
Hobnail Papillary Thyroid Carcinoma, A Systematic Review and Meta-Analysis

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
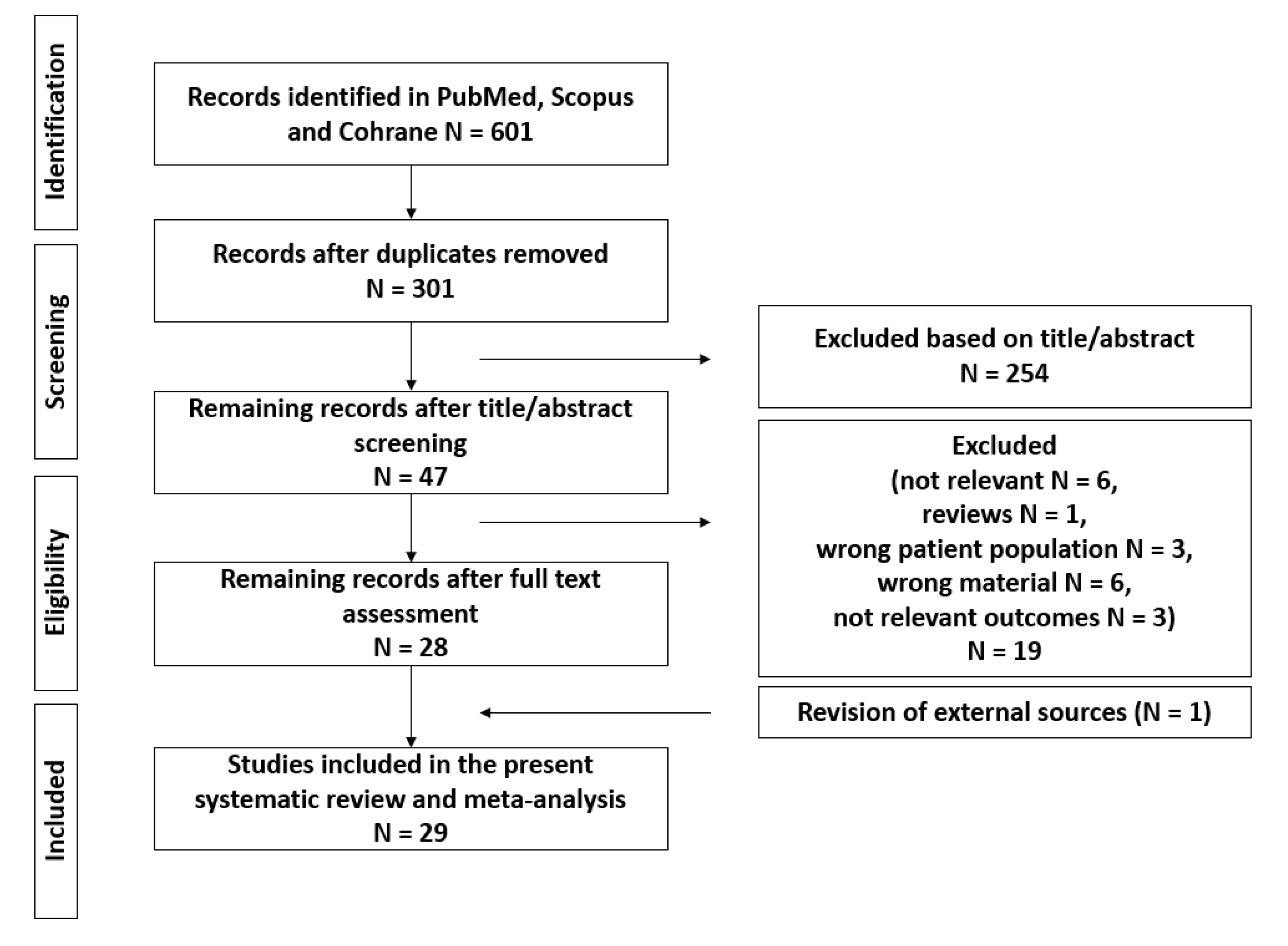
2. Materials and Methods
3. Results
3.1. Descriptive Characteristics of the Included Studies
3.2. Primary Meta-Analysis
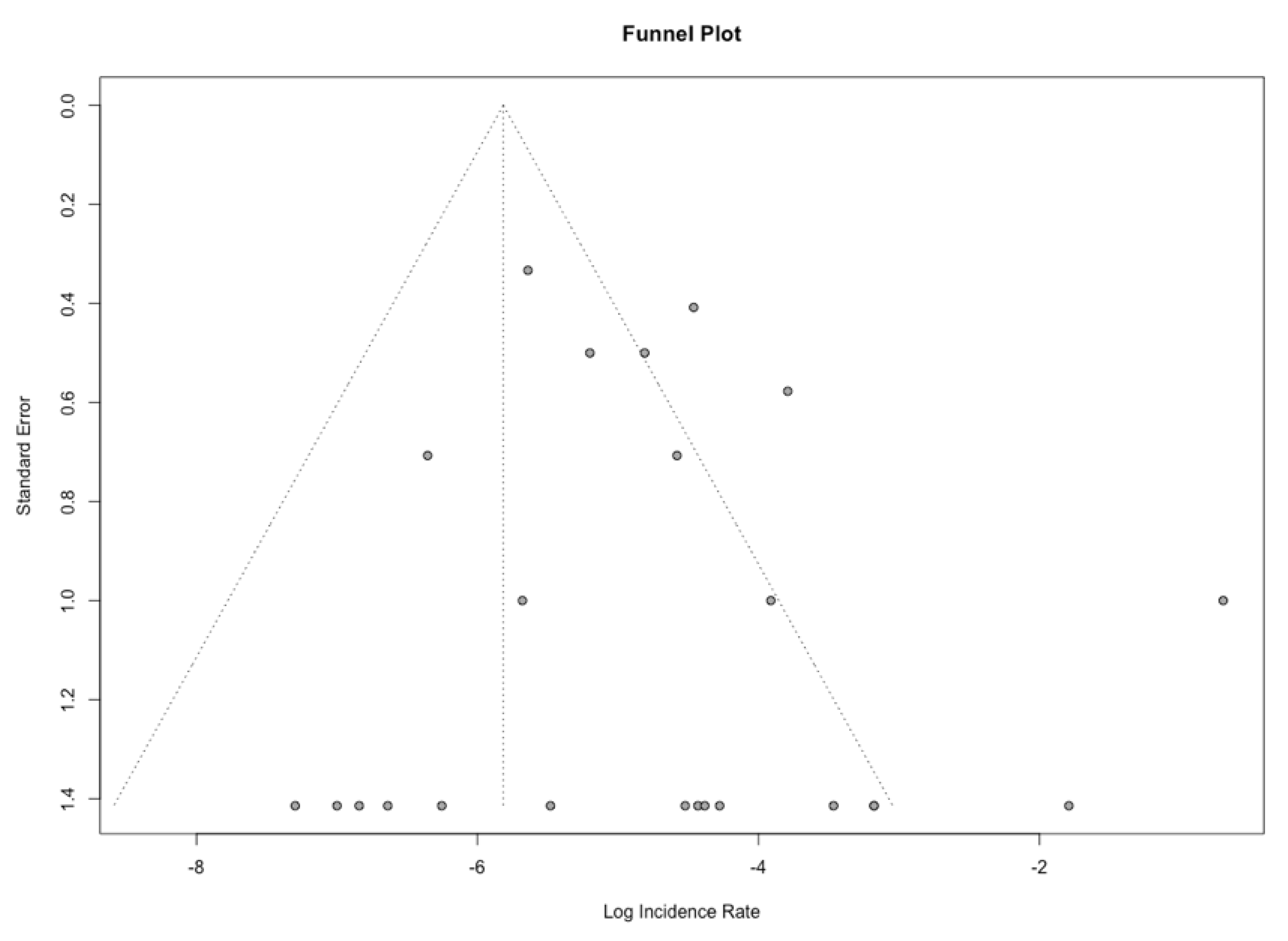
3.3. Exploratory Analyses
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- SEER. Cancer. Available online: https://seer.cancer.gov/statfacts/html/thyro.html (accessed on 31 December 2021).
- Miranda-Filho, A.; Lortet-Tieulent, J.; Bray, F.; Cao, B.; Franceschi, S.; Vaccarella, S.; Maso, L.D. Thyroid cancer incidence trends by histology in 25 countries: A population-based study. Lancet Diabetes Endocrinol. 2021, 9, 225–234. [Google Scholar] [CrossRef]
- Ito, Y.; Miyauchi, A.; Kihara, M.; Fukushima, M.; Higashiyama, T.; Miya, A. Overall Survival of Papillary Thyroid Carcinoma Patients: A Single-Institution Long-Term Follow-Up of 5897 Patients. World J. Surg. 2018, 42, 615–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baloch, Z.W.; Asa, S.L.; Barletta, J.A.; Ghossein, R.A.; Juhlin, C.C.; Jung, C.K.; LiVolsi, V.A.; Papotti, M.G.; Sobrinho-Simoes, M.; Tallini, G.; et al. Overview of the 2022 WHO Classification of Thyroid Neoplasms. Endocr. Pathol. 2022, 33, 27–63. [Google Scholar] [CrossRef] [PubMed]
- Coca-Pelaz, A.; Shah, J.P.; Hernandez-Prera, J.C.; Ghossein, R.A.; Rodrigo, J.P.; Hartl, D.M.; Olsen, K.D.; Shaha, A.R.; Zafereo, M.; Suarez, C.; et al. Papillary Thyroid Cancer-Aggressive Variants and Impact on Management: A Narrative Review. Adv. Ther. 2020, 37, 3112–3128. [Google Scholar] [CrossRef]
- Nath, M.C.; Erickson, L.A. Aggressive Variants of Papillary Thyroid Carcinoma: Hobnail, Tall Cell, Columnar, and Solid. Adv. Anat. Pathol. 2018, 25, 172–179. [Google Scholar] [CrossRef]
- Silver, C.E.; Owen, R.P.; Rodrigo, J.P.; Rinaldo, A.; Devaney, K.O.; Ferlito, A. Aggressive variants of papillary thyroid carcinoma. Head Neck 2011, 33, 1052–1059. [Google Scholar] [CrossRef]
- Bai, Y.; Kakudo, K.; Nakamura, M.; Ozaki, T.; Li, Y.; Liu, Z.; Mori, I.; Miyauchi, A.; Zhou, G. Loss of cellular polarity/cohesiveness in the invasive front of papillary thyroid carcinoma and periostin expression. Cancer Lett. 2009, 281, 188–195. [Google Scholar] [CrossRef]
- Kakudo, K.; Tang, W.; Ito, Y.; Mori, I.; Nakamura, Y.; Miyauchi, A. Papillary carcinoma of the thyroid in Japan: Subclassification of common type and identification of low risk group. J. Clin. Pathol. 2004, 57, 1041–1046. [Google Scholar] [CrossRef] [Green Version]
- Asioli, S.; Erickson, L.A.; Sebo, T.J.; Zhang, J.; Jin, L.; Thompson, G.B.; Lloyd, R.V. Papillary thyroid carcinoma with prominent hobnail features: A new aggressive variant of moderately differentiated papillary carcinoma. A clinicopathologic, immunohistochemical, and molecular study of eight cases. Am. J. Surg. Pathol. 2010, 34, 44–52. [Google Scholar] [CrossRef]
- Asioli, S.; Erickson, L.A.; Righi, A.; Lloyd, R.V. Papillary thyroid carcinoma with hobnail features: Histopathologic criteria to predict aggressive behavior. Hum. Pathol. 2013, 44, 320–328. [Google Scholar] [CrossRef]
- Asioli, S.; Maletta, F.; Pagni, F.; Pacchioni, D.; Vanzati, A.; Mariani, S.; Palestini, N.; Lloyd, R.V.; Sapino, A. Cytomorphologic and molecular features of hobnail variant of papillary thyroid carcinoma: Case series and literature review. Diagn. Cytopathol. 2014, 42, 78–84. [Google Scholar] [CrossRef]
- Lino-Silva, L.S.; Dominguez-Malagon, H.R.; Caro-Sanchez, C.H.; Salcedo-Hernandez, R.A. Thyroid gland papillary carcinomas with “micropapillary pattern”, a recently recognized poor prognostic finding: Clinicopathologic and survival analysis of 7 cases. Hum. Pathol. 2012, 43, 1596–1600. [Google Scholar] [CrossRef]
- Watutantrige-Fernando, S.; Vianello, F.; Barollo, S.; Bertazza, L.; Galuppini, F.; Cavedon, E.; Censi, S.; Benna, C.; Ide, E.C.; Parisi, A.; et al. The Hobnail Variant of Papillary Thyroid Carcinoma: Clinical/Molecular Characteristics of a Large Monocentric Series and Comparison with Conventional Histotypes. Thyroid 2018, 28, 96–103. [Google Scholar] [CrossRef]
- Amacher, A.M.; Goyal, B.; Lewis, J.S., Jr.; El-Mofty, S.K.; Chernock, R.D. Prevalence of a hobnail pattern in papillary, poorly differentiated, and anaplastic thyroid carcinoma: A possible manifestation of high-grade transformation. Am. J. Surg. Pathol. 2015, 39, 260–265. [Google Scholar] [CrossRef]
- Ragazzi, M.; Torricelli, F.; Donati, B.; Ciarrocchi, A.; Biase, D.D.; Tallini, G.; Zanetti, E.; Bisagni, A.; Kuhn, E.; Giordano, D.; et al. Coexisting well-differentiated and anaplastic thyroid carcinoma in the same primary resection specimen: Immunophenotypic and genetic comparison of the two components in a consecutive series of 13 cases and a review of the literature. Virchows Arch. 2021, 478, 265–281. [Google Scholar] [CrossRef]
- Lin, J.S.; Murad, M.H.; Leas, B.; Treadwell, J.R.; Chou, R.; Ivlev, I.; Kansagara, D. A Narrative Review and Proposed Framework for Using Health System Data with Systematic Reviews to Support Decision-making. J. Gen. Intern. Med. 2020, 35, 1830–1835. [Google Scholar] [CrossRef]
- Bancos, I.; Atkinson, E.; Eng, C.; Young, W.F., Jr.; Neumann, H.P.H.; International Pheochromocytoma; Pregnancy Study Group. Maternal and fetal outcomes in phaeochromocytoma and pregnancy: A multicentre retrospective cohort study and systematic review of literature. Lancet Diabetes Endocrinol. 2021, 9, 13–21. [Google Scholar] [CrossRef]
- Wong, K.S.; Chen, T.Y.; Higgins, S.E.; Howitt, B.E.; Lorch, J.H.; Alexander, E.K.; Marqusee, E.; Cho, N.L.; Nehs, M.A.; Doherty, G.M.; et al. A potential diagnostic pitfall for hobnail variant of papillary thyroid carcinoma. Histopathology 2020, 76, 707–713. [Google Scholar] [CrossRef]
- Pedder, H.; Saari, G.; Keeney, E.; Nunes, V. Data extraction for complex meta-analysis (DECiMAL) guide. Syst. Rev. 2016, 5, 212. [Google Scholar] [CrossRef] [Green Version]
- Stijnen, T.; Hamza, T.H.; Ozdemir, P. Random effects meta-analysis of event outcome in the framework of the generalized linear mixed model with applications in sparse data. Stat. Med. 2010, 29, 3046–3067. [Google Scholar] [CrossRef]
- Lin, L.; Chu, H. Meta-analysis of Proportions Using Generalized Linear Mixed Models. Epidemiology 2020, 31, 713–717. [Google Scholar] [CrossRef]
- Schwarzer, G.; Chemaitelly, H.; Abu-Raddad, L.J.; Rücker, G. Seriously misleading results using inverse of Freeman-Tukey double arcsine transformation in meta-analysis of single proportions. Res. Synth. Methods 2019, 10, 476–483. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Spiegelhalter, D.J. A re-evaluation of random-effects meta-analysis. J. R. Stat. Soc. Ser. A 2009, 172, 137–159. [Google Scholar] [CrossRef] [Green Version]
- Donaldson, L.B.; Yan, F.; Morgan, P.F.; Kaczmar, J.M.; Fernandes, J.K.; Nguyen, S.A.; Jester, R.L.; Day, T.A. Hobnail variant of papillary thyroid carcinoma: A systematic review and meta-analysis. Endocrine 2021, 72, 27–39. [Google Scholar] [CrossRef]
- Aliyev, E.; Ladra-Gonzalez, M.J.; Sanchez-Ares, M.; Abdulkader-Nallib, I.; Piso-Neira, M.; Rodriguez-Carnero, G.; Vieiro-Balo, P.; Perez-Becerra, R.; Gude-Sampedro, F.; Barreiro-Morandeira, F.; et al. Thyroid Papillary Microtumor: Validation of the (Updated) Porto Proposal Assessing Sex Hormone Receptor Expression and Mutational BRAF Gene Status. Am. J. Surg. Pathol. 2020, 44, 1161–1172. [Google Scholar] [CrossRef]
- Agarwal, S.; Sadiq, Q.; Ortanca, I. Hobnail cells in encapsulated papillary thyroid carcinoma: Report of 2 cases with immunohistochemical and molecular findings and literature analysis. Pathol. Res. Pract. 2020, 216, 152678. [Google Scholar] [CrossRef]
- Al-Yahri, O.; Abdelaal, A.; Ansari, W.E.; Farghaly, H.; Murshed, K.; Zirie, M.A.; Hassan, M.S.A. First ever case report of co-occurrence of hobnail variant of papillary thyroid carcinoma and intrathyroid parathyroid adenoma in the same thyroid lobe. Int. J. Surg. Case Rep. 2020, 70, 40–52. [Google Scholar] [CrossRef]
- Arrangoiz, R.; Moran, R.; Corona, L.; Boy, J.; Cordera, F.; Caba, D.; Juarez, M.M.; Moreno, E.; Luque-de-Leon, E. Papillary Thyroid Carcinoma Hobnail Variant: A Report of Two Cases and Literature Review. Am. J. Otolaryngol. Head Neck Surg. 2020, 3, 1087. [Google Scholar]
- Bellevicine, C.; Cozzolino, I.; Malapelle, U.; Zeppa, P.; Troncone, G. Cytological and molecular features of papillary thyroid carcinoma with prominent hobnail features: A case report. Acta Cytol. 2012, 56, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Cameselle-Teijeiro, J.M.; Rodriguez-Perez, I.; Celestino, R.; Eloy, C.; Piso-Neira, M.; Abdulkader-Nallib, I.; Soares, P.; Sobrinho-Simoes, M. Hobnail Variant of Papillary Thyroid Carcinoma: Clinicopathologic and Molecular Evidence of Progression to Undifferentiated Carcinoma in 2 Cases. Am. J. Surg. Pathol. 2017, 41, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Cruz, V.D.; Lopez, J.; Lifante, J.C.; Decaussin-Petrucci, M. Carcinome papillaire de la thyroïde à cellules en clous de tapissier. Ann. Pathol. 2020, 41, 201–206. [Google Scholar] [CrossRef]
- Graef, A.D.; Heede, K.V.D.; Meert, V.; Slycke, S.V. Papillary thyroid carcinoma with hobnail features showing rapid progression and therapy resistance. Acta Chir. Belg. 2021, 121, 77–85. [Google Scholar] [CrossRef]
- Ieni, A.; Barresi, V.; Cardia, R.; Licata, L.; Bari, F.D.; Benvenga, S.; Tuccari, G. The micropapillary/hobnail variant of papillary thyroid carcinoma: A review of series described in the literature compared to a series from one southern Italy pathology institution. Rev. Endocr. Metab. Disord. 2016, 17, 521–527. [Google Scholar] [CrossRef]
- Ito, Y.; Hirokawa, M.; Hayashi, T.; Ota, H.; Oshita, M.; Kihara, M.; Miya, A.; Miyauchi, A. Case report: Exceptionally rapid growth character of hobnail variant of papillary thyroid carcinoma: A report of four cases. Endocr. J. 2020, 67, 1047–1053. [Google Scholar] [CrossRef]
- Liu, J.; Brown, R.E.; Rubenfeld, S.; Karni, R.J. Papillary Thyroid Carcinoma with Prominent Hobnail Features Diagnosed Preoperatively by Fine Needle Aspiration and Demonstrating Constitutive Activation of mTOR Signaling Pathway: A Case Report. J. Clin. Exp. Pathol. 2013, 3, 152. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Kim, Y.; Jeon, S.; Bae, J.S.; Jung, S.L.; Jung, C.K. Cytologic, clinicopathologic, and molecular features of papillary thyroid carcinoma with prominent hobnail features: 10 case reports and systematic literature review. Int. J. Clin. Exp. Pathol. 2015, 8, 7988–7997. [Google Scholar]
- Lilo, M.T.; Bishop, J.A.; Ali, S.Z. Hobnail variant of papillary thyroid carcinoma: A case with an unusual presentation. Diagn. Cytopathol. 2017, 45, 754–756. [Google Scholar] [CrossRef]
- Lubitz, C.C.; Economopoulos, K.P.; Pawlak, A.C.; Lynch, K.; Dias-Santagata, D.; Faquin, W.C.; Sadow, P.M. Hobnail variant of papillary thyroid carcinoma: An institutional case series and molecular profile. Thyroid 2014, 24, 958–965. [Google Scholar] [CrossRef]
- Morandi, L.; Righi, A.; Maletta, F.; Rucci, P.; Pagni, F.; Gallo, M.; Rossi, S.; Caporali, L.; Sapino, A.; Lloyd, R.V.; et al. Somatic mutation profiling of hobnail variant of papillary thyroid carcinoma. Endocr.-Relat. Cancer 2017, 24, 107–117. [Google Scholar] [CrossRef] [Green Version]
- Naciu, A.M.; Verri, M.; Crescenzi, A.; Taffon, C.; Longo, F.; Frasca, L.; Tabacco, G.; Monte, L.; Palermo, A.; Crucitti, P.; et al. Hobnail variant of papillary thyroid carcinoma showing goiter-like presentation and rapid growth. Endocrinol. Diabetes Metab. Case Rep. 2021, 2021. [Google Scholar] [CrossRef]
- Teng, L.; Deng, W.; Lu, J.; Zhang, J.; Ren, X.; Duan, H.; Chuai, S.; Duan, F.; Gao, W.; Lu, T.; et al. Hobnail variant of papillary thyroid carcinoma: Molecular profiling and comparison to classical papillary thyroid carcinoma, poorly differentiated thyroid carcinoma and anaplastic thyroid carcinoma. Oncotarget 2017, 8, 22023–22033. [Google Scholar] [CrossRef]
- Woodford, R.L.; Nikiforov, Y.E.; Hunt, J.L.; Bellizzi, A.M.; Zhang, X.; Mills, S.E.; Stelow, E.B. Encapsulated papillary oncocytic neoplasms of the thyroid: Morphologic, immunohistochemical, and molecular analysis of 18 cases. Am. J. Surg. Pathol. 2010, 34, 1582–1590. [Google Scholar] [CrossRef]
- Mehrotra, S.; Lapadat, R.; Barkan, G.A.; Pambuccian, S.E. “Teardrop”, “comet”, and “bowling-pin” cells in a hobnail variant of papillary thyroid carcinoma fine needle aspirate. Diagn. Cytopathol. 2019, 47, 839–842. [Google Scholar] [CrossRef]
- Motosugi, U.; Murata, S.; Nagata, K.; Yasuda, M.; Shimizu, M. Thyroid papillary carcinoma with micropapillary and hobnail growth pattern: A histological variant with intermediate malignancy? Thyroid 2009, 19, 535–537. [Google Scholar] [CrossRef]
- Schwock, J.; Desai, G.; Devon, K.M.; Mete, O.; Dube, V. Hobnail-variant of papillary thyroid carcinoma in liquid-based cytology. Diagn. Cytopathol. 2015, 43, 990–992. [Google Scholar] [CrossRef]
- Poma, A.M.; Macerola, E.; Proietti, A.; Vignali, P.; Sparavelli, R.; Torregrossa, L.; Matrone, A.; Basolo, A.; Elisei, R.; Santini, F.; et al. Clinical-Pathological Features and Treatment Outcome of Patients With Hobnail Variant Papillary Thyroid Carcinoma. Front. Endocrinol. 2022, 13, 842424. [Google Scholar] [CrossRef]
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in Thyroid Cancer Incidence and Mortality in the United States, 1974–2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Viola, D.; Elisei, R.; Bendlova, B.; Yip, L.; Mian, C.; Vianello, F.; Tuttle, R.M.; et al. Association between BRAF V600E mutation and mortality in patients with papillary thyroid cancer. JAMA 2013, 309, 1493–1501. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Chen, T.; Zeng, W.; Wang, S.; Xiong, Y.; Liu, Z.; Huang, T. Reevaluating the prognostic significance of male gender for papillary thyroid carcinoma and microcarcinoma: A SEER database analysis. Sci. Rep. 2017, 7, 11412. [Google Scholar] [CrossRef]
- Schonfeld, S.J.; Neta, G.; Sturgis, E.M.; Pfeiffer, R.M.; Hutchinson, A.A.; Xu, L.; Wheeler, W.; Guenel, P.; Rajaraman, P.; Vathaire, F.D.; et al. Common genetic variants in sex hormone pathway genes and papillary thyroid cancer risk. Thyroid 2012, 22, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Tang, J.; Kong, D.; Cui, Q.; Wang, K.; Gong, Y.; Wu, G. Impact of Gender and Age on the Prognosis of Differentiated Thyroid Carcinoma: A Retrospective Analysis Based on SEER. Horm. Cancer 2018, 9, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Jonklaas, J.; Nogueras-Gonzalez, G.; Munsell, M.; Litofsky, D.; Ain, K.B.; Bigos, S.T.; Brierley, J.D.; Cooper, D.S.; Haugen, B.R.; Ladenson, P.W.; et al. The impact of age and gender on papillary thyroid cancer survival. J. Clin. Endocrinol. Metab. 2012, 97, E878–E887. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Dai, W.; Liang, Y.; Xia, N. Impact of Age on the Prognosis of Papillary Thyroid Carcinoma. Arch. Iran Med. 2020, 23, 169–174. [Google Scholar] [PubMed]
- Kaliszewski, K.; Diakowska, D.; Nowak, L.; Wojtczak, B.; Rudnicki, J. The age threshold of the 8th edition AJCC classification is useful for indicating patients with aggressive papillary thyroid cancer in clinical practice. BMC Cancer 2020, 20, 1166. [Google Scholar] [CrossRef]
- Davies, L.; Welch, H.G. Current thyroid cancer trends in the United States. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 317–322. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | N | Sex (m:f) | Age Range | Size Range (mm) | Hc >30% | Ete | Lvi | Histological Combinations | Fu (Months Range) | Outcome | BRAF mut. | Dm | Ln |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Agrawal 2020 [27] | 2 | 1:1 | 22–68 | 22–35 | 1/2 | 0/2 | 0/2 | PTC | 6–10 | 2/2 AND | 2/2 | 0/2 | 0/2 |
| Al-Yahri 2020 [28] | 1 | 0:1 | 61 | 20 | NA | 0/1 | 0/1 | NA | 12 | 1/1 AND | 1/1 | 0/1 | 0/1 |
| Aliyev 2020 [26] | 1 | 1:0 | 75 | 19 | 1/1 | 1/1 | 1/1 | PTC, FV | NA | NA | NA | NA | 1/1 |
| Amacher 2015 [15] | 11 | 7:4 | 22–76 | 9–65 | 2/6 | 4/5 | NA | PTC, PDC, ATC, TC, CC | 3.6–228 | 3/11 AND, 2/11 AWD, 6/11 DOD | 2/4 | 4/7 | 10/10 |
| Arrangoiz 2020 [29] | 2 | 1:1 | 31–33 | 25–27 | 1/2 | NA | NA | PTC | 18–24 | 2/2 AND | NA | 0/2 | NA |
| Asioli 2013 [11] | 24 | 6:18 | 28–78 | 10–70 | 12/24 | NA | 17/24 | NA | 4–274 | 12/24 AND, 3/24 AWD, 8/24 DOD, 1/24 DOC | NA | 10/23 | 13/24 |
| Asioli 2014 [12] | 5 | 2:3 | 27–86 | 20–90 | 2/5 | NA | 4/5 | PTC, FV | 2–24 | 4/5 AND, 1/5 AWD | 3/5 | 0/5 | 3/5 |
| Bellevicine 2012 [30] | 1 | 1:0 | 57 | 20 | NA | NA | NA | PTC | NA | NA | 1/1 | NA | NA |
| Cameselle-Teijeiro 2017 [31] | 2 | 1:1 | 53–62 | 17–65 | 2/2 | 2/2 | 2/2 | PTC, PDC, FV, ST | 67–128 | 2/2 DOD | 1/2 | 2/2 | 2/2 |
| Da Cruz 2020 [32] | 1 | 1:0 | 67 | 49 | 1/1 | NA | 1/1 | PDC, ATC | 50 | 1/1 DOD | NA | 1/1 | 1/1 |
| De Graef 2021 [33] | 1 | 0:1 | 38 | entire gland | 1/1 | 1/1 | NA | PTC, FV, ST | 2 | 1/1 DOD | 1/1 | 1/1 | 1/1 |
| Ieni 2016 [34] | 8 | 2:6 | 47–69 | 10–32 | 8/8 | NA | 4/8 | NA | 39–60 | 8/8 AND | 3/8 | 0/8 | 2/8 |
| Ito 2020 [35] | 4 | 0:4 | 70–79 | 19–42 | 4/4 | 2/2 | 2/2 | PTC, TC | 5–18 | 3/4 AND, 1/4 AWD | NA | 1/4 | 4/4 |
| Lee 2015 [37] | 10 | 4:6 | 32–68 | 6–40 | 10/10 | 7/10 | 8/10 | PTC, FV, TC | 9–28 | 9/10 AND, 1/10 AWD | 8/10 | 0/10 | 8/10 |
| Lilo 2017 [38] | 1 | 1:0 | 81 | 14 | 1/1 | 1/1 | 1/1 | NA | NA | NA | NA | NA | NA |
| Lino-Silva 2012 [13] | 7 | 4:3 | 27–68 | 39–50 | 0/7 | NA | 5/7 | NA | 63–84 | 3/7 AWD, 4/7 DOD | NA | 3/7 | 5/7 |
| Liu 2013 [36] | 1 | 0:1 | 17 | 32 | 1/1 | 1/1 | 1/1 | PTC, FV, ST | 12 | 1/1 AWD | NA | 0/1 | 1/1 |
| Lubitz 2014 [39] | 12 | 3:9 | 21–80 | 5–65 | 10/10 | 7/12 | 5/12 | PTC, TC, ATC | 12–57 | 7/11 AND, 3/11 AWD, 1/11 DOD | 8/10 | 3/12 | 10/12 |
| Mehrotra 2019 [44] | 1 | 0:1 | 66 | 53 | 1/1 | 0/1 | 1/1 | PTC, FV, TC | NA | NA | NA | 0/1 | 1/1 |
| Morandi 2017 [40] | 18 | 4:14 | 3 < 45, 15 > 45 | 12 < 40, 6 > 40 | 18/18 | 16/18 | 18/18 | NA | 7–128 | 7/18 AND, 7/18 AWD, 4/18 DOD | 12/18 | 8/18 | NA |
| Motosugi 2009 [45] | 1 | 1:0 | 57 | 55 | 1/1 | 1/1 | 0/1 | NA | NA | NA | 0/1 | 0/1 | |
| Naciu 2021 [41] | 1 | 1:0 | 47 | entire gland | 1/1 | 1/1 | NA | PTC | 36 | 1/1 AND | 1/1 | 0/1 | 0/1 |
| Poma 2022 [47] | 99 | 41:58 | 49.8 (15.9) * | 18 (13–24) ** | 34/99 | 40/99 | 49/99 | PTC, TCV, ST, CLC | 12 | 19/39 AND, 20/39 AWD | 69/88 | NA | 32/99 |
| Ragazzi 2020 [16] | 1 | 0:1 | 71 | 50 | 0/1 | NA | NA | PTC, ATC | 3 | 1/1 AWD | 1/1 | 1/1 | 1/1 |
| Schwock 2015 [46] | 1 | 0:1 | 26 | 21 | 1/1 | NA | NA | PTC, TC | NA | NA | NA | NA | 1/1 |
| Teng 2017 [42] | 18 | 5:13 | 23–78 | 10–50 | 18/18 | 6/18 | 2/18 | PTC, TCV, CC | 12–101 | 13/16 AND, 1/16 AWD, 1/16 DOD, 1/16 DOC | 16/17 | 2/18 | 10/17 |
| Watutantrige-Fernando 2018 [14] | 25 | 10:15 | 24–73 | 7–80 | 16/25 | NA | 24/25 | NA | 13–67 | 13/19 AND, 6/19 AWD | 14/24 | 3/10 | 17/24 |
| Wong 2020 [19] | 7 | 2:5 | 48–92 | 25–80 | 6/7 | 5/7 | NA | PTC, ATC, TC | median 23 | 3/7 AND, 1/7 AWD, 3/7 DOD | 3/3 | 3/7 | 6/7 |
| Woodford 2010 [43] | 18 | 2:16 | 14–86 | NA | NA | 2/18 | 8/18 | PTC, FV | 3–166 | 12/13 AND, 1/13 AWD | 0/9 | 0/18 | 1/13 |
| current study | 6 | 5:1 | 31–53 | 11–50 | 1/5 | 3/6 | 2/5 | PTC, PDC, TC, FV | 5–106 | 2/5 AND, 3/5 AWD | 2/5 | 1/5 | 3/5 |
| Summary of all studies | 290 | 105 (36%): 185 (64%) | 14–92 (51.3) | 5–90 (29.8) | 155 (59%) | 101 (49%) | 155 (59%) | PTC 125 (63%), 2 + S 46 (23%), PDC/ATC 4 (2%), TC 18 (9%), CLC 1 (0.5%), NOS 2 (1%) | 2–274 (42.6) | AND 121 (58%), AWD 55 (26%), DOD 31 (14.8%), DOC < 0.1% | 150 (71%) | 43 (26%) | 135 (52%) |
| Characteristic | OR | 95% CI | p-Value |
|---|---|---|---|
| Size | 1.03 | 1.00, 1.06 | 0.032 |
| HPTC 30% No | - | - | - |
| HPTC 30% Yes | 0.76 | 0.26, 2.28 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spyroglou, A.; Kostopoulos, G.; Tseleni, S.; Toulis, K.; Bramis, K.; Mastorakos, G.; Konstadoulakis, M.; Vamvakidis, K.; Alexandraki, K.I. Hobnail Papillary Thyroid Carcinoma, A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2785. https://doi.org/10.3390/cancers14112785
Spyroglou A, Kostopoulos G, Tseleni S, Toulis K, Bramis K, Mastorakos G, Konstadoulakis M, Vamvakidis K, Alexandraki KI. Hobnail Papillary Thyroid Carcinoma, A Systematic Review and Meta-Analysis. Cancers. 2022; 14(11):2785. https://doi.org/10.3390/cancers14112785
Chicago/Turabian StyleSpyroglou, Ariadni, Georgios Kostopoulos, Sofia Tseleni, Konstantinos Toulis, Konstantinos Bramis, George Mastorakos, Manousos Konstadoulakis, Kyriakos Vamvakidis, and Krystallenia I. Alexandraki. 2022. "Hobnail Papillary Thyroid Carcinoma, A Systematic Review and Meta-Analysis" Cancers 14, no. 11: 2785. https://doi.org/10.3390/cancers14112785