
VATS Pleurectomy Decortication Is a Reasonable Alternative for Higher Risk Patients in the Management of Malignant Pleural Mesothelioma: An Analysis of Short-Term Outcomes


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
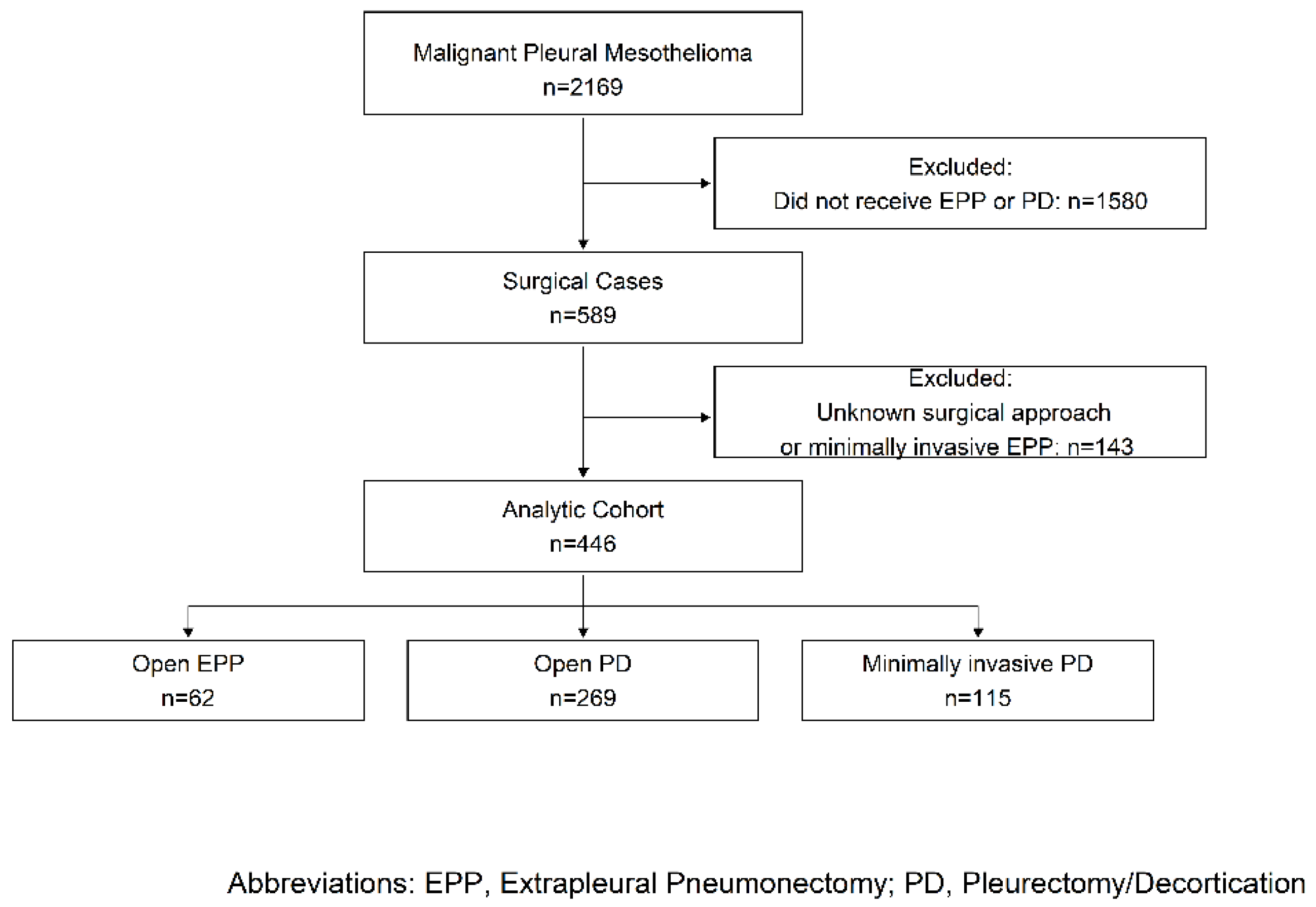
2.1. Data Source and Sample Selection
2.2. Predictors and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Extrapleural Pneumonectomy vs. Pleurectomy Decortication
3.2. Minimally Invasive vs. Open P/D
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taioli, E.; Wolf, A.S.; Camacho-Rivera, M.; Kaufman, A.; Lee, D.S.; Nicastri, D.; Rosenzweig, K.; Flores, R.M. Determinants of survival in malignant pleural mesothelioma: A Surveillance, Epidemiology, and End Results (SEER) study of 14,228 patients. PLoS ONE 2015, 10, e0145039. [Google Scholar] [CrossRef] [PubMed]
- Flores, R.M.; Pass, H.I.; Seshan, V.E.; Dycoco, J.; Zakowski, M.; Carbone, M.; Bains, M.S.; Rusch, V.W. Extrapleural pneumonectomy versus pleurectomy/decortication in the surgical management of malignant pleural mesothelioma: Results in 663 patients. J. Thorac. Cardiovasc. 2008, 135, 620–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gerwen, M.; Wolf, A.; Liu, B.; Flores, R.; Taioli, E. Short-term outcomes of pleurectomy decortication and extrapleural pneumonectomy in mesothelioma. J. Surg. Oncol. 2018, 118, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Taoili, E.; Wolf, A.S.; Flores, R.M. Meta-analysis of survival after pleurectomy decortication versus extrapleural pneumonectomy in mesothelioma. Ann. Thorac. Surg. 2015, 99, 472–480. [Google Scholar] [CrossRef] [PubMed]
- Magouliotis, D.E.; Tasiopoulou, V.S.; Athanassiadi, K. Updated meta-analysis of survival after extrapleural pneumonectomy versus pleurectomy/decortication in mesothelioma. Gen. Thorac. Cardiovasc. Surg. 2019, 67, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Burt, B.M.; Cameron, R.B.; Mollberg, N.M.; Kosinski, A.S.; Schipper, P.H.; Shrager, J.B.; Vigneswaran, W.T. Malignant pleural mesothelioma and the Society of Thoracic Surgeons Database: An analysis of surgical morbidity and mortality. J. Thorac. Cardiovasc. Surg. 2014, 148, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rena, O.; Casadio, C. Extrapleural pneumonectomy for early stage malignant pleural mesothelioma: A harmful procedure. Lung Cancer 2012, 77, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, R.M.; Lieberman-Cribbin, W.; Wolf, A.; Flores, R.M.; Taioli, E. Systematic review of quality of life following pleurectomy decortication and extrapleural pneumonectomy for malignant pleural mesothelioma. BMC Cancer 2018, 18, 1188. [Google Scholar] [CrossRef] [PubMed]
- Whitson, B.A.; Groth, S.S.; Duval, S.J.; Swanson, S.J.; Maddaus, M.A. Surgery for early-stage non-small cell lung cancer: A systematic review of the video-assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann. Thorac. Surg. 2008, 86, 2008–2016. [Google Scholar] [CrossRef] [PubMed]
- Taioli, E.; Lee, D.S.; Lesser, M.; Flores, R.M. Long-term survival in video-assisted thoracoscopic lobectomy versus open lobectomy in lung-cancer patients: A meta-analysis. Eur. J. Cardiothorac. Surg. 2013, 44, 591–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef] [PubMed]
- Martin-Ucar, A.E.; Edwards, J.G.; Rengajaran, A.; Muller, S.; Waller, D.A. Palliative surgical debulking in malignant mesothelioma. Predictors of survival and symptom control. Eur. J. Cardio Thorac. Surg. 2001, 20, 1117–1121. [Google Scholar] [CrossRef] [Green Version]
- Rintoul, R.C.; Ritchie, A.J.; Edwards, J.G.; Waller, D.A.; Coonar, A.S.; Bennett, M.; Lovato, E.; Hughes, V.; Fox-Rushby, J.A.; Sharples, L.D.; et al. Efficacy and cost of video-assisted thoracoscopic partial pleurectomy versus talc pleurodesis in patients with malignant pleural mesothelioma (MesoVATS): An open-label, randomised, controlled trial. Lancet 2014, 384, 1118–1127. [Google Scholar] [CrossRef] [Green Version]
- Matthews, C.; Freeman, C.; Sharples, L.D.; Fox-Rushby, J.; Tod, A.; Maskell, N.A.; Edwards, J.G.; Coonar, A.S.; Sivasothy, P.; Hughes, V.; et al. MesoTRAP: A feasibility study that includes a pilot clinical trial comparing video-assisted thoracoscopic partial pleurectomy decortication with indwelling pleural catheter in patients with trapped lung due to malignant pleural mesothelioma designed to address recruitment and randomisation uncertainties and sample size requirements for a phase III trial. BMJ Open Respir. Res. 2019, 6, e000368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halstead, J.C.; Lim, E.; Venkateswaran, R.M.; Charman, S.C.; Goddard, M.; Ritchie, A.J. Improved survival with VATS pleurectomy-decortication in advanced malignant mesothelioma. Eur. J. Surg. Oncol. 2005, 31, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Pass, H.I.; Temeck, B.K.; Kranda, K.; Steinberg, S.M.; Feuerstein, I.R. Preoperative tumour volume is associated with outcome in malignant pleural mesothelioma. J. Thorac. Cardiovasc. Surg. 1998, 115, 310–317. [Google Scholar] [CrossRef] [Green Version]
- Nakas, A.; Martin Ucar, A.E.; Edwards, J.G.; Waller, D.A. The role of video-assisted thoracoscopic pleurectomy/decortication in the therapeutic management of malignant pleural mesothelioma. Eur. J. Cardio Thorac. Surg. 2008, 33, 83–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | P/D (n = 269) | EPP (n = 62) | p-Value |
|---|---|---|---|
| Patient and Admission Characteristics | N (%) | N (%) | |
| Mean Age, years (SE) | 69.1 (0.5) | 64.6 (0.8) | <0.0001 |
| Gender | 0.9314 | ||
| Male | 201 (74.7) | 46 (74.2) | |
| Female | 68 (25.3) | 16 (25.8) | |
| Race | 0.1726 | ||
| NHW | 214 (79.6) | ≥11 * | |
| Hispanic or Non-White | 55 (20.4) | <11 * | |
| Primary Insurance Payer | 0.0217 | ||
| Non-Government | 120 (45.1) | 38 (61.3) | |
| Government | 146 (54.9) | 24 (38.7) | |
| Type of Admission | 0.0552 | ||
| Elective | 237 (88.8) | ≥11 * | |
| Urgent/Emergency | 30 (11.2) | <11 * | |
| Number of Comorbidities | 0.0002 | ||
| 0–1 | 120 (44.6) | 44 (71.0) | |
| ≥2 | 149 (55.4) | 18 (29.0) | |
| Complications | |||
| Cardiovascular | 36 (13.4) | 20 (32.3) | 0.0004 |
| Pulmonary | 92 (34.2) | 13 (21.0) | 0.0439 |
| Infection | 13 (4.8) | <11 * | 0.1395 |
| Bleeding | <11 * | <11 * | 0.4381 |
| Supraventricular arrhythmia | 0.0003 | ||
| No | 242 (90.0) | 45 (72.6) | |
| Yes | 27 (10.0) | 17 (27.4) | |
| Any Complication | 0.8248 | ||
| No | 156 (58.0) | 35 (56.5) | |
| Yes | 113 (42.0) | 27 (43.5) |
| EPP vs. P/D | ||
|---|---|---|
| Variable | ORadj * (95% CI) | p-Value |
| Age (years) | 0.91 (0.86–0.96) | 0.0011 |
| Gender | ||
| Female vs. Male | 0.88 (0.42–1.84) | 0.7347 |
| Race/Ethnicity | ||
| Hispanic or Non-White vs. Non-Hispanic White | 0.57 (0.22–1.45) | 0.2354 |
| Admission Type | ||
| Urgent/Emergency vs. Elective | 0.21 (0.05–0.97) | 0.0450 |
| Insurance | ||
| Non-Government vs. Government | 0.82 (0.37–1.79) | 0.6103 |
| Number of Comorbidities | ||
| ≥2 vs. 0–1 | 0.62 (0.32–1.22) | 0.1637 |
| Any Complication (Y vs. N) | Cardiovascular Complication (Y vs. N) | Supraventricular Arrhythmia (Y vs. N) | Pulmonary Complication (Y vs. N) | |
|---|---|---|---|---|
| ORadj * (95% CI); p-Value | ORadj * (95% CI); p-Value | ORadj * (95% CI); p-Value | ORadj * (95% CI); p-Value | |
| Multivariable Analysis (n = 326) | ||||
| EPP vs. P/D | 2.12 (1.08–4.18); 0.0302 | 5.00 (2.23–11.24); <0.0001 | 6.63 (2.64–16.64); <0.0001 | 0.89 (0.41–1.91); 0.7619 |
| Propensity-Matched Analysis (n = 100) | ||||
| EPP vs. P/D | 1.11 (0.45–2.73); 0.8186 | 2.60 (0.93–7.29); 0.0694 | 2.75 (0.88–8.64); 0.0832 | 0.58 (0.23–1.48); 0.2571 |
| Variable | Open (n = 269) | Minimally Invasive (n = 115) | p-Value |
|---|---|---|---|
| Patient and Admission Characteristics | N (%) | N (%) | |
| Mean Age, years (SE) | 69.1 (0.5) | 71.8 (1.0) | 0.0132 |
| Gender | 0.5773 | ||
| Male | 201 (74.7) | 89 (77.4) | |
| Female | 68 (25.3) | 26 (22.6) | |
| Race | 0.0524 | ||
| NHW | 214 (79.6) | 81 (70.4) | |
| Hispanic or Non-White | 55 (20.4) | 34 (29.6) | |
| Primary Insurance Payer | 0.1194 | ||
| Non-Government | 120 (45.1) | 42 (36.5) | |
| Government | 146 (54.9) | 73 (63.5) | |
| Type of Admission | <0.0001 | ||
| Elective | 237 (88.8) | 60 (52.6) | |
| Urgent/Emergency | 30 (11.2) | 54 (47.4) | |
| Number of Comorbidities | 0.7899 | ||
| 0–1 | 120 (44.6) | 53 (46.1) | |
| ≥2 | 149 (55.4) | 62 (53.9) | |
| Complications | |||
| Cardiovascular | 36 (13.4) | 11 (9.6) | 0.2958 |
| Pulmonary | 92 (34.2) | 31 (27.0) | 0.1635 |
| Infection | 13 (4.8) | <11 * | 0.8369 |
| Bleeding | <11 * | <11 * | 0.7296 |
| Any Complication | 0.0995 | ||
| No | 156 (58.0) | 77 (67.0) | |
| Yes | 113 (42.0) | 38 (33.0) |
| Minimally Invasive vs. Open | ||
|---|---|---|
| Variable | ORadj * (95% CI) | p-Value |
| Age (years) | 1.05 (1.01–1.08) | 0.0106 |
| Gender | ||
| Female vs. Male | 0.90 (0.49–1.64) | 0.7343 |
| Race/Ethnicity | ||
| Hispanic or Non-White vs. Non-Hispanic White | 1.37 (0.76–2.49) | 0.3008 |
| Admission Type | ||
| Urgent/Emergency vs. Elective | 7.18 (4.07–12.64) | <0.0001 |
| Insurance | ||
| Non-Government vs. Government | 1.11 (0.61–2.00) | 0.7353 |
| Number of Comorbidities | ||
| ≥2 vs. 0–1 | 0.66 (0.40–1.10) | 0.1126 |
| Any Complication (Y vs. N) | Cardiovascular Complication (Y vs. N) | Pulmonary Complication (Y vs. N) | |
|---|---|---|---|
| ORadj * (95% CI); p-Value | ORadj * (95% CI); p-Value | ORadj * (95% CI); p-Value | |
| Multivariable Analysis (n = 378) | |||
| Minimally Invasive vs. Open | 0.58 (0.34–1.01); 0.0524 | 0.88 (0.40–1.95); 0.7518 | 0.55 (0.31–0.99); 0.0448 |
| Propensity-Matched analysis (n = 150) | |||
| Minimally Invasive vs. Open | 0.70 (0.37–1.32); 0.2649 | 1.13 (0.43–2.92); 0.8085 | 0.65 (0.30–1.38); 0.2606 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.-S.; Carollo, A.; Alpert, N.; Taioli, E.; Flores, R. VATS Pleurectomy Decortication Is a Reasonable Alternative for Higher Risk Patients in the Management of Malignant Pleural Mesothelioma: An Analysis of Short-Term Outcomes. Cancers 2021, 13, 1068. https://doi.org/10.3390/cancers13051068
Lee D-S, Carollo A, Alpert N, Taioli E, Flores R. VATS Pleurectomy Decortication Is a Reasonable Alternative for Higher Risk Patients in the Management of Malignant Pleural Mesothelioma: An Analysis of Short-Term Outcomes. Cancers. 2021; 13(5):1068. https://doi.org/10.3390/cancers13051068
Chicago/Turabian StyleLee, Dong-Seok, Andrea Carollo, Naomi Alpert, Emanuela Taioli, and Raja Flores. 2021. "VATS Pleurectomy Decortication Is a Reasonable Alternative for Higher Risk Patients in the Management of Malignant Pleural Mesothelioma: An Analysis of Short-Term Outcomes" Cancers 13, no. 5: 1068. https://doi.org/10.3390/cancers13051068