
Cost-Effectiveness of Immune Checkpoint Inhibitors in Urothelial Carcinoma—A Review

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
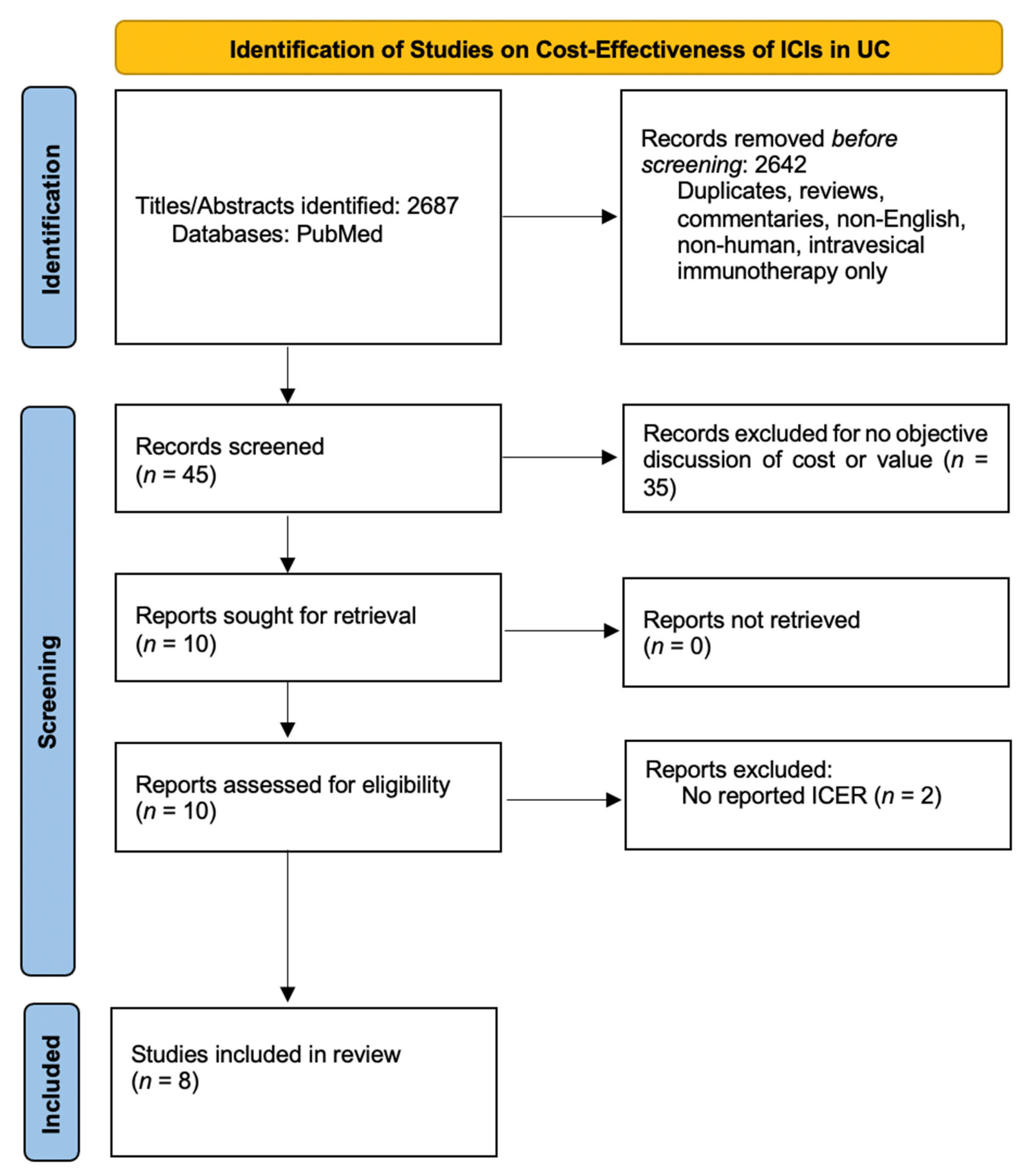
2.1. Search Strategy
2.2. Data Selection
2.3. Data Extraction and Analysis
2.4. Quality and Risk of Bias
3. Results
3.1. Quality and Risk of Bias
3.2. Primary Outcome
3.3. Non-Muscle Invasive
3.4. Muscle-Invasive
3.5. Advanced/Metastatic
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anastasiadis, A.; de Reijke, T.M. Best practice in the treatment of nonmuscle invasive bladder cancer. Ther. Adv. Urol. 2012, 4, 13–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef]
- Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 329–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellmunt, J.; Powles, T.; Vogelzang, N.J. A review on the evolution of PD-1/PD-L1 immunotherapy for bladder cancer: The future is now. Cancer Treat. Rev. 2017, 54, 58–67. [Google Scholar] [CrossRef] [Green Version]
- Balar, A.V.; Kamat, A.M.; Kulkarni, G.S.; Uchio, E.M.; Boormans, J.L.; Roumiguié, M.; Krieger, L.E.M.; Singer, E.A.; Bajorin, D.F.; Grivas, P.; et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. 2021, 22, 919–930. [Google Scholar] [CrossRef]
- Necchi, A.; Anichini, A.; Raggi, D.; Briganti, A.; Massa, S.; Lucianò, R.; Colecchia, M.; Giannatempo, P.; Mortarini, R.; Bianchi, M.; et al. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J. Clin. Oncol. 2018, 36, 3353–3360. [Google Scholar] [CrossRef] [Green Version]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, A.; Lebret, T.; Shariat, S.; Park, S.H.; et al. First results from the phase 3 CheckMate 274 trial of adjuvant nivolumab vs placebo in patients who underwent radical surgery for high-risk muscle-invasive urothelial carcinoma (MIUC). J. Clin. Oncol. 2021, 39, 391. [Google Scholar] [CrossRef]
- Vuky, J.; Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Bellmunt, J.; Powles, T.; Bajorin, D.; Hahn, N.M.; Savage, M.J.; et al. Long-Term Outcomes in KEYNOTE-052: Phase II Study Investigating First-Line Pembrolizumab in Cisplatin-Ineligible Patients With Locally Advanced or Metastatic Urothelial Cancer. J. Clin. Oncol. 2020, 38, 2658–2666. [Google Scholar] [CrossRef] [PubMed]
- Fradet, Y.; Bellmunt, J.; Vaughn, D.J.; Lee, J.L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; Necchi, A.; et al. Randomized phase III KEYNOTE-045 trial of pembrolizumab versus paclitaxel, docetaxel, or vinflunine in recurrent advanced urothelial cancer: Results of >2 years of follow-up. Ann. Oncol. 2019, 30, 970–976. [Google Scholar] [CrossRef]
- Watts, R.D.; Li, I.W. Use of Checklists in Reviews of Health Economic Evaluations, 2010 to 2018. Value Health 2019, 22, 377–382. [Google Scholar] [CrossRef]
- Wijnen, B.F.M.; van Mastrigt, G.; Redekop, W.K.; Majoie, H.J.M.; de Kinderen, R.; Evers, S. How to prepare a systematic review of economic evaluations for informing evidence-based healthcare decisions: Data extraction, risk of bias, and transferability (part 3/3). Expert Rev. Pharm. Outcomes Res. 2016, 16, 723–732. [Google Scholar] [CrossRef] [Green Version]
- Wymer, K.M.; Sharma, V.; Saigal, C.S.; Chamie, K.; Litwin, M.S.; Packiam, V.T.; Mossanetn, M.; Pagliaro, L.C.; Borah, B.J.; Boorjian, S.A. Cost-Effectiveness Analysis of Pembrolizumab for Bacillus Calmette-Guérin-Unresponsive Carcinoma In Situ of the Bladder. J. Urol. 2021, 205, 1326–1335. [Google Scholar] [CrossRef] [PubMed]
- Khaki, A.R.; Shan, Y.; Nelson, R.E.; Kaul, S.; Gore, J.L.; Grivas, P.; Williams, S.B. Cost-effectiveness analysis of neoadjuvant immune checkpoint inhibition vs. cisplatin-based chemotherapy in muscle invasive bladder cancer. Urol. Oncol. 2021, 39, 732.e9–732.e16. [Google Scholar] [CrossRef] [PubMed]
- Hale, O.; Patterson, K.; Lai, Y.; Meng, Y.; Li, H.; Godwin, J.L.; Moreno, B.H.; Mamtani, R. Cost-effectiveness of Pembrolizumab versus Carboplatin-based Chemotherapy as First-line Treatment of PD-L1–positive Locally Advanced or Metastatic Urothelial Carcinoma Ineligible for Cisplatin-based Therapy in the United States. Clin. Genitourin. Cancer 2021, 19, e17–e30. [Google Scholar] [CrossRef]
- Parmar, A.; Richardson, M.; Coyte, P.C.; Cheng, S.; Sander, B.; Chan, K.K.W. A cost–utility analysis of atezolizumab in the second-line treatment of patients with metastatic bladder cancer. Curr. Oncol. 2020, 27, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Slater, R.L.; Lai, Y.; Zhong, Y.; Li, H.; Meng, Y.; Moreno, B.H.; Godwin, J.L.; Frenkl, T.; Sonpavde, G.P.; Mamtani, R. The cost effectiveness of pembrolizumab versus chemotherapy or atezolizumab as second-line therapy for advanced urothelial carcinoma in the United States. J. Med. Econ. 2020, 23, 967–977. [Google Scholar] [CrossRef]
- Criss, S.D.; Weaver, D.T.; Sheehan, D.F.; Lee, R.J.; Pandharipande, P.V.; Kong, C.Y. Effect of PD-L1 testing on the cost-effectiveness and budget impact of pembrolizumab for advanced urothelial carcinoma of the bladder in the United States. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 180.e11–180.e18. [Google Scholar] [CrossRef] [PubMed]
- Sarfaty, M.; Hall, P.S.; Chan, K.K.W.; Virik, K.; Leshno, M.; Gordon, N.; Moore, A.; Neiman, V.; Rosenbaum, E.; Goldstein, D.A. Cost-effectiveness of Pembrolizumab in Second-line Advanced Bladder Cancer. Eur. Urol. 2018, 74, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, T.; Prabhu, V.S.; Li, H.; Xu, R.; Zarabi, N.; Zhong, Y.; Pellissier, J.M.; Perini, R.F.; De Wit, R.; Mamtani, R. Cost-effectiveness of Pembrolizumab as Second-line Therapy for the Treatment of Locally Advanced or Metastatic Urothelial Carcinoma in Sweden. Eur. Urol. Oncol. 2020, 3, 663–670. [Google Scholar] [CrossRef] [Green Version]
- Powles, T.; Rodriguez-Vida, A.; Duran, I.; Crabb, S.J.; van der Heijden, M.S.; Font Pous, A.; Gravis, G.; Herranz, U.A.; Protheroe, A.; Ravaud, A.; et al. A phase II study investigating the safety and efficacy of neoadjuvant atezolizumab in muscle invasive bladder cancer (ABACUS). J. Clin. Oncol. 2018, 36, 4506. [Google Scholar] [CrossRef]
- Van Dijk, N.; Gil-Jimenez, A.; Silina, K.; Hendricksen, K.; Smit, L.A.; de Feijter, J.M.; van Montfoort, M.L.; van Rooijen, C.; Peters, D.; Broeks, A.; et al. Preoperative ipilimumab plus nivolumab in locoregionally advanced urothelial cancer: The NABUCCO trial. Nat. Med. 2020, 26, 1839–1844. [Google Scholar] [CrossRef]
- Powles, T.; Durán, I.; van der Heijden, M.S.; Loriot, Y.; Vogelzang, N.J.; De Giorgi, U.; Oudard, S.; Retz, M.M.; Castellano, D.; Bamias, A.; et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): A multicentre, open-label, phase 3 randomised controlled trial. Lancet 2018, 391, 748–757. [Google Scholar] [CrossRef]
- Gupta, S.; Kamat, A.M. NICE’s rejection of pembrolizumab for platinum-refractory urothelial carcinoma: Is there a greater good? Nat. Rev. Urol. 2020, 17, 491–492. [Google Scholar] [CrossRef] [PubMed]
- Evers, S.; Goossens, M.; de Vet, H.; van Tulder, M.; Ament, A. Criteria list for assessment of methodological quality of economic evaluations: Consensus on Health Economic Criteria. Int. J. Technol. Assess. Health Care 2005, 21, 240–245. [Google Scholar] [CrossRef] [Green Version]
- Grossman, H.B.; Natale, R.B.; Tangen, C.M.; Speights, V.; Vogelzang, N.J.; Trump, D.L.; White, R.W.D.; Sarosdy, M.F.; Wood, D.P.; Raghavan, D.; et al. Neoadjuvant Chemotherapy plus Cystectomy Compared with Cystectomy Alone for Locally Advanced Bladder Cancer. N. Engl. J. Med. 2003, 349, 859–866. [Google Scholar] [CrossRef]
- Dash, A.; Pettus, J.A.; Herr, H.W.; Bochner, B.; Dalbagni, G.; Donat, S.; Russo, P.; Boyle, M.G.; Milowsky, M.I.; Bajorin, D.F. A Role for Neoadjuvant Gemcitabine Plus Cisplatin in Muscle-Invasive Urothelial Carcinoma of the Bladder: A Retrospective Experience. Cancer 2008, 113, 2471–2477. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Siefker-Radtke, A.; de Braud, F.; Basso, U.; Calvo, E.; Bono, P.; Morse, M.A.; Ascierto, P.A.; Lopez-Martin, J.; Brossart, P.; et al. Nivolumab Alone and With Ipilimumab in Previously Treated Metastatic Urothelial Carcinoma: CheckMate 032 Nivolumab 1 mg/kg Plus Ipilimumab 3 mg/kg Expansion Cohort Results. J. Clin. Oncol. 2019, 37, 1608–1616. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.D.; Wilkinson, C.L.; Pope, E.F.; Chambers, J.D.; Cohen, J.T.; Neumann, P.J. The influence of time horizon on results of cost-effectiveness analyses. Expert Rev. Pharm. Outcomes Res. 2017, 17, 615–623. [Google Scholar] [CrossRef]
- Davis, A.A.; Patel, V.G. The role of PD-L1 expression as a predictive biomarker: An analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 278. [Google Scholar] [CrossRef] [PubMed]
- Nanavaty, M.; Kaura, S.; Mwamburi, M.; Mwamburi, M.; Gogate, A.; Proach, J.; Nyandege, A.; Khan, Z.M. The Use of Incremental Cost-Effectiveness Ratio Thresholds in Health Technology Assessment Decisions. J. Clin. Pathw. 2015, 1, 29–36. [Google Scholar]


{kind=link}
| Stage | Reference | Cohort | Method | Total Cost | QALY | ICER (Per QALY) | WTP Threshold (Per QALY) | Conclusion |
|---|---|---|---|---|---|---|---|---|
| NMIBC | Wymer et al., 2020 [13], USA | Pembrolizumab (PB) vs. intravesical gemcitabine/docetaxel (GD) vs. upfront radical cystectomy (RC) for BCG-refractory NMIBC | Markov Model, 5-year horizon, Medicare payor perspective, base year 2019 | Index 1 PB: $191,297 GD: $43,488 RC: $39,367 Index 2 PB: $189,902 GD: $38,192 | Index 1 PB: 4.39 GD: 4.32 RC: 4.29 Index 2 PB: 4.35 GD: 4.21 | Index 1 PB/RC: $1,403,008 PB/GD: $2,011,923 Index 2 PB/GD: $1,073,240 | $100,000 | PB is not cost-effective compared to RC or intravesical GD for BCG-refractory NMIBC |
| MIBC | Khaki et al., 2021 [14], USA * | Neoadjuvant PB vs. ddMVAC. Secondary gemcitabine/cisplatin (GC), atezolizumab (AZ) and nivolumab/ipilimumab (NI) assessment | Decision analysis simulation, 2-year horizon based on RFS given no OS data, third-party payor perspective, base year 2020 | PB: $30,556 ddMVAC: $22,515 GC: $910 AZ:$18,838 NI: $74,052 | PB: 0.591 ddMVAC: 0.576 GC: 0.567 AZ: 0.578 NI: 0.611 | PB/ddMVAC: $522,143 AZ/ddMVAC: Dominates (−$1838/500) NI/ddMVAC: $1,464,119 PB/GC: $1,225,058 AZ/GC: $1,629,855 NI/GC: $1,662,327 | $100,000 | PB is not cost-effective compared to ddMVAC or GC as a neoadjuvant treatment based on 2-year RFS AZ may be cost-effective compared to ddMVAC, not GC |
| Treatment | Reference | Cohort | Method | Total Cost | QALY | ICER (Per QALY) | WTP Threshold (Per QALY) | Conclusion |
|---|---|---|---|---|---|---|---|---|
| First-line | Hale et al., 2020 [15], USA | First-line PB vs. gemcitabine plus carboplatin (GCa) in cisplatin-ineligible patients with CPS ≥ 10 | Partitioned survival model, 20-year time horizon, third-party payor perspective, AEs included, base year 2018 | PB: $225,334 GCa: $66,773 | PB: 2.91 GCa: 0.90 | PB/GCa: $78,925 | $150,000 | PB may be cost-effective relative to GCa for 1L treatment for PD-L1 positive, cisplatin-ineligible patients with metastatic UC |
| Second-line | Parmar et al., 2020 [16], Canada | AZ vs. chemotherapy (taxanes) as second line treatment after progression on cisplatin | Partitioned survival model, 5-year horizon, Canadian healthcare system perspective, includes AEs and end-of-life care, base year 2018 | AZ: C$90,290 Chemo: C $8,466 | AZ: 0.75 Chemo: 0.76 | AZ/Chemo: C $430,652 AZ/Chemo: C$334,387 (for subgroup PDL1 expression > 5%) AZ/Chemo: C $305,408 (for extended 10-year horizon) | C$100,000 | AZ is not considered cost-effective relative to taxanes as 2L treatment for advanced UC ICER improves with PD-L1 stratification and longer time horizon |
| Slater et al., 2020 [17], USA | PB vs. chemotherapy (taxanes) after progression on first-line therapy Secondary analysis comparing PB and AZ | Partitioned survival model, 20-year horizon, third-party payor perspective, base year 2018 | PB: $140,556 Chemo: $34,257 PB: $152,753 AZ: $179,211 | PB: 1.79 Chemo: 0.66 PB: 1.79 AZ: 1.03 | PB/Chemo: $93,481 PB/AZ: Dominates (−$34,813) | $100,000 | PB may be cost-effective compared to taxanes for advanced UC Indirect comparison suggests PB more cost-effective than AZ | |
| Criss et al., 2018 [18], USA | Cost-effectiveness of PD-L1 testing in second-line treatment. Compared chemotherapy (taxanes), PB, and PB for PD-L1 > 1% with chemotherapy for PD-L1 < 1% | Microsimulation model, 5-year horizon, US healthcare system perspective, base year 2017 | PD-L1 > 1%: $27,579 Chemo: $17,732 PB: $40,573 | PD-L1 > 1%: 0.51 Chemo: 0.43 PB: 0.58 | PD-L1 > 1%/chemo: $122,933 PB/PD-L1 >1%: $197,383 | $100,000 | The cost-effectiveness of PB improves when PD-L1 status is included, but still fails to meet the WTP threshold | |
| Sarfaty et al., 2018 [19], multi-national * | PB vs. chemotherapy (taxanes) for second-line treatment | Markov model, 5-year horizon, third-party payor perspective, included AEs, base year 2017 | * USA: $44,325 UK: $33,271 Canada: $33,869 Australia: $36,154 | * USA: 0.36 UK: 0.36 Canada: 0.37 Australia: 0.36 | USA: $122,557 UK: $91,995 Canada: $90,099 Australia: $99,966 | USA: $150,000 UK: $65,000 Canada: $80,000 Australia: $60,000 | PB may be cost-effective compared to chemotherapy at the WTP threshold set for the USA | |
| Srivastava et al., 2018 [20], Sweden | PB vs. chemotherapy (taxanes, vinflunine) for second-line treatment | Partitioned survival model, 15-year horizon, included AEs, base year 2018 | PB: €98,354 Vinflunine: €28,501 PB: €98,348 Taxane: €25,182 PB: €98,208 Chemo: €25,054 | PB: 1.99 Vinflunine: 0.61 PB: 1.99 Taxane: 1.09 PB:1.99 Chemo: 0.97 | PB/Vinflunine: €50,529 PB/Taxane: €81,356 PB/Chemo: €71,924 | €100,000 | PB may be cost-effective relative to vinflunine and taxanes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walia, A.S.; Sweis, R.F.; Agarwal, P.K.; Kader, A.K.; Modi, P.K. Cost-Effectiveness of Immune Checkpoint Inhibitors in Urothelial Carcinoma—A Review. Cancers 2022, 14, 73. https://doi.org/10.3390/cancers14010073
Walia AS, Sweis RF, Agarwal PK, Kader AK, Modi PK. Cost-Effectiveness of Immune Checkpoint Inhibitors in Urothelial Carcinoma—A Review. Cancers. 2022; 14(1):73. https://doi.org/10.3390/cancers14010073
Chicago/Turabian StyleWalia, Arman S., Randy F. Sweis, Piyush K. Agarwal, Andrew K. Kader, and Parth K. Modi. 2022. "Cost-Effectiveness of Immune Checkpoint Inhibitors in Urothelial Carcinoma—A Review" Cancers 14, no. 1: 73. https://doi.org/10.3390/cancers14010073