
Time to Pregnancy, Obstetrical and Neonatal Outcomes after Breast Cancer: A Study from the Maternity Network for Young Breast Cancer Patients

 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Tumors
2.2. Treatments
2.3. Identification of Pregnancy Cases
2.4. Pregnancy Planning, Time to Evolutive Pregnancy, Obstetrical and Neonatal Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Tumor Characteristics and Treatment
3.2. Pregnancies after BC
3.3. Time to Pregnancy
3.3.1. Time from Diagnosis to Pregnancy
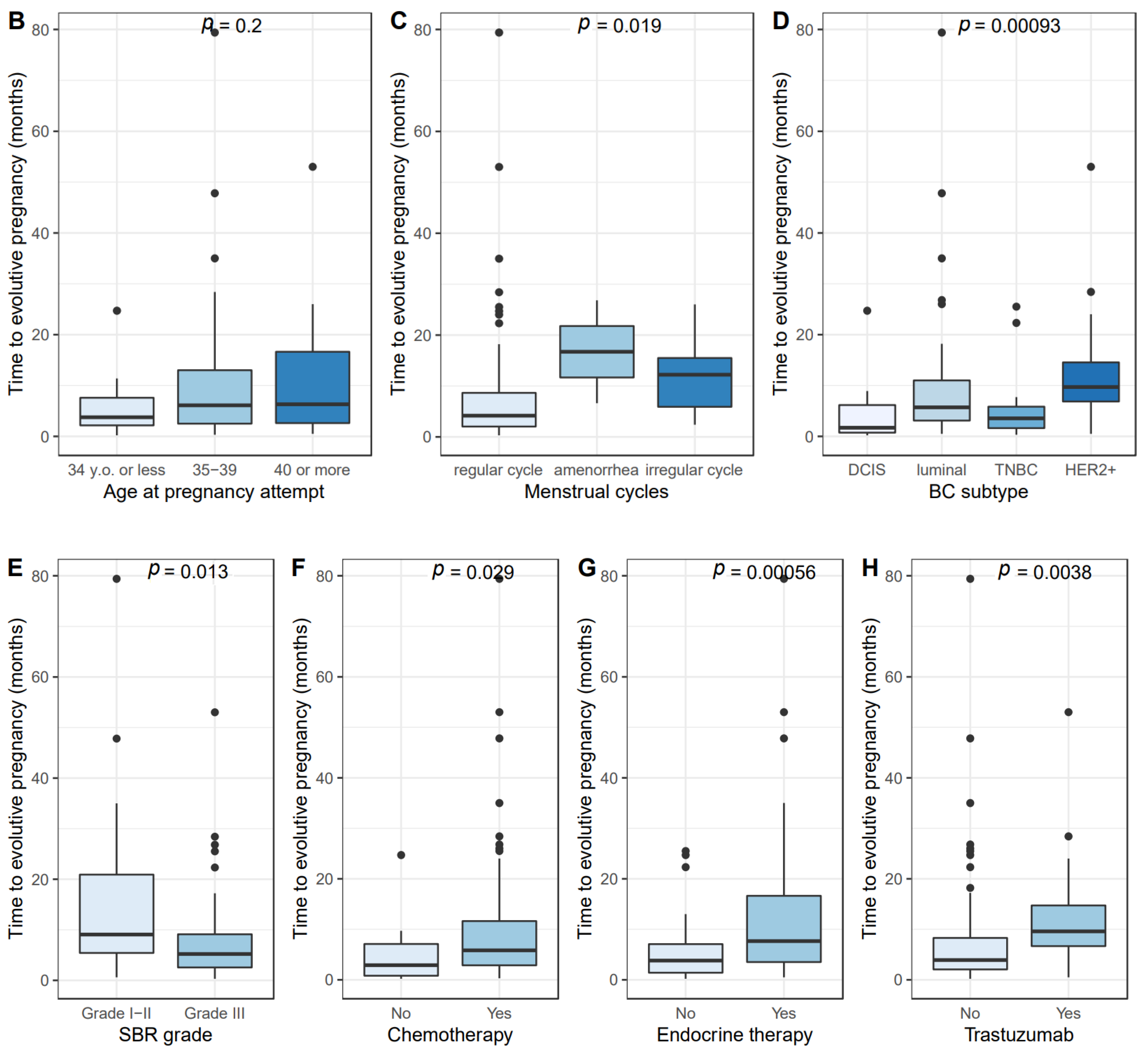
3.3.2. Time from First Attempt to the Occurrence of Pregnancy
3.4. Obstetrical and Neonatal Outcomes
4. Discussion
- 18% of pregnancies were unplanned, representing nearly one pregnancy out of five, and this rate notably includes eight pregnancies occurring during treatment. Of note, 39% of these unplanned pregnancies ended up with an abortion, whether elective or for medical reasons. Our results are consistent with previous literature, with abortion rates varying from 3% to 42% [1,19,20,23,24,25]. Contraception in breast cancer patient is a topic that has garnered little attention so far. However, it is particularly important because planning pregnancy in these patients is crucial from a medical point of view. For patients who do not wish to become pregnant, pregnancy should be actively avoided, particularly during chemotherapy and tamoxifen treatment, as these medications are known for their teratogenic effects. Our results highlight the fact that the contraception topic is insufficiently addressed in young breast cancer patients.
- Most pregnancies occurred spontaneously, and the median time to a pregnancy resulting in a live birth was short. Our results are in line with the time to pregnancy reported in general population. A prospective cohort of 960 patients aged 30 to 44 years old found that median time to pregnancy was 3 months for women under 38 years old, 4 months for women aged 38-39 years old, 8 months for women aged 40–41 years old, and longer than 12 months for women aged 42 or older [37]. In a preconception cohort study, 46.3% women (n = 141) aged from 37 to 39 years old became pregnant within six cycles (95%CI [37.3–55.3]) [38]. In global population, time to pregnancy is known to increase with age and be longer in nulliparous women [37,38,39]. In a recent multicenter prospective cohort study, up to 69% of BC patients wishing to conceive became pregnant within 5 years after diagnosis. Younger age at diagnosis was significantly associated to the occurrence of a pregnancy [40]. However, to our knowledge, data on time from pregnancy attempt to pregnancy occurrence have not been published so far in a selected population of BC patients, and the results we present here are unprecedented. Previous studies mainly focused on the time interval between BC diagnosis and live birth, and provide delays varying from 23 to 45 months according to the different studies led so far [19,20,22,24,25,41,42,43,44,45,46]. In Gerstl et al.’s meta-analysis of 2 523 BC patients who became pregnant after BC treatment, the mean interval to the first pregnancy was 29 months (range: 11–63 months) and 40 months (range: 10–228 months) to a first live birth [46]. Consistently, the mean interval from surgery to first pregnancy was of 45.4 months in our cohort. We found that the time interval was significantly different according to HR status, which is consistent with the fact BC patients are generally advised to take endocrine therapy for at least 2 years before becoming pregnant [47].
- Obstetrical and neonatal after breast cancer were reassuring. Our analyses report an overall miscarriage rate of 22%, and the miscarriage rate was significantly associated with increasing age. Gerst et al.’s meta-analysis [46] reported an overall early pregnancy loss rate of 12%, varying from 2% to 24% according to studies [1,19,20,23,24,25,42,44,45,48]. Age of patients is known to be a risk factor of miscarriage, with an increasing risk with age [49]. Our 22% miscarriage rate is to interpret in light with the fact that 29% of the patients were 40 y.o. and older at pregnancy beginning in our cohort.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Partridge, A.H.; Gelber, S.; Peppercorn, J.; Ginsburg, E.; Sampson, E.; Rosenberg, R.; Przypyszny, M.; Winer, E.P. Fertility and Menopausal Outcomes in Young Breast Cancer Survivors. Clin. Breast Cancer 2008, 8, 65–69. [Google Scholar] [CrossRef]
- Anders, C.K.; Johnson, R.; Litton, J.; Phillips, M.; Bleyer, A. Breast Cancer Before Age 40 Years. Semin. Oncol. 2009, 36, 237–249. [Google Scholar] [CrossRef] [Green Version]
- Insttitut National du Cancer. Les Cancers en France. Available online: https://www.e-cancer.fr/ressources/cancers_en_france/#page=64 (accessed on 17 January 2021).
- Cancer Research UK. Breast Cancer Survival Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer/survival (accessed on 23 January 2021).
- Mathews, T.J.; Hamilton, B.E. Mean Age of Mothers Is on the Rise: United States, 2000–2014; NCHS Data Brief; US Department of Health and Human Services: Washington, DC, USA, 2016; pp. 1–8.
- Mills, M.; Rindfuss, R.R.; McDonald, P.; Te Velde, E. Why Do People Postpone Parenthood? Reasons and Social Policy Incentives. Hum. Reprod. Update 2011, 17, 848–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, T.J.; Hamilton, B.E. Delayed Childbearing: More Women Are Having Their First Child. Later in Life; NCHS Data Brief; US Department of Health and Human Services: Washington, DC, USA, 2009; pp. 1–8.
- Lambertini, M.; Peccatori, F.A.; Demeestere, I.; Amant, F.; Wyns, C.; Stukenborg, J.-B.; Paluch-Shimon, S.; Halaska, M.J.; Uzan, C.; Meissner, J.; et al. Fertility Preservation and Post-Treatment Pregnancies in Post-Pubertal Cancer Patients: ESMO Clinical Practice Guidelines†. Ann. Oncol. 2020, 31, 1664–1678. [Google Scholar] [CrossRef]
- Anders, C.K.; Hsu, D.S.; Broadwater, G.; Acharya, C.R.; Foekens, J.A.; Zhang, Y.; Wang, Y.; Marcom, P.K.; Marks, J.R.; Febbo, P.G.; et al. Young Age at Diagnosis Correlates with Worse Prognosis and Defines a Subset of Breast Cancers with Shared Patterns of Gene Expression. J. Clin. Oncol. 2008, 26, 3324–3330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Partridge, A.H.; Hughes, M.E.; Warner, E.T.; Ottesen, R.A.; Wong, Y.-N.; Edge, S.B.; Theriault, R.L.; Blayney, D.W.; Niland, J.C.; Winer, E.P.; et al. Subtype-Dependent Relationship Between Young Age at Diagnosis and Breast Cancer Survival. J. Clin. Oncol. 2016, 34, 3308–3314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azim, H.A.; Partridge, A.H. Biology of Breast Cancer in Young Women. Breast Cancer Res. 2014, 16, 427. [Google Scholar] [CrossRef]
- Kudela, E.; Samec, M.; Kubatka, P.; Nachajova, M.; Laucekova, Z.; Liskova, A.; Dokus, K.; Biringer, K.; Simova, D.; Gabonova, E.; et al. Breast Cancer in Young Women: Status Quo and Advanced Disease Management by a Predictive, Preventive, and Personalized Approach. Cancers 2019, 11, 1791. [Google Scholar] [CrossRef] [Green Version]
- Amaadour, L.; El Mrabet, F.Z.; Atreche, L.; El Rhazi, K.; Oualla, K.; Benbrahim, Z.; Arifi, S.; Mellas, N. Chemotherapy induced ovarian failure in breast cancer: Retrospective study of 100 cases. Bull. Cancer 2020, 107, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Poggio, F.; Levaggi, A.; Lambertini, M. Chemotherapy-Induced Premature Ovarian Failure and Its Prevention in Premenopausal Breast Cancer Patients. Expert Rev. Qual. Life Cancer Care 2016, 1, 5–7. [Google Scholar] [CrossRef] [Green Version]
- Mauri, D.; Gazouli, I.; Zarkavelis, G.; Papadaki, A.; Mavroeidis, L.; Gkoura, S.; Ntellas, P.; Amylidi, A.-L.; Tsali, L.; Kampletsas, E. Chemotherapy Associated Ovarian Failure. Front. Endocrinol. 2020, 11. [Google Scholar] [CrossRef]
- Paluch-Shimon, S.; Cardoso, F.; Partridge, A.H.; Abulkhair, O.; Azim, H.A.; Bianchi-Micheli, G.; Cardoso, M.-J.; Curigliano, G.; Gelmon, K.A.; Harbeck, N.; et al. ESO–ESMO 4th International Consensus Guidelines for Breast Cancer in Young Women (BCY4). Ann. Oncol. 2020, 31, 674–696. [Google Scholar] [CrossRef]
- Oktay, K.; Harvey, B.E.; Partridge, A.H.; Quinn, G.P.; Reinecke, J.; Taylor, H.S.; Wallace, W.H.; Wang, E.T.; Loren, A.W. Fertility Preservation in Patients with Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1994–2001. [Google Scholar] [CrossRef] [PubMed]
- American Society of Clinical Oncology. Pregnancy After Breast Cancer Does Not Increase Chance of Recurrence. Available online: https://www.asco.org/about-asco/press-center/news-releases/pregnancy-after-breast-cancer-does-not-increase-chance (accessed on 23 January 2021).
- Lambertini, M.; Kroman, N.; Ameye, L.; Cordoba, O.; Pinto, A.; Benedetti, G.; Jensen, M.-B.; Gelber, S.; Del Grande, M.; Ignatiadis, M.; et al. Long-Term Safety of Pregnancy Following Breast Cancer According to Estrogen Receptor Status. J. Natl. Cancer Inst. 2018, 110, 426–429. [Google Scholar] [CrossRef] [Green Version]
- Kroman, N.; Jensen, M.-B.; Wohlfahrt, J.; Ejlertsen, B.; Danish Breast Cancer Cooperative Group. Pregnancy after Treatment of Breast Cancer—A Population-Based Study on Behalf of Danish Breast Cancer Cooperative Group. Acta Oncol. 2008, 47, 545–549. [Google Scholar] [CrossRef]
- Córdoba, O.; Bellet, M.; Vidal, X.; Cortés, J.; Llurba, E.; Rubio, I.T.; Xercavins, J. Pregnancy after Treatment of Breast Cancer in Young Women Does Not Adversely Affect the Prognosis. Breast 2012, 21, 272–275. [Google Scholar] [CrossRef] [PubMed]
- Azim, H.A.; Kroman, N.; Paesmans, M.; Gelber, S.; Rotmensz, N.; Ameye, L.; De Mattos-Arruda, L.; Pistilli, B.; Pinto, A.; Jensen, M.-B.; et al. Prognostic Impact of Pregnancy After Breast Cancer According to Estrogen Receptor Status: A Multicenter Retrospective Study. J. Clin. Oncol. 2013, 31, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Blakely, L.J.; Buzdar, A.U.; Lozada, J.A.; Shullaih, S.A.; Hoy, E.; Smith, T.L.; Hortobagyi, G.N. Effects of Pregnancy after Treatment for Breast Carcinoma on Survival and Risk of Recurrence. Cancer 2004, 100, 465–469. [Google Scholar] [CrossRef]
- Ives, A.; Saunders, C.; Bulsara, M.; Semmens, J. Pregnancy after Breast Cancer: Population Based Study. BMJ 2007, 334, 194. [Google Scholar] [CrossRef] [Green Version]
- Gelber, S.; Coates, A.S.; Goldhirsch, A.; Castiglione-Gertsch, M.; Marini, G.; Lindtner, J.; Edelmann, D.Z.; Gudgeon, A.; Harvey, V.; Gelber, R.D. Effect of Pregnancy on Overall Survival after the Diagnosis of Early-Stage Breast Cancer. J. Clin. Oncol. 2001, 19, 1671–1675. [Google Scholar] [CrossRef]
- Hartman, E.K.; Eslick, G.D. The Prognosis of Women Diagnosed with Breast Cancer before, during and after Pregnancy: A Meta-Analysis. Breast Cancer Res. Treat. 2016, 160, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Sankila, R.; Heinävaara, S.; Hakulinen, T. Survival of Breast Cancer Patients after Subsequent Term Pregnancy: “Healthy Mother Effect”. Am. J. Obstet. Gynecol. 1994, 170, 818–823. [Google Scholar] [CrossRef]
- El Hachem, H.; Atallah, D.; Grynberg, M. Fertility Preservation in Breast Cancer Patients. Future Oncol. 2014, 10, 1767–1777. [Google Scholar] [CrossRef]
- Velentgas, P.; Daling, J.R.; Malone, K.E.; Weiss, N.S.; Williams, M.A.; Self, S.G.; Mueller, B.A. Pregnancy after Breast Carcinoma. Cancer 1999, 85, 2424–2432. [Google Scholar] [CrossRef]
- Mueller, B.A.; Simon, M.S.; Deapen, D.; Kamineni, A.; Malone, K.E.; Daling, J.R. Childbearing and Survival after Breast Carcinoma in Young Women. Cancer 2003, 98, 1131–1140. [Google Scholar] [CrossRef]
- Hamy, A.-S.; Porcher, R.; Eskenazi, S.; Cuvier, C.; Giacchetti, S.; Coussy, F.; Hocini, H.; Tournant, B.; Perret, F.; Bonfils, S.; et al. Anti-Müllerian Hormone in Breast Cancer Patients Treated with Chemotherapy: A Retrospective Evaluation of Subsequent Pregnancies. Reprod. BioMed. Online 2016, 32, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Elston, C.W.; Ellis, I.O. Pathological Prognostic Factors in Breast Cancer. I. The Value of Histological Grade in Breast Cancer: Experience from a Large Study with Long-Term Follow-Up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Harvey, J.M.; Clark, G.M.; Osborne, C.K.; Allred, D.C. Estrogen Receptor Status by Immunohistochemistry Is Superior to the Ligand-Binding Assay for Predicting Response to Adjuvant Endocrine Therapy in Breast Cancer. J. Clin. Oncol. 1999, 17, 1474–1481. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef] [PubMed]
- Labrosse, J.; Lam, T.; Sebbag, C.; Benque, M.; Abdennebi, I.; Merckelbagh, H.; Osdoit, M.; Priour, M.; Guerin, J.; Balezeau, T.; et al. Text Mining in Electronic Medical Records Enables Quick and Efficient Identification of Pregnancy Cases Occurring After Breast Cancer. JCO Clin. Cancer Inform. 2019, 3, 1–12. [Google Scholar] [CrossRef]
- Royal College of Obstetricians and Gynaecologists. Small-for-Gestational-Age Fetus, Investigation and Management (Green-Top Guideline No. 31). Available online: https://www.rcog.org.uk/en/guidelines-research-services/guidelines/gtg31/ (accessed on 21 February 2021).
- Steiner, A.Z.; Jukic, A.M.Z. Impact of Female Age and Nulligravidity on Fecundity in an Older Reproductive Age Cohort. Fertil. Steril. 2016, 105, 1584–1588.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wesselink, A.K.; Rothman, K.J.; Hatch, E.E.; Mikkelsen, E.M.; Sørensen, H.T.; Wise, L.A. Age and Fecundability in a North American Preconception Cohort Study. Am. J. Obstet. Gynecol. 2017, 217, 667.e1–667.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothman, K.J.; Wise, L.A.; Sørensen, H.T.; Riis, A.H.; Mikkelsen, E.M.; Hatch, E.E. Volitional Determinants and Age-Related Decline in Fecundability: A General Population Prospective Cohort Study in Denmark. Fertil. Steril. 2013, 99, 1958–1964. [Google Scholar] [CrossRef] [Green Version]
- Poorvu, P.D.; Gelber, S.I.; Zheng, Y.; Ruddy, K.J.; Tamimi, R.M.; Peppercorn, J.; Schapira, L.; Borges, V.F.; Come, S.E.; Lambertini, M.; et al. Pregnancy after Breast Cancer: Results from a Prospective Cohort of Young Women with Breast Cancer. Cancer 2020. [Google Scholar] [CrossRef]
- Langagergaard, V.; Gislum, M.; Skriver, M.V.; Nørgård, B.; Lash, T.L.; Rothman, K.J.; Sørensen, H.T. Birth Outcome in Women with Breast Cancer. Br. J. Cancer 2006, 94, 142–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldrat, O.; Kroman, N.; Peccatori, F.A.; Cordoba, O.; Pistilli, B.; Lidegaard, O.; Demeestere, I.; Azim, H.A. Pregnancy Following Breast Cancer Using Assisted Reproduction and Its Effect on Long-Term Outcome. Eur. J. Cancer 2015, 51, 1490–1496. [Google Scholar] [CrossRef]
- Anderson, C.; Engel, S.M.; Anders, C.K.; Nichols, H.B. Live Birth Outcomes after Adolescent and Young Adult Breast Cancer: Live Births after Breast Cancer. Int. J. Cancer 2018, 142, 1994–2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, L.; Kalder, M.; Arabin, B.; Kostev, K. Impact of Prior Breast Cancer on Mode of Delivery and Pregnancy-Associated Disorders: A Retrospective Analysis of Subsequent Pregnancy Outcomes. J. Cancer Res. Clin. Oncol. 2017, 143, 1069–1074. [Google Scholar] [CrossRef]
- Dieci, M.V.; Ghiotto, C.; Barbieri, C.; Griguolo, G.; Saccardi, C.; Gangemi, M.; Pluchinotta, A.; Di Liso, E.; Giorgi, C.A.; Giarratano, T.; et al. Patterns of Fertility Preservation and Pregnancy Outcome After Breast Cancer at a Large Comprehensive Cancer Center. J. Women Health 2019, 28, 544–550. [Google Scholar] [CrossRef] [Green Version]
- Gerstl, B.; Sullivan, E.; Ives, A.; Saunders, C.; Wand, H.; Anazodo, A. Pregnancy Outcomes After a Breast Cancer Diagnosis: A Systematic Review and Meta-Analysis. Clin. Breast Cancer 2018, 18, e79–e88. [Google Scholar] [CrossRef]
- Ekholm, M.; Bendahl, P.-O.; Fernö, M.; Nordenskjöld, B.; Stål, O.; Rydén, L. Two Years of Adjuvant Tamoxifen Provides a Survival Benefit Compared With No Systemic Treatment in Premenopausal Patients With Primary Breast Cancer: Long-Term Follow-Up (>25 Years) of the Phase III SBII:2pre Trial. J. Clin. Oncol 2016, 34, 2232–2238. [Google Scholar] [CrossRef]
- Rippy, E.E.; Karat, I.F.; Kissin, M.W. Pregnancy after Breast Cancer: The Importance of Active Counselling and Planning. Breast 2009, 18, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Nybo Andersen, A.M.; Wohlfahrt, J.; Christens, P.; Olsen, J.; Melbye, M. Maternal Age and Fetal Loss: Population Based Register Linkage Study. BMJ 2000, 320, 1708–1712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, H.; Gagnon, R.; Sermer, M. Diabetes in Pregnancy. J. Obstet. Gynaecol. Can. 2016, 38, 667–679.e1. [Google Scholar] [CrossRef] [PubMed]
- Steegers, E.A.P.; von Dadelszen, P.; Duvekot, J.J.; Pijnenborg, R. Pre-Eclampsia. Lancet 2010, 376, 631–644. [Google Scholar] [CrossRef]
- Hartnett, K.P.; Ward, K.C.; Kramer, M.R.; Lash, T.L.; Mertens, A.C.; Spencer, J.B.; Fothergill, A.; Howards, P.P. The Risk of Preterm Birth and Growth Restriction in Pregnancy after Cancer: The Risk of Preterm Birth and Growth Restriction. Int. J. Cancer 2017, 141, 2187–2196. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Engel, S.M.; Mersereau, J.E.; Black, K.Z.; Wood, W.A.; Anders, C.K.; Nichols, H.B. Birth Outcomes among Adolescent and Young Adult Cancer Survivors. JAMA Oncol. 2017, 3, 1078. [Google Scholar] [CrossRef] [PubMed]
- Dalberg, K.; Eriksson, J.; Holmberg, L. Birth Outcome in Women with Previously Treated Breast Cancer—A Population-Based Cohort Study from Sweden. PLoS Med. 2006, 3, e336. [Google Scholar] [CrossRef] [PubMed]
- ENP 2016_rapport_complet.Pdf. Available online: https://www.epopé.inserm.fr (accessed on 17 January 2021).
- Meta-Analysis of Pregnancy Outcomes in Breast Cancer Survivors. The ASCO Post. Available online: https://ascopost.com/news/december-2020/meta-analysis-of-pregnancy-outcomes-in-breast-cancer-survivors/ (accessed on 25 January 2021).
- Lambertini, M.; Ameye, L.; Hamy, A.-S.; Zingarello, A.; Poorvu, P.D.; Carrasco, E.; Grinshpun, A.; Han, S.; Rousset-Jablonski, C.; Ferrari, A.; et al. Pregnancy after Breast Cancer in Patients with Germline BRCA Mutations. J. Clin. Oncol. 2020, 38, 3012–3023. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Characteristics | n1 | % |
|---|---|---|---|
| Age at BC diagnosis (years) | 32.8 [+/−4.0] | ||
| Body Mass Index | 22.1 [+/3.4] | ||
| Subtype | Luminal | 45 | 40.9 |
| TNBC | 34 | 30.9 | |
| HER2-positive | 31 | 28.2 | |
| Clinical T stage (TNM) * | T0—Tis | 18 | 13.5 |
| T1 | 55 | 41.5 | |
| T2 | 49 | 36.8 | |
| T3 | 9 | 6.8 | |
| T4 | 2 | 1.5 | |
| Clinical N stage (TNM) * | N0 | 76 | 57.1 |
| N+ | 57 | 42.9 | |
| Invasive or DCIS | Invasive | 116 | 87.2 |
| DCIS | 17 | 12.8 | |
| Histological type | Non specific type (NST) | 106 | 98.1 |
| Lobular | 2 | 1.9 | |
| Grade | Grade I | 4 | 3.7 |
| Grade II | 31 | 29.0 | |
| Grade III | 72 | 67.3 | |
| Primary treatment | Surgery | 88 | 66.2 |
| Neoadjuvant treatment | 45 | 33.8 | |
| Type of surgery | Lumpectomy | 60 | 57.1 |
| Mastectomy | 45 | 42.9 | |
| Axillary surgery | Sentinel node biopsy (SNB) | 21 | 20.2 |
| Axillary node dissection | 78 | 75.0 | |
| No axillary surgery | 5 | 4.8 | |
| Lymph nodes involved | N- | 95 | 71.4 |
| N+ | 38 | 28.6 | |
| Chemotherapy | Yes | 102 | 76.7 |
| Anthracycline—taxanes | 77 | 57.9 | |
| Anthracycline | 18 | 13.5 | |
| Taxanes | 7 | 5.3 | |
| No | 31 | 23.3 | |
| Radiotherapy | Yes | 86 | 65 |
| No | 47 | 35 | |
| Trastuzumab | Yes ** | 30 | 22.6 |
| No | 103 | 77.4 | |
| Endocrine therapy | Yes | 53 | 39.8 |
| No | 80 | 60.2 |
| Variable | Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Mean | Median | Coefficient | CI | p | Coefficient | CI | p | |
| Age at BC diagnosis (years) | |||||||||
| <34 | 63 | 8.3 | 5.2 | 0.64 | |||||
| 35–39 | 21 | 11.9 | 5.9 | 0.314 | (−0.307–0.934) | ||||
| ≥40 | 5 | 9.4 | 6.6 | −0.109 | (−1.253–1.036) | ||||
| Age at pregnancy attempt (years) | |||||||||
| <34 | 30 | 5.3 | 3.75 | 0.2 | |||||
| 35–39 | 45 | 11 | 6.1 | 0.397 | (−0.178–0.973) | ||||
| ≥40 | 14 | 12.3 | 6.3 | 0.562 | (−0.228–1.352) | ||||
| Subtype | |||||||||
| Luminal | 35 | 11.3 | 5.7 | 0.004 | |||||
| TNBC | 20 | 5.4 | 3.55 | −0.62 | (−1.219–0.021) | ||||
| HER2 | 19 | 13.4 | 9.7 | 0.392 | (−0.217–1.001) | ||||
| Clinical T stage (TNM) | |||||||||
| T0-T1 | 49 | 9.6 | 5.2 | 0.83 | |||||
| T2 | 35 | 8.8 | 6.1 | 0.126 | (−0.422–0.674) | ||||
| T3-T4 | 5 | 8.9 | 3.8 | 0.008 | (−1.154–1.17) | ||||
| Clinical N stage (TNM) | |||||||||
| N0 | 54 | 10.1 | 5.4 | 0.7 | |||||
| N1-N2-N3 | 35 | 7.9 | 5.8 | 0.054 | (−0.48–0.589) | ||||
| Invasive or DCIS | |||||||||
| Invasive | 77 | 10 | 5.8 | 0.02 | |||||
| DCIS | 12 | 4.6 | 1.7 | 1.049 | (0.316–1.781) | ||||
| Histological type | |||||||||
| Non specific type (NST) | 71 | 6 | 0.624 | 0.02 | |||||
| Lobular | 2 | 41.1 | 0.963 | (−0.615–2.541) | |||||
| Grade | |||||||||
| Grade I–II | 22 | 15.9 | 9.05 | 0.01 | |||||
| Grade III | 51 | 7.9 | 5.2 | −0.716 | (−1.267–0.164) | ||||
| Lymph nodes involved | |||||||||
| N- | 65 | 8.9 | 5.2 | 0.46 | |||||
| N+ | 24 | 10.2 | 6.2 | 0.281 | (−0.305–0.867) | ||||
| Chemotherapy | |||||||||
| Yes | 70 | 10.4 | 5.85 | 0.03 | |||||
| No | 19 | 4.9 | 2.9 | 0.83 | (0.217–1.443) | ||||
| Chemotherapy regimen | |||||||||
| Anthracycline—taxanes | 51 | 10.2 | 5.9 | 0.902 | (0.27–1.535) | 0.1 | |||
| Anthracycline | 15 | 12.7 | 3.9 | 0.864 | (0.05–1.677) | ||||
| Taxanes | 4 | 4.2 | 3.85 | −0.212 | (−1.507–1.083) | ||||
| Trastuzumab | |||||||||
| Yes | 18 | 13.5 | 9.6 | 0.004 | |||||
| No | 71 | 8.2 | 3.9 | 0.792 | (0.163–1.421) | ||||
| Endocrine therapy | |||||||||
| Yes | 42 | 13.6 | 7.65 | 0.001 | 0.001 | ||||
| No | 47 | 5.4 | 3.8 | 0.936 | (0.451–1.421) | 0.936 | (0.451–1.421) | ||
| Menstrual cycle before pregnancy attempt | |||||||||
| Regular Cycle | 66 | 8.5 | 4.15 | 0.02 | |||||
| amenorrhea | 2 | 16.7 | 16.7 | ||||||
| Irregular cycle | 12 | 12.1 | 12.2 | 1.136 | (−0.463–2.736) | ||||
| Variables | n1 (%) |
|---|---|
| Mutiple pregnancy | |
| No | 125 (95.4) |
| Yes | 6 (4.6) |
| Obstetrical complications | |
| Gestational diabetes | 10 (38.5) |
| Pre-eclampsia | 5 (19.2) |
| Hypertension | 2 (7.7) |
| Premature labor | 2 (7.7) |
| Intra-uterine growth restriction | 2 (7.7) |
| Hemorragia | 1 (3.8) |
| Hydramnios | 1 (3.8) |
| Macrosomia | 1 (3.8) |
| Metastatic recurrence | 1 (3.8) |
| Placenta praevia | 1 (3.8) |
| Metabolic and vascular complications | |
| No | 114 (87.0) |
| Yes | 17 (13.0) |
| Pregnancy term (weeks of amenorrhea) | 39.2 [2.0] |
| <32 weeks | 1 (0.9) |
| 32–36 weeks | 7 (6.1) |
| ≥37 weeks | 107 (93.0) |
| Labor | |
| Induction | 23 (30.3) |
| Scheduled | 9 (11.8) |
| Spontaneous | 44 (57.9) |
| Delivery route | |
| Caesarean section | 32 (37.6) |
| Vaginal delivery | 53 (62.4) |
| Birth weight (in grams) | 3253.0 [SD: 550.8] |
| Birth size (in centimeters) | 49.5 [SD: 2.6] |
| Cranial perimeter (in centimeters) | 34.5 [SD: 1.7] |
| Apgar | |
| 1 min | 9.3 [SD: 1.7] |
| 5 min | 9.8 [SD: 0.8] |
| Gender | |
| Female | 49 (53.3) |
| Male | 43 (46.7) |
| Post-partum complications | |
| Embolisation | 1 (25.0) |
| Hypertension | 3 (75.0) |
| Breastfeeding | |
| No | 29 (40.8) |
| Yes | 42 (59.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Labrosse, J.; Lecourt, A.; Hours, A.; Sebbag, C.; Toussaint, A.; Laas, E.; Coussy, F.; Grandal, B.; Dumas, E.; Daoud, E.; et al. Time to Pregnancy, Obstetrical and Neonatal Outcomes after Breast Cancer: A Study from the Maternity Network for Young Breast Cancer Patients. Cancers 2021, 13, 1070. https://doi.org/10.3390/cancers13051070
Labrosse J, Lecourt A, Hours A, Sebbag C, Toussaint A, Laas E, Coussy F, Grandal B, Dumas E, Daoud E, et al. Time to Pregnancy, Obstetrical and Neonatal Outcomes after Breast Cancer: A Study from the Maternity Network for Young Breast Cancer Patients. Cancers. 2021; 13(5):1070. https://doi.org/10.3390/cancers13051070
Chicago/Turabian StyleLabrosse, Julie, Anne Lecourt, Alice Hours, Clara Sebbag, Aullene Toussaint, Enora Laas, Florence Coussy, Beatriz Grandal, Elise Dumas, Eric Daoud, and et al. 2021. "Time to Pregnancy, Obstetrical and Neonatal Outcomes after Breast Cancer: A Study from the Maternity Network for Young Breast Cancer Patients" Cancers 13, no. 5: 1070. https://doi.org/10.3390/cancers13051070