
A New Possible Cut-Off of Cytokeratin 19 mRNA Copy Number by OSNA in the Sentinel Node of Breast Cancer Patients to Avoid Unnecessary Axillary Dissection: A 10-Year Experience in a Tertiary Breast Unit


 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Intraoperative SLN Analysis with OSNA Assay
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fisher, B.; Bauer, M.; Wickerham, D.L.; Redmond, C.K.; Fisher, E.R.; Cruz, A.B.; Foster, R.; Gardner, B.; Lerner, H.; Margolese, R.; et al. Relation of number of positive axillary nodes to the prognosis of patients with primary breast cancer. An NSABP update. Cancer 1983, 52, 1551–1557. [Google Scholar] [CrossRef]
- Veronesi, U.; Paganelli, G.; Viale, G.; Luini, A.; Zurrida, S.; Galimberti, V.; Intra, M.; Veronesi, P.; Maisonneuve, P.; Gatti, G.; et al. Sentinel-lymph-node biopsy as a staging procedure in breast cancer: Update of a randomised controlled study. Lancet Oncol. 2006, 7, 983–990. [Google Scholar] [CrossRef]
- Lyman, G.H.; Giuliano, A.E.; Somerfield, M.R.; Benson, A.B., 3rd; Bodurka, D.C.; Burstein, H.J.; Cochran, A.J.; Cody, H.S., 3rd; Edge, S.B.; Galper, S.; et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J. Clin. Oncol. 2005, 23, 7703–7720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osako, T.; Iwase, T.; Kimura, K.; Yamashita, K.; Horii, R.; Yanagisawa, A.; Akiyama, F. Intraoperative molecular assay for sentinel lymph node metastases in early stage breast cancer: A comparative analysis between one-step nucleic acid amplification whole node assay and routine frozen section histology. Cancer 2011, 117, 4365–4374. [Google Scholar] [CrossRef]
- Layfield, D.M.; Agrawal, A.; Roche, H.; Cutress, R.I. Intraoperative assessment of sentinel lymph nodes in breast cancer. Br. J. Surg. 2011, 98, 4–17. [Google Scholar] [CrossRef]
- Tsujimoto, M.; Nakabayashi, K.; Yoshidome, K.; Kaneko, T.; Iwase, T.; Akiyama, F.; Kato, Y.; Tsuda, H.; Ueda, S.; Sato, K.; et al. One-step nucleic acid amplification for intraoperative detection of lymph node metastasis in breast cancer patients. Clin. Cancer Res. 2007, 13, 4807–4816. [Google Scholar] [CrossRef] [Green Version]
- Chu, P.G.; Weiss, L.M. Keratin expression in human tissues and neoplasms. Histopathology 2002, 40, 403–439. [Google Scholar] [CrossRef]
- Giuliano, A.E.; Ballman, K.V.; McCall, L.; Beitsch, P.D.; Brennan, M.B.; Kelemen, P.R.; Ollila, D.W.; Hansen, N.M.; Whitworth, P.W.; Blumencranz, P.W.; et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 2017, 318, 918–926. [Google Scholar] [CrossRef]
- Zhu, L.; Jin, L.; Li, S.; Chen, K.; Jia, W.; Shan, Q.; Walter, S.; Song, E.; Su, F. Which nomogram is best for predicting non-sentinel lymph node metastasis in breast cancer patients? A meta-analysis. Breast Cancer Res. Treat. 2013, 137, 783–795. [Google Scholar] [CrossRef]
- Meretoja, T.J.; Audisio, R.A.; Heikkila, P.S.; Bori, R.; Sejben, I.; Regitnig, P.; Luschin-Ebengreuth, G.; Zgajnar, J.; Perhavec, A.; Gazic, B.; et al. International multicenter tool to predict the risk of four or more tumor-positive axillary lymph nodes in breast cancer patients with sentinel node macrometastases. Breast Cancer Res. Treat. 2013, 138, 817–827. [Google Scholar] [CrossRef]
- Terrenato, I.; D’Alicandro, V.; Casini, B.; Perracchio, L.; Rollo, F.; De Salvo, L.; di Filippo, S.; di Filippo, F.; Pescarmona, E.; Maugeri-Saccà, M.; et al. A cut-off of 2150 cytokeratin 19 mRNA copy number in sentinel lymph node may be a powerful predictor of non-sentinel lymph node status in breast cancer patients. PLoS ONE 2017, 12, e0171517. [Google Scholar] [CrossRef] [PubMed]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J. Clin. Oncol. 2020, 38, 1346–1366. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.J.; Panel members. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Brenton, J.D.; Carey, L.A.; Ahmed, A.A.; Caldas, C. Molecular classification and molecular forecasting of breast cancer: Ready for clinical application? J. Clin. Oncol. 2005, 23, 7350–7360. [Google Scholar] [CrossRef] [Green Version]
- Tan, P.H.; Ellis, I.; Allison, K.; Brogi, E.; Fox, S.B.; Lakhani, S.; Lazar, A.J.; Morris, E.A.; Sahin, A.; Salgado, R.; et al. The 2019 World Health Organization classification of tumours of the breast. Histopathology 2020, 77, 181–185. [Google Scholar] [CrossRef]
- Galimberti, V.; Cole, B.F.; Viale, G.; Veronesi, P.; Vicini, E.; Intra, M.; Mazzarol, G.; Massarut, S.; Zgajnar, J.; Taffurelli, M.; et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): A phase 3 randomised controlled trial. Lancet Oncol. 2013, 14, 297–305. [Google Scholar] [CrossRef] [Green Version]
- Galimberti, V.; Cole, B.F.; Viale, G.; Veronesi, P.; Vicini, E.; Intra, M.; Mazzarol, G.; Massarut, S.; Zgajnar, J.; Taffurelli, M.; et al. Axillary dissection versus no axillary dissection in patients with breast cancer and sentinel-node micrometastases (IBCSG 23-01): 10-year follow-up of a randomised, controlled phase 3 trial. Lancet Oncol. 2018, 19, 1385–1393. [Google Scholar] [CrossRef]
- Cserni, G. Intraoperative analysis of sentinel lymph nodes in breast cancer by one-step nucleic acid amplification. J. Clin. Pathol. 2012, 65, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Donker, M.; van Tienhoven, G.; Straver, M.E.; Meijnen, P.; van de Velde, C.J.; Mansel, R.E.; Cataliotti, L.; Westenberg, A.H.; Klinkenbijl, J.H.G.; Orzalesi, L.; et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): A randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014, 15, 1303–1310. [Google Scholar] [CrossRef] [Green Version]
- Mansel, R.E.; Fallowfield, L.; Kissin, M.; Goyal, A.; Newcombe, R.G.; Dixon, J.M.; Yiangou, C.; Horgan, K.; Bundred, N.; Monypenny, I.; et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: The ALMANAC Trial. J. Natl. Cancer Inst. 2006, 98, 599–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.J.; Yu, Y.; Hou, X.W.; Chi, J.R.; Ge, J.; Wang, X.; Cao, X.C. The prognostic value of node status in different breast cancer subtypes. Oncotarget 2017, 8, 4563–4571. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Yang, Z.; Liu, X.; Niu, Y. Lymph node status in different molecular subtype of breast cancer: Triple negative tumours are more likely lymph node negative. Oncotarget 2017, 8, 55534–55543. [Google Scholar] [CrossRef] [Green Version]
- Wang, N.N.; Yang, Z.J.; Wang, X.; Chen, L.X.; Zhao, H.M.; Cao, W.F.; Zhang, B. A mathematical prediction model incorporating molecular subtype for risk of non-sentinel lymph node metastasis in sentinel lymph node-positive breast cancer patients: A retrospective analysis and nomogram development. Breast Cancer 2018, 25, 629–638. [Google Scholar] [CrossRef]
- Degnim, A.C.; Griffith, K.A.; Sabel, M.S.; Hayes, D.F.; Cimmino, V.M.; Diehl, K.M.; Lucas, P.C.; Snyder, M.L.; Chang, A.E.; Newman, L.A. Clinicopathologic features of metastasis in nonsentinel lymph nodes of breast carcinoma patients. Cancer 2003, 98, 2307–2315. [Google Scholar] [CrossRef] [Green Version]
- He, Z.; Lan, X.; Tan, Y.; Lin, X.; Wen, G.; Wang, X.; Huang, X.; Yang, F. Identification of Risk Factors Associated with Axillary Lymph Node Metastasis for Sentinel Lymph Node-Positive Breast Cancer Patients. J. Oncol. 2020, 2020, 8884337. [Google Scholar] [CrossRef] [PubMed]
- Bader, A.A.; Tio, J.; Petru, E.; Buhner, M.; Pfahlberg, A.; Volkholz, H.; Tulusan, A.H. T1 breast cancer: Identification of patients at low risk of axillary lymph node metastases. Breast Cancer Res. Treat. 2002, 76, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Cserni, G. Axillary sentinel lymph node micrometastases with extracapsular extension: A distinct pattern of breast cancer metastasis? J. Clin. Pathol. 2008, 61, 115–118. [Google Scholar] [CrossRef]
- Deambrogio, C.; Castellano, I.; Paganotti, A.; Zorini, E.O.; Corsi, F.; Bussone, R.; Franchini, R.; Antona, J.; Miglio, U.; Sapino, A.; et al. A new clinical cut-off of cytokeratin 19 mRNA copy number in sentinel lymph node better identifies patients eligible for axillary lymph node dissection in breast cancer. J. Clin. Pathol. 2014, 67, 702–706. [Google Scholar] [CrossRef] [Green Version]
- Pina, H.; Salleron, J.; Gilson, P.; Husson, M.; Rouyer, M.; Leroux, A.; Rauch, P.; Marchal, F.; Käppeli, M.; Merlin, J.L.; et al. Intraoperative prediction of non-sentinel lymph node metastases in breast cancer using cytokeratin 19 mRNA copy number: A retrospective analysis. Mol. Clin. Oncol. 2022, 16, 58. [Google Scholar] [CrossRef]
- Heilmann, T.; Mathiak, M.; Hofmann, J.; Mundhenke, C.; van Mackelenbergh, M.; Alkatout, I.; Wenners, A.; Eckmann-Scholz, C.; Schem, C. Intra-operative use of one-step nucleic acid amplification (OSNA) for detection of the tumor load of sentinel lymph nodes in breast cancer patients. J. Cancer Res. Clin. Oncol. 2013, 139, 1649–1655. [Google Scholar] [CrossRef] [PubMed]
- Peg, V.; Espinosa-Bravo, M.; Vieites, B.; Vilardell, F.; Antunez, J.R.; de Salas, M.S.; Delgado-Sánchez, J.J.; Pinto, W.; Gozalbo, F.; Petit, A.; et al. Intraoperative molecular analysis of total tumor load in sentinel lymph node: A new predictor of axillary status in early breast cancer patients. Breast Cancer Res. Treat. 2013, 139, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Nabais, C.; Figueiredo, J.; Lopes, P.; Martins, M.; Araujo, A. Total tumor load assessed by one-step nucleic acid amplification assay as an intraoperative predictor for non-sentinel lymph node metastasis in breast cancer. Breast 2017, 32, 33–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinosa-Bravo, M.; Sansano, I.; Perez-Hoyos, S.; Ramos, M.; Sancho, M.; Xercavins, J.; Rubio, I.T.; Peg, V. Prediction of non-sentinel lymph node metastasis in early breast cancer by assessing total tumoral load in the sentinel lymph node by molecular assay. Eur. J. Surg. Oncol. 2013, 39, 766–773. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | No ALN+ (n = 86) | ≥1 ALN+ (n = 116) | p-Value |
|---|---|---|---|
| Age | 51 (49–55) | 48 (47–53) | 0.41 |
| BMI (Kg/m2) | 25 (22–27) | 26 (24–28) | 0.33 |
| Surgical treatment | |||
| Conservative | 72 (84%) | 95 (82%) | 0.8 |
| Mastectomy | 14 (16%) | 21 (18%) | 0.8 |
| Histological type | |||
| Invasive Ductal carcinoma | 71 (82.5%) | 88 (75.8%) | 0.32 |
| Invasive Lobular carcinoma | 9 (10.5%) | 19 (16.4%) | 0.31 |
| Invasive Ductal and Lobular carcinoma | 3 (3.5%) | 6 (5.2%) | 0.7 |
| Ductal Carcinoma In Situ | 0 | 2 (1.7%) | 0.5 |
| Other | 3 (3.5%) | 1 (0.9%) | 0.3 |
| Tumor size | |||
| pT1a | 2 (2.3%) | 1 (0.9%) | 0.5 |
| pT1b | 20 (23.3%) | 12 (10.2%) | * <0.05 |
| pT1c | 40 (46.5%) | 37 (32%) | * <0.05 |
| pT2 | 23 (26.7%) | 52 (44.8%) | * <0.05 |
| pT3 | 1 (1.2%) | 14 (12.1%) | * <0.005 |
| Grading | |||
| 1 | 12 (14%) | 5 (4%) | * <0.05 |
| 2 | 45 (52%) | 46 (40%) | 0.09 |
| 3 | 29 (34%) | 65 (56%) | * <0.005 |
| Estrogen Receptor status | |||
| Positive | 74 (86%) | 95 (82%) | 0.5 |
| Negative | 12 (14%) | 21 (18%) | 0.5 |
| Progesterone Receptor status | |||
| Positive | 47 (54.6%) | 61 (52.5%) | 0.8 |
| Negative | 39 (45.4%) | 55 (47.5%) | 0.8 |
| HER2 expression by IHC | |||
| Positive | 28 (32.5%) | 37 (32%) | 1 |
| Negative | 58 (67.5%) | 79 (68%) | 1 |
| Ki67% | |||
| <20% | 47 (54.6%) | 68 (58.6%) | 0.6 |
| ≥20% | 39 (45.4%) | 48 (41.4%) | 0.6 |
| Surrogate molecular subtypes | |||
| Luminal A | 30 (35%) | 46 (40%) | 0.5 |
| Luminal B | 47(54.6%) | 56 (48%) | 0.4 |
| HER2 enriched | 5 (5.8%) | 7 (6%) | 1 |
| Triple-negative | 4 (4.6%) | 7 (6%) | 0.7 |
| Characteristics | No ALN+ (n = 86) | ≥1 ALN+ (n = 116) | p-Value |
|---|---|---|---|
| SLN size (main) | 1.5 cm (1.2–2) | 1.5 cm (1.2–1.9) | 0.9 |
| SLN weight | 0.58 gm (0.4–0.9) | 0.6 gm (0.4–0.9) | 0.2 |
| SLN CK19 mRNA copies | 49,500 (range 11,625–179,700) | 89,000 (range 20,000–443,350) | * <0.05 |
| LNs removed at ALND | 19 (17–24) | 21 (17.75–24.25) | 0.3 |
| LNs positive at ALND | 0 | 3 (2–5) | * <0.005 |
| Study | N. of Pts | Cut-Off (Copies/µL) | Years | AUC (%) | Se (%) | Sp (%) | PPV (%) | NPV (%) | Method |
|---|---|---|---|---|---|---|---|---|---|
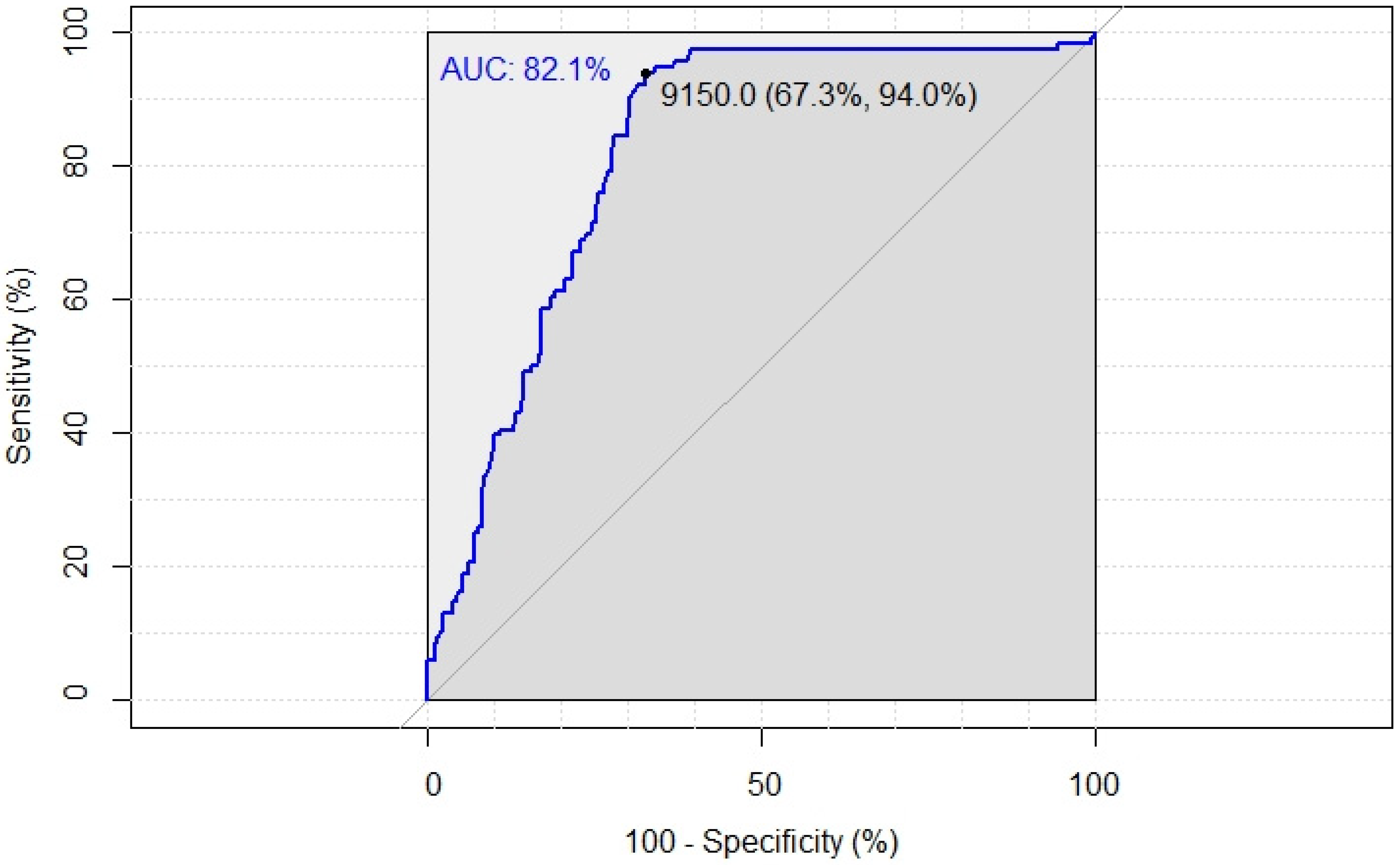
| Present study | 1339 202 ++ 126 + | 9150 | 13 | 82.1 | 94 | 67.3 | 61.2 | 95.3 | Maximalcopy |
| Tsujimoto et al. [6] | 5000 | 78.6 | 56.8 | 44.8 | 85.6 | Maximal copy | |||
| Deambrogio et al. [29] | 1296 117 ++ 123 + | 7700 | 3 | 69 | 78 | 57 | 50 | 83 | |
| Pina et al. [30] | 812 197 ++ | 5000 | 4 | 77 | 75 | 72 | 40.5 | 91.9 | Maximal copy |
| Heilmann et al. [31] | 143 39 ++ | 7900 | 91 | 61 | 1 mm central for histology, rest for OSNA | ||||
| Peg et al.* [32] | 697 ++ | 15,000 | 1 | 70 | 76.7 | 55.2 | 41.1 | 85.5 | TTL |
| Terrenato et al. | 1140 172 ++ 146 + | 2150 | 3 | 76 | 94.9 | 51.4 | 46.5 | 95.8 | TTL |
| Nabais et al. [33] | 598 58 ++ | 190,000 | 4 | 80 | 73.3 | 74.4 | 88.9 | TTL | |
| Espinosa-Bravo et al. * [34] | 306 108 ++ | 120,000 | 1 | 71 | 47 | 85.3 | 56 | 80 | TTL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomasicchio, G.; Mastropasqua, M.G.; Picciariello, A.; Montanaro, A.E.; Signorile, D.; Cirilli, A.; Punzo, C. A New Possible Cut-Off of Cytokeratin 19 mRNA Copy Number by OSNA in the Sentinel Node of Breast Cancer Patients to Avoid Unnecessary Axillary Dissection: A 10-Year Experience in a Tertiary Breast Unit. Cancers 2022, 14, 3384. https://doi.org/10.3390/cancers14143384
Tomasicchio G, Mastropasqua MG, Picciariello A, Montanaro AE, Signorile D, Cirilli A, Punzo C. A New Possible Cut-Off of Cytokeratin 19 mRNA Copy Number by OSNA in the Sentinel Node of Breast Cancer Patients to Avoid Unnecessary Axillary Dissection: A 10-Year Experience in a Tertiary Breast Unit. Cancers. 2022; 14(14):3384. https://doi.org/10.3390/cancers14143384
Chicago/Turabian StyleTomasicchio, Giovanni, Mauro Giuseppe Mastropasqua, Arcangelo Picciariello, Alda Elena Montanaro, Daniela Signorile, Alfredo Cirilli, and Clelia Punzo. 2022. "A New Possible Cut-Off of Cytokeratin 19 mRNA Copy Number by OSNA in the Sentinel Node of Breast Cancer Patients to Avoid Unnecessary Axillary Dissection: A 10-Year Experience in a Tertiary Breast Unit" Cancers 14, no. 14: 3384. https://doi.org/10.3390/cancers14143384