
Prognostic Assessment in High-Grade Soft-Tissue Sarcoma Patients: A Comparison of Semantic Image Analysis and Radiomics

 , , , ,
, , , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
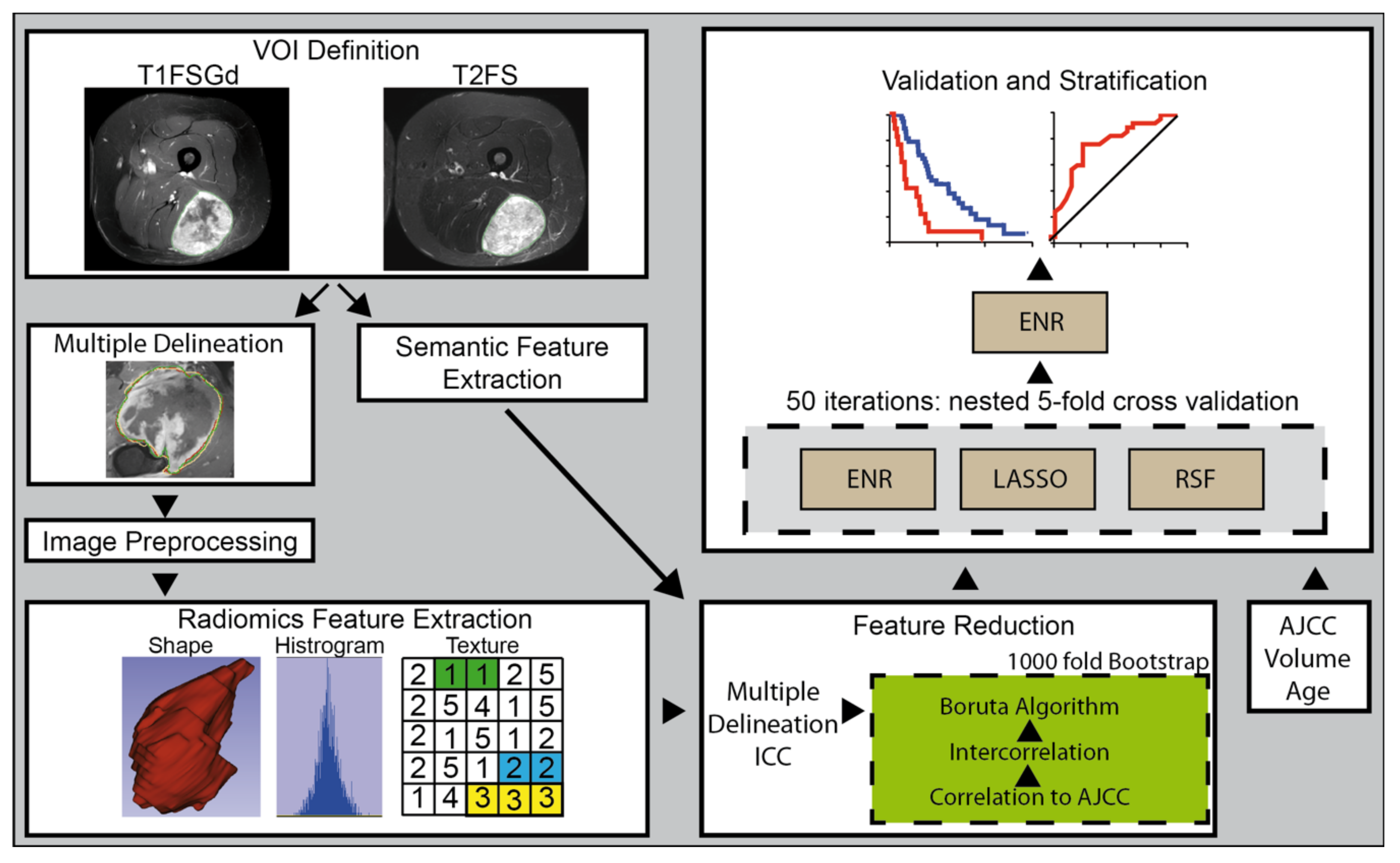
2.2. Image Acquisition and Definition of Volume of Interests
2.3. Image Preprocessing and Radiomic Feature Extraction
2.4. ComBat Batch Harmonization
2.5. Semantic Imaging Features
2.6. Modeling Strategy
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics, Histology and VOI Definition
3.2. Interrater Agreement of Semantic Imaging Features
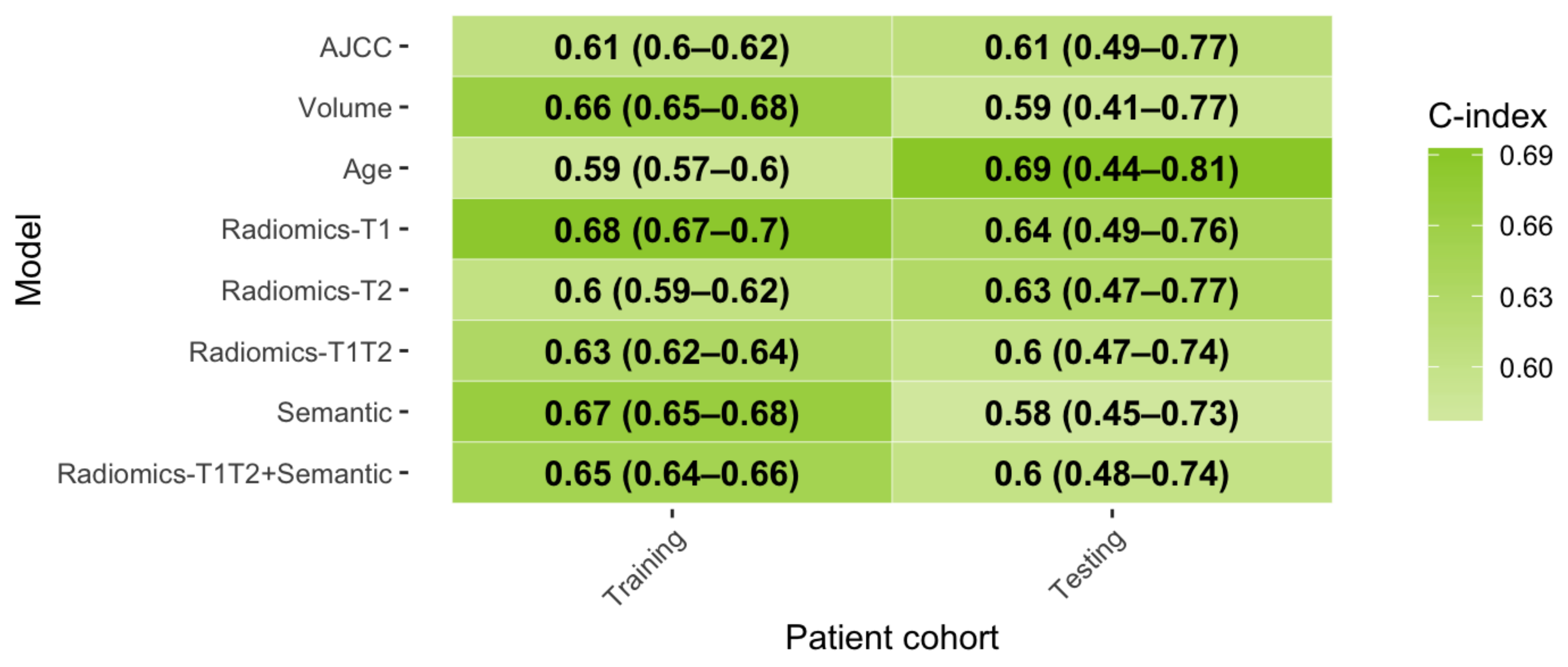
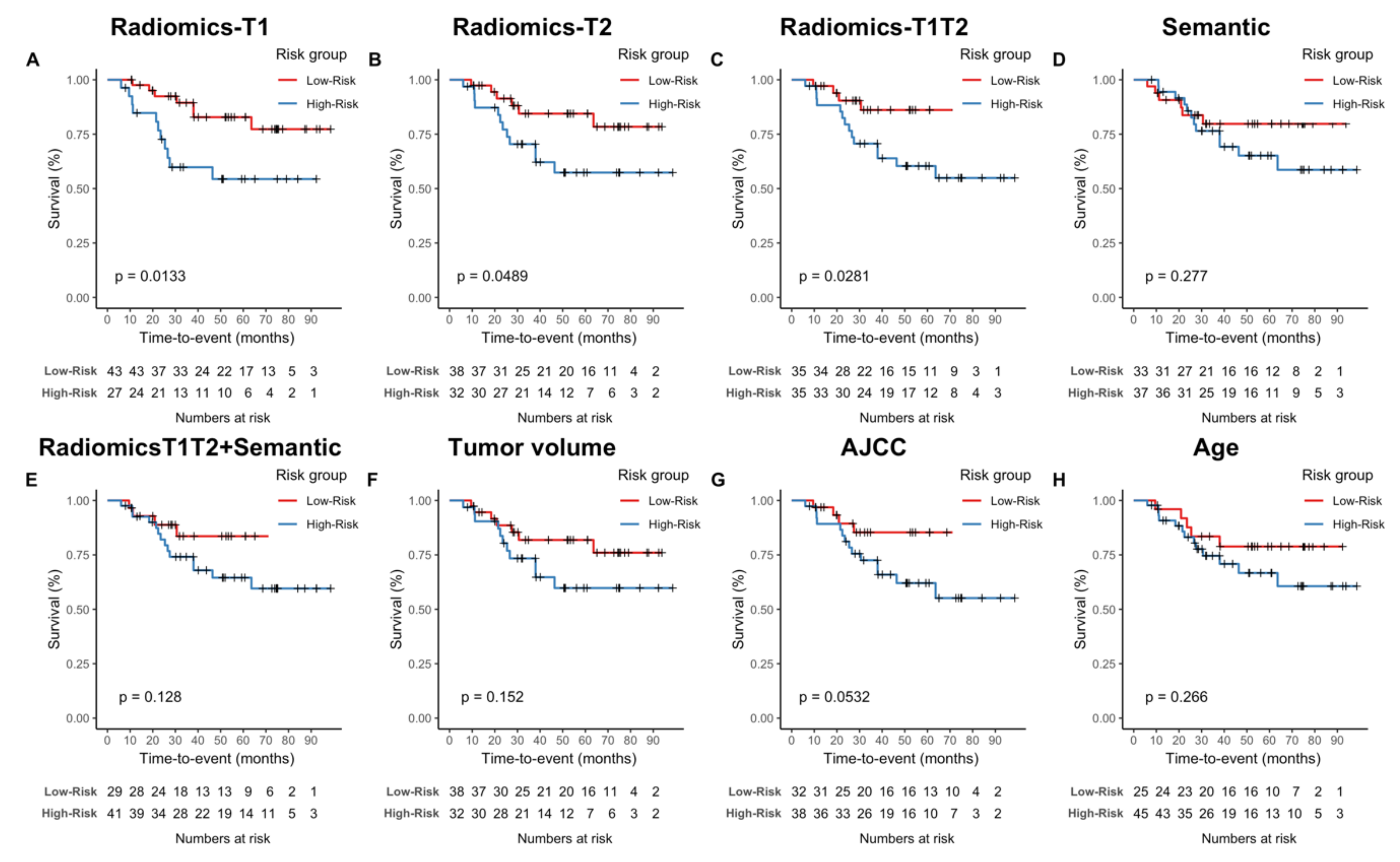
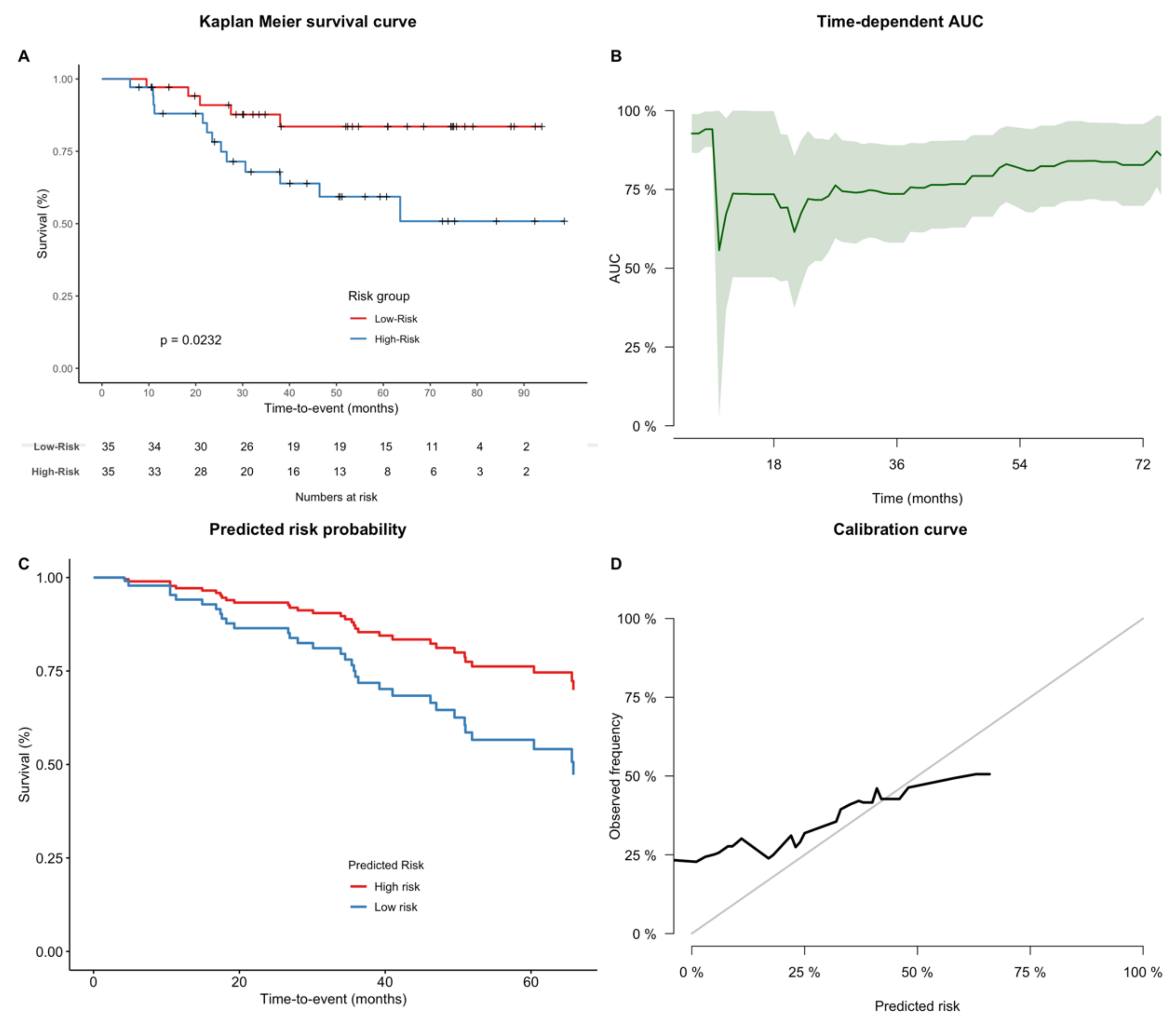
3.3. Comparison of Semantic Imaging Features and Radiomics for Prediction of Overall Survival
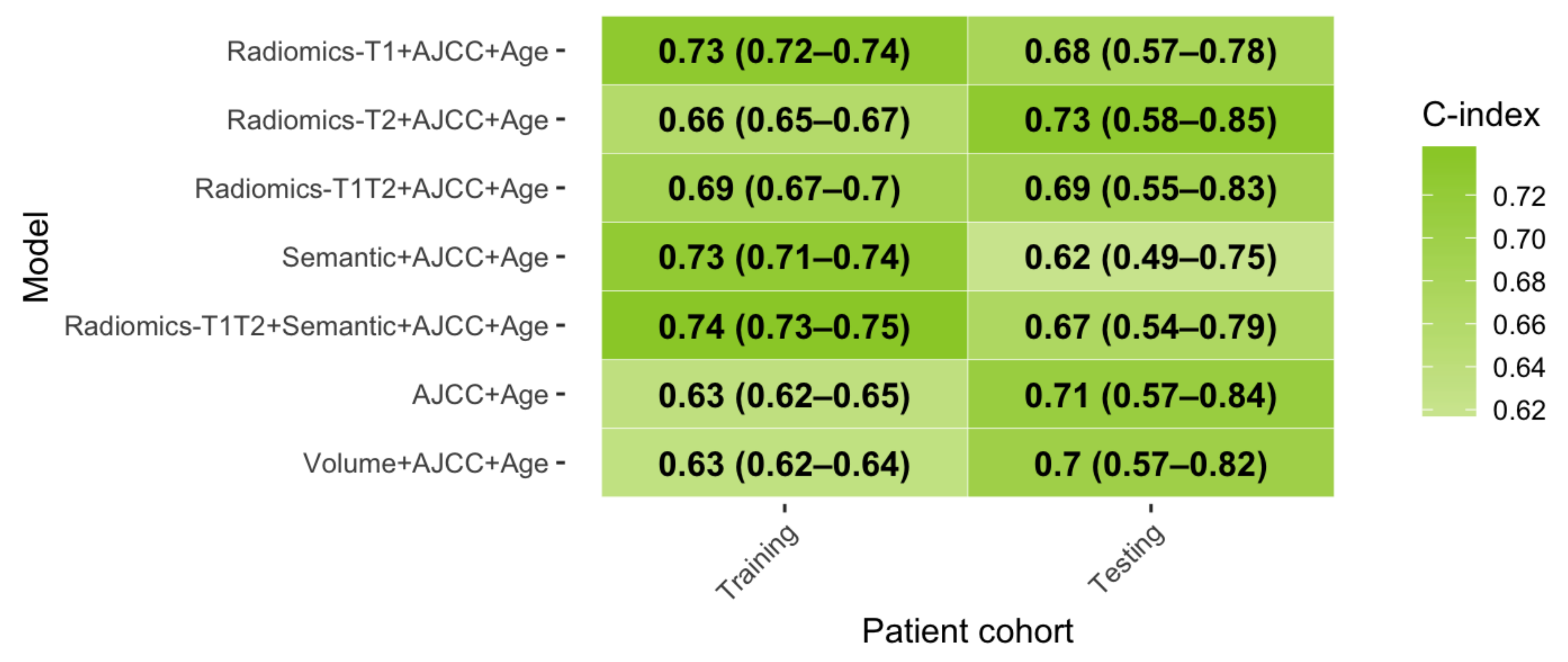
3.4. Relevance of Combined Clinical-Imaging Models
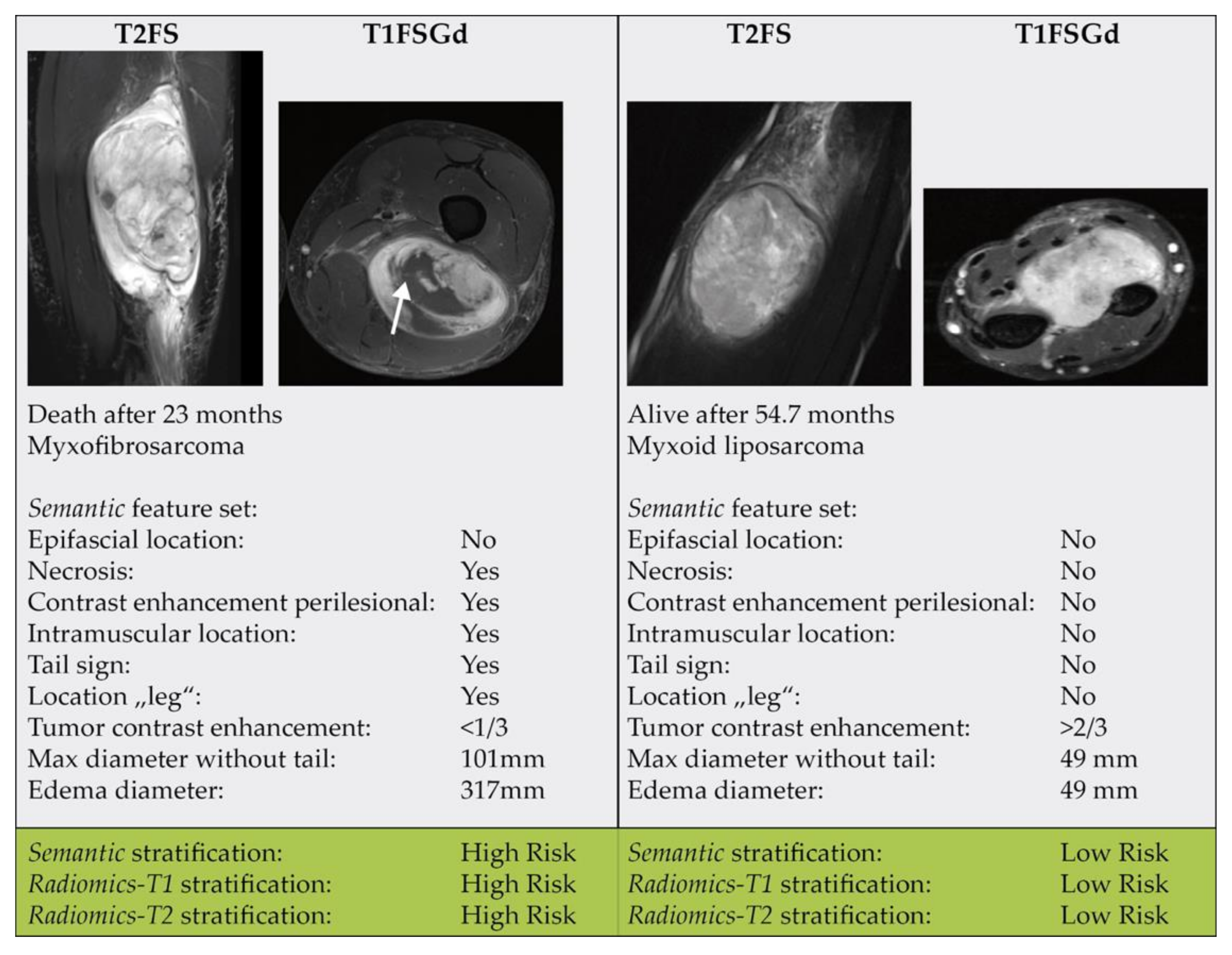
3.5. Relevance of Single Imaging Parameters
3.6. Analysis of Model Calibration
3.7. Assessment of the Impact of the Independence of the Test Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gutierrez, J.C.; Perez, E.A.; Franceschi, D.; Moffat, F.L.; Livingstone, A.S.; Koniaris, L.G. Outcomes for Soft-Tissue Sarcoma in 8249 Cases from a Large State Cancer Registry. J. Surg. Res. 2007, 141, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Gerrand, C.H.; Rankin, K. The treatment of soft-tissue sarcomas of the extremities. Prospective randomized evaluations of (1) limb-sparing surgery plus radiation therapy compared with amputation and (2) the role of adjuvant chemotherapy. Class. Pap. Orthop. 2014, 483–484. [Google Scholar] [CrossRef]
- Koshy, M.; Rich, S.; Mohiuddin, M. Improved Survival with Radiation Therapy in High Grade Soft Tissue Sarcomas of the Extremities: A SEER Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 77, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alektiar, K.M.; Brennan, M.F.; Healey, J.H.; Singer, S. Impact of intensity-modulated radiation therapy on local control in primary soft-tissue sarcoma of the extremity. J. Clin. Oncol. 2008, 26, 3440–3444. [Google Scholar] [CrossRef]
- Peeken, J.C.; Knie, C.; Kessel, K.A.; Habermehl, D.; Kampfer, S.; Dapper, H.; Devecka, M.; Von Eisenhart-rothe, R.; Specht, K.; Weichert, W.; et al. Neoadjuvant image-guided helical intensity modulated radiotherapy of extremity sarcomas—A single center experience. Radiat. Oncol. 2019, 14, 4–11. [Google Scholar] [CrossRef]
- Muehlhofer, H.M.L.; Schlossmacher, B.; Lenze, U.; Lenze, F.; Burgkart, R.; Gersing, A.S.; Peeken, J.C.; Combs, S.E.; Von Eisenhart-Rothe, R.; Knebel, C. Oncological Outcome and Prognostic Factors of Surgery for Soft Tissue Sarcoma After Neoadjuvant or Adjuvant Radiation Therapy: A Retrospective Analysis over 15 Years. Anticancer Res. 2021, 41, 359–368. [Google Scholar] [CrossRef]
- Peeken, J.C.; Goldberg, T.; Knie, C.; Komboz, B.; Bernhofer, M.; Pasa, F.; Kessel, K.A.; Tafti, P.D.; Rost, B.; Nüsslin, F.; et al. Treatment-related features improve machine learning prediction of prognosis in soft tissue sarcoma patients. Strahlentherapie Onkol. 2018, 194, 824–834. [Google Scholar] [CrossRef]
- Peeken, J.C.; Hesse, J.; Haller, B.; Kessel, K.A.; Nüsslin, F.; Combs, S.E. Semantic imaging features predict disease progression and survival in glioblastoma multiforme patients. Strahlenther. Onkol. 2018, 194, 580–590. [Google Scholar] [CrossRef]
- Wu, G.; Woodruff, H.C.; Sanduleanu, S.; Refaee, T.; Jochems, A.; Leijenaar, R.; Gietema, H.; Shen, J.; Wang, R.; Xiong, J.; et al. Preoperative CT-based radiomics combined with intraoperative frozen section is predictive of invasive adenocarcinoma in pulmonary nodules: A multicenter study. Eur. Radiol. 2020, 30, 2680–2691. [Google Scholar] [CrossRef] [Green Version]
- Peeken, J.C.; Goldberg, T.; Pyka, T.; Bernhofer, M.; Wiestler, B.; Kessel, K.A.; Tafti, P.D.; Nüsslin, F.; Braun, A.E.; Zimmer, C.; et al. Combining multimodal imaging and treatment features improves machine learning-based prognostic assessment in patients with glioblastoma multiforme. Cancer Med. 2019, 8, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Crombé, A.; Marcellin, P.J.; Buy, X.; Stoeckle, E.; Brouste, V.; Italiano, A.; Le Loarer, F.; Kind, M. Soft-tissue sarcomas: Assessment of MRI features correlating with histologic grade and patient outcome. Radiology 2019, 291, 710–721. [Google Scholar] [CrossRef]
- Peeken, J.C.; Nüsslin, F.; Combs, S.E. “Radio-oncomics”—The potential of radiomics in radiation oncology. Strahlenther. Onkol. 2017, 193, 767–779. [Google Scholar] [CrossRef]
- Peeken, J.C.; Wiestler, B.; Combs, S.E. The potential of radiomics in clinical application. In Image Guided Radiooncology; Debus, J., Schober, O., Kiessling, F., Eds.; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Peeken, J.C.; Bernhofer, M.; Wiestler, B.; Goldberg, T.; Cremers, D.; Rost, B.; Wilkens, J.J.; Combs, S.E.; Nüsslin, F. Radiomics in radiooncology—Challenging the medical physicist. Phys. Med. 2018, 48, 27–36. [Google Scholar] [CrossRef]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.P.M.; Granton, P.; Zegers, C.M.L.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.W.L.; Velazquez, E.R.; Leijenaar, R.T.H.; Parmar, C.; Grossmann, P.; Carvalho, S.; Cavalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Rios Velazquez, E.; Parmar, C.; Liu, Y.; Coroller, T.P.; Cruz, G.; Stringfield, O.; Ye, Z.; Makrigiorgos, M.; Fennessy, F.; Mak, R.H.; et al. Somatic mutations drive distinct imaging phenotypes in lung cancer. Cancer Res. 2017, 77, 3922–3930. [Google Scholar] [CrossRef] [Green Version]
- Diehn, M.; Nardini, C.; Wang, D.S.; McGovern, S.; Jayaraman, M.; Liang, Y.; Aldape, K.; Cha, S.; Kuo, M.D. Identification of noninvasive imaging surrogates for brain tumor gene-expression modules. Proc. Natl. Acad. Sci. USA 2008, 105, 5213–5218. [Google Scholar] [CrossRef] [Green Version]
- Peeken, J.C.; Shouman, M.A.; Kroenke, M.; Rauscher, I.; Maurer, T.; Gschwend, J.E.; Eiber, M.; Combs, S.E. A CT-based radiomics model to detect prostate cancer lymph node metastases in PSMA radioguided surgery patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2968–2977. [Google Scholar] [CrossRef]
- Peeken, J.C.; Molina-Romero, M.; Diehl, C.; Menze, B.H.; Straube, C.; Meyer, B.; Zimmer, C.; Wiestler, B.; Combs, S.E. Deep learning derived tumor infiltration maps for personalized target definition in Glioblastoma radiotherapy. Radiother. Oncol. 2019, 138, 166–172. [Google Scholar] [CrossRef]
- Leger, S.; Zwanenburg, A.; Leger, K.; Lohaus, F.; Linge, A.; Schreiber, A.; Kalinauskaite, G.; Tinhofer, I.; Guberina, N.; Guberina, M.; et al. Comprehensive Analysis of Tumour Sub-Volumes for Radiomic Risk Modelling in Locally Advanced HNSCC. Cancers 2020, 12, 3047. [Google Scholar] [CrossRef]
- Spraker, M.B.; Wootton, L.S.; Hippe, D.S.; Ball, K.C.; Peeken, J.C.; Macomber, M.W.; Chapman, T.R.; Hoff, M.; Kim, E.Y.; Pollack, S.M.; et al. MRI Radiomic Features Are Independently Associated with Overall Survival in Soft Tissue Sarcoma. Adv. Radiat. Oncol. 2019, 4, 413–421. [Google Scholar] [CrossRef] [Green Version]
- Vallières, M.; Freeman, C.R.; Skamene, S.R.; El Naqa, I. A radiomics model from joint FDG-PET and MRI texture features for the prediction of lung metastases in soft-tissue sarcomas of the extremities. Phys. Med. Biol. 2015, 60, 5471–5496. [Google Scholar] [CrossRef]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Fedorov, A.; Beichel, R.; Kalphaty-Cramer, J.; Finet, J.; Fillion-Robbin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D slicers as an image computing platform for the quantitative imaging network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Tustison, N.J.; Gee, J.C. N4ITK: Nick’s N3 ITK Implementation for MRI Bias Field Correction. Insight J. 2009, 9, 1–8. [Google Scholar]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [Green Version]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 191145. [Google Scholar] [CrossRef] [Green Version]
- Depeursinge, A.; Andrearczyk, V.; Whybra, P.; van Griethuysen, J.; Müller, H.; Schaer, R.; Vallières, M.; Zwanenburg, A. Standardised convolutional filtering for radiomics. arXiv 2020, arXiv:2006.05470. [Google Scholar]
- Steiger, P.; Sood, R. How Can Radiomics Be Consistently Applied across Imagers and Institutions? Radiology 2019, 291, 60–61. [Google Scholar] [CrossRef]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2007, 8, 118–127. [Google Scholar] [CrossRef]
- Lucia, F.; Visvikis, D.; Vallières, M.; Desseroit, M.; Miranda, O.; Robin, P.; Bonaffini, P.A.; Alfieri, J.; Masson, I.; Mervoyer, A.; et al. External validation of a combined PET and MRI radiomics model for prediction of recurrence in cervical cancer patients treated with chemoradiotherapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 864–877. [Google Scholar] [CrossRef] [PubMed]
- Orlhac, F.; Frouin, F.; Nioche, C.; Ayache, N.; Buvat, I. Validation of A Method to Compensate Multicenter Effects Affecting CT Radiomics. Radiology 2019, 291, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortin, J.; Parker, D.; Tunç, B.; Watanabe, T.; Elliott, M.A.; Ruparel, K.; Roalf, D.R.; Satterthwaite, T.D.; Gur, R.C.; Gur, R.E.; et al. NeuroImage Harmonization of multi-site diffusion tensor imaging data. Neuroimage 2017, 161, 149–170. [Google Scholar] [CrossRef] [PubMed]
- Holzapfel, K.; Regler, J.; Baum, T.; Rechl, H.; Specht, K.; Haller, B.; von Eisenhart-Rothe, R.; Gradinger, R.; Rummeny, E.J.; Woertler, K. Local Staging of Soft-Tissue Sarcoma: Emphasis on Assessment of Neurovascular Encasement—Value of MR Imaging in 174 Confirmed Cases. Radiology 2015, 275, 501–509. [Google Scholar] [CrossRef]
- Petscavage-Thomas, J.M.; Walker, E.A.; Logie, C.I.; Clarke, L.E.; Duryea, D.M.; Murphey, M.D. Soft-tissue myxomatous lesions: Review of salient imaging features with pathologic comparison. Radiographics 2014, 34, 964–980. [Google Scholar] [CrossRef]
- Yoo, H.J.; Hong, S.H.; Kang, Y.; Choi, J.-Y.; Moon, K.C.; Kim, H.-S.; Han, I.; Yi, M.; Kang, H.S. MR imaging of myxofibrosarcoma and undifferentiated sarcoma with emphasis on tail sign; diagnostic and prognostic value. Eur. Radiol. 2014, 24, 1749–1757. [Google Scholar] [CrossRef]
- Knebel, C.; Neumann, J.; Schwaiger, B.J.; Karampinos, D.C.; Pfeiffer, D.; Specht, K.; Lenze, U.; Von Eisenhart-Rothe, R.; Rummeny, E.J.; Woertler, K.; et al. Differentiating atypical lipomatous tumors from lipomas with magnetic resonance imaging: A comparison with MDM2 gene amplification status. BMC Cancer 2019, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tibshirani, R. Regression Shrinkage and Selection Via the Lasso. J. R. Stat. Soc. Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Ishwaran, H.; Gerds, T.A.; Kogalur, U.B.; Moore, R.D.; Gange, S.J.; Lau, B.M. Random survival forests for competing risks. Biostatistics 2014, 15, 757–773. [Google Scholar] [CrossRef] [Green Version]
- Waldron, L.; Pintilie, M.; Tsao, M.S.; Shepherd, F.A.; Huttenhower, C.; Jurisica, I. Optimized application of penalized regression methods to diverse genomic data. Bioinformatics 2011, 27, 3399–3406. [Google Scholar] [CrossRef] [Green Version]
- AJCC. Cancer Staging Manual, 8th ed.; Amin, M.B., Edge, S., Greene, F., Byrd, D.R., Brookland, R.K., Washington, M.K., Gershenwald, J.E., Compton, C.C., Hess, K.R., Sullivan, D.C., et al., Eds.; Springer International Publishing: New York, NY, USA, 2017. [Google Scholar]
- Kursa, M.B.; Rudnicki, W.R. Feature selection with the boruta package. J. Stat. Softw. 2010, 36, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Wu, G.; Woodruff, H.C.; Shen, J.; Refaee, T.; Sanduleanu, S.; Abdalla, I.; Leijenaar, R.T.H.; Wang, R.; Xiong, J.; Bian, J.; et al. Diagnosis of Invasive Lung Adenocarcinoma Based on Chest CT Radiomic Features of Part-Solid Pulmonary Nodules: A Multicenter Study. Radiology 2020, 192431. [Google Scholar] [CrossRef]
- Lang, M.; Binder, M.; Richter, J.; Schratz, P.; Pfisterer, F.; Coors, S.; Au, Q.; Casalicchio, G.; Kotthoff, L.; Bischl, B. mlr3: A modern object-oriented machine learning framework in R. J. Open Source Softw. 2019, 4, 1903. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [Green Version]
- Altman, D.G. Practical Statistics for Medical Research; Chapman and Hall/CRC: Boca Raton, FL, USA, 2018; ISBN 978-0-41227-630-9. [Google Scholar]
- Wortman, J.R.; Tirumani, S.H.; Jagannathan, J.P.; Tirumani, H.; Shinagare, A.B.; Hornick, J.L.; Ramaiya, N.H. Primary Extremity Liposarcoma: MRI Features, Histopathology, and Clinical Outcomes. J. Comput. Assist. Tomogr. 2016, 40, 791–798. [Google Scholar] [CrossRef]
- Mühlhofer, H.; Gersing, A.; Pfeiffer, D.; Wörtler, K.; Lenze, U.; Lenze, F.; Lallinger, V.; Haller, B.; Burgkart, R.; von Eisenhart-Rothe, R.; et al. Preoperative evaluation of myxofibrosarcoma: Prognostic value and reproducibility of different features on MRI. Anticancer Res. 2020, 40, 5793–5800. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Löck, S. Why validation of prognostic models matters? Radiother. Oncol. 2018, 127, 370–373. [Google Scholar] [CrossRef]
- Peeken, J.C.; Bernhofer, M.; Spraker, M.B.; Pfeiffer, D.; Devecka, M.; Thamer, A.; Shouman, M.A.; Ott, A.; Nüsslin, F.; Mayr, N.A.; et al. CT-based radiomic features predict tumor grading and have prognostic value in patients with soft tissue sarcomas treated with neoadjuvant radiation therapy. Radiother. Oncol. 2019, 135, 187–196. [Google Scholar] [CrossRef]
- Zer, A.; Prince, R.M.; Amir, E.; Abdul Razak, A.R. Multi-agent chemotherapy in advanced soft tissue sarcoma (STS)—A systematic review and meta-analysis. Cancer Treat. Rev. 2018, 63, 71–78. [Google Scholar] [CrossRef]
- Wong, P.; Houghton, P.; Kirsch, D.G.; Finkelstein, S.E.; Monjazeb, A.M.; Xu-Welliver, M.; Dicker, A.P.; Ahmed, M.; Vikram, B.; Teicher, B.A.; et al. Combining targeted agents with modern radiotherapy in soft tissue sarcomas. J. Natl. Cancer Inst. 2014, 106, 16–18. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, G.K.; Tap, W.D.; Qin, L.-X.; Livingston, M.B.; Undevia, S.D.; Chmielowski, B.; Agulnik, M.; Schuetze, S.M.; Reed, D.R.; Okuno, S.H.; et al. Cixutumumab and temsirolimus for patients with bone and soft-tissue sarcoma: A multicentre, open-label, phase 2 trial. Lancet Oncol. 2013, 14, 371–382. [Google Scholar] [CrossRef] [Green Version]
- Pollack, S.M.; He, Q.; Yearley, J.H.; Emerson, R.; Vignali, M.; Zhang, Y.; Redman, M.W.; Baker, K.K.; Cooper, S.; Donahue, B.; et al. T-cell infiltration and clonality correlate with programmed cell death protein 1 and programmed death-ligand 1 expression in patients with soft tissue sarcomas. Cancer 2017, 123, 3291–3304. [Google Scholar] [CrossRef] [Green Version]
- Gronchi, A.; Hindi, N.; Cruz, J.; Blay, J.-Y.; Sanfilippo, R.; Morosi, C.; Romero, J.; Peinado, J.; Lopez-Pousa, A.; Alvarez Alvarez, R.M.; et al. Trabectedin and radiotherapy in soft-tissue sarcoma (TRASTS) study: An international, prospective, phase I/II trial—A collaborative Spanish (GEIS), Italian (ISG), and French (FSG) groups study. J. Clin. Oncol. 2017, 35, 11061. [Google Scholar] [CrossRef]
- Gluck, W.L.; Gounder, M.M.; Frank, R.; Eskens, F.; Blay, J.Y.; Cassier, P.A.; Soria, J.-C.; Chawla, S.; de Weger, V.; Wagner, A.J.; et al. Phase 1 study of the MDM2 inhibitor AMG 232 in patients with advanced P53 wild-type solid tumors or multiple myeloma. Investig. New Drugs 2020, 38, 831–843. [Google Scholar] [CrossRef] [Green Version]
- Peeken, J.C.; Spraker, M.B.; Knebel, C.; Dapper, H.; Pfeiffer, D.; Devecka, M.; Thamer, A.; Shouman, M.A.; Ott, A.; von Eisenhart-Rothe, R.; et al. Tumor grading of soft tissue sarcomas using MRI-based radiomics. EBioMedicine 2019, 48, 332–340. [Google Scholar] [CrossRef] [Green Version]
- Yan, R.; Hao, D.; Li, J.; Liu, J.; Hou, F.; Chen, H.; Duan, L.; Huang, C.; Wang, H.; Yu, T. Magnetic Resonance Imaging-Based Radiomics Nomogram for Prediction of the Histopathological Grade of Soft Tissue Sarcomas: A Two-Center Study. J. Magn. Reson. Imaging 2021. [Google Scholar] [CrossRef]
- Gennaro, N.; Reijers, S.; Bruining, A.; Messiou, C.; Haas, R.; Colombo, P.; Bodalal, Z.; Beets-Tan, R.; van Houdt, W.; van der Graaf, W.T.A. Imaging response evaluation after neoadjuvant treatment in soft tissue sarcomas: Where do we stand? Crit. Rev. Oncol. Hematol. 2021, 160, 103309. [Google Scholar] [CrossRef]
- Crombé, A.; Périer, C.; Kind, M.; De Senneville, B.D.; Le Loarer, F.; Italiano, A.; Buy, X.; Saut, O. T2-based MRI Delta-radiomics improve response prediction in soft-tissue sarcomas treated by neoadjuvant chemotherapy. J. Magn. Reson. Imaging 2018, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Lin, P.; Yang, P.F.; Chen, S.; Shao, Y.Y.; Xu, L.; Wu, Y.; Teng, W.; Zhou, X.Z.; Li, B.H.; Luo, C.; et al. A Delta-radiomics model for preoperative evaluation of Neoadjuvant chemotherapy response in high-grade osteosarcoma. Cancer Imaging 2020, 20, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sica, G.T. Bias in Research Studies. Radiology 2006, 238, 780–789. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Description |
|---|---|
| Anatomical region | 1: chest/back, 2: neck, 3: leg, 4: gluteal/pelvis 5: arm, 6: hand, 7: foot |
| Localization | 1: epifascial, 2: subfascial, 3: epi- and subfascial, 4: intramuscular, 5: intermuscular; 6 intra- and intermuscular |
| Image pattern | 1: multinodular, 2: mass-like round/oval, 3: superficial spread |
| Borders | 1: well defined /pushing type, 2: focal infiltrating, 3: diffuse infiltrating |
| Dominant STIR Signal intensity | 1: hypointense, 2: isointense, 3: hyperintense |
| STIR Homogeneity | 1: homogenous, 2: inhomogenous |
| Contrast enhancement of the tumor | 1:<1/3 of the tumor, 2: 1/3–2/3, 3: >2/3 |
| Homogeneity of Tumor contrast enhancement | 1: homogeneous, 2: inhomogeneous |
| Tail sign | 1: present, 0: absent, 2: uncertain |
| Vascularization | 1: present, 0: absent |
| Necrosis | 1: present, 0: absent |
| perilesional Edema | 1: present, 0: absent |
| perilesional Contrast enhancement | 1: present, 0: absent |
| Max diameter (in mm without tail) | in mm |
| Edema diameter (in mm) | in mm |
| Institution | Testing Cohort | Training Cohort | p-Value 1 | p-Value Adjusted 1 | |
|---|---|---|---|---|---|
| Accrual time | 2010–2016 | 2007–2015 | |||
| Total Patients | 71 p | 108 p | |||
| Primary | 66 p (93%) | 108 p (100%) | <0.001 * | <0.001 * | |
| Recurrent | 5 p (7%) | 0 p | |||
| Location | Lower Extremity | 56 p (79%) | 75 p (70%) | 0.36 | 1.0 |
| Upper Extremity | 10 p (14%) | 17 p (16%) | |||
| Trunk | 5 p (7%) | 16 p (14%) | |||
| Age | m 57 (r 17–87) | m 53.7 (r 19.1–88.5) | 0.16 | 1.0 | |
| Gender | female | 35 p (49%) | 29 (27%) | 0.005 * | 0.078 |
| male | 36 p (51%) | 76 (70%) | |||
| unknown | 0 p | 3 p (3%) | |||
| T-stage 2 | 1 | 4 p (6%) | 9 p (8%) | 0.40 | 1.0 |
| 2 | 30 p (42%) | 32 p (30%) | |||
| 3 | 23 p (32%) | 41 p (38%) | |||
| 4 | 14 p (20%) | 26 p (24%) | |||
| M-stage 2 | 0 | 71 p (100%) | 108 p (100%) | - | - |
| 1 | 0 p (0%) | 0 p (0%) | |||
| N-stage 2 | 0 | 69 p (97%) | 108 p (100%) | 0.16 | 1.0 |
| 1 | 2 p (3%) | 0 p | |||
| Grading 3 | 1 | 0 p (0%) | 0 p (0%) | 0.88 | 1.0 |
| 2 | 28 p (39%) | 44 p (40%) | |||
| 3 | 43 p (51%) | 64 p (60%) | |||
| AJCC-Stage 2 | IIA | 9 p (13%) | 15 (14%) | 0.0025 * | 0.045 * |
| IIB | 4 p (6%) | 32 (29%) | |||
| III | 48 p (68%) | 61 (58%) | |||
| Margin-status | positive | 12 p (17%) | 28 p (26%) | 0.011 | 0.18 |
| negative | 53 p (75%) | 76 p (70%) | |||
| unknown | 2 p (3%) | 3 p (3%) | |||
| no resection | 4 p (6%) | 1 p (1%) | |||
| RT type | post-operative | 15 p (21%) | 32 (29%) | <0.001 * | 0.007 * |
| neoadjuvant | 52 p (72%) | 75 p (70%) | |||
| definitive | 4 p (6%) | 1 p (1%) | |||
| Total RT Dose | m 50 Gy(r 28–70 Gy) | m 50 Gy(r 38–50Gy) | <0.001 * | <0.001 * | |
| Chemotherapy | 3/71 p (4%) | 64 p (59%) | <0.001 * | <0.001 * | |
| Median OS | 40.1 (r 6.0–105.5) | 39.9 (r 4.2–130.4) | 0.53 | 1.0 |
| Combined Cohort | ||
|---|---|---|
| Feature | HR (95% CI) | p-Value |
| Anatomic region | 0.58 (0.33–1) | 0.067 |
| Localization | 1.2 (0.95–1.5) | 0.12 |
| Image pattern | 0.94 (0.59–1.5) | 0.8 |
| Borders | 1.3 (0.86–1.9) | 0.22 |
| Maximal diameter without tail (in mm) | 1 (1–1) | 0.022 |
| Dominant STIR signal intensity | 1.3 (0.45–3.5) | 0.66 |
| STIR homogeneity | 1.5 (0.74–2.9) | 0.27 |
| Tumor contrast enhancement | 0.74 (0.52–1.1) | 0.1 |
| Homogeneity of Tumor contrast enhancement | 1 (0.54–1.9) | 0.98 |
| Tail sign | 1.5 (0.86–2.6) | 0.16 |
| Vascularization | 0.95 (0.47–1.9) | 0.88 |
| Necrosis | 1.9 (1–3.6) | 0.039 |
| Edema perilesional (in mm) | 1.1 (0.6–1.9) | 0.81 |
| Edema diameter | 1 (1–1) | 0.043 |
| Contrast enhancement perilesional | 1.5 (0.85–2.6) | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peeken, J.C.; Neumann, J.; Asadpour, R.; Leonhardt, Y.; Moreira, J.R.; Hippe, D.S.; Klymenko, O.; Foreman, S.C.; von Schacky, C.E.; Spraker, M.B.; et al. Prognostic Assessment in High-Grade Soft-Tissue Sarcoma Patients: A Comparison of Semantic Image Analysis and Radiomics. Cancers 2021, 13, 1929. https://doi.org/10.3390/cancers13081929
Peeken JC, Neumann J, Asadpour R, Leonhardt Y, Moreira JR, Hippe DS, Klymenko O, Foreman SC, von Schacky CE, Spraker MB, et al. Prognostic Assessment in High-Grade Soft-Tissue Sarcoma Patients: A Comparison of Semantic Image Analysis and Radiomics. Cancers. 2021; 13(8):1929. https://doi.org/10.3390/cancers13081929
Chicago/Turabian StylePeeken, Jan C., Jan Neumann, Rebecca Asadpour, Yannik Leonhardt, Joao R. Moreira, Daniel S. Hippe, Olena Klymenko, Sarah C. Foreman, Claudio E. von Schacky, Matthew B. Spraker, and et al. 2021. "Prognostic Assessment in High-Grade Soft-Tissue Sarcoma Patients: A Comparison of Semantic Image Analysis and Radiomics" Cancers 13, no. 8: 1929. https://doi.org/10.3390/cancers13081929