
Prognostic Significance of Glucocorticoid Receptor Expression in Cancer: A Systematic Review and Meta-Analysis


Abstract
:Simple Summary
Abstract
1. Background
2. Methods
2.1. Study Registration
2.2. Data Sources and Search Strategy
2.3. Study Selection and Inclusion Criteria
2.4. Evaluation of Quality and Risk of Bias
2.5. Statistical Analysis for Meta-Analysis
3. Results
3.1. QUIPS Assessment
3.2. Overall Survival
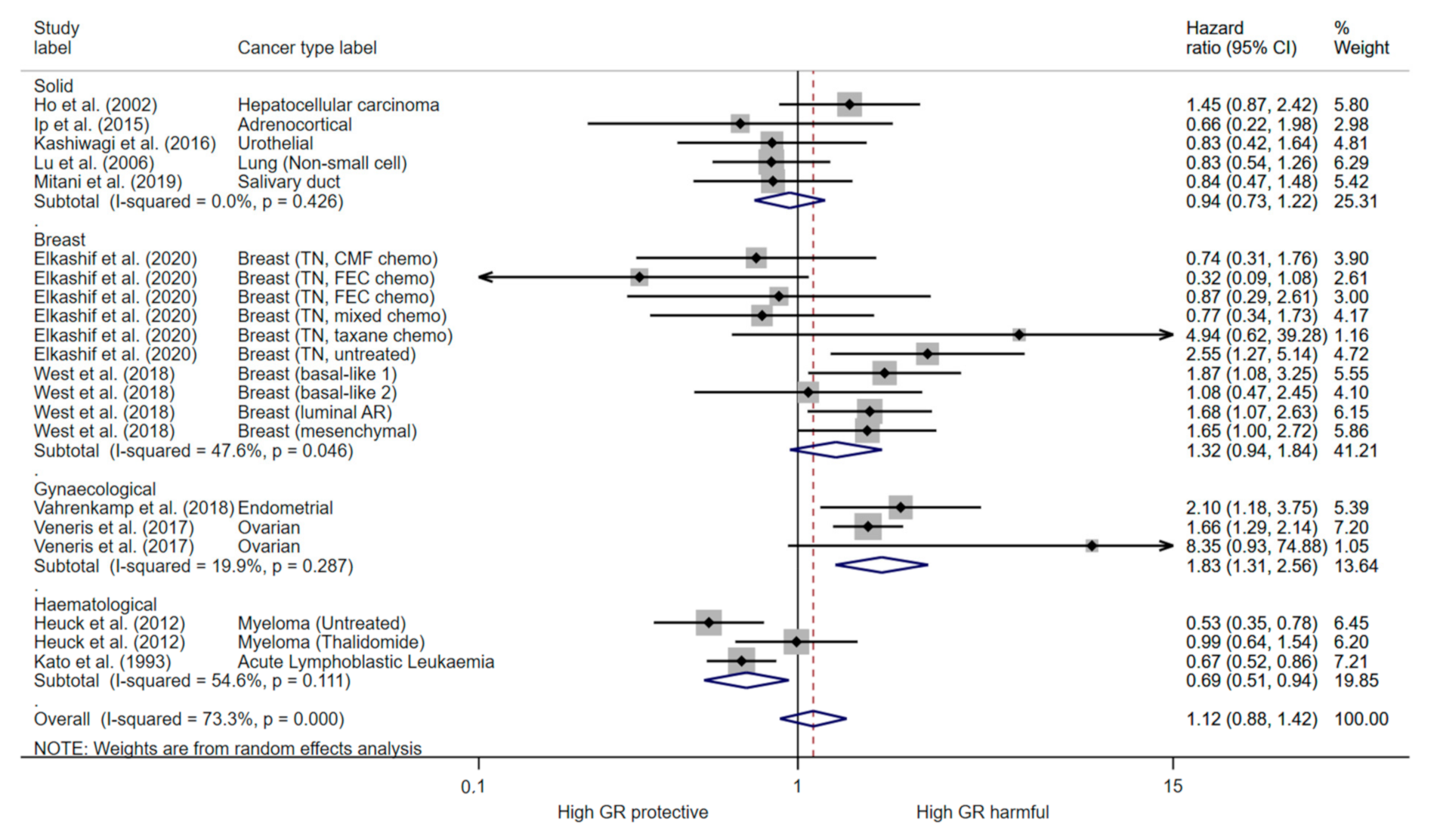
3.3. Progression Free Survival
3.4. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- McKay, L.; Cidlowski, J. Corticosteroids in the treatment of neoplasms. In Cancer Medicine; Kufe, D.W., Pollock, R.E., Weichselbaum, R.R., Blast, R.C., Jr., Gansler, T.S., Holland, J.F., Frei, E., III, Eds.; BC Decker: Hamilton, ON, USA, 2003. [Google Scholar]
- Pufall, M.A. Glucocorticoids and Cancer. Adv. Exp. Med. Biol. 2015, 872, 315–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrelli, F.; Bukovec, R.; Perego, G.; Luisa, R.; Luciani, A.; Zaniboni, A.; Ghidini, A. Association of steroid use with survival in solid tumours. Eur. J. Cancer 2020, 141, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Mattern, J.; Haferkamp, A.; Pfitzenmaier, J.; Hohenfellner, M.; Rittgen, W.; Edler, L.; Debatin, K.M.; Groene, E.; Herr, I. Corticosteroid-induced chemotherapy resistance in urological cancers. Cancer Biol. Ther. 2006, 5, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ní Chonghaile, T.; Concannon, C.G.; Szegezdi, E.; Gorman, A.M.; Samali, A. Dexamethasone inhibits apoptosis in C6 glioma cells through increased expression of Bcl-XL. Apoptosis 2006, 11, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Runnebaum, I.B.; Brüning, A. Glucocorticoids inhibit cell death in ovarian cancer and up-regulate caspase inhibitor cIAP2. Clin. Cancer Res. 2005, 11, 6325–6332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrella, A.; Ercolino, S.F.; Festa, M.; Gentilella, A.; Tosco, A.; Conzen, S.D.; Parente, L. Dexamethasone inhibits TRAIL-induced apoptosis of thyroid cancer cells via Bcl-xL induction. Eur. J. Cancer 2006, 42, 3287–3293. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.T.; Wang, L.H. New dimension of glucocorticoids in cancer treatment. Steroids 2016, 111, 84–88. [Google Scholar] [CrossRef] [Green Version]
- Obradović, M.M.S.; Hamelin, B.; Manevski, N.; Couto, J.P.; Sethi, A.; Coissieux, M.-M.; Münst, S.; Okamoto, R.; Kohler, H.; Schmidt, A.; et al. Glucocorticoids promote breast cancer metastasis. Nature 2019, 567, 540–544. [Google Scholar] [CrossRef]
- Sorrentino, G.; Ruggeri, N.; Zannini, A.; Ingallina, E.; Bertolio, R.; Marotta, C.; Neri, C.; Cappuzzello, E.; Forcato, M.; Rosato, A.; et al. Glucocorticoid receptor signalling activates YAP in breast cancer. Nat. Commun. 2017, 8, 14073. [Google Scholar] [CrossRef] [Green Version]
- McKay, L.; Cidlowski, J.A. Physiologic and pharmacologic effects of corticosteroids. In Cancer Medicine, 6th ed.; Kufe, D., Pollock, R.E., Weichselbaum, R.R., Eds.; BC Decker: Hamilton, ON, USA, 2003. [Google Scholar]
- Annett, S.; Moore, G.; Robson, T. FK506 binding proteins and inflammation related signalling pathways; basic biology, current status and future prospects for pharmacological intervention. Pharmacol. Ther. 2020, 215, 107623. [Google Scholar] [CrossRef]
- Kumar, R.; Thompson, E.B. Gene regulation by the glucocorticoid receptor: Structure:function relationship. J. Steroid Biochem. Mol. Biol. 2005, 94, 383–394. [Google Scholar] [CrossRef]
- Ray, A.; Prefontaine, K.E. Physical association and functional antagonism between the p65 subunit of transcription factor NF-kappa B and the glucocorticoid receptor. Proc. Natl. Acad. Sci. USA 1994, 91, 752–756. [Google Scholar] [CrossRef] [Green Version]
- Schüle, R.; Rangarajan, P.; Kliewer, S.; Ransone, L.J.; Bolado, J.; Yang, N.; Verma, I.M.; Evans, R.M. Functional antagonism between oncoprotein c-Jun and the glucocorticoid receptor. Cell 1990, 62, 1217–1226. [Google Scholar] [CrossRef]
- Wu, W.; Chaudhuri, S.; Brickley, D.R.; Pang, D.; Karrison, T.; Conzen, S.D. Microarray analysis reveals glucocorticoid-regulated survival genes that are associated with inhibition of apoptosis in breast epithelial cells. Cancer Res. 2004, 64, 1757–1764. [Google Scholar] [CrossRef] [Green Version]
- McNamara, K.M.; Kannai, A.; Sasano, H. Possible roles for glucocorticoid signalling in breast cancer. Mol. Cell. Endocrinol. 2018, 466, 38–50. [Google Scholar] [CrossRef]
- Kumar, R. Emerging role of glucocorticoid receptor in castration resistant prostate cancer: A potential therapeutic target. J. Cancer 2020, 11, 696–701. [Google Scholar] [CrossRef] [Green Version]
- Sitruk-Ware, R.; Spitz, I.M. Pharmacological properties of mifepristone: Toxicology and safety in animal and human studies. Contraception 2003, 68, 409–420. [Google Scholar] [CrossRef]
- Johanssen, S.; Allolio, B. Mifepristone (RU 486) in Cushing’s syndrome. Eur. J. Endocrinol. 2007, 157, 561–569. [Google Scholar] [CrossRef]
- Bamberger, C.M.; Chrousos, G.P. The glucocorticoid receptor and RU 486 in man. Ann. N. Y. Acad. Sci. 1995, 761, 296–310. [Google Scholar] [CrossRef]
- Tieszen, C.R.; Goyeneche, A.A.; Brandhagen, B.N.; Ortbahn, C.T.; Telleria, C.M. Antiprogestin mifepristone inhibits the growth of cancer cells of reproductive and non-reproductive origin regardless of progesterone receptor expression. BMC Cancer 2011, 11, 207. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.-F.; Kawachi, M.H.; Lin, F.-F.; Stallcup, M.R.; Grunberg, S.M. Growth inhibition of androgen-insensitive human prostate carcinoma cells by a 19-norsteroid derivative agent, mifepristone. Prostate 1995, 26, 194–204. [Google Scholar] [CrossRef]
- Rocereto, T.F.; Saul, H.M.; Aikins, J.A., Jr.; Paulson, J. Phase II study of mifepristone (RU486) in refractory ovarian cancer. Gynecol. Oncol. 2000, 77, 429–432. [Google Scholar] [CrossRef]
- Taplin, M.E.; Manola, J.; Oh, W.K.; Kantoff, P.W.; Bubley, G.J.; Smith, M.; Barb, D.; Mantzoros, C.; Gelmann, E.P.; Balk, S.P. A phase II study of mifepristone (RU-486) in castration-resistant prostate cancer, with a correlative assessment of androgen-related hormones. BJU Int. 2008, 101, 1084–1089. [Google Scholar] [CrossRef]
- Skor, M.N.; Wonder, E.L.; Kocherginsky, M.; Goyal, A.; Hall, B.A.; Cai, Y.; Conzen, S.D. Glucocorticoid receptor antagonism as a novel therapy for triple-negative breast cancer. Clin. Cancer Res. 2013, 19, 6163–6172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stringer, E.M.; Skor, M.N.; Fleming, G.F.; Conzen, S.D. The role of the glucocorticoid receptor (GR) in inhibiting chemotherapy-induced apoptosis in high-grade serous ovarian carcinoma (HGS-OvCa). J. Clin. Oncol. 2013, 31, 11101. [Google Scholar] [CrossRef]
- Block, T.S.; Murphy, T.I.; Munster, P.N.; Nguyen, D.P.; Lynch, F.J. Glucocorticoid receptor expression in 20 solid tumor types using immunohistochemistry assay. Cancer Manag. Res. 2017, 9, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Matthews, L.C.; Berry, A.A.; Morgan, D.J.; Poolman, T.M.; Bauer, K.; Kramer, F.; Spiller, D.G.; Richardson, R.V.; Chapman, K.E.; Farrow, S.N.; et al. Glucocorticoid receptor regulates accurate chromosome segregation and is associated with malignancy. Proc. Natl. Acad. Sci. USA 2015, 112, 5479–5484. [Google Scholar] [CrossRef] [Green Version]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Allegra, J.C.; Lippman, M.E.; Simon, R.; Thompson, E.B.; Barlock, A.; Green, L.; Huff, K.K.; Do, H.M.; Aitken, S.C.; Warren, R. Association between steroid hormone receptor status and disease-free interval in breast cancer. Cancer Treat. Rep. 1979, 63, 1271–1277. [Google Scholar]
- Theocharis, S.; Kouraklis, G.; Margeli, A.; Agapitos, E.; Ninos, S.; Karatzas, G.; Koutselinis, A. Glucocorticoid receptor (GR) immunohistochemical expression is correlated with cell cycle-related molecules in human colon cancer. Dig. Dis. Sci. 2003, 48, 1745–1750. [Google Scholar] [CrossRef] [PubMed]
- Woenckhaus, J.; Franke, F.E.; Hackethal, A.; Von Georgi, R.; Münstedt, K. Glucocorticosteroid receptors in ovarian carcinomas. Oncol. Rep. 2006, 15, 1137–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lien, H.C.; Lu, Y.S.; Shun, C.T.; Yao, Y.T.; Chang, W.C.; Cheng, A.L. Differential expression of glucocorticoid receptor in carcinomas of the human digestive system. Histopathology 2008, 52, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.; Kocherginsky, M.; Conzen, S.D. Activation of the glucocorticoid receptor is associated with poor prognosis in estrogen receptor-negative breast cancer. Cancer Res. 2011, 71, 6360–6370. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Izumi, K.; Li, Y.; Ishiguro, H.; Miyamoto, H. Contrary regulation of bladder cancer cell proliferation and invasion by dexamethasone-mediated glucocorticoid receptor signals. Mol. Cancer Ther. 2012, 11, 2621–2632. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Lan, X.; Wu, D.; Sunkel, B.; Ye, Z.; Huang, J.; Liu, Z.; Clinton, S.K.; Jin, V.X.; Wang, Q. Ligand-dependent genomic function of glucocorticoid receptor in triple-negative breast cancer. Nat. Commun. 2015, 6, 8323. [Google Scholar] [CrossRef] [Green Version]
- Puhr, M.; Hoefer, J.; Eigentler, A.; Ploner, C.; Handle, F.; Schaefer, G.; Kroon, J.; Leo, A.; Heidegger, I.; Eder, I.; et al. The glucocorticoid receptor is a key player for prostate cancer cell survival and a target for improved antiandrogen therapy. Clin. Cancer Res. 2018, 24, 927–938. [Google Scholar] [CrossRef] [Green Version]
- Kanai, A.; McNamara, K.M.; Iwabuchi, E.; Miki, Y.; Onodera, Y.; Guestini, F.; Khalid, F.; Sagara, Y.; Ohi, Y.; Rai, Y.; et al. Significance of glucocorticoid signaling in triple-negative breast cancer patients: A newly revealed interaction with androgen signaling. Breast Cancer Res. Treat. 2020, 180, 97–110. [Google Scholar] [CrossRef]
- McNamara, K.M.; Guestini, F.; Sauer, T.; Touma, J.; Bukholm, I.R.; Lindstrom, J.C.; Sasano, H.; Geisler, J. In breast cancer subtypes steroid sulfatase (STS) is associated with less aggressive tumour characteristics. Br. J. Cancer 2018, 118, 1208–1216. [Google Scholar] [CrossRef]
- Abduljabbar, R.; Negm, O.H.; Lai, C.F.; Jerjees, D.A.; Al-Kaabi, M.; Hamed, M.R.; Tighe, P.J.; Buluwela, L.; Mukherjee, A.; Green, A.R.; et al. Clinical and biological significance of glucocorticoid receptor (GR) expression in breast cancer. Breast Cancer Res. Treat. 2015, 150, 335–346. [Google Scholar] [CrossRef]
- Elkashif, A.; Bingham, V.; Haddock, P.; Humphries, M.P.; McQuaid, S.; Mullan, P.B.; McCarthy, H.O.; Buckley, N.E. Glucocorticoid receptor expression predicts good outcome in response to taxane-free, anthracycline-based therapy in triple negative breast cancer. J. Oncol. 2020, 2020, 3712825. [Google Scholar] [CrossRef]
- Gokon, Y.; Fujishima, F.; Taniyama, Y.; Ishida, H.; Yamagata, T.; Sawai, T.; Uzuki, M.; Ichikawa, H.; Itakura, Y.; Takahashi, K.; et al. Glucocorticoid receptor and serum- and glucocorticoid-induced kinase-1 in esophageal adenocarcinoma and adjacent Barrett’s esophagus. Pathol. Int. 2020. [Google Scholar] [CrossRef]
- Heuck, C.J.; Szymonifka, J.; Hansen, E.; Shaughnessy, J.D., Jr.; Usmani, S.Z.; van Rhee, F.; Anaissie, E.; Nair, B.; Waheed, S.; Alsayed, Y.; et al. Thalidomide in total therapy 2 overcomes inferior prognosis of myeloma with low expression of the glucocorticoid receptor gene NR3C1. Clin. Cancer Res. 2012, 18, 5499–5506. [Google Scholar] [CrossRef] [Green Version]
- Ho, W.L.; Wu, C.C.; Yeh, D.C.; Chen, J.T.; Huang, C.C.; Lin, Y.L.; Liu, T.J.; P’Eng F, K. Roles of the glucocorticoid receptor in resectable hepatocellular carcinoma. Surgery 2002, 131, 19–25. [Google Scholar] [CrossRef]
- Ip, J.C.; Pang, T.; Glover, A.; Soon, P.; Zhao, J.; Clarke, S.; Robinson, B.G.; Gill, A.J.; Sidhu, S.B. Immunohistochemical validation of overexpressed genes identified by global expression microarrays in adrenocortical carcinoma reveals potential predictive and prognostic biomarkers. Oncologist 2015, 20, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Ishiguro, H.; Kawahara, T.; Zheng, Y.; Netto, G.J.; Miyamoto, H. Reduced glucocorticoid receptor expression predicts bladder tumor recurrence and progression. Am. J. Clin. Pathol. 2014, 142, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Kashiwagi, E.; Fujita, K.; Yamaguchi, S.; Fushimi, H.; Ide, H.; Inoue, S.; Mizushima, T.; Reis, L.O.; Sharma, R.; Netto, G.J.; et al. Expression of steroid hormone receptors and its prognostic significance in urothelial carcinoma of the upper urinary tract. Cancer Biol. Ther. 2016, 17, 1188–1196. [Google Scholar] [CrossRef] [Green Version]
- Kato, G.J.; Quddus, F.F.; Shuster, J.J.; Boyett, J.; Pullen, J.D.; Borowitz, M.J.; Whitehead, V.M.; Crist, W.M.; Leventhal, B.G. High glucocorticoid receptor content of leukemic blasts is a favorable prognostic factor in childhood acute lymphoblastic leukemia. Blood 1993, 82, 2304–2309. [Google Scholar] [CrossRef] [Green Version]
- Kost, B.P.; Beyer, S.; Schroder, L.; Zhou, J.; Mayr, D.; Kuhn, C.; Schulze, S.; Hofmann, S.; Mahner, S.; Jeschke, U.; et al. Glucocorticoid receptor in cervical cancer: An immunhistochemical analysis. Arch. Gynecol. Obstet. 2019, 299, 203–209. [Google Scholar] [CrossRef]
- Lu, Y.S.; Lien, H.C.; Yeh, P.Y.; Kuo, S.H.; Chang, W.C.; Kuo, M.L.; Cheng, A.L. Glucocorticoid receptor expression in advanced non-small cell lung cancer: Clinicopathological correlation and in vitro effect of glucocorticoid on cell growth and chemosensitivity. Lung Cancer 2006, 53, 303–310. [Google Scholar] [CrossRef]
- Mimae, T.; Tsuta, K.; Takahashi, F.; Yoshida, A.; Kondo, T.; Murakami, Y.; Okada, M.; Takeuchi, M.; Asamura, H.; Tsuda, H. Steroid receptor expression in thymomas and thymic carcinomas. Cancer 2011, 117, 4396–4405. [Google Scholar] [CrossRef] [PubMed]
- Mitani, Y.; Lin, S.H.; Pytynia, K.B.; Ferrarotto, R.; El-Naggar, A.K. Reciprocal and autonomous glucocorticoid and androgen receptor activation in salivary duct carcinoma. Clin. Cancer Res. 2020, 26, 1175–1184. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Wang, D.; Yuan, X.; Liu, Y.; Guo, X.; Li, J.; Song, J. Glucocorticoid receptor-IRS-1 axis controls EMT and the metastasis of breast cancers. J. Mol. Cell Biol. 2019, 11, 1042–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, M.; Kim, Y.; Park, Y.; Ahn, H. Taxane-based chemotherapy induced androgen receptor splice variant 7 in patients with castration-resistant prostate cancer: A tissue-based analysis. Sci. Rep. 2019, 9, 16794. [Google Scholar] [CrossRef]
- Surati, M.; Robinson, M.; Nandi, S.; Faoro, L.; Demchuk, C.; Rolle, C.E.; Kanteti, R.; Ferguson, B.D.; Hasina, R.; Gangadhar, T.C.; et al. Proteomic characterization of non-small cell lung cancer in a comprehensive translational thoracic oncology database. J. Clin. Bioinforma. 2011, 1, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Tangen, I.L.; Veneris, J.T.; Halle, M.K.; Werner, H.M.; Trovik, J.; Akslen, L.A.; Salvesen, H.B.; Conzen, S.D.; Fleming, G.F.; Krakstad, C. Expression of glucocorticoid receptor is associated with aggressive primary endometrial cancer and increases from primary to metastatic lesions. Gynecol. Oncol. 2017, 147, 672–677. [Google Scholar] [CrossRef]
- Ueki, S.; Fujishima, F.; Kumagai, T.; Ishida, H.; Okamoto, H.; Takaya, K.; Sato, C.; Taniyma, Y.; Kamei, T.; Sasano, H. GR, Sgk1, and NDRG1 in esophageal squamous cell carcinoma: Their correlation with therapeutic outcome of neoadjuvant chemotherapy. BMC Cancer 2020, 20, 161. [Google Scholar] [CrossRef] [Green Version]
- Vahrenkamp, J.M.; Yang, C.H.; Rodriguez, A.C.; Almomen, A.; Berrett, K.C.; Trujillo, A.N.; Guillen, K.P.; Welm, B.E.; Jarboe, E.A.; Janat-Amsbury, M.M.; et al. Clinical and genomic crosstalk between glucocorticoid receptor and estrogen receptor alpha in endometrial cancer. Cell Rep. 2018, 22, 2995–3005. [Google Scholar] [CrossRef] [Green Version]
- Veneris, J.T.; Darcy, K.M.; Mhawech-Fauceglia, P.; Tian, C.; Lengyel, E.; Lastra, R.R.; Pejovic, T.; Conzen, S.D.; Fleming, G.F. High glucocorticoid receptor expression predicts short progression-free survival in ovarian cancer. Gynecol. Oncol. 2017, 146, 153–160. [Google Scholar] [CrossRef]
- Veneris, J.T.; Huang, L.; Churpek, J.E.; Conzen, S.D.; Fleming, G.F. Glucocorticoid receptor expression is associated with inferior overall survival independent of BRCA mutation status in ovarian cancer. Int. J. Gynecol. Cancer 2019. [Google Scholar] [CrossRef]
- West, D.C.; Kocherginsky, M.; Tonsing-Carter, E.Y.; Dolcen, D.N.; Hosfield, D.J.; Lastra, R.R.; Sinnwell, J.P.; Thompson, K.J.; Bowie, K.R.; Harkless, R.V.; et al. Discovery of a glucocorticoid receptor (GR) activity signature using selective GR antagonism in ER-negative breast cancer. Clin. Cancer Res. 2018, 24, 3433–3446. [Google Scholar] [CrossRef] [Green Version]
- West, D.C.; Pan, D.; Tonsing-Carter, E.Y.; Hernandez, K.M.; Pierce, C.F.; Styke, S.C.; Bowie, K.R.; Garcia, T.I.; Kocherginsky, M.; Conzen, S.D. GR and ER coactivation alters the expression of differentiation genes and associates with improved ER+ breast cancer outcome. Mol. Cancer Res. 2016, 14, 707–719. [Google Scholar] [CrossRef] [Green Version]
- Yakirevich, E.; Matoso, A.; Sabo, E.; Wang, L.J.; Tavares, R.; Meitner, P.; Morris, D.J.; Pareek, G.; Delellis, R.A.; Resnick, M.B. Expression of the glucocorticoid receptor in renal cell neoplasms: An immunohistochemical and quantitative reverse transcriptase polymerase chain reaction study. Hum. Pathol. 2011, 42, 1684–1692. [Google Scholar] [CrossRef]
- Yeh, D.C.; Cheng, S.B.; Yu, C.C.; Ho, W.L.; Wu, C.C.; Liu, T.J.; P’Eng F, K. Role of glucocorticoid receptor in serosa-involved gastric carcinoma after gastrectomy. J. Gastrointest. Surg. 2006, 10, 706–711. [Google Scholar] [CrossRef]
- Karvonen, H.; Arjama, M.; Kaleva, L.; Niininen, W.; Barker, H.; Koivisto-Korander, R.; Tapper, J.; Pakarinen, P.; Lassus, H.; Loukovaara, M.; et al. Glucocorticoids induce differentiation and chemoresistance in ovarian cancer by promoting ROR1-mediated stemness. Cell Death Dis. 2020, 11, 790. [Google Scholar] [CrossRef]
- Veneris, J.T.; Hou, X.; Weroha, S.J.; Heinzen, E.P.; Maurer, M.J.; Oberg, A.L.; Conzen, S.D.; Fleming, G.F. Selective and nonselective GR antagonists in combination with chemotherapy in ovarian cancer PDX models. J. Clin. Oncol. 2019, 37. [Google Scholar] [CrossRef]
- MacKay, H.J.; Freixinos, V.R.; Fleming, G.F. Therapeutic targets and opportunities in endometrial cancer: Update on endocrine therapy and nonimmunotherapy targeted options. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 1–11. [Google Scholar] [CrossRef]
- Kach, J.; Conzen, S.D.; Szmulewitz, R.Z. Targeting the glucocorticoid receptor in breast and prostate cancers. Sci. Transl. Med. 2015, 7, 305ps319. [Google Scholar] [CrossRef] [Green Version]
- Prekovic, S.; Schuurman, K.; Manjón, A.G.; Buijs, M.; Peralta, I.M.; Wellenstein, M.D.; Yavuz, S.; Barrera, A.; Monkhorst, K.; Huber, A.; et al. Glucocorticoids regulate cancer cell dormancy. bioRxiv 2019, 750406. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Country | Cancer Site(s) | Recruitment Period | Follow Up | Tumor Sample Size | Histological Subtypes (n) | Sex | Treatment (n) | ||
| Range (Months) | Mean/Median (Months) | ||||||||||
| Abduljabbar et al. [42] | 2015 | UK | Breast | NR | NR | 107 | 999 | DC (846), LC (80), MC (20), special types (44) | All F | NR | |
| Elkashif et al. [43] | 2020 | UK | Breast | NR | NR | NR | 295 | NR | All F | FEC (129), CMF (77), FEC-DTX (18), TAM/RTx (17), A/C (14), none (13), NR (1) | |
| Gokon et al. [44] | 2020 | Japan | Oesophageal | NR | NR | NR | 87 | OAC all | M: 73 F: 14 | NR | |
| Heuck et al. [45] | 2012 | USA | Myeloma | NR | NR | NR | 668 | NR | M: 199 F: 152 | Thalidomide (323), | |
| Ho et al. [46] | 2002 | Taiwan | Liver | 1993–1997 | NR | NR | 92 | NR | M: 69 F: 23 | None | |
| Ip et al. [47] | 2015 | Australia | Adrenal | 1998–2003 | NR | 34 | 61 | All ACC | M: 26 F: 38 | Mitotane (25), RTx (14), CTx (22) | |
| Ishiguro et al. [48] | 2014 | USA | Bladder | NR | NR | NR | 152 | Urothelial (106), SCC (3), NR (43) | M: 114 F: 35 | Intravesicle BCG (17) | |
| Kashiwagi et al. [49] | 2016 | Japan | Bladder | NR | NR | 37 | 99 | NR | M: 60 F: 39 | NR | |
| Kato et al. [50] | 1993 | USA | Acute lymphoblastic leukaemia | 1981–1984 | ≤113 | NR | 546 | ALL | M: 290 F: 256 | Vincristine & prednisone with SoC and 6-mercaptopurine and methotrexate or SoC and methotrexate | |
| Kost et al. [51] | 2019 | Germany | Cervical | 1993–2002 | ≤235 | NR | 250 | SCC (202), AC (48) | All F | NR | |
| Lu et al. [52] | 2006 | Taiwan | Lung | 1995–2000 | NR | NR | 85 | AC (55), SCC (21), large cell (3), other (6) | M: 49 F: 36 | GEM/CDDP (62), PTX/CDDP (18), GEM alone (6) | |
| Mimae et al. [53] | 2011 | Japan | Thymic | 1973–2009 | 0.03–356.1 | 64.6 | 140 | A + AB (57), B1 + B2 (40), B3 (6), TC (37) + | M: 53 F: 87 | NR | |
| Mitani et al. [54] | 2020 | USA | Salivary duct | 1983–2011 | ≤60 | NR | 67 | NR | M: 48 F: 19 | NR | |
| Shi et al. [55] | 2019 | China | Breast | NR | NR | NR | 150 | NR | NR | NR | |
| Shim et al. [56] | 2019 | South Korea | Prostate | 2000–2013 | NR | NR | 95 | NR | All M | Hormonal (33), DTX (27) | |
| Surati et al. [57] | 2011 | USA | Lung | NR | NR | NR | 93 | AC (58), LCC (18), SCC (15), non-specified (14) | M: 63 F: 42 | NR | |
| Tangen et al. [58] | 2017 | Norway | Endometrial | 2001–2005 | NR | NR | 724 | ED (582), A-SCC (6), CC (28), SP (67), CS (28), UD/other (13) | All F | CTx (126), RTx (61), CT/RTx (5), hormonal (5), none (527) | |
| Ueki et al. [59] | 2020 | Japan | Oesophageal | 2008–2015 | NR | NR | 98 | SCC all | M: 83 F: 15 | CDDP (98), DEX (98) | |
| Vahrenkamp et al. [60] | 2018 | USA | Endometrial | NR | NR | NR | 177 | NR | All F | NR | |
| Veneris et al. [61] | 2017 | USA | Ovarian | 1995–2010 | 26.3–71.2 (IQR) | 43.4 | 341 | SE (240), ED (32), CC (42), mucinous (17), other (10) | All F | Adjuvant CTx (341) | |
| Veneris et al. [62] | 2019 | USA | Ovarian | NR | NR | NR | 222 | Serous (222) | All F | NR | |
| West et al. [63] | 2018 | USA | Breast (ER-) | NR | NR | NR | 623 | Basal-like 1 (171), Basal-like 2 (75), mesenchymal (175), luminal AR (202) | All F | Tam., Tam + AI, AI & | |
| West et al. [64] | 2016 | USA | Breast (ER+) | NR | NR | NR | 502 | Oestrogen receptor positive | All F | Adjuvant CTx and/or Tam (number of patients NR) | |
| Yakirevich et al. [65] | 2011 | USA | Renal | 1998–2006 | 1–88 | 36 | 200 | CRCC (147), PRCC (23), CHRCC (16), OC (14) | M: 139 F: 61 | None | |
| Yeh et al. [66] | 2006 | Taiwan | Gastric | 1997–1999 | ≤72 | NR | 75 | NR | M: 58 F: 17 | NR | |
| Study | Mean/Median Age (Years) | Tumor Grade (n) | Tumor Stage | Technique for GR Assessment | Antibody (Clone, Animal, Manufacturer, Dilution) | Definition of GR+ | GR+/High, No. (%) | ||||
| Magnitude | Location of Staining | ||||||||||
| Abduljabbar et al. [42] | 54 | 1 (153), 2 (324), 3 (513) | I (603), II (306), III (81) | IHC | SC-1003, rabbit, Santa Cruz Biotechnology, 1:80 | ≥10% | Nuclear and cytoplasmic | 617 (61.8) | |||
| Elkashif et al. [43] | 45, 49, 50, 54 | 1 (0), 2 (25), 3 (221) | NR | IHC | D8H2, NR, Cell Signaling Technology, 1:50 | NR | Nuclear | 220 (74.6) | |||
| Gokon et al. [44] | 68.9, 65.2 | Well/moderate (73), poor (14) | I (51), II (8), III (22), IV (6) | IHC | D6H2L, NR, Cell Signaling Technology, 1:400 | >4.0 | NR | 50 (57.5) | |||
| Heuck et al. [45] | NR | NR | NR | Microarray | N/A | 895 | N/A | NR | |||
| Ho et al. [46] | 57 | 1/2 (41), 3/4 (51) | II (26), III (35), IV (31) | DCC | N/A | NR | N/A | 63 (68.5) | |||
| Ip et al. [47] | 50 | NR | I (2), II (23), III (16), IV (20) ^ | IHC | 4H2, NR, Novocastra, 1:20 | >1 | Nuclear and cytoplasmic | NR | |||
| Ishiguro et al. [48] | NR | Low grade (53), high grade (96) | NR | IHC | H300, NR, Santa Cruz Biotechnology, 1:200 | ≥1% | Nuclear | 129 (86.6) | |||
| Kashiwagi et al. [49] | 71 | Low (15), high (84) | pTa-pT1 (37), pT2-pT4 (62) | IHC | H-300, NR, Santa Cruz Biotechnology, 1:200 | >1% | Nuclear | 62 (62.6) | |||
| Kato et al. [50] | NR | NR | NR | RLB | N/A | NR | N/A | 314 (57.5) | |||
| Kost et al. [51] | 47 | 1 (21), 2 (143), 3 (78), unclassified (8) | I (64), II (49), III (37), IV (7), NS (93) # | IHC | 4H2, mouse, Novocastra, 1:30 | ≥1% | Nuclear | 161 (64.4) | |||
| Lu et al. [52] | NR | NR | IIIb (14), IV (71) | IHC | PA1-511A, NR, Affinity Bioreagents, 1:500 | >10% | NR | 43 (51) | |||
| Mimae et al. [53] | 57.4 | NR | I + II (98), III + IV (42) ## | IHC | H8004, NR, Perseus Proteomics, 1:200 | Allred score ≥3 | NR | 116 (82.9) | |||
| Mitani et al. [54] | 62 | NR | I/II (4), III/IV (40) | IHC | NR, mouse, BD Biosciences, 1:100 | NR | Nuclear | 12 (23.6) | |||
| Shi et al. [55] | NR | NR | I (10), II (83), III (46) & | IHC | D8H2, rabbit, Cell Signaling Technology, NR | ≥7% | Nuclear | 68 (45.3) | |||
| Shim et al. [56] | 73 | 7 (11), 8 (12), 9 (46), 10 (26) $ | NR | qPCR | N/A | NR | N/A | (16.2) | |||
| Surati et al. [57] | 61 | NR | I (49), II (12), III (32), IV (6), NS (6) | IHC | NR, NR, Novocastra, NR | NR | Nuclear and cytoplasmic | NR | |||
| Tangen et al. [58] | NR | 1/2 (489), 3 (92) | I/II (615), III/IV (109) # | IHC | D8H2, rabbit, Cell Signaling Technology, 1:500 | ≥10% | NR | 186 (25.7) | |||
| Ueki et al. [59] | NR | Well/moderate (84), poor (10), unclassified (4) | pT1a-pT1b (28), pT2-pT4b (70) | IHC | D6H2L, NR, Cell Signaling Technology, 1:400 | ≥10% | Nuclear | 52 (53.1) | |||
| Vahrenkamp et al. [60] | NR | NR | NR | RNA seq | N/A | 30th percentile | N/A | NR | |||
| Veneris et al. (2017) [61] | 58 | 1 (30), 2 (62), 3 (249) | I/II (96), III/IV (245) # | IHC | D8H2 XP, rabbit, Cell Signaling, 1:500 | ≥1% | Nuclear | 133 (39) | |||
| Veneris et al. (2019) [62] | 59 | 2 (23), 3 (192), unclassified (7) | I (3), II (12), III (168), IV (38), unclassified (1) # | Microarray | N/A | NR | N/A | 111 (50) | |||
| West et al. (2018) [63] | 51 & | NR | NR | Microarray | N/A | NR | N/A | 163 (26.2) | |||
| West et al. (2016) [64] | NR | NR | NR | Microarray | N/A | 25th percentile | N/A | 311 (61.9) | |||
| Yakirevich et al. [65] | 68 | 1 (13), 2 (82), 3 (71), 4 (20) | I (109), II (30), III (33), IV (14) | IHC | PA1-511A, rabbit, Affinity Bioreagents, 1:500 | NR | Nuclear | 106 (53) | |||
| Yeh et al. [66] | 62, 64 | Well (1), moderate (26), poorly (48) | pT3 (39), pT4 (36) | DCC | N/A | NR | Cytosol | 31 (41.3) | |||
| Study. | Cancer Site(s) | Total Number of Patients/ Deaths or Progressions | OS/CSS | PFS/RFS/DFS | Adjustments | ||||
|---|---|---|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | ||||
| Abduljabbar et al. [42] | Breast | NR | HR 1.09 | 0.86–1.37 | 0.48 | NR | NR | NR | Multivariate variables NR |
| Elkashif et al. [43] | Breast ER-ve untreated | NR | HR 2.615 | 1.189–5.751 | 0.0196 | HR 2.55 | 1.267–5.142 | 0.0087 | Unadjusted |
| Elkashif et al. | Breast (TMA #1 FEC) | NR | HR 0.2296 | 0.6689–0.7882 | 0.0194 | HR 0.8724 | 0.2917–2.609 | 0.8122 | Unadjusted |
| Elkashif et al. | Breast (TMA #2 FEC) | NR | HR 0.3201 | 0.07484–1.370 | 0.1246 | HR 0.3189 | 0.09401–1.082 | 0.2365 | Unadjusted |
| Elkashif et al. | Breast (TMA #3 CMF) | NR | HR 0.9010 | 0.3534–2.298 | 0.8324 | HR 0.7407 | 0.3115–1.761 | 0.5343 | Unadjusted |
| Elkashif et al. | Breast (TMA #3 taxane) | NR | HR 1.424 | 0.1079–18.79 | 0.7717 | HR 4.939 | 0.6210–39.28 | 0.2365 | Unadjusted |
| Elkashif et al. | Breast (TMA #4 AC) | NR | HR 0.7301 | 0.3271–1.630 | 0.4610 | HR 0.7726 | 0.3443–1.734 | 0.5458 | Unadjusted |
| Gokon et al. [44] | Oesophageal | NR | HR 0.69 | 0.30–1.62 | 0.4 | NR | NR | NR | Unadjusted |
| Heuck et al. * [45] | Myeloma (non-thalidomide) | NR | HR 0.53 | 0.35–078 | NR | HR 0.68 | 0.49–0.94 | NR | Unadjusted |
| Heuck et al. * | Myeloma (thalidomide treated) | NR | HR 0.99 | 0.64–1.54 | NR | HR 0.68 | 0.61–1.28 | NR | Unadjusted |
| Ho et al. * [46] | Liver | 92/62 | HR 5.88 (A), 2.06 (UA) | 2.06–16.81 (A), 0.9–4.69 (UA) | NR | HR 2.56 (A), 1.45 (UA) | 1.32–5 (A), 0.87–2.42 (UA) | 0.002 (UA) | Multivariate variables NR |
| Ip et al. [47] | Adrenal | NR | HR 1.1 | 0.45–2.7 | 0.84 | HR 0.66 | 0.22–2.0 | 0.462 | Unadjusted |
| Ishiguro et al. * [48] | Bladder (invasive) | NR | NR | NR | NR | HR 0.597 | 0.263–1.356 | 0.082 | Multivariate variables NR |
| Ishiguro et al. * | Bladder (non-invasive) | NR | NR | NR | NR | HR 0.704 | 0.184–2.703 | 0.165 | Multivariate variables NR |
| Kashiwagi et al. * [49] | Bladder | NR | HR 0.78 | 0.36–1.69 | NR | HR 0.83 | 0.419–1.643 | 0.664 | Unadjusted |
| Kato et al. * [50] | Leukaemia | 546/254 | NR | NR | NR | HR 0.65 | 0.51–0.84 | NR | Unadjusted |
| Kost et al. [51] | Cervical | 250/49 | HR 0.575 | 0.328–1.009 | 0.054 | NR | NR | NR | Multivariate variables NR |
| Lu et al. * [52] | Lung | 85/55 | HR 0.74 | 0.49–1.14 | 0.014 | HR 0.83 | 0.54–1.26 | 0.039 | Multivariate variables NR |
| Mimae et al. [53] | Thymic | 140/28 | HR 0.24 (A) HR 0.35 (UA) | 0.10–0.61 (A) 0.15–0.83 (UA) | 0.0025 (A) 0.013 (UA) | NR | NR | NR | Multivariate variables NR |
| Mitani et al. * [54] | Salivary duct | NR | HR 1.27 | 0.73–2.2 | 0.026 | HR 0.84 | 0.47–1.48 | NR | Unadjusted |
| Shi et al. [55] | Breast | NR | HR 2.875 | 1.491 | 4.866 | NR | NR | NR | Unadjusted |
| Shim et al. [56] | Prostate | NR | HR 1.79 (UA), 0.953 (A) | 1.009–3.165 (UA), 0.398–1.890 (A) | NR | NR | NR | NR | Multivariate variables NR |
| Surati et al. [57] | Lung | NR | HR 0.76 | 0.59–0.97 | 0.03 | NR | NR | NR | Disease stage and age |
| Tangen et al. [58] | Endometrial (all) | NR | HR 1.6 (A), 3.0 (UA) | 1.03–2.47 (A), 2.0–4.5 (UA) | 0.036 (A), <0.001 (UA) | NR | NR | NR | Age, FIGO stage, histological grade |
| Ueki et al. [59] | Oesophageal | NR | HR 1.6737 (A), 1.8991 (UA) | 0.8299–3.5502 (A) 1.006–3.7409(UA) | 0.1524 (A), 0.0479 (UA) | NR | NR | NR | Multivariate variables NR |
| Vahrenkamp et al. * [60] | Endometrial | NR | HR 2.1 | 1.16–3.7 | NR | HR 2.1 | 1.18–3.75 | 0.012 | Unadjusted |
| Veneris et al. (2017) [61] | Ovarian (cohort 1) | NR | HR 0.96 (A), 1.18 (UA) | 0.71–1.30 (A), 0.89–1.56 (UA) | 0.8 | HR 1.41 (A), 1.66 (UA) | 1.08–1.84 (A), 1.29–2.14 (UA) | 0.012 | Age, histological subtype, grade, stage, presence of gross residual disease after debulking |
| Veneris et al. (2017) | Ovarian (cohort 2) | NR | NR | NR | HR 8.35 | 0.93–74.88 | 0.023 | unadjusted | |
| Veneris et al. (2019) [62] | Ovarian | NR | HR 1.55 (A), 1.4 (UA) | 1.06 to 2.26 (A), 0.98–1.9 (UA) | 0.0251 (A), 0.068 (UA) | NR | NR | NR | Age, race, histological grade |
| West et al. (2018) * [63] | Breast (basal-like 1) | 171/67 | NR | NR | NR | HR 1.87 | 1.08–3.25 | 0.013 | Unadjusted |
| West et al. (2018) * | Breast (basal-like 2) | 75/30 | NR | NR | NR | HR 1.08 | 0.47–2.45 | NR | Unadjusted |
| West et al. (2018) * | Breast (mesenchymal) | 175/82 | NR | NR | NR | HR 1.65 | 1–2.27 | 0.04 | Unadjusted |
| West et al. (2018) * | Breast (luminal AR) | 202/94 | NR | NR | NR | HR 1.68 | 1.07–2.63 | 0.015 | Unadjusted |
| West et al. (2016) [64] | Breast | NR | NR | NR | NR | HR 0.35 | 0.26–0.47 | 7.8 × 10−14 | Unadjusted |
| Yakirevich et al. * [65] | Renal | NR | HR 0.66 | 0.32–1.33 | 0.1 | NR | NR | NR | Unadjusted |
| Yeh et al. * [66] | Gastric | 75/59 | HR 1.3 | 0.71–2.38 | 0.0465 | NR | NR | NR | Unadjusted |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakour, N.; Moriarty, F.; Moore, G.; Robson, T.; Annett, S.L. Prognostic Significance of Glucocorticoid Receptor Expression in Cancer: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 1649. https://doi.org/10.3390/cancers13071649
Bakour N, Moriarty F, Moore G, Robson T, Annett SL. Prognostic Significance of Glucocorticoid Receptor Expression in Cancer: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(7):1649. https://doi.org/10.3390/cancers13071649
Chicago/Turabian StyleBakour, Noor, Frank Moriarty, Gillian Moore, Tracy Robson, and Stephanie L. Annett. 2021. "Prognostic Significance of Glucocorticoid Receptor Expression in Cancer: A Systematic Review and Meta-Analysis" Cancers 13, no. 7: 1649. https://doi.org/10.3390/cancers13071649