
Does the Presence of Circulating Tumor Cells in High-Risk Early Breast Cancer Patients Predict the Site of First Metastasis—Results from the Adjuvant SUCCESS A Trial

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Patients
2.3. CTC Detection
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. CTC Status before and after Chemotherapy
3.3. Localisation of First Metastatic Disease
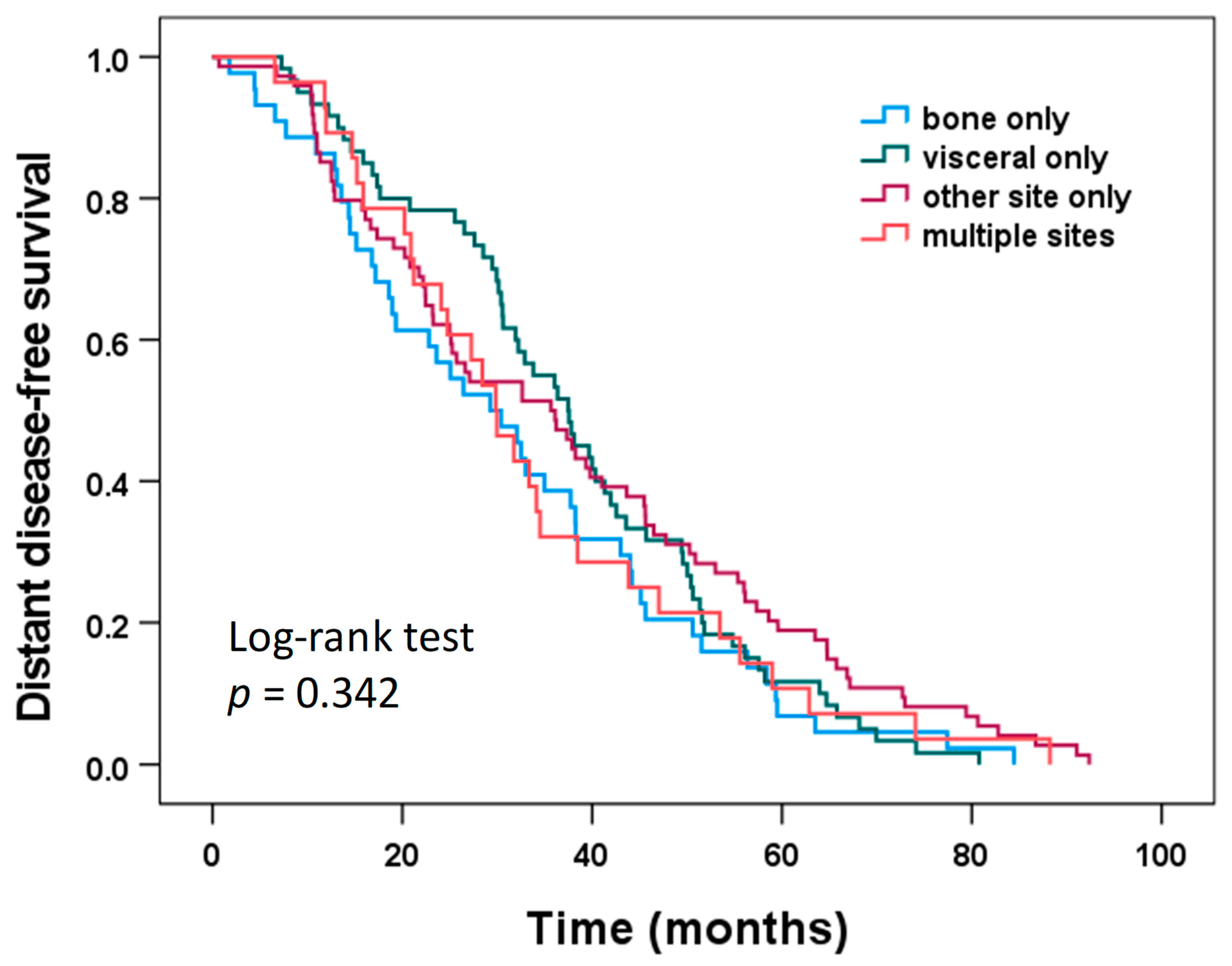
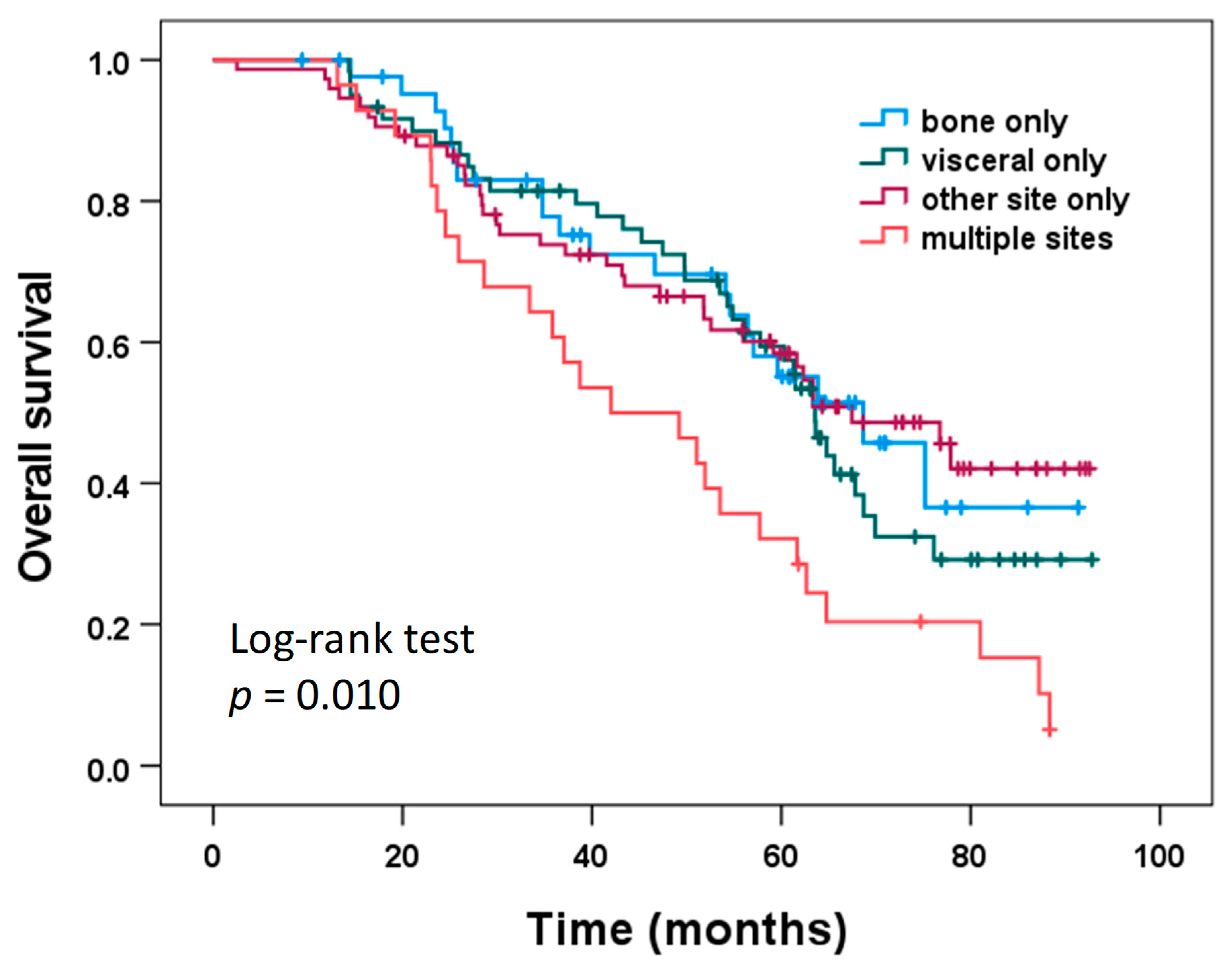
3.4. Distant Disease-Free Survival (DDFS) and Overall Survival (OS) According to Site of First Metastatic Disease
3.5. CTC Status and Metastatic Site
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Cobain, E.; Paoletti, C.; Smerage, J.; Hayes, D. Clinical Applications of Circulating Tumor Cells in Breast Cancer. Tumor Liq. Biopsies 2020, 215, 147–160. [Google Scholar] [CrossRef]
- Pauken, C.M.; Kenney, S.R.; Brayer, K.J.; Guo, Y.; Brown-Glaberman, U.A.; Marchetti, D. Heterogeneity of Circulating Tumor Cell Neoplastic Subpopulations Outlined by Single-Cell Transcriptomics. Cancers 2021, 13, 4885. [Google Scholar] [CrossRef]
- Dujon, A.; Capp, J.-P.; Brown, J.; Pujol, P.; Gatenby, R.; Ujvari, B.; Alix-Panabières, C.; Thomas, F. Is There One Key Step in the Metastatic Cascade? Cancers 2021, 13, 3693. [Google Scholar] [CrossRef]
- Balcik-Ercin, P.; Cayrefourcq, L.; Soundararajan, R.; Mani, S.A.; Alix-Panabières, C. Epithelial-to-Mesenchymal Plasticity in Circulating Tumor Cell Lines Sequentially Derived from a Patient with Colorectal Cancer. Cancers 2021, 13, 5408. [Google Scholar] [CrossRef] [PubMed]
- Banys-Paluchowski, M.; Reinhardt, F.; Fehm, T. Disseminated Tumor Cells and Dormancy in Breast Cancer Progression. Adv. Exp. Med. Biol. 2020, 1220, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Hofbauer, L.; Bozec, A.; Rauner, M.; Jakob, F.; Perner, S.; Pantel, K. Novel approaches to target the microenvironment of bone metastasis. Nat. Rev. Clin. Oncol. 2021, 18, 488–505. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.M.M.; et al. Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef]
- Janni, W.J.; Rack, B.; Terstappen, L.W.M.M.; Pierga, J.-Y.; Taran, F.-A.; Fehm, T.; Hall, C.; de Groot, M.R.; Bidard, F.-C.; Friedl, T.W.P.; et al. Pooled Analysis of the Prognostic Relevance of Circulating Tumor Cells in Primary Breast Cancer. Clin. Cancer Res. 2016, 22, 2583–2593. [Google Scholar] [CrossRef]
- Rack, B.; Schindlbeck, C.; Jückstock, J.; Andergassen, U.; Hepp, P.; Zwingers, T.; Friedl, T.W.P.; Lorenz, R.; Tesch, H.; Fasching, P.A.; et al. Circulating Tumor Cells Predict Survival in Early Average-to-High Risk Breast Cancer Patients. JNCI J. Natl. Cancer Inst. 2014, 106, dju066. [Google Scholar] [CrossRef]
- Sparano, J.; O’Neill, A.; Alpaugh, K.; Wolff, A.C.; Northfelt, D.W.; Dang, C.T.; Sledge, G.W.; Miller, K.D. Association of Circulating Tumor Cells With Late Recurrence of Estrogen Receptor–Positive Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2018, 4, 1700. [Google Scholar] [CrossRef] [PubMed]
- Trapp, E.; Janni, W.; Schindlbeck, C.; Jückstock, J.; Andergassen, U.; de Gregorio, A.; Alunni-Fabbroni, M.; Tzschaschel, M.; Polasik, A.; Koch, J.G.; et al. Presence of Circulating Tumor Cells in High-Risk Early Breast Cancer During Follow-Up and Prognosis. JNCI J. Natl. Cancer Inst. 2019, 111, 380–387. [Google Scholar] [CrossRef]
- Puvanesarajah, S.; Gapstur, S.M.; Patel, A.V.; Sherman, M.E.; Flanders, W.D.; Gansler, T.; Troester, M.A.; Gaudet, M.M. Mode of detection and breast cancer mortality by follow-up time and tumor characteristics among screened women in Cancer Prevention Study-II. Breast Cancer Res. Treat. 2019, 177, 679–689. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Kennecke, H.; Yerushalmi, R.; Woods, R.; Cheang, M.C.U.; Voduc, D.; Speers, C.H.; Nielsen, T.O.; Gelmon, K. Metastatic Behavior of Breast Cancer Subtypes. J. Clin. Oncol. 2010, 28, 3271–3277. [Google Scholar] [CrossRef] [PubMed]
- Moschetti, I.; Cinquini, M.; Lambertini, M.; Levaggi, A.; Liberati, A. Follow-up strategies for women treated for early breast cancer. Cochrane Database Syst. Rev. 2016, 2016, CD001768. [Google Scholar] [CrossRef] [PubMed]
- Rojas, M.P.; Telaro, E.; Russo, A.; Moschetti, I.; Coe, L.; Fossati, R.; Palli, D.; del Roselli, T.M.; Liberati, A. Follow-up strategies for women treated for early breast cancer. Cochrane Database Syst Rev. 2005, 1, CD001768. [Google Scholar]
- Rojas, M.P.M.; Telaro, E.; Moschetti, I.; Coe, L.; Fossati, R.; Liberati, A.; Rosselli, M.D.T. Follow-up strategies for women treated for early breast cancer. Cochrane Database Syst Rev. 2000, 4, CD001768.pub2. [Google Scholar]
- Rosselli Del Turco, M.; Palli, D.; Cariddi, A.; Ciatto, S.; Pacini, P.; Distante, V. Intensive diagnostic follow-up after treatment of primary breast cancer. A randomized trial. National Research Council Project on Breast Cancer follow-up. JAMA 1994, 271, 1593–1597. [Google Scholar] [CrossRef]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.L.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. J. Clin. Oncol. 2016, 34, 611–635. [Google Scholar] [CrossRef]
- Royce, M.; Osgood, C.; Mulkey, F.; Bloomquist, E.; Pierce, W.; Roy, A.; Kalavar, S.; Ghosh, S.; Philip, R.; Rizvi, F.; et al. FDA Approval Summary: Abemaciclib With Endocrine Therapy for High-Risk Early Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Cortes, J.; Dent, R.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.; Hui, R.; et al. Event-free Survival with Pembrolizumab in Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2022, 386, 556–567. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.; Tutt, J.; Kaufman, B.; Viale, G.; Fumagalli, D.; Rastogi, P.; Gelber, R.; de Azambuja, E.; Fielding, A.; Balmaña, J.; et al. Adjuvant Olaparib for Patients with BRCA1- or BRCA2-Mutated Breast Cancer. N. Engl. J. Med. 2021, 384, 2394–2405. [Google Scholar] [CrossRef] [PubMed]
- Van Mackelenbergh, M.; Seither, F.; Möbus, V.; O’Shaughnessy, J.; Martin, M.; Joensuu, H.; Untch, M.; Nitz, U.; Steger, G.; Miralles, J.; et al. Effects of capecitabine as part of neo-/adjuvant chemotherapy—A meta-analysis of individual breast cancer patient data from 13 randomised trials including 15,993 patients. Eur. J. Cancer 2022, 166, 185–201. [Google Scholar] [CrossRef] [PubMed]
- Von Minckwitz, G.; Huang, C.; Mano, M.; Loibl, S.; Mamounas, E.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Gray, R.J.; Ravdin, P.M.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E.; Dees, E.C.; Goetz, M.P.; et al. Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer. N. Engl. J. Med. 2019, 380, 2395–2405. [Google Scholar] [CrossRef]
- Nitz, U.; Gluz, O.; Graeser, M.; Christgen, M.; Kuemmel, S.; Grischke, E.; Braun, M.; Augustin, D.; Potenberg, J.; Krauss, K.; et al. De-escalated neoadjuvant pertuzumab plus trastuzumab therapy with or without weekly paclitaxel in HER2-positive, hormone receptor-negative, early breast cancer (WSG-ADAPT-HER2+/HR−): Survival outcomes from a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2022, 23, 625–635. [Google Scholar] [CrossRef]
- Kalinsky, K.; Barlow, W.; Gralow, J.; Meric-Bernstam, F.; Albain, K.; Hayes, D.; Lin, N.; Perez, E.; Goldstein, L.; Chia, S.; et al. 21-Gene Assay to Inform Chemotherapy Benefit in Node-Positive Breast Cancer. N. Engl. J. Med. 2021, 385, 2336–2347. [Google Scholar] [CrossRef]
- Ignatiadis, M.; Litière, S.; Rothe, F.; Riethdorf, S.; Proudhon, C.; Fehm, T.; Aalders, K.; Forstbauer, H.; Fasching, P.; Brain, E.; et al. Trastuzumab versus observation for HER2 nonamplified early breast cancer with circulating tumor cells (EORTC 90091-10093, BIG 1-12, Treat CTC): A randomized phase II trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2018, 29, 1777–1783. [Google Scholar] [CrossRef]
- Naume, B.; Synnestvedt, M.; Falk, R.; Wiedswang, G.; Weyde, K.; Risberg, T.; Kersten, C.; Mjaaland, I.; Vindi, L.; Sommer, H.; et al. Clinical outcome with correlation to disseminated tumor cell (DTC) status after DTC-guided secondary adjuvant treatment with docetaxel in early breast cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3848–3857. [Google Scholar] [CrossRef]
- Neelima, V.; Sally, G.; Laura, P.; Jimmy, H.; Michelle, M.; Goga, A.; Moasser, M.; Magbanua, M.; Park, J.W.; Rugo, H.S. Evaluation of disseminated tumor cells and circulating tumor cells in patients with breast cancer receiving adjuvant zoledronic acid. NPJ Breast Cancer 2021, 7, 113. [Google Scholar] [CrossRef]
- Smerage, J.; Barlow, W.; Hortobagyi, G.; Winer, E.; Srkalovic, G.; Tejwani, S.; Schott, A.; O’Rourke, M.; Lew, D.; Doyle, G.; et al. Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 3483–3489. [Google Scholar] [CrossRef] [PubMed]
- De Gregorio, A.; Häberle, L.; Fasching, P.; Müller, V.; Schrader, I.; Lorenz, R.; Forstbauer, H.; Friedl, T.; Bauer, E.; de Gregorio, N.; et al. Gemcitabine as adjuvant chemotherapy in patients with high-risk early breast cancer-results from the randomized phase III SUCCESS-A trial. Breast Cancer Res. BCR 2020, 22, 111. [Google Scholar] [CrossRef] [PubMed]
- Friedl, T.; Fehm, T.; Müller, V.; Lichtenegger, W.; Blohmer, J.; Lorenz, R.; Forstbauer, H.; Fink, V.; Bekes, I.; Huober, J.; et al. Prognosis of Patients with Early Breast Cancer Receiving 5 Years vs 2 Years of Adjuvant Bisphosphonate Treatment: A Phase 3 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 1149. [Google Scholar] [CrossRef] [PubMed]
- Singletary, S.E.; Allred, C.; Ashley, P.; Bassett, L.W.; Berry, D.; Bland, K.I.; Borgen, P.I.; Clark, G.; Edge, S.B.; Hayes, D.F.; et al. Revision of the American Joint Committee on Cancer Staging System for Breast Cancer. J. Clin. Oncol. 2002, 20, 3628–3636. [Google Scholar] [CrossRef] [PubMed]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 2002, 41, 154–161. [Google Scholar] [CrossRef]
- Riethdorf, S.; Fritsche, H.; Müller, V.; Rau, T.; Schindlbeck, C.; Rack, B.; Janni, W.; Coith, C.; Beck, K.; Jänicke, F.; et al. Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: A validation study of the CellSearch system. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2007, 13, 920–928. [Google Scholar] [CrossRef]
- Trapp, E.K.; Majunke, L.; Zill, B.; Sommer, H.; Andergassen, U.; Koch, J.; Harbeck, N.; Mahner, S.; Friedl, T.W.P.; Janni, W.; et al. LKB1 pro-oncogenic activity triggers cell survival in circulating tumor cells. Mol. Oncol. 2017, 11, 1508–1526. [Google Scholar] [CrossRef]
- Janni, W.; Vogl, F.; Wiedswang, G.; Synnestvedt, M.; Fehm, T.; Jückstock, J.; Borgen, E.; Rack, B.; Braun, S.; Sommer, H.; et al. Persistence of disseminated tumor cells in the bone marrow of breast cancer patients predicts increased risk for relapse—A European pooled analysis. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2011, 17, 2967–2976. [Google Scholar] [CrossRef]
- Salvador, F.; Llorente, A.; Gomis, R.R. From latency to overt bone metastasis in breast cancer: Potential for treatment and prevention. J. Pathol. 2019, 249, 6–18. [Google Scholar] [CrossRef]
- Coleman, R. Clinical benefits of bone targeted agents in early breast cancer. Breast 2019, 48, S92–S96. [Google Scholar] [CrossRef]
- Gralow, J.; Barlow, W.; Paterson, A.; M’iao, J.; Lew, D.; Stopeck, A.; Hayes, D.; Hershman, D.; Schubert, M.; Clemons, M.; et al. Phase III Randomized Trial of Bisphosphonates as Adjuvant Therapy in Breast Cancer: S0307. J. Natl. Cancer Inst. 2020, 112, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Banys, M.; Solomayer, E.-F.; Gebauer, G.; Janni, W.; Krawczyk, N.; Lueck, H.-J.; Becker, S.; Huober, J.; Kraemer, B.; Wackwitz, B.; et al. Influence of zoledronic acid on disseminated tumor cells in bone marrow and survival: Results of a prospective clinical trial. BMC Cancer 2013, 13, 480. [Google Scholar] [CrossRef] [PubMed]
- Kasimir-Bauer, S.; Reiter, K.; Aktas, B.; Bittner, A.; Weber, S.; Keller, T.; Kimmig, R.; Hoffmann, O. Different prognostic value of circulating and disseminated tumor cells in primary breast cancer: Influence of bisphosphonate intake? Sci. Rep. 2016, 6, 26355. [Google Scholar] [CrossRef]
- Dasgupta, A.; Lim, A.R.; Ghajar, C.M. Circulating and disseminated tumor cells: Harbingers or initiators of metastasis? Mol. Oncol. 2017, 11, 40–61. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, E.; Haque, I.S.; Roberts, C.E.S.; Speicher, M.R. Current and future perspectives of liquid biopsies in genomics-driven oncology. Nat. Rev. Genet. 2019, 20, 71–88. [Google Scholar] [CrossRef]
- Baccelli, I.; Schneeweiss, A.; Riethdorf, S.; Stenzinger, A.; Schillert, A.; Vogel, V.; Klein, C.; Saini, M.; Bäuerle, T.; Wallwiener, M.; et al. Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat. Biotechnol. 2013, 31, 539–544. [Google Scholar] [CrossRef]
- Khatcheressian, J.L.; Hurley, P.; Bantug, E.; Esserman, L.J.; Grunfeld, E.; Halberg, F.; Hantel, A.; Henry, N.L.; Muss, H.B.; Smith, T.J.; et al. Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2013, 31, 961–965. [Google Scholar] [CrossRef]
- Runowicz, C.D.; Leach, C.R.; Henry, N.L.; Henry, K.S.; Mackey, H.T.; Cowens-Alvarado, R.L.; Cannady, R.S.; Pratt-Chapman, M.L.; Edge, S.B.; Jacobs, L.A.; et al. American Cancer Society/American Society of Clinical Oncology Breast Cancer Survivorship Care Guideline. J. Clin. Oncol. 2015, 66, 43–73. [Google Scholar]
- Alix-Panabières, C.; Pantel, K. Liquid Biopsy: From Discovery to Clinical Application. Cancer Discov. 2021, 11, 858–873. [Google Scholar] [CrossRef]
- Müller, V.; Banys-Paluchowski, M.; Friedl, T.; Fasching, P.; Schneeweiss, A.; Hartkopf, A.; Wallwiener, D.; Rack, B.; Meier-Stiegen, F.; Huober, J.; et al. Prognostic relevance of the HER2 status of circulating tumor cells in metastatic breast cancer patients screened for participation in the DETECT study program. ESMO Open 2021, 6, 100299. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.; Prat, A.; Chae, Y.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Tibbe, A.G.; Miller, M.C.; Terstappen, L.W. Statistical considerations for enumeration of circulating tumor cells. Cytom. Part. J. Int. Soc. Anal. Cytol. 2007, 71, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Cullinane, C.; Fleming, C.; O’Leary, D.P.; Hassan, F.; Kelly, L.; Mj, O.; Ma, C.; Hp, R. Association of Circulating Tumor DNA With Disease-Free Survival in Breast Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e2026921. [Google Scholar] [CrossRef]
- Zhou, Q.; Gampenrieder, S.P.; Frantal, S.; Rinnerthaler, G.; Singer, C.F.; Egle, D.; Pfeiler, G.; Bartsch, R.; Wette, V.; Pichler, A.; et al. Persistence of ctDNA in Patients with Breast Cancer During Neoadjuvant Treatment Is a Significant Predictor of Poor Tumor Response. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2022, 28, 697–707. [Google Scholar] [CrossRef]
- Burstein, H.J.; Somerfield, M.R.; Barton, D.L.; Dorris, A.; Fallowfield, L.J.; Jain, D.; Johnston, S.; Korde, L.; Litton, J.; Macrae, E.; et al. Endocrine Treatment and Targeted Therapy for Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor 2-Negative Metastatic Breast Cancer: ASCO Guideline Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 3959–3977. [Google Scholar] [CrossRef]
- Suppan, C.; Graf, R.; Jahn, S.; Zhou, Q.; Klocker, E.V.; Bartsch, R.; Terbuch, A.; Kashofer, K.; Regitnig, P.; Lindenmann, J.; et al. Sensitive and robust liquid biopsy-based detection of PIK3CA mutations in hormone-receptor-positive metastatic breast cancer patients. Br. J. Cancer 2022, 126, 456–463. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CTC Assessment at Baseline | |||
|---|---|---|---|
| Variable | Yes n = 206 | No n = 167 | p-Value 1 |
| Age (years) | 0.279 2 | ||
| Median | 55 | 54 | |
| Range | 27–75 | 26–86 | |
| Body mass index (kg/m2) | 0.420 2 | ||
| Median | 26.2 | 25.9 | |
| Range | 18.5–47.0 | 16.7–44.9 | |
| Tumor stage | 0.463 3 | ||
| pT1 | 57 (27.7%) | 49 (29.3%) | |
| pT2 | 121 (58.7%) | 100 (59.9%) | |
| pT3 | 20 (9.7%) | 13 (7.8%) | |
| pT4 | 8 (3.9%) | 5 (3.0%) | |
| Nodal stage | 0.693 3 | ||
| pN0 | 44 (21.4%) | 36 (21.6%) | |
| pN1 | 79 (38.3%) | 60 (35.9%) | |
| pN2 | 42 (20.4%) | 34 (20.4%) | |
| pN3 | 41 (19.9%) | 37 (22.2%) | |
| Histological grading | 0.042 3 | ||
| G1 | 3 (1.5%) | 3 (1.8%) | |
| G2 | 71 (34.5%) | 75 (44.9%) | |
| G3 | 132 (64.1%) | 89 (53.3%) | |
| Histological type | 0.411 4 | ||
| ductal | 166 (80.6%) | 141 (84.4%) | |
| lobular | 29 (14.1%) | 16 (9.6%) | |
| other | 11 (5.3%) | 10 (6.0%) | |
| Hormone receptor status | 0.112 4 | ||
| negative | 83 (40.3%) | 81 (48.5%) | |
| positive | 123 (59.7%) | 86 (51.5%) | |
| HER2 status | 0.332 4 | ||
| negative | 158 (76.7%) | 122 (73.1%) | |
| positive | 45 (21.8%) | 44 (26.3%) | |
| unknown | 3 (1.5%) | 1 (0.6%) | |
| Menopausal status | 0.497 4 | ||
| premenopausal | 78 (37.9%) | 69 (41.3%) | |
| postmenopausal | 128 (62.1%) | 98 (58.7%) | |
| Type of surgery | 0.678 4 | ||
| breast conserving | 114 (55.3%) | 96 (57.5%) | |
| mastectomy | 92 (44.7%) | 71 (42.5%) | |
| Adjuvant chemotherapy arm 5 | 0.724 4 | ||
| FEC-DocG | 100 (48.5%) | 78 (46.7%) | |
| FEC-Doc | 106 (51.5%) | 89 (53.3%) | |
| Zoledronate treatment arm | 0.217 4 | ||
| 5 years | 107 (51.9%) | 76 (45.5%) | |
| 2 years | 99 (48.1%) | 91 (54.5%) | |
| Radiotherapy | 0.600 4 | ||
| no | 20 (9.7%) | 19 (11.4%) | |
| yes | 186 (90.3%) | 148 (88.6%) | |
| Endocrine therapy | 0.2214 | ||
| no | 70 (34.0%) | 67 (40.1%) | |
| yes | 136 (66.0%) | 100 (59.9%) | |
| HER2-targeted therapy | 0.490 4 | ||
| no | 164 (79.6%) | 128 (76.6%) | |
| yes | 42 (20.4%) | 39 (23.4%) | |
| Site of first metastatic disease | 0.260 4 | ||
| Bone only | 44 (21.4% | 33 (19.8%) | |
| Visceral only | 60 (29.1%) | 37 (22.2%) | |
| Single other site only | 74 (35.9%) | 76 (45.5%) | |
| Multiple sites | 28 (13.6%) | 21 (12.6%) | |
| Location of First Distant Recurrence | CTC Status at Baseline (n = 206) | CTC Status at Baseline (n = 159) | CTC Status after Chemotherapy (n = 159) | |||
|---|---|---|---|---|---|---|
| CTC Negative (n = 136) | CTC Positive (n = 70) | CTC Negative (n = 107) | CTC Positive (n = 52) | CTC Negative (n = 115) | CTC Positive (n = 44) | |
| Bone only | 26 (19.1%) | 18 (25.7%) | 24 (22.4%) | 12 (23.1%) | 23 (20.0%) | 13 (29.5%) |
| Visceral only | 45 (33.1%) | 15 (21.4%) | 36 (33.6%) | 12 (23.1%) | 37 (32.2%) | 11 (25.0%) |
| Other site only | 51 (37.5%) | 23 (32.9%) | 37 (34.6%) | 15 (28.8%) | 41 (35.7%) | 11 (25.0%) |
| Multiple sites | 14 (10.3%) | 14 (20.0%) | 10 (9.3%) | 13 (25.0) | 14 (12.2%) | 9 (20.5%) |
| Location of First Distant Recurrence | CTC Change Group (n = 159) | |||
|---|---|---|---|---|
| neg/neg (n = 79) | neg/pos (n = 28) | pos/neg (n = 36) | pos/pos (n = 16) | |
| Bone only | 17 (21.5%) | 7 (25.0%) | 6 (16.7%) | 6 (37.5%) |
| Visceral only | 29 (36.7%) | 7 (25.0%) | 8 (22.2%) | 4 (25.0%) |
| Other site only | 27 (34.2%) | 10 (35.7%) | 14 (38.9%) | 1 (6.3%) |
| Multiple sites | 6 (7.6%) | 4 (14.3%) | 8 (22.2%) | 5 (31.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trapp, E.K.; Fasching, P.A.; Fehm, T.; Schneeweiss, A.; Mueller, V.; Harbeck, N.; Lorenz, R.; Schumacher, C.; Heinrich, G.; Schochter, F.; et al. Does the Presence of Circulating Tumor Cells in High-Risk Early Breast Cancer Patients Predict the Site of First Metastasis—Results from the Adjuvant SUCCESS A Trial. Cancers 2022, 14, 3949. https://doi.org/10.3390/cancers14163949
Trapp EK, Fasching PA, Fehm T, Schneeweiss A, Mueller V, Harbeck N, Lorenz R, Schumacher C, Heinrich G, Schochter F, et al. Does the Presence of Circulating Tumor Cells in High-Risk Early Breast Cancer Patients Predict the Site of First Metastasis—Results from the Adjuvant SUCCESS A Trial. Cancers. 2022; 14(16):3949. https://doi.org/10.3390/cancers14163949
Chicago/Turabian StyleTrapp, Elisabeth K., Peter A. Fasching, Tanja Fehm, Andreas Schneeweiss, Volkmar Mueller, Nadia Harbeck, Ralf Lorenz, Claudia Schumacher, Georg Heinrich, Fabienne Schochter, and et al. 2022. "Does the Presence of Circulating Tumor Cells in High-Risk Early Breast Cancer Patients Predict the Site of First Metastasis—Results from the Adjuvant SUCCESS A Trial" Cancers 14, no. 16: 3949. https://doi.org/10.3390/cancers14163949