
Durvalumab after Sequential High Dose Chemoradiotherapy versus Standard of Care (SoC) for Stage III NSCLC: A Bi-Centric Retrospective Comparison Focusing on Pulmonary Toxicity

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Chemoradiotherapy
2.3. Immunotherapy
2.4. Follow-Up
2.5. Statistics and Endpoints
3. Results
3.1. Patients
3.2. Treatment
3.2.1. Chemotherapy
3.2.2. Radiotherapy
3.2.3. Immunotherapy
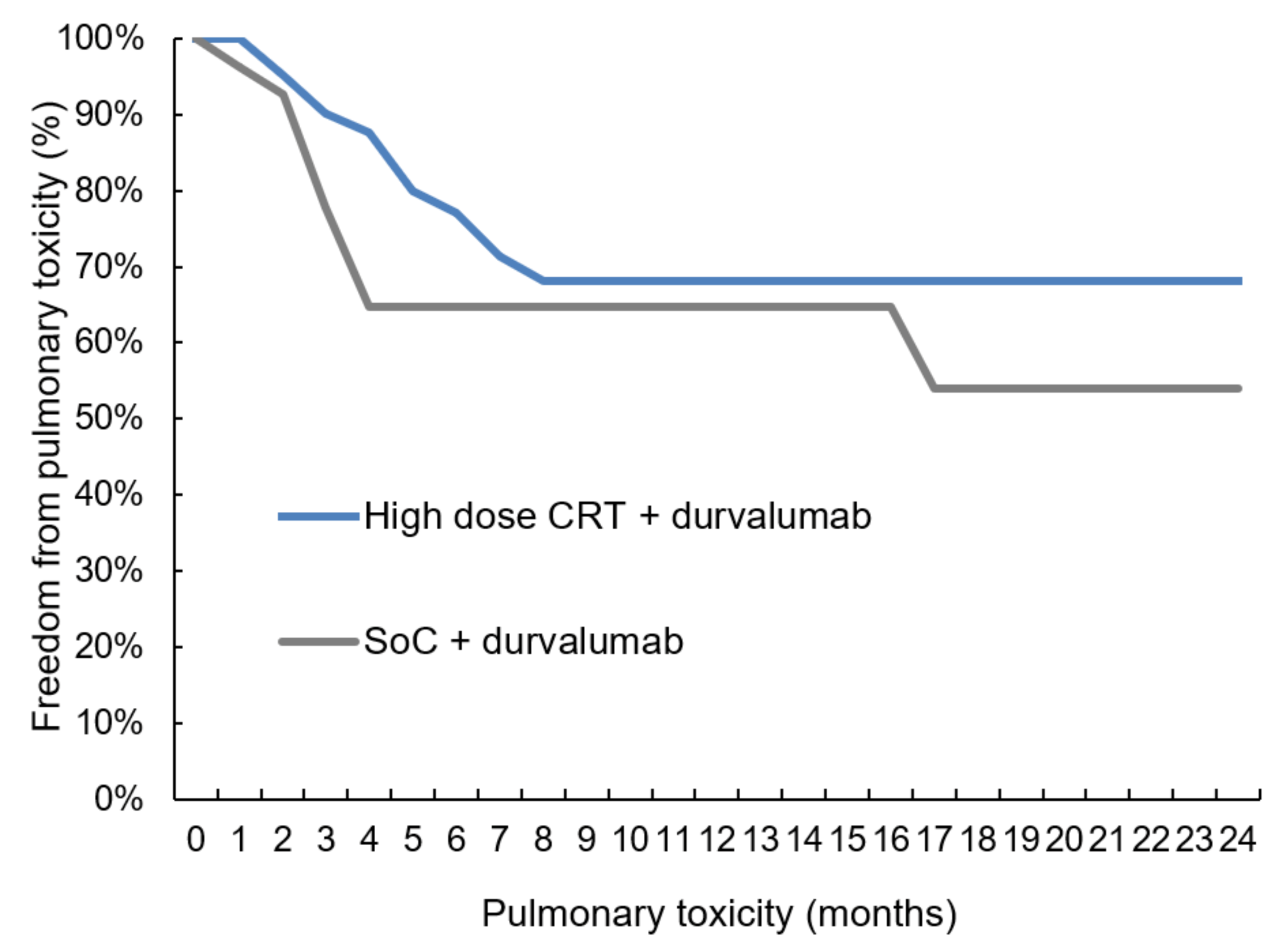
3.3. Toxicity
3.4. Pulmonary Function Changes after High-Dose Chemoradiotherapy
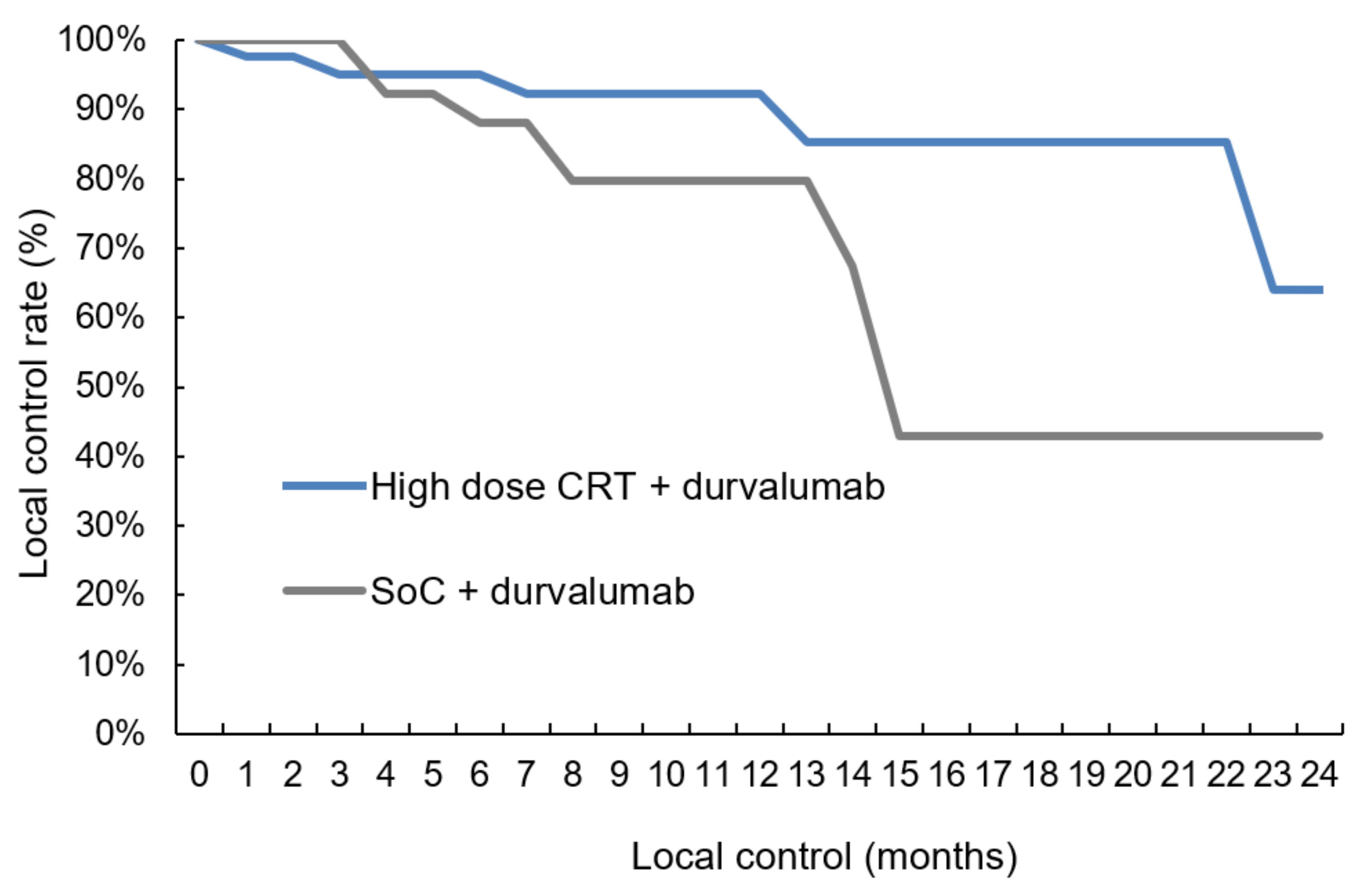
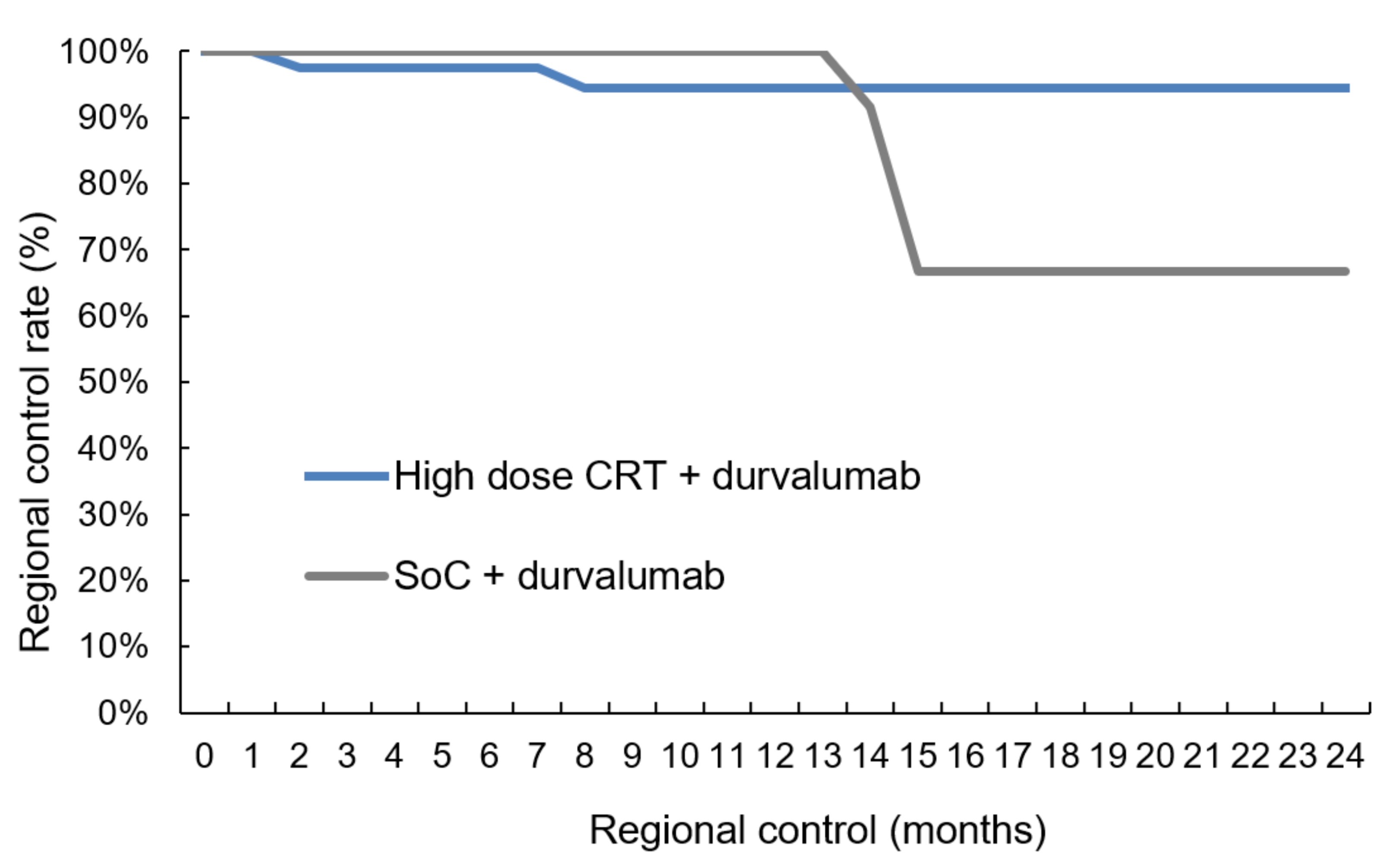
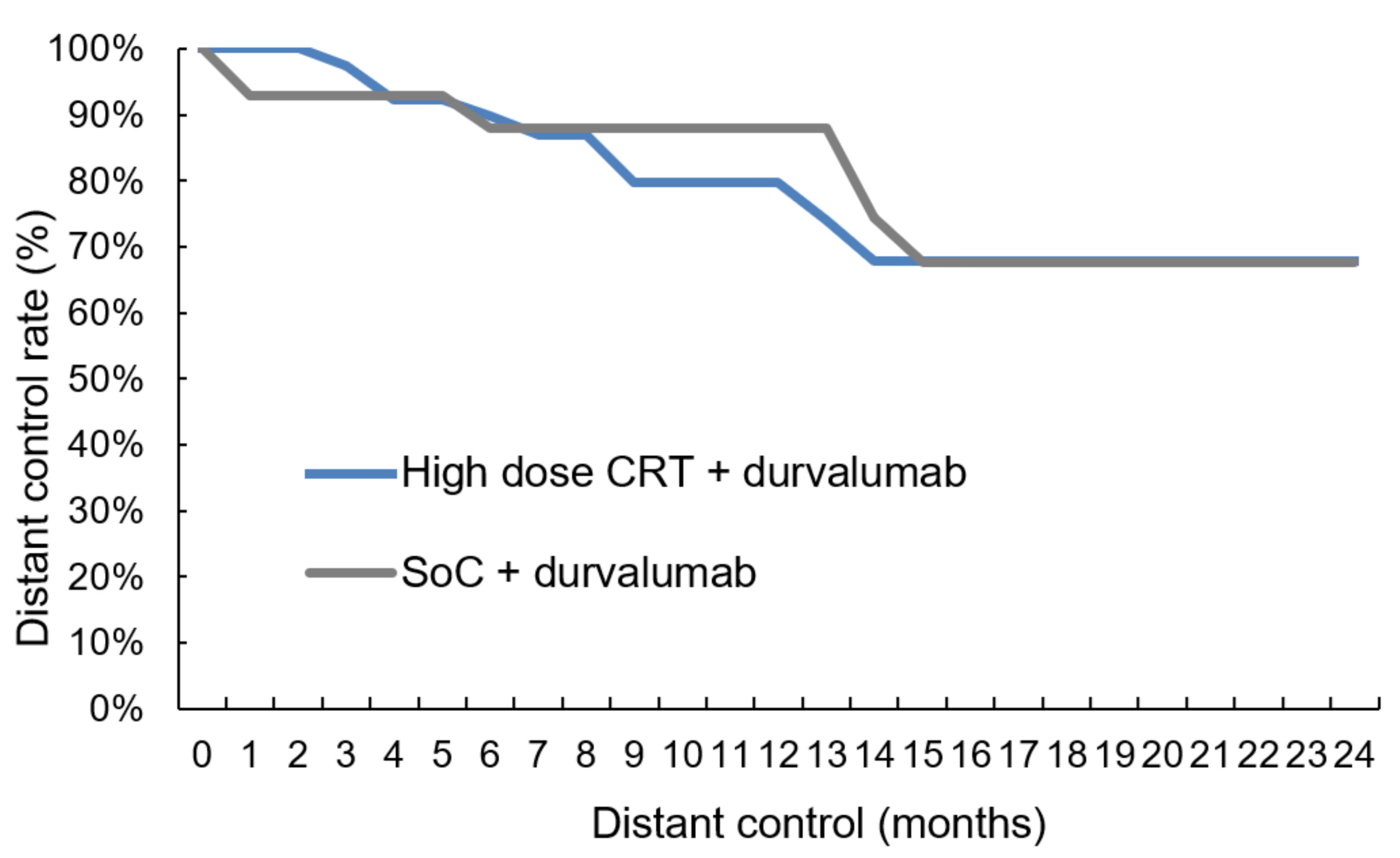
3.5. Local, Regional and Distant Control
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CIP | checkpoint inhibitor pneumonitis |
| CTV | clinical target volume |
| CRT | chemoradiotherapy |
| EBUS-TBNA | endobronchial ultrasound-guided transbronchial needle aspiration |
| EQD2 | biologically equivalent dose in 2 Gy fractions |
| GTV | gross tumor volume |
| ICI | immune-checkpoint inhibitor |
| ILD | interstitial lung disease |
| irAE | immune-related adverse events |
| LC | local control |
| LRC | loco-regional control |
| MLD | mean lung dose |
| NSCLC | non-small cell lung cancer |
| OS | overall survival |
| PD-L1 | programmed death-ligand 1 |
| PFS | progression-free survival |
| PFT | pulmonary function test |
| PTV | planning target volume |
| RC | regional control |
| RT | radiotherapy |
| RWD | real-world data |
| SoC | standard of care |
| VMAT | volumetric arc therapy |
| V20total lung | lung volume that receives 20 Gy or more |
References
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef]
- Malvezzi, M.; Carioli, G.; Bertuccio, P.; Boffetta, P.; Levi, F.; La Vecchia, C.; Negri, E. European cancer mortality predictions for the year 2017, with focus on lung cancer. Ann. Oncol. 2017, 28, 1117–1123. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef]
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Garassino, M.C.; Hui, R.; Quantin, X.; et al. Five-Year Survival Outcomes From the PACIFIC Trial: Durvalumab After Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2022, 40, 1301. [Google Scholar] [CrossRef]
- Auperin, A.; Le Pechoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef]
- Curran, W.J., Jr.; Paulus, R.; Langer, C.J.; Komaki, R.; Lee, J.S.; Hauser, S.; Movsas, B.; Wasserman, T.; Rosenthal, S.A.; Gore, E.; et al. Sequential vs. concurrent chemoradiation for stage III non-small cell lung cancer: Randomized phase III trial RTOG 9410. J. Natl. Cancer Inst. 2011, 103, 1452–1460. [Google Scholar] [CrossRef]
- Zehentmayr, F.; Grambozov, B.; Kaiser, J.; Fastner, G.; Sedlmayer, F. Radiation dose escalation with modified fractionation schedules for locally advanced NSCLC: A systematic review. Thorac. Cancer 2020, 11, 1375–1385. [Google Scholar] [CrossRef]
- Kaster, T.S.; Yaremko, B.; Palma, D.A.; Rodrigues, G.B. Radical-Intent Hypofractionated Radiotherapy for Locally Advanced Non-Small-Cell Lung Cancer: A Systematic Review of the Literature. Clin. Lung Cancer 2015, 16, 71–79. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- Faivre-Finn, C.; Vicente, D.; Kurata, T.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Spigel, D.R.; Garassino, M.C.; Reck, M.; Senan, S.; et al. Durvalumab after chemoradiotherapy in stage III NSCLC: 4-year survival update from the phase III PACIFIC trial. Ann. Oncol. 2020, 31, S1178–S1179. [Google Scholar] [CrossRef]
- Faehling, M.; Schumann, C.; Christopoulos, P.; Hoffknecht, P.; Alt, J.; Horn, M.; Eisenmann, S.; Schlenska-Lange, A.; Aries, S.P.; Sackmann, S.; et al. Durvalumab after definitive radiochemotherapy (RCT) in locally advanced unresectable NSCLC: Real-world data on survival and safety from the German expanded access program (EAP). Ann. Oncol. 2020, 31, S806–S807. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 2.2021 Featured Updates to the NCCN Guidelines. J. Natl. Compr. Cancer Netw. 2021, 19, 254–266. [Google Scholar] [CrossRef]
- Remon, J.; Soria, J.C.; Peters, S.; Comm, E.G. Early and locally advanced non-small-cell lung cancer: An update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy. Ann. Oncol. 2021, 32, 1637–1642. [Google Scholar] [CrossRef] [PubMed]
- Toi, Y.; Sugawara, S.; Kawashima, Y.; Aiba, T.; Kawana, S.; Saito, R.; Tsurumi, K.; Suzuki, K.; Shimizu, H.; Sugisaka, J.; et al. Association of Immune-Related Adverse Events with Clinical Benefit in Patients with Advanced Non-Small-Cell Lung Cancer Treated with Nivolumab. Oncologist 2018, 23, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Akamatsu, H.; Murakami, E.; Sasaki, S.; Kanai, K.; Hayata, A.; Tokudome, N.; Akamatsu, K.; Koh, Y.; Ueda, H.; et al. Correlation between immune-related adverse events and efficacy in non-small cell lung cancer treated with nivolumab. Lung Cancer 2018, 126, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Tone, M.; Izumo, T.; Awano, N.; Kuse, N.; Inomata, M.; Jo, T.; Yoshimura, H.; Minami, J.; Takada, K.; Miyamoto, S.; et al. High mortality and poor treatment efficacy of immune checkpoint inhibitors in patients with severe grade checkpoint inhibitor pneumonitis in non-small cell lung cancer. Thorac. Cancer 2019, 10, 2006–2012. [Google Scholar] [CrossRef]
- Nishino, M.; Giobbie-Hurder, A.; Hatabu, H.; Ramaiya, N.H.; Hodi, S. Incidence of Programmed Cell Death 1 Inhibitor-Related Pneumonitis in Patients With Advanced Cancer A Systematic Review and Meta-analysis. JAMA Oncol. 2016, 2, 1607–1616. [Google Scholar] [CrossRef]
- Fukihara, J.; Sakamoto, K.; Koyama, J.; Ito, T.; Iwano, S.; Morise, M.; Ogawa, M.; Kondoh, Y.; Kimura, T.; Hashimoto, N.; et al. Prognostic Impact and Risk Factors of Immune-Related Pneumonitis in Patients With Non-Small-Cell Lung Cancer Who Received Programmed Death 1 Inhibitors. Clin. Lung Cancer 2019, 20, 442–450.e4. [Google Scholar] [CrossRef]
- Suresh, K.; Voong, K.R.; Shankar, B.; Forde, P.M.; Ettinger, D.S.; Marrone, K.A.; Kelly, R.J.; Hann, C.L.; Levy, B.; Feliciano, J.L.; et al. Pneumonitis in Non-Small Cell Lung Cancer Patients Receiving Immune Checkpoint Immunotherapy: Incidence and Risk Factors. J. Thorac. Oncol. 2018, 13, 1930–1939. [Google Scholar] [CrossRef]
- Cui, P.F.; Liu, Z.F.; Wang, G.Q.; Ma, J.X.; Qian, Y.Y.; Zhang, F.; Han, C.; Long, Y.P.; Li, Y.; Zheng, X.; et al. Risk factors for pneumonitis in patients treated with anti-programmed death-1 therapy: A case-control study. Cancer Med. 2018, 7, 4115–4120. [Google Scholar] [CrossRef]
- Cho, J.Y.; Kim, J.; Lee, J.S.; Kim, Y.J.; Kim, S.H.; Lee, Y.J.; Cho, Y.J.; Yoon, H.I.; Lee, J.H.; Lee, C.T.; et al. Characteristics, incidence, and risk factors of immune checkpoint inhibitor related pneumonitis in patients with non-small cell lung cancer. Lung Cancer 2018, 125, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Shimizu, J.; Hasegawa, T.; Horio, Y.; Inaba, Y.; Yatabe, Y.; Hida, T. Pre-existing pulmonary fibrosis is a risk factor for anti-PD-1-related pneumonitis in patients with non-small cell lung cancer: A retrospective analysis. Lung Cancer 2018, 125, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Oshima, Y.; Tanimoto, T.; Yuji, K.; Tojo, A. EGFR-TKI-Associated Interstitial Pneumonitis in Nivolumab-Treated Patients With Non-Small Cell Lung Cancer. JAMA Oncol. 2018, 4, 1112–1115. [Google Scholar] [CrossRef] [PubMed]
- Lisberg, A.; Cummings, A.; Goldman, J.W.; Bornazyan, K.; Reese, N.; Wang, T.; Coluzzi, P.; Ledezma, B.; Mendenhall, M.; Hunt, J.; et al. A Phase II Study of Pembrolizumab in EGFR-Mutant, PD-L1+, Tyrosine Kinase Inhibitor Naive Patients With Advanced NSCLC. J. Thorac. Oncol. 2018, 13, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Raben, D.; Rimner, A.; Senan, S.; Broadhurst, H.; Pellas, T.; Dennis, P.A.; Faivre-Finn, C. Patterns of Disease Progression with Durvalumab in Stage III Non-small Cell Lung Cancer (PACIFIC). Int. J. Radiat. Oncol. 2019, 105, 683. [Google Scholar] [CrossRef]
- Landman, Y.; Jacobi, O.; Kurman, N.; Yariv, O.; Peretz, I.; Rotem, O.; Dudnik, E.; Zer, A.; Allen, A.M. Durvalumab after concurrent chemotherapy and high-dose radiotherapy for locally advanced non-small cell lung cancer. Oncoimmunology 2021, 10, 1959979. [Google Scholar] [CrossRef]
- Johnson, M.D.; Sura, K.; Mangona, V.S.; Glick, A.; Wallace, M.; Ye, H.; Grills, I.S. Matched-Pair Analysis of High Dose Versus Standard Dose Definitive Chemoradiation for Locally Advanced Non-Small-Cell Lung Cancer. Clin. Lung Cancer 2017, 18, 149–155. [Google Scholar] [CrossRef]
- Wurstbauer, K.; Deutschmann, H.; Dagn, K.; Kopp, P.; Zehentmayr, F.; Lamprecht, B.; Porsch, P.; Wegleitner, B.; Studnicka, M.; Sedlmayer, F. DART-bid (Dose-differentiated accelerated radiation therapy, 1.8 Gy twice daily)—A novel approach for non-resected NSCLC: Final results of a prospective study, correlating radiation dose to tumor volume. Radiat. Oncol. 2013, 8, 49. [Google Scholar] [CrossRef]
- Zehentmayr, F.; Sohn, M.; Exeli, A.K.; Wurstbauer, K.; Troller, A.; Deutschmann, H.; Fastner, G.; Fussl, C.; Steininger, P.; Kranzinger, M.; et al. Normal tissue complication models for clinically relevant acute esophagitis (>/= grade 2) in patients treated with dose differentiated accelerated radiotherapy (DART-bid). Radiat. Oncol. 2015, 10, 121. [Google Scholar] [CrossRef]
- Grambozov, B.; Wolf, F.; Kaiser, J.; Wass, R.; Fastner, G.; Gaisberger, C.; Rettenbacher, L.; Studnicka, M.; Pirich, C.; Sedlmayer, F.; et al. Pulmonary function decreases moderately after accelerated high-dose irradiation for stage III non-small cell lung cancer. Thorac. Cancer 2019, 11, 369–378. [Google Scholar] [CrossRef]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar] [PubMed]
- Wurstbauer, K.; Zehentmayr, F.; Deutschmann, H.; Dagn, K.; Exeli, A.K.; Kopp, P.; Porsch, P.; Maurer, B.; Studnicka, M.; Sedlmayer, F. DART-bid for loco-regionally advanced NSCLC: Summary of acute and late toxicity with long-term follow-up; experiences with pulmonary dose constraints. Strahlenther. Onkol. 2017, 193, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): A randomised, phase 2, open-label trial. Lancet 2019, 393, 2051–2058. [Google Scholar] [CrossRef]
- Rubinstein, L.V.; Korn, E.L.; Freidlin, B.; Hunsberger, S.; Ivy, S.P.; Smith, M.A. Design issues of randomized phase II trials and a proposal for phase II screening trials. J. Clin. Oncol. 2005, 23, 7199–7206. [Google Scholar] [CrossRef]
- Zhao, Q.; Liu, M.; Wang, Z.T.; Huang, W.; Li, X.A.; Zhou, T.; Zhang, J.; Zhang, Z.C.; Wang, Q.; Yu, S.Z.; et al. High dose radiation therapy based on normal tissue constraints with concurrent chemotherapy achieves promising survival of patients with unresectable stage III non-small cell lung cancer. Radiother. Oncol. 2020, 145, 7–12. [Google Scholar] [CrossRef]
- Desilets, A.; Blanc-Durand, F.; Lau, S.; Hakozaki, T.; Kitadai, R.; Malo, J.; Belkaid, W.; Richard, C.; Messaoudene, M.; Cvetkovic, L.; et al. Durvalumab therapy following chemoradiation compared with a historical cohort treated with chemoradiation alone in patients with stage III non-small cell lung cancer: A real-world multicentre study. Eur. J. Cancer 2021, 142, 83–91. [Google Scholar] [CrossRef]
- Girard, N.; Smit, H.J.M.; Sibille, A.; McDonald, F.; Mornex, F.; Garassino, M.C.C.; Filippi, A.R.; Peters, S.; Field, J.K.; Christoph, D.C.; et al. PACIFIC-R real-world study: Treatment duration and interim analysis of progression-free survival in unresectable stage III NSCLC patients treated with durvalumab after chemoradiotherapy. Ann. Oncol. 2021, 32, S939–S940. [Google Scholar] [CrossRef]
- Jung, H.A.; Noh, J.M.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; Ahn, M.J.; Pyo, H.; Ahn, Y.C.; Park, K. Real world data of durvalumab consolidation after chemoradiotherapy in stage III non-small-cell lung cancer. Lung Cancer 2020, 146, 23–29. [Google Scholar] [CrossRef]
- Chu, C.H.; Chiu, T.H.; Wang, C.C.; Chang, W.C.; Huang, A.C.C.; Liu, C.Y.; Wang, C.L.; Ko, H.W.; Chung, F.T.; Hsu, P.C.; et al. Consolidation treatment of durvalumab after chemoradiation in real-world patients with stage III unresectable non-small cell lung cancer. Thorac. Cancer 2020, 11, 1541–1549. [Google Scholar] [CrossRef]
- Garassino, M.C.; Mazieres, J.; Reck, M.; Chouaid, C.; Bischoff, H.; Reinmuth, N.; Cove-Smith, L.; Mansy, T.; Cortinovis, D.; Migliorino, M.R.; et al. Safety and efficacy outcomes with durvalumab after sequential chemoradiotherapy (sCRT) in stage III, unresectable NSCLC (PACIFIC-6). Ann. Oncol. 2022, 33, S81–S82. [Google Scholar] [CrossRef]
- Peters, S.; Dafni, U.; Boyer, M.; De Ruysscher, D.; Faivre-Finn, C.; Felip, E.; Garrido, P.; Girard, N.; Guckenberger, M.; Haanen, J.; et al. Position of a panel of international lung cancer experts on the approval decision for use of durvalumab in stage III non-small-cell lung cancer (NSCLC) by the Committee for Medicinal Products for Human Use (CHMP). Ann. Oncol. 2019, 30, 161–165. [Google Scholar] [CrossRef]
- Furuse, K.; Fukuoka, M.; Kawahara, M.; Nishikawa, H.; Takada, Y.; Kudoh, S.; Katagami, N.; Ariyoshi, Y. Phase III study of concurrent versus sequential thoracic radiotherapy in combination with mitomycin, vindesine, and cisplatin in unresectable stage III non-small-cell lung cancer. J. Clin. Oncol. 1999, 17, 2692–2699. [Google Scholar] [CrossRef] [PubMed]
- Fournel, P.; Robinet, G.; Thomas, P.; Souquet, P.J.; Lena, H.; Vergnenegre, A.; Delhoume, J.Y.; Le Treut, J.; Silvani, J.A.; Dansin, E.; et al. Randomized phase III trial of sequential chemoradiotherapy compared with concurrent chemoradiotherapy in locally advanced non-small-cell lung cancer: Groupe Lyon-Saint-Etienne d’Oncologie Thoracique-Groupe Francais de Pneumo-Cancerologie NPC 95-01 Study. J. Clin. Oncol. 2005, 23, 5910–5917. [Google Scholar] [CrossRef] [PubMed]
- Zatloukal, P.; Petruzelka, L.; Zemanova, M.; Havel, L.; Janku, F.; Judas, L.; Kubik, A.; Krepela, E.; Fiala, P.; Pecen, L. Concurrent versus sequential chemoradiotherapy with cisplatin and vinorelbine in locally advanced non-small cell lung cancer: A randomized study. Lung Cancer 2004, 46, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.D. Are the results of RTOG 0617 mysterious? Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 1042–1044. [Google Scholar] [CrossRef]
- Jabbour, S.K.; Lee, K.H.; Frost, N.; Breder, V.V.; Kowalski, D.M.; Alawin, I.A.; Levchenko, E.; Reguart, N.; Martinez-Marti, A.; Houghton, B.; et al. KEYNOTE-799: Phase 2 trial of pembrolizumab plus platinum chemotherapy and radiotherapy for unresectable, locally advanced, stage 3 NSCLC. J. Clin. Oncol. 2021, 39, 8512. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statistics | High-Dose CRT (Salzburg) | Standard of Care (Vienna) | Statistics |
|---|---|---|---|
| n = 42 | n = 36 | p-value | |
| Age | |||
| mean (SD) | 64.5 (8.6) | 62.8 (8.9) | 0.390 |
| ≤65 years (%) | 47.6 | 57.5 | - |
| Sex (%) | |||
| female | 28.6 | 50.0 | 0.411 |
| male | 71.4 | 50.0 | - |
| ECOG (%) | |||
| <2 | 100 | 97.2 | 1 |
| Smoking status (%) | |||
| current, ex-smoker | 88.9 | 97.5 | 0.278 |
| never | 11.1 | 2.5 | - |
| Histology (%) | |||
| SCC | 38.1 | 40.0 | 0.799 |
| AC | 61.9 | 50.0 | - |
| NOS | 0.0 | 10.0 | - |
| Statistics | High-Dose CRT (Salzburg) | Standard of Care (Vienna) | Statistics | |
|---|---|---|---|---|
| n = 42 | n = 36 | p-Value | ||
| Chemotherapy | Number of cycles (%) | <0.001 | ||
| 1 | 2.4 | 2.5 | ||
| 2 | 97.6 | 15.0 | ||
| 3 | 0.0 | 27.5 | ||
| 4 | 0.0 | 55.0 | ||
| Agents (%) | <0.001 | |||
| Carboplatinum/Pemetrexed | 59.5 | 27.5 | ||
| Carboplatinum/Gemcitabine | 31.0 | 0.0 | ||
| Carboplatinum/Taxotere | 2.4 | 0.0 | ||
| Carboplatinum mono | 0.0 | 10.0 | ||
| Carboplatinum/Vinorelbin | 0.0 | 7.5 | ||
| Cisplatinum mono | 0.0 | 12.5 | ||
| Cisplatinum/Pemetrexed | 2.4 | 17.5 | ||
| Cisplatinum/Vinorelbin | 0.0 | 25.0 | ||
| Cisplatinum/Gemcitabine | 4.8 | 0.0 | ||
| Radiotherapy | Total dose (Gy) | <0.001 | ||
| Median (Min, Max) | 72.0 (54.0, 123.2) | 59.4 (30.0, 89.4) | ||
| Biologically effective dose (Gy) | <0.001 | |||
| Median (Min, Max) | 72.0 (58.5, 121.0) | 58.4 (32.5, 88.4) | ||
| Tumor PTV (mL) | 0.013 | |||
| Median (Min, Max) | 70.5 (9.0, 507) | 159.2 (22.7, 939.3) | ||
| Lymphnode PTV (mL) | 0.012 | |||
| Median (Min, Max) | 100.0 (9.0, 920.0) | 268.5 (32.0, 939.3) | ||
| Mean lung dose (Gy) | <0.001 | |||
| Median (Min, Max) | 13.0 (6.0, 18.0) | 16.7 (6.0, 34.0) | ||
| V20 total lung (%) | 0.008 | |||
| Median (Min, Max) | 20.5 (6.0, 32.0) | 16.0 (5.4, 32.1) | ||
| Immunotherapy | Interval end of RT and start of ICI (days) | 0.841 | ||
| Median (Min, Max) | 18.5 (4.0, 127.0) | 22.0 (2.0, 114.0) | ||
| Cycles (no.) | 0.031 | |||
| Median (Min, Max) | 14 (1, 26) | 8 (1, 21) | ||
| Statistics | High-Dose CRT (Salzburg) | Standard of Care (Vienna) | Statistics |
|---|---|---|---|
| n = 42 | n = 36 | p-Value | |
| Pneumonitis or pneumonia (%) | 28.6 | 27.8 | 0.599 |
| Hepatitis (%) | 9.5 | 0.0 | 0.089 |
| Thyreoiditis (%) | 4.8 | 13.8 | 0.182 |
| Clinical Outcome Correlations | ||||
|---|---|---|---|---|
| Variable | Regional Control | Distant Control | ||
| Local Control | CC | p-value | CC | p-value |
| 0.379 | 0.001 | 0.288 | 0.016 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wass, R.; Hochmair, M.; Kaiser, B.; Grambozov, B.; Feurstein, P.; Weiß, G.; Moosbrugger, R.; Sedlmayer, F.; Lamprecht, B.; Studnicka, M.; et al. Durvalumab after Sequential High Dose Chemoradiotherapy versus Standard of Care (SoC) for Stage III NSCLC: A Bi-Centric Retrospective Comparison Focusing on Pulmonary Toxicity. Cancers 2022, 14, 3226. https://doi.org/10.3390/cancers14133226
Wass R, Hochmair M, Kaiser B, Grambozov B, Feurstein P, Weiß G, Moosbrugger R, Sedlmayer F, Lamprecht B, Studnicka M, et al. Durvalumab after Sequential High Dose Chemoradiotherapy versus Standard of Care (SoC) for Stage III NSCLC: A Bi-Centric Retrospective Comparison Focusing on Pulmonary Toxicity. Cancers. 2022; 14(13):3226. https://doi.org/10.3390/cancers14133226
Chicago/Turabian StyleWass, Romana, Maximilian Hochmair, Bernhard Kaiser, Brane Grambozov, Petra Feurstein, Gertraud Weiß, Raphaela Moosbrugger, Felix Sedlmayer, Bernd Lamprecht, Michael Studnicka, and et al. 2022. "Durvalumab after Sequential High Dose Chemoradiotherapy versus Standard of Care (SoC) for Stage III NSCLC: A Bi-Centric Retrospective Comparison Focusing on Pulmonary Toxicity" Cancers 14, no. 13: 3226. https://doi.org/10.3390/cancers14133226