn, A.E.; Petrasich, M.; Ruskova, A.; Chan, G. Myeloblasts in normal bone marrows expressing leukaemia-associated immunophenotypes. Pathology 2019, 51, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Kriegsmann, K.; Löffler, H.; Eckstein, V.; Schulz, R.; Kräker, S.; Braun, U.; Luft, T.; Hegenbart, U.; Schönland, S.; Dreger, P.; et al. CD7 is expressed on a subset of normal CD34-positive myeloid precursors. Eur. J. Haematol. 2018, 101, 318–325. [Google Scholar] [CrossRef] [PubMed]
- Cui, W.; Zhang, D.; Cunningham, M.T.; Tilzer, L. Leukemia-associated aberrant immunophenotype in patients with acute myeloid leukemia: Changes at refractory disease or first relapse and clinicopathological findings. Int. J. Lab. Hematol. 2014, 36, 636–649. [Google Scholar] [CrossRef] [PubMed]
- Sui, J.; Chen, Q.; Zhang, Y.; Sheng, Y.; Wu, J.; Li, J.; Weng, X.; Chen, B. Identifying leukemia-associated immunophenotype-based individualized minimal residual disease in acute myeloid leukemia and its prognostic significance. Am. J. Hematol. 2019, 94, 528–538. [Google Scholar] [CrossRef]
- Schuurhuis, G.J.; Ossenkoppele, G.J.; Kelder, A.; Cloos, J. Measurable residual disease in acute myeloid leukemia using flow cytometry: Approaches for harmonization/standardization. Expert Rev. Hematol. 2018, 11, 921–935. [Google Scholar] [CrossRef] [PubMed]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Kalina, T.; Flores-Montero, J.; van der Velden, V.H.J.; Martin-Ayuso, M.; Böttcher, S.; Ritgen, M.; Almeida, J.; Lhermitte, L.; Asnafi, V.; Mendonça, A.; et al. EuroFlow standardization of flow cytometer instrument settings and immunophenotyping protocols. Leukemia 2012, 26, 1986–2010. [Google Scholar] [CrossRef]
- Van Dongen, J.J.M.; Lhermitte, L.; Böttcher, S.; Almeida, J.R.S.; van der Velden, V.H.J.; Flores-Montero, J.; Rawstron, A.; Asnafi, V.; Lecrevisse, Q.; Lucio, P.; et al. EuroFlow antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive and malignant leukocytes. Leukemia 2012, 26, 1908–1975. [Google Scholar] [CrossRef]
- Lhermitte, L.; Barreau, S.; Morf, D.; Fernandez, P.; Grigore, G.; Barrena, S.; de Bie, M.; Flores-Montero, J.; Brüggemann, M.; Mejstrikova, E.; et al. Automated identification of leukocyte subsets improves standardization of database-guided expert-supervised diagnostic orientation in acute leukemia: A EuroFlow study. Mod. Pathol. 2020, 34, 59–69. [Google Scholar] [CrossRef]
- Aanei, C.-M.; Veyrat-Masson, R.; Selicean, C.; Marian, M.; Rigollet, L.; Trifa, A.P.; Tomuleasa, C.; Serban, A.; Cherry, M.; Flandrin-Gresta, P.; et al. Database-Guided Analysis for Immunophenotypic Diagnosis and Follow-Up of Acute Myeloid Leukemia with Recurrent Genetic Abnormalities. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef]
- Paiva, B.; Vidriales, M.-B.; Sempere, A.; Tarín, F.; Colado, E.; Benavente, C.; Cedena, M.-T.; Sánchez, J.; Caballero-Velazquez, T.; Cordón, L.; et al. Impact of measurable residual disease by decentralized flow cytometry: A PETHEMA real-world study in 1076 patients with acute myeloid leukemia. Leukemia 2021, 35, 2358–2370. [Google Scholar] [CrossRef] [PubMed]
- Vial, J.; Lechevalier, N.; Lacombe, F.; Dumas, P.-Y.; Bidet, A.; Leguay, T.; Vergez, F.; Pigneux, A.; Béné, M. Unsupervised Flow Cytometry Analysis Allows for an Accurate Identification of Minimal Residual Disease Assessment in Acute Myeloid Leukemia. Cancers 2021, 13, 629. [Google Scholar] [CrossRef] [PubMed]
- Ossenkoppele, G.J.; van de Loosdrecht, A.A.; Schuurhuis, G.J. Review of the relevance of aberrant antigen expression by flow cytometry in myeloid neoplasms. Br. J. Haematol. 2011, 153, 421–436. [Google Scholar] [CrossRef]
- Rossi, G.; Guinot, J.F.N.; Fontana, A.; Minervini, M.M.; García-Dabrio, M.C.; Cascavilla, N. CD117-CD15 in acute myeloid leukemia: No role as LAIP in the study of minimal residual disease. Eur. J. Haematol. 2012, 90, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Al-Mawali, A.; Gillis, D.; Hissaria, P.; Lewis, I. Incidence, Sensitivity, and Specificity of Leukemia-Associated Phenotypes in Acute Myeloid Leukemia Using Specific Five-Color Multiparameter Flow Cytometry. Am. J. Clin. Pathol. 2008, 129, 934–945. [Google Scholar] [CrossRef] [PubMed]
- Voskova, D.; Schoch, C.; Schnittger, S.; Hiddemann, W.; Haferlach, T.; Kern, W. Stability of leukemia-associated aberrant immunophenotypes in patients with acute myeloid leukemia between diagnosis and relapse: Comparison with cytomorphologic, cytogenetic, and molecular genetic findings. Cytometry 2004, 62B, 25–38. [Google Scholar] [CrossRef]
- Orfao, A.; Chillón, M.C.; Bortoluci, A.M.; López-Berges, M.C.; García-Sanz, R.; Gonzalez, M.; Tabernero, M.D.; García-Marcos, M.A.; Rasillo, A.I.; Hernández-Rivas, J.; et al. The flow cytometric pattern of CD34, CD15 and CD13 expression in acute myeloblastic leukemia is highly characteristic of the presence of PML-RARalpha gene rearrangements. Haematologica 1999, 84, 405–412. [Google Scholar]
- Andrieu, V.; Radford-Weissis, I.; Troussard, X.; Chane, C.; Valensi, F.; Guesnu, M.; Haddad, E.; Viguier, F.; Dreyfus, F.; Varet, B.; et al. Molecular detection of t(8;21)/AML1-ETO in AML M1/M2: Correlation with cytogenetics, morphology and immunophenotype. Br. J. Haematol. 1996, 92, 855–865. [Google Scholar] [CrossRef]
- Adriaansen, H.J.; Boekhorst, P.A.T.; Hagemeijer, A.M.; van der Schoot, C.E.; Delwel, H.R.; van Dongen, J.J. Acute myeloid leukemia M4 with bone marrow eosinophilia (M4Eo) and inv(16)(p13q22) exhibits a specific immunophenotype with CD2 expression. Blood 1993, 81, 3043–3051. [Google Scholar] [CrossRef]
- Bhatia, M.; Wang, J.C.Y.; Kapp, U.; Bonnet, D.; Dick, J.E. Purification of primitive human hematopoietic cells capable of repopulating immune-deficient mice. Proc. Natl. Acad. Sci. USA 1997, 94, 5320–5325. [Google Scholar] [CrossRef]
- Jordan, C.T. The leukemic stem cell. Best Pract. Res. Clin. Haematol. 2007, 20, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Haubner, S.; Perna, F.; Köhnke, T.; Schmidt, C.; Berman, S.; Augsberger, C.; Schnorfeil, F.M.; Krupka, C.; Lichtenegger, F.S.; Liu, X.; et al. Coexpression profile of leukemic stem cell markers for combinatorial targeted therapy in AML. Leukemia 2018, 33, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Patkar, N.; Kakirde, C.; Shaikh, A.F.; Salve, R.; Bhanshe, P.; Chatterjee, G.; Rajpal, S.; Joshi, S.; Chaudhary, S.; Kodgule, R.; et al. Clinical impact of panel-based error-corrected next generation sequencing versus flow cytometry to detect measurable residual disease (MRD) in acute myeloid leukemia (AML). Leukemia 2021, 35, 1392–1404. [Google Scholar] [CrossRef] [PubMed]
- Getta, B.M.; Devlin, S.M.; Levine, R.L.; Arcila, M.E.; Mohanty, A.S.; Zehir, A.; Tallman, M.S.; Giralt, S.A.; Roshal, M. Multicolor Flow Cytometry and Multigene Next-Generation Sequencing Are Complementary and Highly Predictive for Relapse in Acute Myeloid Leukemia after Allogeneic Transplantation. Biol. Blood Marrow Transplant. 2017, 23, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Zeijlemaker, W.; Gratama, J.W.; Schuurhuis, G.J. Tumor heterogeneity makes AML a “moving target” for detection of residual disease. Cytom. B Clin. Cytom. 2014, 86, 3–14. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics (n = 145) | |
|---|---|
| Sex (Male/Female) | 145 (78/69) |
| Mean age (range) | 61.9 (18–92) |
| Leucocytes × 109(range) | 26.3 (0.3–323) |
| Hemoglobin (g/L) (range) | 93.5 (35.3–143.3) |
| Platelets × 109(range) | 44.9 (2–402) |
| % Bone marrow blasts (range) | 55.7 (11–99) |
| AML Subtypes (WHO classification) | |
| AML with recurrent genetic abnormalites | 88 (60.7%) |
| t(8;21) RUNX1-RUNX1T1 | 10 (6.9%) |
| Inv16 CBFB-MYH11 | 13 (8.9%) |
| t(15;17) PML-RARα | 11 (7.6%) |
| t(9;11) KMT2A-MLLT3 | 9 (6.2%) |
| t(6;9) DEK-NUP214 | 2 (1.4%) |
| Inv3 GATA2 | 1 (0.7%) |
| Mutated NPM1 | 32 (22.1%) |
| Bialelic mutation of CEBPA | 5 (3.4%) |
| Mutated RUNX1 | 4 (2.8%) |
| t(9;22) BCR-ABL | 1 (0.7%) |
| AML with myelodisplasia-related changes | 15 (10.3%) |
| Therapy-related neoplasms | 5 (3.4%) |
| AML, NOS | 37 (25.5%) |
| AML with minimal differentiation | 7 (4.8%) |
| AML without maduration | 9 (6.2%) |
| AML with maduration | 6 (4.1%) |
| Acute monoblastic and monocytic leukemia | 12 (8.3%) |
| Acute erithroid leukemia | 2 (1.4%) |
| Acute megakaryoblastic leukemia | 1 (0.7%) |
| Karyotype | |
| Normal | 28 (19.3%) |
| Recurrent | 46 (31.7%) |
| Isolated | 18 (12.4%) |
| complex | 15 (10.3%) |
| not valuable | 28 (19.3%) |
| Other molecular findings | |
| FLT3 | 34 (22.8%) |
| DNMT3A | 17 (11.7%) |
| IDH1/IDH2 | 13 (9.1%) |
| N-RAS | 12 (8.3%) |
| ASXL1 | 7 (4.8%) |
| SRFS2 | 11 (4.1%) |
| Others | 37 (22.1%) |
| Non determined | 26 (17.9%) |
| Compartment | Tube | Marker Expression | N | % | Specificity (X) | Range |
|---|---|---|---|---|---|---|
| I Common myeloid progenitor (CD117+/CD34+/CD45dim/HLADR+) | BB * | HLA-DRLO | 66 | 21.29 | 0.02458 | 0.00020–0.11120 |
| 1 | CD13HI | 19 | 6.13 | 0.02740 | 0.00087–0.13657 | |
| CD13LO | 10 | 3.23 | 0.03569 | 0.00463–0.23399 | ||
| 2 | CD64HI | 25 | 8.06 | 0.08999 | 0.01118–0.36406 | |
| 3 | CD71LO | 27 | 8.71 | 0.02702 | 0.00184–0.10109 | |
| 4 | CD7HI | 18 | 5.81 | 0.03547 | 0.00039–0.14360 | |
| CD56HI | 17 | 5.48 | 0.02225 | 0.00025–0.14360 | ||
| 5 | CD38LO | 21 | 6.77 | 0.03170 | 0.00027–0.13689 | |
| CD15HI | 20 | 6.45 | 0.04528 | 0.00377–0.13789 | ||
| 6 | CD123HI | 42 | 13.55 | 0.02254 | 0.00190–0.13594 | |
| miscellaneous | 84 | 27.10 | ||||
| II Early Monocytic precursor (CD117+/CD34dim/CD45dim/HLADR++) | BB * | CD34LO | 30 | 9.68 | 0.01832 | 0.00101–0.13354 |
| HLA-DRLO | 10 | 3.23 | 0.04299 | 0.00471–0.13354 | ||
| 1 | CD13LO | 5 | 1.61 | 0.01827 | 0.00470–0.01524 | |
| 2 | CD64LO | 11 | 3.55 | 0.02494 | 0.00096–0.05389 | |
| 3 | CD36LO | 7 | 2.26 | 0.01087 | 0.00121–0.02657 | |
| 5 | CD15LO | 14 | 4.52 | 0.02494 | 0.00056–0.08699 | |
| miscellaneous | 10 | 3.23 | ||||
| III Early Granulocytic precursor (CD117+/CD34+/CD45dim/ HLADRdim) | BB * | HLA-DRLO | 68 | 21.94 | 0.23994 | 0.00066–2.60679 |
| CD34LO | 15 | 4.84 | 0.13253 | 0.00124–0.94985 | ||
| 2 | CD64LO | 13 | 4.19 | 0.08943 | 0.01174–0.35095 | |
| 3 | CD71LO | 18 | 5.81 | 0.28597 | 0.00180–3.54725 | |
| 5 | CD15LO | 23 | 7.42 | 0.07621 | 0.00237–0.27567 | |
| CD4LO | 18 | 5.81 | 0.05802 | 0.00066–0.72277 | ||
| miscellaneous | 15 | 4.84 | ||||
| V Intermediate-mature monocytes (CD117+/-/CD34-/CD45+/HLADR+) | BB * | CD34LO | 20 | 6.45 | 0.14280 | 0.00061–0.68111 |
| HLA-DRHI | 9 | 2.90 | 0.01812 | 0.00027–0.06233 | ||
| 4 | CD56HI | 8 | 2.58 | 0.01607 | 0.00187–0.07922 | |
| 1 | CD13LO | 6 | 1.94 | 0.32114 | 0.00980–1.24166 | |
| miscellaneous | 24 | 7.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piñero, P.; Morillas, M.; Gutierrez, N.; Barragán, E.; Such, E.; Breña, J.; García-Hernández, M.C.; Gil, C.; Botella, C.; González-Navajas, J.M.; et al. Identification of Leukemia-Associated Immunophenotypes by Databaseguided Flow Cytometry Provides a Highly Sensitive and Reproducible Strategy for the Study of Measurable Residual Disease in Acute Myeloblastic Leukemia. Cancers 2022, 14, 4010. https://doi.org/10.3390/cancers14164010
Piñero P, Morillas M, Gutierrez N, Barragán E, Such E, Breña J, García-Hernández MC, Gil C, Botella C, González-Navajas JM, et al. Identification of Leukemia-Associated Immunophenotypes by Databaseguided Flow Cytometry Provides a Highly Sensitive and Reproducible Strategy for the Study of Measurable Residual Disease in Acute Myeloblastic Leukemia. Cancers. 2022; 14(16):4010. https://doi.org/10.3390/cancers14164010
Chicago/Turabian StylePiñero, Paula, Marina Morillas, Natalia Gutierrez, Eva Barragán, Esperanza Such, Joaquin Breña, María C. García-Hernández, Cristina Gil, Carmen Botella, José M. González-Navajas, and et al. 2022. "Identification of Leukemia-Associated Immunophenotypes by Databaseguided Flow Cytometry Provides a Highly Sensitive and Reproducible Strategy for the Study of Measurable Residual Disease in Acute Myeloblastic Leukemia" Cancers 14, no. 16: 4010. https://doi.org/10.3390/cancers14164010