
Clinical Viability of Boron Neutron Capture Therapy for Personalized Radiation Treatment

 ,
,  ,
,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Fundamental Aspects of BNCT
2.1. BNCT as Targeted Radiotherapy
2.2. Mechanisms of Cell Death in BNCT
2.3. Physical Basis and Dosimetry of BNCT
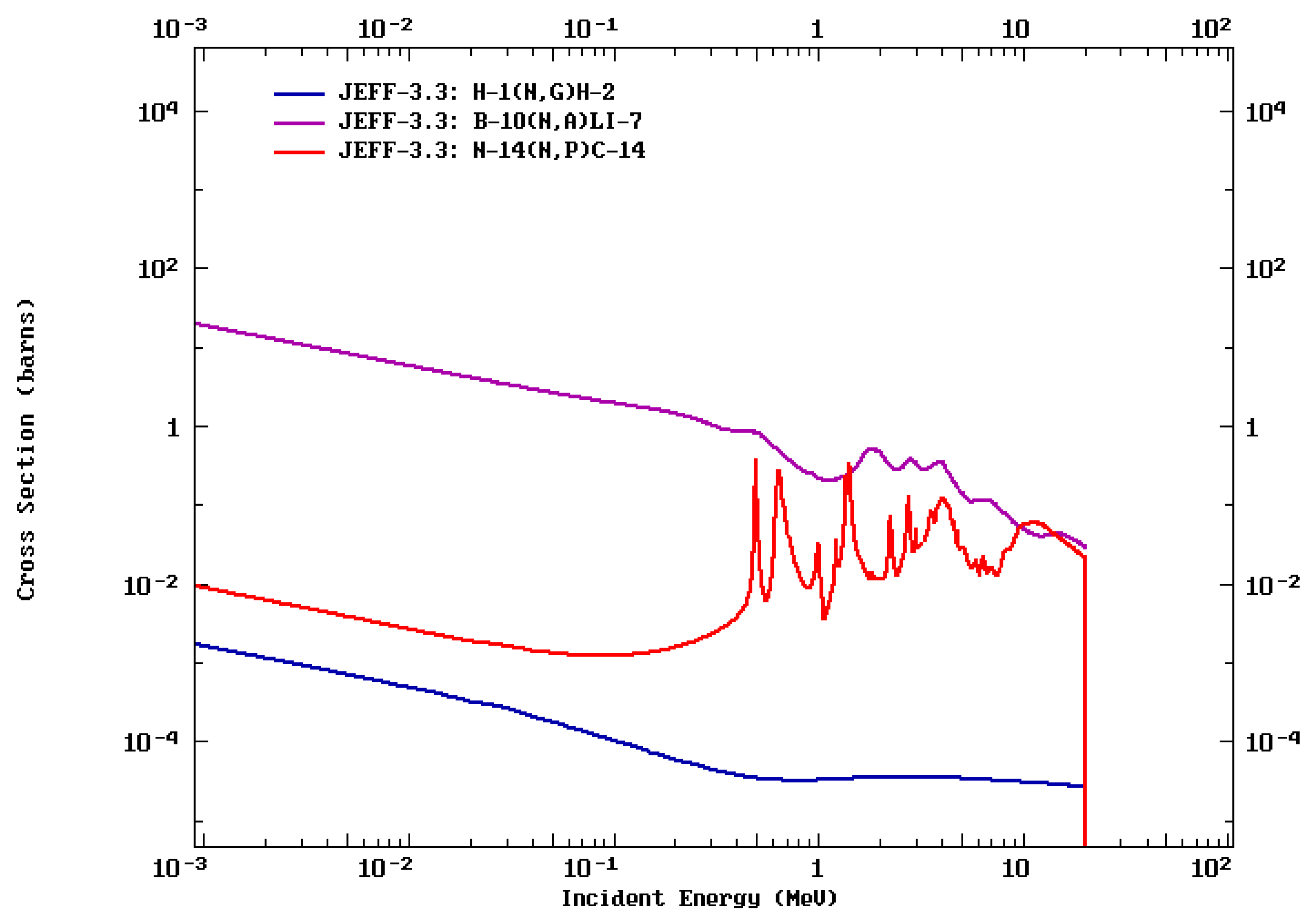
- Fast neutron dose: according to 1H(n, n)p reactions, fast and epithermal neutrons cause elastic neutron collisions with hydrogen in tissue (giving recoiling protons and gammas). Other energy depositions from fast neutron reactions like 12C(n, α) are also included.
- Incident and secondary gamma ray’s dose: Primary gamma dose from the beam port and secondary gamma dose by 1H (n, γ)2H. This component can be used for real time dosimetry with SPECT imaging, as it is further described in Section 3.
- Nitrogen dose: according to the 14N (n, p)14C reaction, the 14N element in the tissue captures a thermal neutron and, as a result, a ~600 keV proton is emitted. The dose is obtained from locally delivered energy from the recoiling 14C nucleus and the energetic proton.
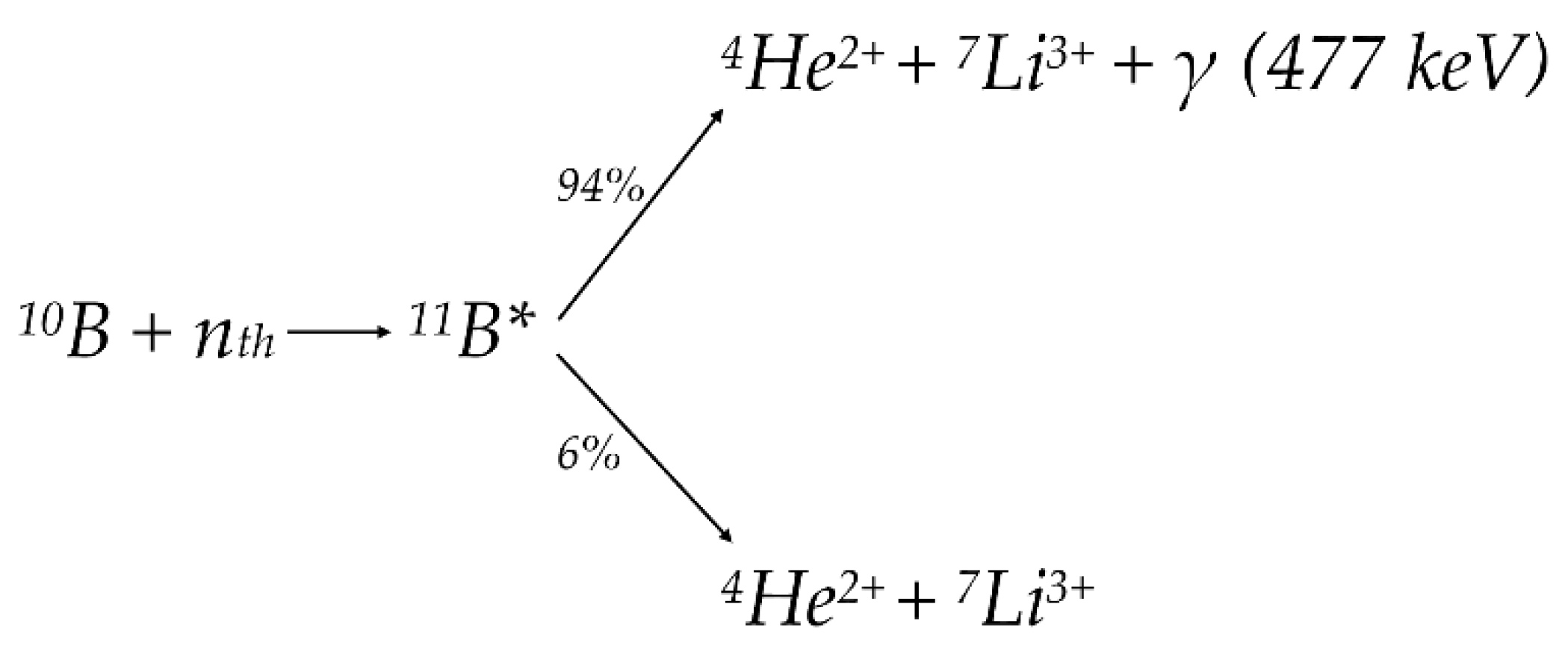
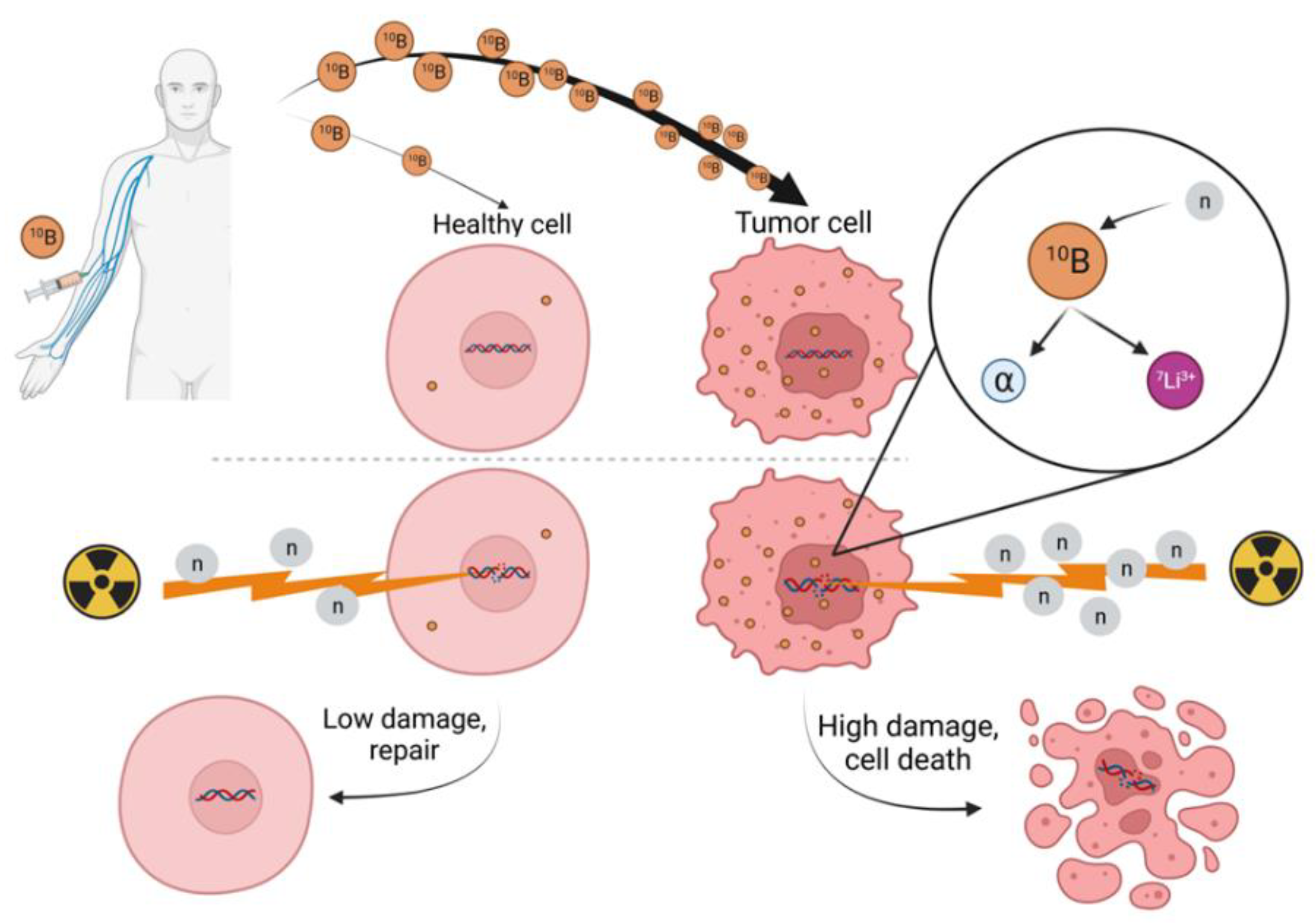
- Boron dose: energy deposited by the 10B (n, α)7Li reaction. 10B captures a thermal neutron, and as a result, an alpha particle and a recoiling 7Li ion are emitted. The dose derived from the reaction products is ~2.31 MeV.
2.4. BNCT Biological Dosimetry
3. Boron Analysis and Boron Imaging in BNCT
3.1. Positron Emission Tomography and Magnetic Resonance Imaging
3.2. Mass Spectrometry Imaging
3.3. Single-Photon Emission Computed Tomography and Prompt Gamma-Photon Detectors
4. Clinical Possibilities of BNCT and Future Perspectives
4.1. New Compact Linac-Based BNCT Neutron Sources
4.2. BNCT Clinical Trials
4.3. BNCT and Personalized Radiotherapy
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. The Hallmarks of Cancer. Cell 2000, 100, 57–70. [Google Scholar] [CrossRef] [Green Version]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atun, R.; Jaffray, D.A.; Barton, M.B.; Bray, F.; Baumann, M.; Vikram, B.; Hanna, T.P.; Knaul, F.M.; Lievens, Y.; Lui, T.Y.M.; et al. Expanding Global Access to Radiotherapy. Lancet Oncol. 2015, 16, 1153–1186. [Google Scholar] [CrossRef]
- Baskar, R.; Lee, K.A.; Yeo, R.; Yeoh, K.-W. Cancer and Radiation Therapy: Current Advances and Future Directions. Int. J. Med. Sci. 2012, 9, 193. [Google Scholar] [CrossRef] [Green Version]
- Fiorino, C.; Guckemberger, M.; Schwarz, M.; van der Heide, U.A.; Heijmen, B. Technology-driven Research for Radiotherapy Innovation. Mol. Oncol. 2020, 14, 1500. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Yang, J.; Fu, S.; Wu, J. Gold Nanoparticles as Radiosensitizers in Cancer Radiotherapy. Int. J. Nanomed. 2020, 15, 9407. [Google Scholar] [CrossRef]
- Farhood, B.; Samadian, H.; Ghorbani, M.; Zakariaee, S.S.; Knaup, C. Physical, Dosimetric and Clinical Aspects and Delivery Systems in Neutron Capture Therapy. Rep. Pract. Oncol. Radiother. 2018, 23, 462–473. [Google Scholar] [CrossRef]
- Nedunchezhian, K.; Aswath, N.; Thiruppathy, M.; Thirugnanamurthy, S. Boron Neutron Capture Therapy—A Literature Review. J. Clin. Diagn. Res. 2016, 10, ZE01–ZE04. [Google Scholar] [CrossRef]
- Macías, M.; Fernández, B.; Praena, J. New Data for the Definition of Neutron Beams for Boron Neutron Capture Therapy. Radiat. Phys. Chem. 2020, 185, 109474. [Google Scholar] [CrossRef]
- Dymova, M.A.; Taskaev, S.Y.; Richter, V.A.; Kuligina, E.V. Boron Neutron Capture Therapy: Current Status and Future Perspectives. Cancer Commun. 2020, 40, 406–421. [Google Scholar] [CrossRef] [PubMed]
- Espain, M.S.; Dattoli Viegas, A.M.; Trivillin, V.A.; Saint Martin, G.; Thorp, S.I.; Curotto, P.; Pozzi, E.C.C.; González, S.J.; Portu, A.M. Neutron Autoradiography to Study the Microdistribution of Boron in the Lung. Appl. Radiat. Isot. 2020, 165, 109331. [Google Scholar] [CrossRef] [PubMed]
- Wittig, A.; Michel, J.; Moss, R.L.; Stecher-Rasmussen, F.; Arlinghaus, H.F.; Bendel, P.; Mauri, P.L.; Altieri, S.; Hilger, R.; Salvadori, P.A.; et al. Boron Analysis and Boron Imaging in Biological Materials for Boron Neutron Capture Therapy (BNCT). Crit. Rev. Oncol./Hematol. 2008, 68, 66–90. [Google Scholar] [CrossRef] [PubMed]
- Qi, P.; Chen, Q.; Tu, D.; Yao, S.; Zhang, Y.; Wang, J.; Xie, C.; Pan, C.; Peng, H. The Potential Role of Borophene as a Radiosensitizer in Boron Neutron Capture Therapy (BNCT) and Particle Therapy (PT). Biomater. Sci. 2020, 8, 2778–2785. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Meng, Y.; Wang, X.; Xia, G.; Zhang, Q. The Endocytic Mechanism and Cytotoxicity of Boron-Containing Vesicles. Chem. Pharm. Bull. 2020, 68, c10-00971. [Google Scholar] [CrossRef]
- Miyatake, S.-I.; Kawabata, S.; Hiramatsu, R.; Kuroiwa, T.; Suzuki, M.; Ono, K. Boron Neutron Capture Therapy of Malignant Gliomas. Prog. Neurol. Surg. 2018, 32, 48–56. [Google Scholar] [CrossRef]
- Yokoyama, K.; Miyatake, S.-I.; Kajimoto, Y.; Kawabata, S.; Doi, A.; Yoshida, T.; Okabe, M.; Kirihata, M.; Ono, K.; Kuroiwa, T. Analysis of Boron Distribution In Vivo for Boron Neutron Capture Therapy Using Two Different Boron Compounds by Secondary Ion Mass Spectrometry. Radiat. Res. 2007, 167, 102–109. [Google Scholar] [CrossRef]
- Puris, E.; Gynther, M.; Auriola, S.; Huttunen, K.M. L-Type Amino Acid Transporter 1 as a Target for Drug Delivery. Pharm. Res. 2020, 37, 88. [Google Scholar] [CrossRef]
- CSID:132497 L-BPA|C9H12BNO4|Chemspider. Available online: http://www.chemspider.com/Chemical-Structure.132497.html (accessed on 1 June 2022).
- Hansch, C.; Rockwell, S.D.; Jow, P.Y.C.; Leo, A.; Steller, E.E. Substituent Constants for Correlation Analysis. J. Med. Chem. 1977, 20, 304–306. [Google Scholar] [CrossRef]
- Suzuki, M. Boron Neutron Capture Therapy (BNCT): A Unique Role in Radiotherapy with a View to Entering the Accelerator-Based BNCT Era. Int. J. Clin. Oncol. 2020, 25, 43–50. [Google Scholar] [CrossRef]
- Borofalan (10B)—Stella Pharma—AdisInsight. Available online: https://adisinsight.springer.com/drugs/800045201 (accessed on 16 September 2021).
- Farr, L.E.; Sweet, W.H.; Robertslon, J.S.; Foster, C.G.; Locksley, H.B.; Sutherland, D.L.; Mendelsohn, M.L.; Stickley, E.E. Neutron Capture Therapy with Boron in the Treatment of Glioblastoma Multiforme. Am. J. Roentgenol. Radium. Ther. Nucl. Med. 1954, 71, 279–293. [Google Scholar] [PubMed]
- Goodwin, J.T.; Farr, L.E.; Sweet, W.H.; Robertson, J.S. Pathological Study of Eight Patients with Glioblastoma Multiforme Treated by Neutron-Capture Therapy Using Boron 10. Cancer 1955, 8, 601–615. [Google Scholar] [CrossRef]
- Hoppenz, P.; Els-Heindl, S.; Kellert, M.; Kuhnert, R.; Saretz, S.; Lerchen, H.-G.; Köbberling, J.; Riedl, B.; Hey-Hawkins, E.; Beck-Sickinger, A.G. A Selective Carborane-Functionalized Gastrin-Releasing Peptide Receptor Agonist as Boron Delivery Agent for Boron Neutron Capture Therapy. J. Org. Chem. 2020, 85, 1446–1457. [Google Scholar] [CrossRef] [PubMed]
- Nakase, I.; Katayama, M.; Hattori, Y.; Ishimura, M.; Inaura, S.; Fujiwara, D.; Takatani-Nakase, T.; Fujii, I.; Futaki, S.; Kirihata, M. Intracellular Target Delivery of Cell-Penetrating Peptide-Conjugated Dodecaborate for Boron Neutron Capture Therapy (BNCT). Chem. Commun. 2019, 55, 13955–13958. [Google Scholar] [CrossRef]
- Nakase, I.; Aoki, A.; Sakai, Y.; Hirase, S.; Ishimura, M.; Takatani-Nakase, T.; Hattori, Y.; Kirihata, M. Antibody-Based Receptor Targeting Using an Fc-Binding Peptide-Dodecaborate Conjugate and Macropinocytosis Induction for Boron Neutron Capture Therapy. ACS Omega 2020, 5, 22731–22738. [Google Scholar] [CrossRef]
- Imperio, D.; Muz, B.; Azab, A.K.; Fallarini, S.; Lombardi, G.; Panza, L. A Short and Convenient Synthesis of Closo-Dodecaborate Sugar Conjugates. Eur. J. Org. Chem. 2019, 2019, 7228–7232. [Google Scholar] [CrossRef]
- Cappelli, A.; Valenti, S.; Mancini, A.; Giuliani, G.; Anzini, M.; Altieri, S.; Bortolussi, S.; Ferrari, C.; Clerici, A.M.; Zonta, C.; et al. Carborane-Conjugated 2-Quinolinecarboxamide Ligands of the Translocator Protein for Boron Neutron Capture Therapy. Bioconjugate Chem. 2010, 21, 2213–2221. [Google Scholar] [CrossRef]
- Worm, D.J.; Hoppenz, P.; Els-Heindl, S.; Kellert, M.; Kuhnert, R.; Saretz, S.; Köbberling, J.; Riedl, B.; Hey-Hawkins, E.; Beck-Sickinger, A.G. Selective Neuropeptide y Conjugates with Maximized Carborane Loading as Promising Boron Delivery Agents for Boron Neutron Capture Therapy. J. Med. Chem. 2020, 63, 2358–2371. [Google Scholar] [CrossRef]
- Feiner, I.V.J.; Pulagam, K.R.; Gómez-Vallejo, V.; Zamacola, K.; Baz, Z.; Caffarel, M.M.; Lawrie, C.H.; Ruiz-de-Angulo, A.; Carril, M.; Llop, J. Therapeutic Pretargeting with Gold Nanoparticles as Drug Candidates for Boron Neutron Capture Therapy. Part. Part. Syst. Charact. 2020, 37, 2000200. [Google Scholar] [CrossRef]
- Pulagam, K.R.; Gona, K.B.; Gómez-Vallejo, V.; Meijer, J.; Zilberfain, C.; Estrela-Lopis, I.; Baz, Z.; Cossío, U.; Llop, J. Gold Nanoparticles as Boron Carriers for Boron Neutron Capture Therapy: Synthesis, Radiolabelling and in Vivo Evaluation. Molecules 2019, 24, 3609. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Li, J.; Shi, Y.; Du, P.; Zhang, Z.; Liu, T.; Zhang, R.; Liu, Z. On-Demand Biodegradable Boron Nitride Nanoparticles for Treating Triple Negative Breast Cancer with Boron Neutron Capture Therapy. ACS Nano 2019, 13, 13843–13852. [Google Scholar] [CrossRef] [PubMed]
- Porras, I. Sulfur-33 Nanoparticles: A Monte Carlo Study of Their Potential as Neutron Capturers for Enhancing Boron Neutron Capture Therapy of Cancer. Appl. Radiat. Isot. 2011, 69, 1838–1841. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Mi, P.; Yang, W. Boron Delivery Agents for Neutron Capture Therapy of Cancer. Cancer Commun. 2018, 38, 35. [Google Scholar] [CrossRef] [Green Version]
- Sauerwein, W.A.G.; Sancey, L.; Hey-Hawkins, E.; Kellert, M.; Panza, L.; Imperio, D.; Balcerzyk, M.; Rizzo, G.; Scalco, E.; Herrmann, K.; et al. Theranostics in Boron Neutron Capture Therapy. Life 2021, 11, 330. [Google Scholar] [CrossRef] [PubMed]
- Matović, J.; Järvinen, J.; Sokka, I.K.; Imlimthan, S.; Raitanen, J.-E.; Montaser, A.; Maaheimo, H.; Huttunen, K.M.; Peräniemi, S.; Airaksinen, A.J.; et al. Exploring the Biochemical Foundations of a Successful GLUT1-Targeting Strategy to BNCT: Chemical Synthesis and In Vitro Evaluation of the Entire Positional Isomer Library of Ortho-Carboranylmethyl-Bearing Glucoconjugates. Mol. Pharm. 2021, 18, 285–304. [Google Scholar] [CrossRef]
- Desouky, O.; Ding, N.; Zhou, G. Targeted and Non-Targeted Effects of Ionizing Radiation. J. Radiat. Res. Appl. Sci. 2015, 8, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Tian, F.; Geng, C.-R.; Tang, X.-B.; Shu, D.-Y.; Ye, H.-F.; Bortolussi, S.; Gong, C.-H. Analysis of Influencing Factors on the Method for Determining Boron Concentration and Dose through Dual Prompt Gamma Detection. Nucl. Sci. Tech. 2021, 32, 35. [Google Scholar] [CrossRef]
- Hu, K.; Yang, Z.; Zhang, L.; Xie, L.; Wang, L.; Xu, H.; Josephson, L.; Liang, S.H.; Zhang, M.-R. Boron Agents for Neutron Capture Therapy. Coord. Chem. Rev. 2020, 405, 213139. [Google Scholar] [CrossRef]
- Elgazzar Abdelhamid, H.; Kazem, N. Biological Effects of Ionizing Radiation. In The Pathophysiologic Basis of Nuclear Medicine; Elgazzar, A.H., Ed.; Springer: Berlin/Heidelberg, Germany, 2006; pp. 540–548. ISBN 978-3-540-47953-6. [Google Scholar]
- Freneau, A.; dos Santos, M.; Voisin, P.; Tang, N.; Bueno Vizcarra, M.; Villagrasa, C.; Roy, L.; Vaurijoux, A.; Gruel, G. Relation between DNA Double-Strand Breaks and Energy Spectra of Secondary Electrons Produced by Different X-ray Energies. Int. J. Radiat. Biol. 2018, 94, 1075–1084. [Google Scholar] [CrossRef]
- Fujita, Y.; Kato, I.; Iwai, S.; Ono, K.; Suzuki, M.; Sakurai, Y.; Ohnishi, K.; Ohnishi, T.; Yura, Y. Role of P53 Mutation in the Effect of Boron Neutron Capture Therapy on Oral Squamous Cell Carcinoma. Radiat. Oncol. 2009, 4, 63. [Google Scholar] [CrossRef] [Green Version]
- Takatsuji, T.; Yoshikawa, I.; Sasaki, M.S. Generalized Concept of the LET-RBE Relationship of Radiation-Induced Chromosome Aberration and Cell Death. J. Radiat. Res. 1999, 40, 59–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maliszewska-Olejniczak, K.; Kaniowski, D.; Araszkiewicz, M.; Tymińska, K.; Korgul, A. Molecular Mechanisms of Specific Cellular DNA Damage Response and Repair Induced by the Mixed Radiation Field During Boron Neutron Capture Therapy. Front. Oncol. 2021, 11, 1799. [Google Scholar] [CrossRef] [PubMed]
- Galluzzi, L.; Vitale, I.; Aaronson, S.A.; Abrams, J.M.; Adam, D.; Agostinis, P.; Alnemri, E.S.; Altucci, L.; Amelio, I.; Andrews, D.W.; et al. Molecular Mechanisms of Cell Death: Recommendations of the Nomenclature Committee on Cell Death 2018. Cell Death Differ. 2018, 25, 486–541. [Google Scholar] [CrossRef]
- Wang, P.; Zhen, H.; Jiang, X.; Zhang, W.; Cheng, X.; Guo, G.; Mao, X.; Zhang, X. Boron Neutron Capture Therapy Induces Apoptosis of Glioma Cells through Bcl-2/Bax. BMC Cancer 2010, 10, 661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuya, Y.; Fukunaga, H.; Omura, M.; Date, H. A Model for Estimating Dose-Rate Effects on Cell-Killing of Human Melanoma after Boron Neutron Capture Therapy. Cells 2020, 9, 1117. [Google Scholar] [CrossRef]
- Seki, K.; Kinashi, Y.; Takahashi, S. Influence of P53 Status on the Effects of Boron Neutron Capture Therapy in Glioblastoma. Anticancer Res. 2015, 35, 169–174. [Google Scholar]
- Rodriguez, C.; Carpano, M.; Curotto, P.; Thorp, S.; Casal, M.; Juvenal, G.; Pisarev, M.; Dagrosa, M.A. In Vitro Studies of DNA Damage and Repair Mechanisms Induced by BNCT in a Poorly Differentiated Thyroid Carcinoma Cell Line. Radiat. Environ. Biophys. 2018, 57, 143–152. [Google Scholar] [CrossRef]
- Syamputra, D.N.I.; Sardjono, Y.; Mahmudah, R.S.N. Dose Analysis of BNCT Treatment Method for Rhabdomyosarcoma in the Head and Neck Regions Based on PHITS Code. ASEAN J. Sci. Technol. Dev. 2020, 35, 235–239. [Google Scholar] [CrossRef] [Green Version]
- Ono, K.; Tanaka, H.; Suzuki, M. Reevaluation of CBE Value of BPA for Hepatocytes. Appl. Radiat. Isot. 2020, 161, 109159. [Google Scholar] [CrossRef]
- Streitmatter, S.W.; Stewart, R.D.; Moffitt, G.; Jevremovic, T. Mechanistic Modeling of the Relative Biological Effectiveness of Boron Neutron Capture Therapy. Cells 2020, 9, 2302. [Google Scholar] [CrossRef]
- Aldossari, S.; McMahon, G.; Lockyer, N.P.; Moore, K.L. Microdistribution and Quantification of the Boron Neutron Capture Therapy Drug BPA in Primary Cell Cultures of Human Glioblastoma Tumour by NanoSIMS. Analyst 2019, 144, 6214–6224. [Google Scholar] [CrossRef] [PubMed]
- Swanepoel, M.W. The Role of the 14N(n,p)14C Reaction in Neutron Irradiation of Soft Tissues. Radiat. Meas. 2010, 45, 1458–1461. [Google Scholar] [CrossRef]
- Kumada, H.; Takada, K. Treatment Planning System and Patient Positioning for Boron Neutron Capture Therapy. Ther. Radiol. Oncol. 2018, 2, 50. [Google Scholar] [CrossRef]
- Lee, C.M.; Lee, H.S. Development of a Dose Estimation Code for BNCT with GPU Accelerated Monte Carlo and Collapsed Cone Convolution Method. Nucl. Eng. Technol. 2022, 54, 1769–1780. [Google Scholar] [CrossRef]
- Hu, N.; Tanaka, H.; Kakino, R.; Yoshikawa, S.; Miyao, M.; Akita, K.; Isohashi, K.; Aihara, T.; Nihei, K.; Ono, K. Evaluation of a Treatment Planning System Developed for Clinical Boron Neutron Capture Therapy and Validation against an Independent Monte Carlo Dose Calculation System. Radiat. Oncol. 2021, 16, 243. [Google Scholar] [CrossRef]
- Judith, F. MCNP TM-A General Monte Carlo N-Particle Transport Code Version 4C; University of California: San Diego, CA, USA, 2000. [Google Scholar]
- Wheeler, F.J.; Wessol, D.E.; Wemple, C.A.; Nigg, D.W.; Albright, C.L.; Cohen, M.T.; Frandsen, M.W.; Harkin, G.J.; Rossmeier, M.B. SERA-an Advanced Treatment Planning System for Neutron Therapy; Idaho National Engineering and Environmental: Idaho Falls, ID, USA, 1999. [Google Scholar]
- Iwase, H.; Niita, K.; Nakamura, T. Development of General-Purpose Particle and Heavy Ion Transport Monte Carlo Code. J. Nucl. Sci. Tehnol. 2012, 39, 1142–1151. [Google Scholar] [CrossRef]
- Hu, N.; Tanaka, H.; Takata, T.; Endo, S.; Masunaga, S.; Suzuki, M.; Sakurai, Y. Evaluation of PHITS for Microdosimetry in BNCT to Support Radiobiological Research. Appl. Radiat. Isot. 2020, 161, 109148. [Google Scholar] [CrossRef]
- Sato, T.; Masunaga, S.; Kumada, H.; Hamada, N. Microdosimetric Modeling of Biological Effectiveness for Boron Neutron Capture Therapy Considering Intra- and Intercellular Heterogeneity in 10B Distribution. Sci. Rep. 2018, 8, 988. [Google Scholar] [CrossRef]
- Evaluated Nuclear Data File (ENDF). Available online: https://www.nndc.bnl.gov/exfor/endf00.jsp (accessed on 13 September 2021).
- International Atomic Energy Agency. Current Status of Neutron Capture Therapy; IAEA: Vienna, Austria, 2001; Volume IAEA-TECDOC-1223. [Google Scholar]
- Incerti, S.; Kyriakou, I.; Bernal, M.A.; Bordage, M.C.; Francis, Z.; Guatelli, S.; Ivanchenko, V.; Karamitros, M.; Lampe, N.; Lee, S.B.; et al. Geant4-DNA Example Applications for Track Structure Simulations in Liquid Water: A Report from the Geant4-DNA Project. Med. Phys. 2018, 45, e722–e739. [Google Scholar] [CrossRef] [Green Version]
- Perry, C.C.; Ramos-Méndez, J.; Milligan, J.R. DNA Condensation with a Boron-Containing Cationic Peptide for Modeling Boron Neutron Capture Therapy. Radiat. Phys. Chem. 2020, 166, 108521. [Google Scholar] [CrossRef]
- Sun, T.; Zhang, Z.; Li, B.; Chen, G.; Xie, X.; Wei, Y.; Wu, J.; Zhou, Y.; Du, Z. Boron Neutron Capture Therapy Induces Cell Cycle Arrest and Cell Apoptosis of Glioma Stem/Progenitor Cells in Vitro. Radiat. Oncol. 2013, 8, 195. [Google Scholar] [CrossRef] [Green Version]
- Pedrosa-Rivera, M.; Praena, J.; Porras, I.; Sabariego, M.P.; Köster, U.; Haertlein, M.; Forsyth, V.T.; Ramírez, J.C.; Jover, C.; Jimena, D.; et al. Thermal Neutron Relative Biological Effectiveness Factors for Boron Neutron Capture Therapy from In Vitro Irradiations. Cells 2020, 9, 2144. [Google Scholar] [CrossRef] [PubMed]
- Staaf, E.; Brehwens, K.; Haghdoost, S.; Czub, J.; Wojcik, A. Gamma-H2AX Foci in Cells Exposed to a Mixed Beam of X-rays and Alpha Particles. Genome Integr. 2012, 3, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masutani, M.; Baiseitov, D.; Itoh, T.; Hirai, T.; Berikkhanova, K.; Murakami, Y.; Zhumadilov, Z.; Imahori, Y.; Hoshi, M.; Itami, J. Histological and Biochemical Analysis of DNA Damage after BNCT in Rat Model. Appl. Radiat. Isot. 2014, 88, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Lapytsko, A.; Kollarovic, G.; Ivanova, L.; Studencka, M.; Schaber, J. FoCo: A Simple and Robust Quantification Algorithm of Nuclear Foci. BMC Bioinform. 2015, 16, 392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-Valverde, J.A.; Jiménez-Ortega, E.; Leal, A. Clinical Feasibility Study of Gold Nanoparticles as Theragnostic Agents for Precision Radiotherapy. Biomedicines 2022, 10, 1214. [Google Scholar] [CrossRef]
- Kuperman, V.Y. Effect of Dose Rate in Hypofractionated Radiotherapy. Phys. Med. 2019, 65, 191–199. [Google Scholar] [CrossRef]
- Faião-Flores, F.; Coelho, P.R.P.; Muniz, R.O.R.; Souza, G.S.; Arruda-Neto, J.; Maria, D.A. Antitumor Potential Induction and Free Radicals Production in Melanoma Cells by Boron Neutron Capture Therapy. Appl. Radiat. Isot. 2011, 69, 1748–1751. [Google Scholar] [CrossRef]
- Mares, V.; Krajcí, D.; Lisá, V. Subcellular Targets of Mercaptoborate (BSH), a Carrier of 10B for Neutron Capture Therapy (BNCT) of Brain Tumors. Physiol. Res. 2003, 52, 629–636. [Google Scholar]
- Romanov, V.; Isohashi, K.; Alobthani, G.; Beshr, R.; Horitsugi, G.; Kanai, Y.; Naka, S.; Watabe, T.; Shimosegawa, E.; Hatazawa, J. Evaluation of the Total Distribution Volume of 18F-FBPA in Normal Tissues of Healthy Volunteers by Non-Compartmental Kinetic Modeling. Ann. Nucl. Med. 2020, 34, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Coderre, J.A.; Chanana, A.D.; Joel, D.D.; Elowitz, E.H.; Micca, P.L.; Nawrocky, M.M.; Chadha, M.; Gebbers, J.O.; Shady, M.; Peress, N.S.; et al. Biodistribution of Boronophenylalanine in Patients with Glioblastoma Multiforme: Boron Concentration Correlates with Tumor Cellularity. Radiat. Res. 1998, 149, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Fukumitsu, N.; Matsumoto, Y. Development of an Imaging Technique for Boron Neutron Capture Therapy. Cells 2021, 10, 2135. [Google Scholar] [CrossRef] [PubMed]
- Menichetti, L.; Petroni, D.; Panetta, D.; Burchielli, S.; Bortolussi, S.; Matteucci, M.; Pascali, G.; del Turco, S.; del Guerra, A.; Altieri, S.; et al. A Micro-PET/CT Approach Using O-(2-[18F]Fluoroethyl)-l-Tyrosine in an Experimental Animal Model of F98 Glioma for BNCT. Appl. Radiat. Isot. 2011, 69, 1717–1720. [Google Scholar] [CrossRef] [PubMed]
- Shimosegawa, E.; Isohashi, K.; Naka, S.; Horitsugi, G.; Hatazawa, J. Assessment of 10B Concentration in Boron Neutron Capture Therapy: Potential of Image-Guided Therapy Using 18FBPA PET. Ann. Nucl. Med. 2016, 30, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Shi, Y.; Zhang, Z.; Liu, H.; Lang, L.; Liu, T.; Chen, X.; Liu, Z. A Metabolically Stable Boron-Derived Tyrosine Serves as a Theranostic Agent for Positron Emission Tomography Guided Boron Neutron Capture Therapy. Bioconjugate Chem. 2019, 30, 2870–2878. [Google Scholar] [CrossRef]
- Sato, A.; Itoh, T.; Imamichi, S.; Kikuhara, S.; Fujimori, H.; Hirai, T.; Saito, S.; Sakurai, Y.; Tanaka, H.; Nakamura, H.; et al. Proteomic Analysis of Cellular Response Induced by Boron Neutron Capture Reaction in Human Squamous Cell Carcinoma SAS Cells. Appl. Radiat. Isot. 2015, 106, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, E.; Wittig, A.; Basilico, F.; Rossi, R.; de Palma, A.; di Silvestre, D.; Sauerwein, W.; Mauri, P. Urinary Proteomics Profiles Are Useful for Detection of Cancer Biomarkers and Changes Induced by Therapeutic Procedures. Molecules 2019, 24, 794. [Google Scholar] [CrossRef] [Green Version]
- Ekholm, F.S.; Matovic, J.; Jarvinen, J.; Bland, H.C.; Sokka, I.K.; Imlimthan, S.; Huttunen, K.M.; Timonen, J.; Peraniemi, S.; Aitio, O.; et al. Addressing the Biochemical Foundations of a Glucose-Based “Trojan Horse”-Strategy to Boron Neutron Capture Therapy: From Chemical Synthesis to in Vitro Assessment. Mol. Pharm. 2020, 17, 3885–3899. [Google Scholar] [CrossRef]
- Balcerzyk, M.; De-Miguel, M.; Guerrero, C.; Fernandez, B. Quantification of Boron Compound Concentration for BNCT Using Positron Emission Tomography. Cells 2020, 9, 2084. [Google Scholar] [CrossRef]
- Nariai, T.; Ishiwata, K.; Kimura, Y.; Inaji, M.; Momose, T.; Yamamoto, T.; Matsumura, A.; Ishii, K.; Ohno, K. PET Pharmacokinetic Analysis to Estimate Boron Concentration in Tumor and Brain as a Guide to Plan BNCT for Malignant Cerebral Glioma. Appl. Radiat. Isot. 2009, 67, S348–S350. [Google Scholar] [CrossRef]
- Watanabe, Y.; Kurihara, H.; Itami, J.; Sasaki, R.; Arai, Y.; Sugimura, K. Relationship between the Uptake of 18F-Borono-L-Phenylalanine and L-[Methyl-11C] Methionine in Head and Neck Tumors and Normal Organs. Radiat. Oncol. 2017, 12, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, T.; Nakai, K.; Nariai, T.; Kumada, H.; Okumura, T.; Mizumoto, M.; Tsuboi, K.; Zaboronok, A.; Ishikawa, E.; Aiyama, H.; et al. The Status of Tsukuba BNCT Trial: BPA-Based Boron Neutron Capture Therapy Combined with X-ray Irradiation. Appl. Radiat. Isot. 2011, 69, 1817–1818. [Google Scholar] [CrossRef] [PubMed]
- Alberti, D.; Deagostino, A.; Toppino, A.; Protti, N.; Bortolussi, S.; Altieri, S.; Aime, S.; Geninatti Crich, S. An Innovative Therapeutic Approach for Malignant Mesothelioma Treatment Based on the Use of Gd/Boron Multimodal Probes for MRI Guided BNCT. J. Control. Release 2018, 280, 31–38. [Google Scholar] [CrossRef]
- Geninatti-Crich, S.; Deagostino, A.; Toppino, A.; Alberti, D.; Venturello, P.; Aime, S. Boronated Compounds for Imaging Guided BNCT Applications. Anti-Cancer Agents Med. Chem. 2012, 12, 543–553. [Google Scholar] [CrossRef]
- Geninatti-Crich, S.; Alberti, D.; Szabo, I.; Deagostino, A.; Toppino, A.; Barge, A.; Ballarini, F.; Bortolussi, S.; Bruschi, P.; Protti, N.; et al. MRI-Guided Neutron Capture Therapy by Use of a Dual Gadolinium/Boron Agent Targeted at Tumour Cells through Upregulated Low-Density Lipoprotein Transporters. Chem. Eur. J. 2011, 17, 8479–8486. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-Y.; Hsieh, H.-H.; Chang, T.-Y.; Lin, J.-J.; Wu, C.-C.; Hsu, M.-H.; Lin, M.-C.; Peng, S.-L. Development of MRI-Detectable Boron-Containing Gold Nanoparticle-Encapsulated Biodegradable Polymeric Matrix for Boron Neutron Capture Therapy (BNCT). Int. J. Mol. Sci. 2021, 22, 8050. [Google Scholar] [CrossRef] [PubMed]
- Kuthala, N.; Vankayala, R.; Li, Y.; Chiang, C.; Hwang, K.C. Engineering Novel Targeted Boron-10-Enriched Theranostic Nanomedicine to Combat against Murine Brain Tumors via MR Imaging-Guided Boron Neutron Capture Therapy. Adv. Mater. 2017, 29, 1700850. [Google Scholar] [CrossRef]
- Bonora, M.; Corti, M.; Borsa, F.; Bortolussi, S.; Protti, N.; Santoro, D.; Stella, S.; Altieri, S.; Zonta, C.; Clerici, A.M.; et al. 1H and 10B NMR and MRI Investigation of Boron- and Gadolinium–Boron Compounds in Boron Neutron Capture Therapy. Appl. Radiat. Isot. 2011, 69, 1702–1705. [Google Scholar] [CrossRef]
- Chandra, S.; Ahamad, T.; Barth, R.F.; Kabalka, G.W. Quantitative Evaluation of Boron Neutron Capture Therapy (BNCT) Drugs for Boron Delivery and Retention at Subcellular-Scale Resolution in Human Glioblastoma Cells with Imaging Secondary Ion Mass Spectrometry (SIMS). J. Microsc. 2014, 254, 146–156. [Google Scholar] [CrossRef] [Green Version]
- Lanni, E.J.; Rubakhin, S.S.; Sweedler, J.V. Mass Spectrometry Imaging and Profiling of Single Cells. J. Proteom. 2012, 75, 5036–5051. [Google Scholar] [CrossRef] [Green Version]
- Barth, R.F.; Kabalka, G.W.; Yang, W.; Huo, T.; Nakkula, R.J.; Shaikh, A.L.; Haider, S.A.; Chandra, S. Evaluation of Unnatural Cyclic Amino Acids as Boron Delivery Agents for Treatment of Melanomas and Gliomas. Appl. Radiat. Isot. 2014, 88, 38–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arlinghaus, H.F.; Fartmann, M.; Kriegeskotte, C.; Dambach, S.; Wittig, A.; Sauerwein, W.; Lipinsky, D. Subcellular Imaging of Cell Cultures and Tissue for Boron Localization with Laser-SNMS. Surf. Interface Anal. 2004, 36, 698–701. [Google Scholar] [CrossRef]
- Chandra, S.; Barth, R.F.; Haider, S.A.; Yang, W.; Huo, T.; Shaikh, A.L.; Kabalka, G.W. Biodistribution and Subcellular Localization of an Unnatural Boron-Containing Amino Acid (Cis-ABCPC) by Imaging Secondary Ion Mass Spectrometry for Neutron Capture Therapy of Melanomas and Gliomas. PLoS ONE 2013, 8, e75377. [Google Scholar] [CrossRef] [PubMed]
- Murata, I.; Kusaka, S.; Minami, K.; Saraue, N.; Tamaki, S.; Kato, I.; Sato, F. Design of SPECT for BNCT to Measure Local Boron Dose with GAGG Scintillator. Appl. Radiat. Isot. 2022, 181, 110056. [Google Scholar] [CrossRef] [PubMed]
- Minsky, D.M.; Valda, A.A.; Kreiner, A.J.; Green, S.; Wojnecki, C.; Ghani, Z. First Tomographic Image of Neutron Capture Rate in a BNCT Facility. Appl. Radiat. Isot. 2011, 69, 1858–1861. [Google Scholar] [CrossRef] [PubMed]
- Minsky, D.M.; Valda, A.A.; Kreiner, A.J.; Green, S.; Wojnecki, C.; Ghani, Z. Experimental Feasibility Studies on a SPECT Tomograph for BNCT Dosimetry. Appl. Radiat. Isot. 2009, 67, S179–S182. [Google Scholar] [CrossRef]
- Winkler, A.; Koivunoro, H.; Reijonen, V.; Auterinen, I.; Savolainen, S. Prompt Gamma and Neutron Detection in BNCT Utilizing a CdTe Detector. Appl. Radiat. Isot. 2015, 106, 139–144. [Google Scholar] [CrossRef]
- Abbene, L.; Principato, F.; Buttacavoli, A.; Gerardi, G.; Bettelli, M.; Zappettini, A.; Altieri, S.; Auricchio, N.; Caroli, E.; Zanettini, S.; et al. Potentialities of High-Resolution 3-D CZT Drift Strip Detectors for Prompt Gamma-Ray Measurements in BNCT. Sensors 2022, 22, 1502. [Google Scholar] [CrossRef]
- Murata, I.; Mukai, T.; Nakamura, S.; Miyamaru, H.; Kato, I. Development of a Thick CdTe Detector for BNCT–SPECT. Appl. Radiat. Isot. 2011, 69, 1706–1709. [Google Scholar] [CrossRef]
- Murata, I.; Nakamura, S.; Manabe, M.; Miyamaru, H.; Kato, I. Characterization Measurement of a Thick CdTe Detector for BNCT-SPECT—Detection Efficiency and Energy Resolution. Appl. Radiat. Isot. 2014, 88, 129–133. [Google Scholar] [CrossRef]
- Kim, M.; Hong, B.H.; Cho, I.; Park, C.; Min, S.-H.; Hwang, W.T.; Lee, W.; Kim, K.M. Design of a Scintillator-Based Prompt Gamma Camera for Boron-Neutron Capture Therapy: Comparison of SrI2 and GAGG Using Monte-Carlo Simulation. Nucl. Eng. Technol. 2021, 53, 626–636. [Google Scholar] [CrossRef]
- Kanno, I.; Nishimatsu, D.; Funama, F. Simulation Study on the Feasibility of Current-Mode SPECT for B-10 Concentration Estimation in Boron Neutron Capture Therapy. J. Instrum. 2019, 14, C02002. [Google Scholar] [CrossRef]
- Goodman, J.H.; Yang, W.; Barth, R.F.; Gao, Z.; Boesel, C.P.; Staubus, A.E.; Gupta, N.; Gahbauer, R.A.; Adams, D.M.; Gibson, C.R.; et al. Boron Neutron Capture Therapy of Brain Tumors: Biodistribution, Pharmacokinetics, and Radiation Dosimetry Sodium Borocaptate in Patients with Gliomas. Neurosurgery 2000, 47, 608–622. [Google Scholar] [CrossRef] [PubMed]
- Verbakel, W.F.A.R. Validation of the Scanning γ-Ray Telescope for in Vivo Dosimetry and Boron Measurements during BNCT. Phys. Med. Biol. 2001, 46, 3269. [Google Scholar] [CrossRef] [PubMed]
- Moro, D.; Colautti, P.; Gualdrini, G.; Masi, M.; Conte, V.; de Nardo, L.; Tornielli, G. Two Miniaturised TEPCS in a Single Detector for BNCT Microdosimetry. Radiat. Prot. Dosim. 2006, 122, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Moro, D.; Colautti, P.; Lollo, M.; Esposito, J.; Conte, V.; de Nardo, L.; Ferretti, A.; Ceballos, C. BNCT Dosimetry Performed with a Mini Twin Tissue-Equivalent Proportional Counters (TEPC). Appl. Radiat. Isot. 2009, 67, S171–S174. [Google Scholar] [CrossRef] [PubMed]
- Kiyanagi, Y.; Sakurai, Y.; Kumada, H.; Tanaka, H. Status of Accelerator-Based BNCT Projects Worldwide. AIP Conf. Proc. 2019, 2160, 050012. [Google Scholar]
- Kato, T.; Hirose, K.; Tanaka, H.; Mitsumoto, T.; Motoyanagi, T.; Arai, K.; Harada, T.; Takeuchi, A.; Kato, R.; Yajima, S.; et al. Design and Construction of an Accelerator-Based Boron Neutron Capture Therapy (AB-BNCT) Facility with Multiple Treatment Rooms at the Southern Tohoku BNCT Research Center. Appl. Radiat. Isot. 2020, 156, 108961. [Google Scholar] [CrossRef]
- BNCT System NeuCure®|BNCT System MEDICAL|Sumitomo Heavy Industries, Ltd. Industrial Equipment Division. Available online: https://www.shi.co.jp/industrial/en/product/medical/bnct/neucure.html (accessed on 30 April 2022).
- IBA Worldwide—Shaping the Future of Proton Therapy. Available online: https://www.iba-worldwide.com/proton-therapy (accessed on 30 April 2022).
- He, H.; Li, J.; Jiang, P.; Tian, S.; Wang, H.; Fan, R.; Liu, J.; Yang, Y.; Liu, Z.; Wang, J. The Basis and Advances in Clinical Application of Boron Neutron Capture Therapy. Radiat. Oncol. 2021, 16, 216. [Google Scholar] [CrossRef]
- Asbury, A.K.; Ojemann, R.G.; Nielsen, S.L.; Sweet, W.H. Neuropathologic Study of Fourteen Cases of Malignant Brain Tumor Treated by Boron-10 Slow Neutron Capture Radiation. J. Neuropathol. Exp. Neurol. 1972, 31, 278–303. [Google Scholar] [CrossRef]
- Sweet, W.H.; Javid, M. The Possible Use of Neutron-Capturing Isotopes Such as Boron 10 in the Treatment of Neoplasms. I. Intracranial Tumors. J. Neurosurg. 1952, 9, 200–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishima, Y.; Ichihashi, M.; Hatta, S.; Honda, C.; Yamamura, K.; Nakagawa, T.; Obara, H.; Shirakawa, J.; Hiratsuka, J.; Taniyama, K. First Human Clinical Trial of Melanoma Neutron Capture. Diagnosis and Therapy. Strahlenther. Onkol. 1989, 165, 251–254. [Google Scholar] [PubMed]
- Joensuu, H.; Kankaanranta, L.; Seppälä, T.; Auterinen, I.; Kallio, M.; Kulvik, M.; Laakso, J.; Vähätalo, J.; Kortesniemi, M.; Kotiluoto, P.; et al. Boron Neutron Capture Therapy of Brain Tumors: Clinical Trials at the Finnish Facility Using Boronophenylalanine. J. Neuro-Oncol. 2003, 62, 123–134. [Google Scholar] [CrossRef]
- Kankaanranta, L.; Seppälä, T.; Koivunoro, H.; Saarilahti, K.; Atula, T.; Collan, J.; Salli, E.; Kortesniemi, M.; Uusi-Simola, J.; Mäkitie, A.; et al. Boron Neutron Capture Therapy in the Treatment of Locally Recurred Head and Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Kankaanranta, L.; Seppälä, T.; Koivunoro, H.; Saarilahti, K.; Atula, T.; Collan, J.; Salli, E.; Kortesniemi, M.; Uusi-Simola, J.; Välimäki, P.; et al. Boron Neutron Capture Therapy in the Treatment of Locally Recurred Head-and-Neck Cancer: Final Analysis of a Phase I/II Trial. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e67–e75. [Google Scholar] [CrossRef]
- Kankaanranta, L.; Seppälä, T.; Koivunoro, H.; Välimäki, P.; Beule, A.; Collan, J.; Kortesniemi, M.; Uusi-Simola, J.; Kotiluoto, P.; Auterinen, I.; et al. L-Boronophenylalanine-Mediated Boron Neutron Capture Therapy for Malignant Glioma Progressing after External Beam Radiation Therapy: A Phase i Study. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 369–376. [Google Scholar] [CrossRef]
- Koivunoro, H.; Hippeläinen, E.; Auterinen, I.; Kankaanranta, L.; Kulvik, M.; Laakso, J.; Seppälä, T.; Savolainen, S.; Joensuu, H. Biokinetic Analysis of Tissue Boron (10B) Concentrations of Glioma Patients Treated with BNCT in Finland. Appl. Radiat. Isot. 2015, 106, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Cruickshank, G.S.; Ngoga, D.; Detta, A.; Green, S.; James, N.D.; Wojnecki, C.; Doran, J.; Hardie, J.; Chester, M.; Graham, N.; et al. A Cancer Research UK Pharmacokinetic Study of BPA-Mannitol in Patients with High Grade Glioma to Optimise Uptake Parameters for Clinical Trials of BNCT. Appl. Radiat. Isot. 2009, 67, S31–S33. [Google Scholar] [CrossRef]
- Yong, Z.; Song, Z.; Zhou, Y.; Liu, T.; Zhang, Z.; Zhao, Y.; Chen, Y.; Jin, C.; Chen, X.; Lu, J.; et al. Boron Neutron Capture Therapy for Malignant Melanoma: First Clinical Case Report in China. Chin. J. Cancer Res. 2016, 28, 634. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.-W.; Chen, Y.-W.; Ho, C.-Y.; Hsueh Liu, Y.-W.; Chou, F.-I.; Liu, Y.-H.; Liu, H.-M.; Peir, J.-J.; Jiang, S.-H.; Chang, C.-W.; et al. Fractionated Boron Neutron Capture Therapy in Locally Recurrent Head and Neck Cancer: A Prospective Phase I/II Trial. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 396–403. [Google Scholar] [CrossRef]
- Wang, L.W.; Liu, Y.W.H.; Chou, F.I.; Jiang, S.H. Clinical Trials for Treating Recurrent Head and Neck Cancer with Boron Neutron Capture Therapy Using the Tsing-Hua Open Pool Reactor. Cancer Commun. 2018, 38, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.-C.; Chuang, K.-S.; Hsueh Liu, Y.-W.; Lin, T.-Y.; Teng, Y.-C.; Wang, L.-W. A Comparison of Dose Distributions in Gross Tumor Volume between Boron Neutron Capture Therapy Alone and Combined Boron Neutron Capture Therapy plus Intensity Modulation Radiation Therapy for Head and Neck Cancer. PLoS ONE 2019, 14, e0210626. [Google Scholar] [CrossRef]
- Lan, T.-L.; Chou, F.-I.; Lin, K.-H.; Pan, P.-S.; Lee, J.-C.; Huang, W.-S.; Liu, Y.-M.; Chao, Y.; Chen, Y.-W. Using Salvage Boron Neutron Capture Therapy (BNCT) for Recurrent Malignant Brain Tumors in Taiwan. Appl. Radiat. Isot. 2020, 160, 109105. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-W.; Lee, Y.-Y.; Lin, C.-F.; Pan, P.-S.; Chen, J.-K.; Wang, C.-W.; Hsu, S.-M.; Kuo, Y.-C.; Lan, T.-L.; Hsu, S.P.C.; et al. Salvage Boron Neutron Capture Therapy for Malignant Brain Tumor Patients in Compliance with Emergency and Compassionate Use: Evaluation of 34 Cases in Taiwan. Biology 2021, 10, 334. [Google Scholar] [CrossRef]
- Ree, A.H.; Redalen, K.R. Personalized Radiotherapy: Concepts, Biomarkers and Trial Design. Br. J. Radiol. 2015, 88, 20150009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Formenti, S.C.; Demaria, S. Combining Radiotherapy and Cancer Immunotherapy: A Paradigm Shift. J. Natl. Cancer Inst. 2013, 105, 256–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giaccia, A.J. Molecular Radiobiology: The State of the Art. J. Clin. Oncol. 2014, 32, 2871–2878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanduleanu, S.; van der Wiel, A.M.A.; Lieverse, R.I.Y.; Marcus, D.; Ibrahim, A.; Primakov, S.; Wu, G.; Theys, J.; Yaromina, A.; Dubois, L.J.; et al. Hypoxia PET Imaging with [18F]-HX4—A Promising Next-Generation Tracer. Cancers 2020, 12, 1322. [Google Scholar] [CrossRef]
- McKinley, E.T.; Ayers, G.D.; Smith, R.A.; Saleh, S.A.; Zhao, P.; Washington, M.K.; Coffey, R.J.; Manning, H.C. Limits of [18F]-FLT PET as a Biomarker of Proliferation in Oncology. PLoS ONE 2013, 8, e58938. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S. PET Radiopharmaceuticals for Personalized Medicine. Curr. Drug Targets 2016, 17, 1894–1907. [Google Scholar] [CrossRef]
- Jiménez-Ortega, E.; Ureba, A.; Vargas, A.; Baeza, J.A.; Wals-Zurita, A.; García-Gómez, F.J.; Barbeiro, A.R.; Leal, A. Dose Painting by Means of Monte Carlo Treatment Planning at the Voxel Level. Phys. Med. 2017, 42, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Bentzen, S.M. Dose Painting and Theragnostic Imaging: Towards the Prescription, Planning and Delivery of Biologically Targeted Dose Distributions in External Beam Radiation Oncology. In Radiation Oncology Advances; Bentzen, S.M., Harari, P.M., Tome, W.A., Mehta, M.P., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; Volume 139, pp. 40–61. [Google Scholar]
- Jiménez-Ortega, E.; Ureba, A.; Baeza, J.A.; Barbeiro, A.R.; Balcerzyk, M.; Parrado-Gallego, Á.; Wals-Zurita, A.; García-Gómez, F.J.; Leal, A. Accurate, Robust and Harmonized Implementation of Morpho-Functional Imaging in Treatment Planning for Personalized Radiotherapy. PLoS ONE 2019, 14, e0210549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carpano, M.; Santa Cruz, G.; Rodriguez, C.; Nievas, S.; Olivera, M.S.; Perona, M.; Boggio, E.; Longhino, J.; Pisarev, M.; Juvenal, G.; et al. Experimental Studies for the Personalized Application of Boron Neutron Capture Therapy to the Treatment of Cutaneous Melanoma. Ther. Radiol. Oncol. 2021, 5, 8. [Google Scholar] [CrossRef]
- Mauri, P.L.; Basilico, F. Proteomic Investigations for Boron Neutron Capture Therapy. In Neutron Capture Therapy; Springer: Berlin/Heidelberg, Germany, 2012; pp. 189–200. [Google Scholar]
- Keener, A.B. Making Radiation Oncology More Personal. Nature 2020, 585, S10–S12. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skwierawska, D.; López-Valverde, J.A.; Balcerzyk, M.; Leal, A. Clinical Viability of Boron Neutron Capture Therapy for Personalized Radiation Treatment. Cancers 2022, 14, 2865. https://doi.org/10.3390/cancers14122865
Skwierawska D, López-Valverde JA, Balcerzyk M, Leal A. Clinical Viability of Boron Neutron Capture Therapy for Personalized Radiation Treatment. Cancers. 2022; 14(12):2865. https://doi.org/10.3390/cancers14122865
Chicago/Turabian StyleSkwierawska, Dominika, José Antonio López-Valverde, Marcin Balcerzyk, and Antonio Leal. 2022. "Clinical Viability of Boron Neutron Capture Therapy for Personalized Radiation Treatment" Cancers 14, no. 12: 2865. https://doi.org/10.3390/cancers14122865