
The Effects of In-Plane Spatial Resolution on CT-Based Radiomic Features’ Stability with and without ComBat Harmonization

 , , , ,
, , , ,  , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
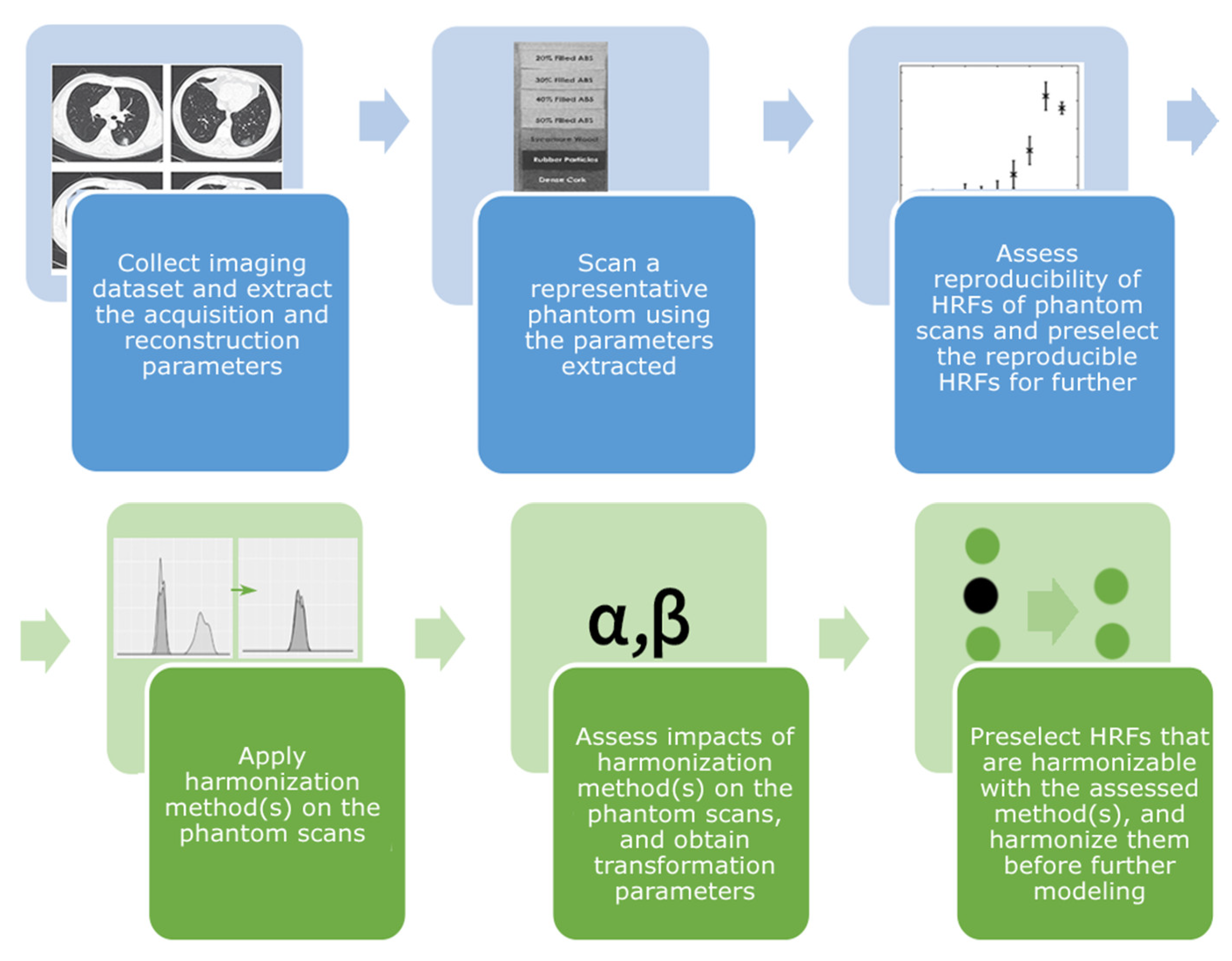
2. Materials and Methods
2.1. Phantom Data
2.2. Interpolation and Image Resampling
2.3. HRFs Extraction
2.4. ComBat Harmonization
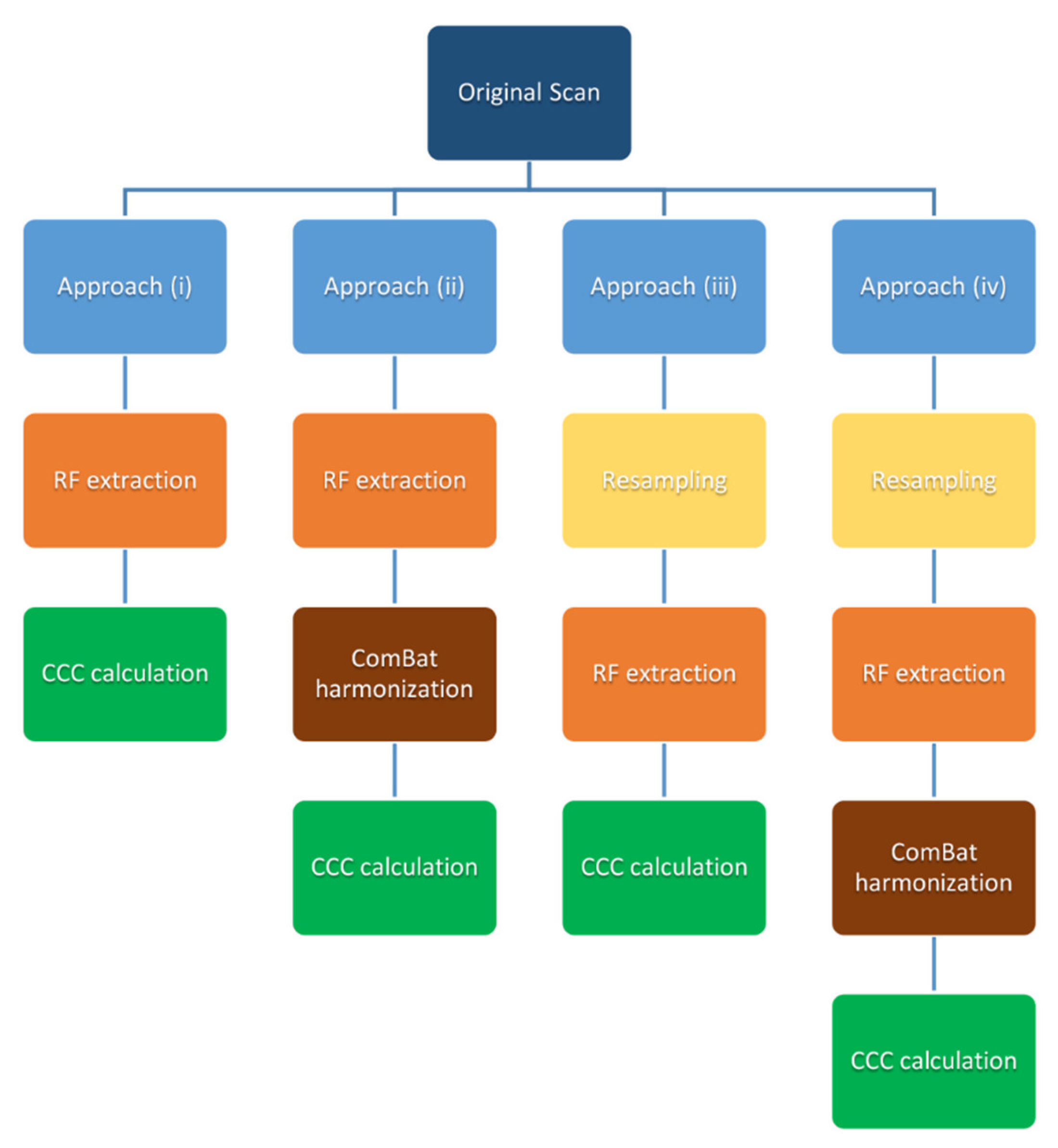
2.5. Statistical Analysis
3. Results
3.1. Approach (i): Effects of IPR on the Reproducibility of HRFs
3.2. Approach (ii): ComBat Harmonization of HRFs Extracted from Original Scans
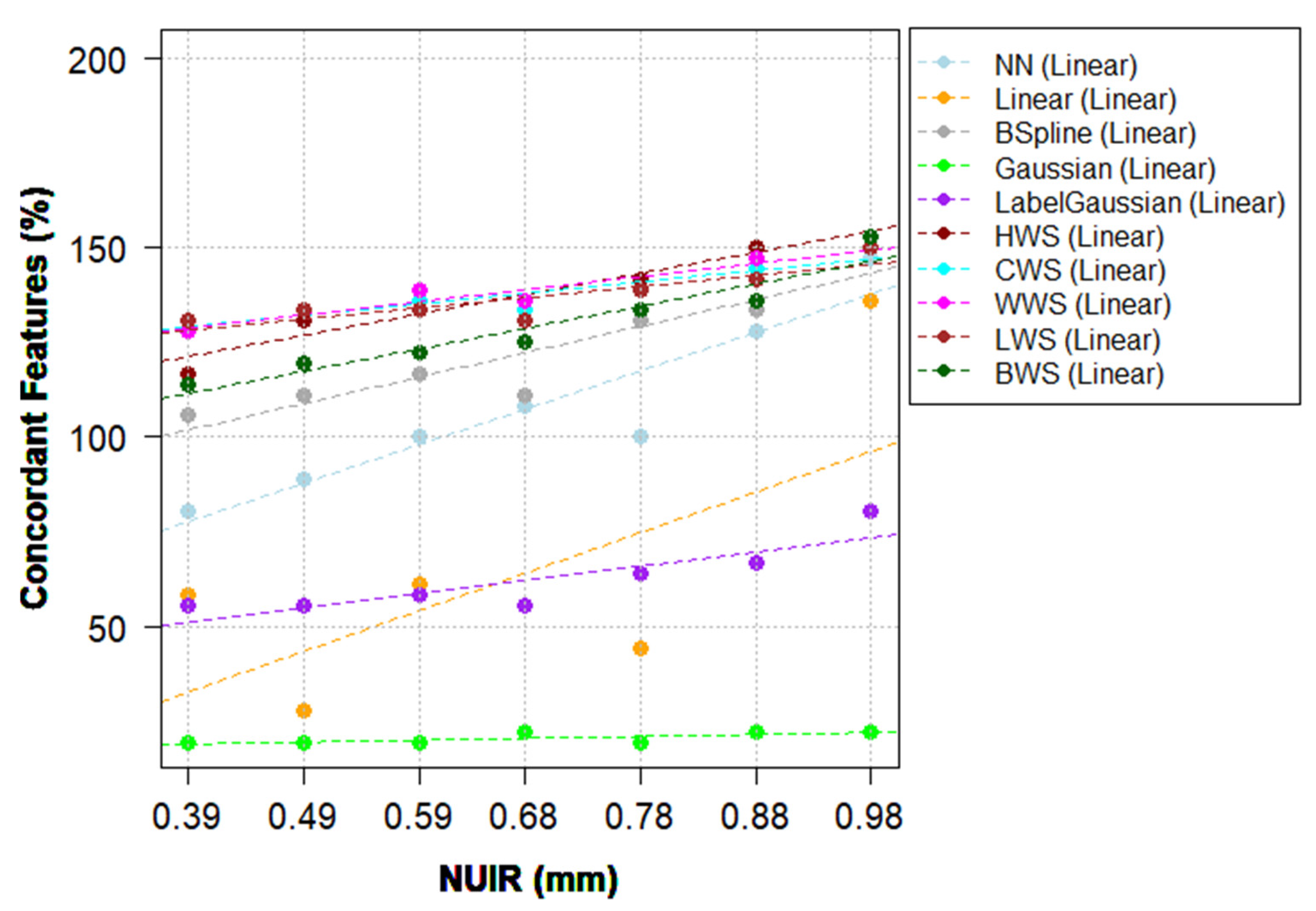
3.3. Approach (iii): The Effects of Different IMs and NUIR on HRFs
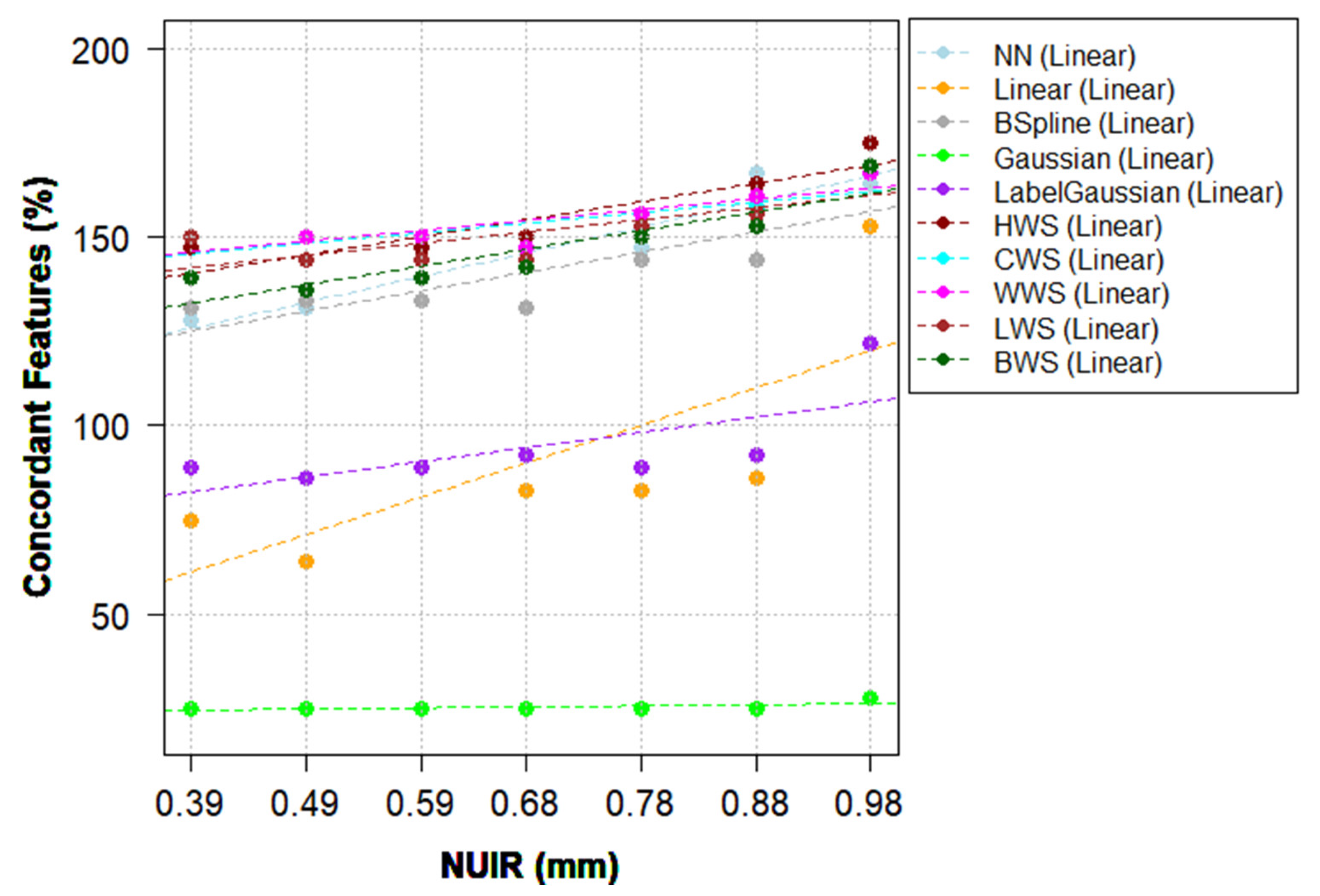
3.4. Approach (iv): The Combination of IMs and ComBat Harmonization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walsh, S.; De Jong, E.E.; Van Timmeren, J.E.; Ibrahim, A.; Compter, I.; Peerlings, J.; Sanduleanu, S.; Refaee, T.; Keek, S.; LaRue, R.T.; et al. Decision Support Systems in Oncology. JCO Clin. Cancer Inform. 2019, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Leijenaar, R.T.; Deist, T.M.; Peerlings, J.; De Jong, E.E.; Van Timmeren, J.; Sanduleanu, S.; LaRue, R.T.; Even, A.J.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, A.; Vallières, M.; Woodruff, H.; Primakov, S.; Beheshti, M.; Keek, S.; Refaee, T.; Sanduleanu, S.; Walsh, S.; Morin, O.; et al. Radiomics analysis for clinical decision support in nuclear medicine. Semin. Nucl. Med. 2019, 49, 438–449. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The process and the challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.S.; Blott, B.H.; Hames, T.K. Review of neural network applications in medical imaging and signal processing. Med. Biol. Eng. Comput. 1992, 30, 449–464. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, L.; Ring, P.; Thomsen, C.; Henriksen, O. Texture analysis in quantitative MR imaging. Tissue characterisation of normal brain and intracranial tumours at 1.5 T. Acta Radiol. 1995, 36, 127–135. [Google Scholar]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A.; et al. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Refaee, T.; Wu, G.; Ibrahim, A.; Halilaj, I.; Leijenaar, R.T.; Rogers, W.; Gietema, H.A.; Hendriks, L.E.; Lambin, P.; Woodruff, H.C. The emerging role of radiomics in COPD and lung cancer. Respiration 2020, 99, 99–107. [Google Scholar] [CrossRef]
- Rogers, W.; Seetha, S.T.; Refaee, T.A.G.; Lieverse, R.I.Y.; Granzier, R.W.Y.; Ibrahim, A.; Keek, S.A.; Sanduleanu, S.; Primakov, S.P.; Beuque, M.P.L.; et al. Radiomics: From qualitative to quantitative imaging. Br. J. Radiol. 2020, 93, 20190948. [Google Scholar] [CrossRef]
- Mackin, D.; Fave, X.; Zhang, L.; Fried, D.; Yang, J.; Taylor, B.; Rodriguez-Rivera, E.; Dodge, C.; Jones, A.K.; Court, L. Measuring computed tomography scanner variability of radiomics features. Investig. Radiol. 2015, 50, 757–765. [Google Scholar] [CrossRef]
- Berenguer, R.; Pastor-Juan, M.D.R.; Canales-Vázquez, J.; Castro-García, M.; Villas, M.V.; Legorburo, F.M.; Sabater, S. Radiomics of CT features may be nonreproducible and redundant: Influence of CT acquisition parameters. Radiology 2018, 288, 407–415. [Google Scholar] [CrossRef]
- Strimbu, K.; Tavel, J.A. What are biomarkers? Curr. Opin. HIV AIDS 2010, 5, 463. [Google Scholar] [CrossRef]
- Davis, A.T.; Palmer, A.L.; Pani, S.; Nisbet, A. Assessment of the variation in CT scanner performance (image quality and Hounsfield units) with scan parameters, for image optimisation in radiotherapy treatment planning. Phys. Med. 2018, 45, 59–64. [Google Scholar] [CrossRef]
- Ibrahim, A.; Primakov, S.; Beuque, M.; Woodruff, H.; Halilaj, I.; Wu, G.; Refaee, T.; Granzier, R.; Widaatalla, Y.; Hustinx, R.; et al. Radiomics for precision medicine: Current challenges, future prospects, and the proposal of a new framework. Methods 2021, 188, 20–29. [Google Scholar] [CrossRef]
- Van Timmeren, J.E.; Leijenaar, R.T.; van Elmpt, W.; Wang, J.; Zhang, Z.; Dekker, A.; Lambin, P. Test-retest data for radiomics feature stability analysis: Generalizable or study-specific? Tomography 2016, 2, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Peerlings, J.; Woodruff, H.C.; Winfield, J.M.; Ibrahim, A.; Van Beers, B.E.; Heerschap, A.; Jackson, A.; Wildberger, J.E.; Mottaghy, F.M.; DeSouza, N.M.; et al. Stability of radiomics features in apparent diffusion coefficient maps from a multi-centre test-retest trial. Sci. Rep. 2019, 9, 4800. [Google Scholar] [CrossRef] [PubMed]
- Zhovannik, I.; Bussink, J.; Traverso, A.; Shi, Z.; Kalendralis, P.; Wee, L.; Dekker, A.; Fijten, R.; Monshouwer, R. Learning from scanners: Bias reduction and feature correction in radiomics. Clin. Transl. Radiat. Oncol. 2019, 19, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Traverso, A.; Wee, L.; Dekker, A.; Gillies, R. Repeatability and reproducibility of radiomic features: A systematic review. Int. J. Radiat. Oncol. 2018, 102, 1143–1158. [Google Scholar] [CrossRef] [PubMed]
- Papanikolaou, N.; Matos, C.; Koh, D.M. How to develop a meaningful radiomic signature for clinical use in oncologic patients. Cancer Imaging 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Shafiq-Ul-Hassan, M.; Latifi, K.; Zhang, G.; Ullah, G.; Gillies, R.; Moros, E. Voxel size and gray level normalization of CT radiomic features in lung cancer. Sci. Rep. 2018, 8, 10545. [Google Scholar] [CrossRef] [PubMed]
- Shafiq-Ul-Hassan, M.; Zhang, G.G.; Latifi, K.; Ullah, G.; Hunt, D.C.; Balagurunathan, Y.; Abdalah, M.A.; Schabath, M.B.; Goldgof, D.G.; Mackin, D.; et al. Intrinsic dependencies of CT radiomic features on voxel size and number of gray levels. Med. Phys. 2017, 44, 1050–1062. [Google Scholar] [CrossRef] [PubMed]
- Thévenaz, P.; Blu, T.; Unser, M. Image interpolation and resampling of medical imaging, processing and analysis. In Handbook of Medical Imaging, Processing and Analysis; Academic Press: Cambridge, MA, USA, 2000. [Google Scholar]
- Haddad, M.; Porenta, G. Impact of reorientation algorithms on quantitative myocardial SPECT perfusion imaging. J. Nucl. Med. 1998, 39, 1864–1869. [Google Scholar]
- Menon, S.; Damian, A.; Hu, S.; Ravi, N.; Rudin, C. PULSE: Self-supervised photo upsampling via latent space exploration of generative models. In Proceedings of the 2020 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Seattle, WA, USA, 16–18 June 2020; pp. 2437–2445. Available online: openaccess.thecvf.com (accessed on 15 March 2021).
- Parker, J.A.; Kenyon, R.V.; Troxel, D.E. Comparison of interpolating methods for image resampling. IEEE Trans. Med. Imaging 1983, 2, 31–39. [Google Scholar] [CrossRef]
- Johnson, W.E.; Li, C.; Rabinovic, A. Adjusting batch effects in microarray expression data using empirical Bayes methods. Biostatistics 2006, 8, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Orlhac, F.; Frouin, F.; Nioche, C.; Ayache, N.; Buvat, I. Validation of a method to compensate multicenter effects affecting CT radiomic features. Radiology 2019, 291, 53–59. [Google Scholar] [CrossRef]
- Orlhac, F.; Boughdad, S.; Philippe, C.; Stalla-Bourdillon, H.; Nioche, C.; Champion, L.; Soussan, M.; Frouin, F.; Frouin, V.; Buvat, I. A postreconstruction harmonization method for multicenter radiomic studies in PET. J. Nucl. Med. 2018, 59, 1321–1328. [Google Scholar] [CrossRef]
- Mackin, D.; Fave, X.; Zhang, L.; Fried, D.; Yang, J.; Taylor, B.; Rodriguez-Rivera, E.; Dodge, C.; Jones, A.K.; Court, L. Credence cartridge radiomics phantom CT Scans. The Cancer Imaging Archive (TCIA) 2017. Available online: https://wiki.cancerimagingarchive.net/display/Public/Credence+Cartridge+Radiomics+Phantom+CT+Scans (accessed on 5 March 2021).
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Lowekamp, B.C.; Chen, D.T.; Eibanez, L.; Eblezek, D. The design of SimpleITK. Front. Aging Neurosci. 2013, 7, 45. [Google Scholar] [CrossRef]
- Hou, H.; Andrews, H.C. Cubic splines for image interpolation and digital filtering. IEEE Trans. Acoust. Speech Signal Process. 1978, 26, 508–517. [Google Scholar] [CrossRef]
- Meijering, E.H.; Niessen, W.J.; Viergever, M.A. Quantitative evaluation of convolution-based methods for medical image interpolation. Med. Image Anal. 2001, 5, 111–126. [Google Scholar] [CrossRef]
- Stevenson, M.; Stevenson, M.M.; BiasedUrn, I. Package “epiR.”. Available online: https://vps.fmvz.usp.br/CRAN/web/packages/epiR/epiR.pdf (accessed on 10 March 2021).
- R Core Team. R Language Definition; R Foundation for Statistical Computing: Vienna, Austria, 2000. [Google Scholar]
- Gandrud, C. Reproducible Research with R and R Studio; Productivity Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Lin, L.I.-K. A Concordance Correlation Coefficient to Evaluate Reproducibility. Biometrics 1989, 45, 255. [Google Scholar] [CrossRef]
- McBride, G.B. A Proposal for Strength-of-Agreement Criteria for Lin’s Concordance Correlation Coefficient; National Institute of Water & Atmospheric Research Ltd.: Hamilton, New Zealand, 2005. [Google Scholar]
- Zar, J.H. Spearman Rank Correlation. In Encyclopedia of Biostatistics; Wiley: Hoboken, NJ, USA, 2005. [Google Scholar]
- LaRue, R.T.H.M.; Van Timmeren, J.E.; De Jong, E.E.C.; Feliciani, G.; Leijenaar, R.T.H.; Schreurs, W.M.J.; Sosef, M.N.; Raat, F.H.P.J.; Van Der Zande, F.H.R.; Das, M.; et al. Influence of gray level discretization on radiomic feature stability for different CT scanners, tube currents and slice thicknesses: A comprehensive phantom study. Acta Oncol. 2017, 56, 1544–1553. [Google Scholar] [CrossRef]
- Ligero, M.; Jordi-Ollero, O.; Bernatowicz, K.; Garcia-Ruiz, A.; Delgado-Muñoz, E.; Leiva, D.; Mast, R.; Suarez, C.; Sala-Llonch, R.; Calvo, N.; et al. Minimizing acquisition-related radiomics variability by image resampling and batch effect correction to allow for large-scale data analysis. Eur. Radiol. 2021, 31, 1460–1470. [Google Scholar] [CrossRef] [PubMed]
- Da-Ano, R.; Masson, I.; Lucia, F.; Doré, M.; Robin, P.; Alfieri, J.; Rousseau, C.; Mervoyer, A.; Reinhold, C.; Castelli, J.; et al. Performance comparison of modified ComBat for harmonization of radiomic features for multicenter studies. Sci. Rep. 2020, 10, 10248. [Google Scholar] [CrossRef] [PubMed]
- Vetter, T.R.; Schober, P. Agreement analysis. Anesth. Analg. 2018, 126, 2123–2128. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scanner | Pixel Spacing (mm2) | |
|---|---|---|
| Discovery STE | LightSpeed Pro 32 | |
| CCR-2-001 | CCR-2-022 | 0.39 × 0.39 |
| CCR-2-002 | CCR-2-023 | 0.49 × 0.49 |
| CCR-2-003 | CCR-2-024 | 0.59 × 0.59 |
| CCR-2-004 | CCR-2-025 | 0.68 × 0.68 |
| CCR-2-005 | CCR-2-026 | 0.78 × 0.78 |
| CCR-2-006 | CCR-2-027 | 0.88 × 0.88 |
| CCR-2-007 | CCR-2-028 | 0.98 × 0.98 |
| Scan | CCR-2-001 | CCR-2-002 | CCR-2-003 | CCR-2-004 | CCR-2-005 | CCR-2-006 |
|---|---|---|---|---|---|---|
| CCR-2-002 | 75 (82.4%) | |||||
| CCR-2-003 | 57 (62.6%) | 78 (85.7%) | ||||
| CCR-2-004 | 53 (58.2%) | 64 (70.3%) | 83 (91.2%) | |||
| CCR-2-005 | 50 (54.9%) | 61 (67.0%) | 72 (79.1%) | 86 (94.5%) | ||
| CCR-2-006 | 51 (56.0%) | 58 (63.7%) | 68 (74.7%) | 76 (83.5%) | 85 (93.4%) | |
| CCR-2-007 | 39 (42.9%) | 42 (46.2%) | 44 (48.4%) | 52 (57.1%) | 60 (64.9%) | 83 (91.2%) |
| Scan | CCR-2-001 | CCR-2-002 | CCR-2-003 | CCR-2-004 | CCR-2-005 | CCR-2-006 |
|---|---|---|---|---|---|---|
| CCR-2-002 | 79 (86.8%) | |||||
| CCR-2-003 | 65 (71.4%) | 79 (86.8%) | ||||
| CCR-2-004 | 59 (64.8%) | 70 (76.9%) | 83 (91.2%) | |||
| CCR-2-005 | 58 (63.7%) | 66 (72.5%) | 75 (82.4%) | 87 (95.6%) | ||
| CCR-2-006 | 57 (62.6%) | 65 (71.4%) | 70 (76.9%) | 84 (92.3%) | 86 (94.5%) | |
| CCR-2-007 | 48 (52.7%) | 55 (60.4%) | 57 (62.6%) | 60 (65.9%) | 73 (80.2%) | 84 (92.3%) |
| Scan | CCR-2-001 | CCR-2-002 | CCR-2-003 | CCR-2-004 | CCR-2-005 | CCR-2-006 |
|---|---|---|---|---|---|---|
| CCR-2-002 | 89 (97.8%) | |||||
| CCR-2-003 | 86 (94.5%) | 88 (96.7%) | ||||
| CCR-2-004 | 86 (94.5%) | 85 (93.4%) | 88 (96.7%) | |||
| CCR-2-005 | 86 (94.5%) | 88 (96.7%) | 91 (100%) | 89 (97.8%) | ||
| CCR-2-006 | 78 (85.7%) | 77 (84.6%) | 83 (91.2%) | 79 (86.8%) | 88 (96.7%) | |
| CCR-2-007 | 53 (58.2%) | 53 (58.2%) | 55 (60.4%) | 54 (59.3%) | 60 (65.9%) | 85 (93.4%) |
| Scan | CCR-2-022 | CCR-2-023 | CCR-2-024 | CCR-2-025 | CCR-2-026 | CCR-2-027 |
|---|---|---|---|---|---|---|
| CCR-2-023 | 89 (97.8%) | |||||
| CCR-2-024 | 86 (94.5%) | 88 (96.7%) | ||||
| CCR-2-025 | 86 (94.5%) | 85 (93.4%) | 88 (96.7%) | |||
| CCR-2-026 | 86 (94.5%) | 88 (96.7%) | 91 (100%) | 89 (97.8%) | ||
| CCR-2-027 | 79 (86.8%) | 78 (85.7%) | 84 (92.3%) | 84 (92.3%) | 89 (97.8%) | |
| CCR-2-028 | 57 (62.6%) | 61 (67.0%) | 60 (65.9%) | 59 (64.8%) | 72 (79.1%) | 85 (93.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, A.; Refaee, T.; Primakov, S.; Barufaldi, B.; Acciavatti, R.J.; Granzier, R.W.Y.; Hustinx, R.; Mottaghy, F.M.; Woodruff, H.C.; Wildberger, J.E.; et al. The Effects of In-Plane Spatial Resolution on CT-Based Radiomic Features’ Stability with and without ComBat Harmonization. Cancers 2021, 13, 1848. https://doi.org/10.3390/cancers13081848
Ibrahim A, Refaee T, Primakov S, Barufaldi B, Acciavatti RJ, Granzier RWY, Hustinx R, Mottaghy FM, Woodruff HC, Wildberger JE, et al. The Effects of In-Plane Spatial Resolution on CT-Based Radiomic Features’ Stability with and without ComBat Harmonization. Cancers. 2021; 13(8):1848. https://doi.org/10.3390/cancers13081848
Chicago/Turabian StyleIbrahim, Abdalla, Turkey Refaee, Sergey Primakov, Bruno Barufaldi, Raymond J. Acciavatti, Renée W. Y. Granzier, Roland Hustinx, Felix M. Mottaghy, Henry C. Woodruff, Joachim E. Wildberger, and et al. 2021. "The Effects of In-Plane Spatial Resolution on CT-Based Radiomic Features’ Stability with and without ComBat Harmonization" Cancers 13, no. 8: 1848. https://doi.org/10.3390/cancers13081848