
An Observational Cohort Study on 194 Supraglottic Cancer Patients: Implications for Laser Surgery and Adjuvant Treatment

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| adj. ther. | adjuvant therapy |
| aRT | adjuvant RT |
| aCRT | adjuvant chemoradiotherapy |
| age (cont.) | age (continuous) |
| CCI | Charlson Comorbidity Index |
| CI | confidence interval |
| Colon-Ca | Colon cancer |
| DSS | disease specific survival |
| HR | hazard ratio |
| HNSCC | head and neck squamous cell carcinoma |
| LT-S | long-term survivor, i.e., living at the end of follow-up time |
| m | months |
| n.a. | not applicable |
| ND = neck diss | neck dissection |
| NSCLC | non-small cell lung cancer |
| OP+/-a[C]RT | surgery with adjuvant radiotherapy or adjuvant chemoradiotherapy, as indicated by risk and stage |
| OPL | open partial laryngectomy |
| Pneumo | Pneumonia |
| pCRT | primary chemoradiotherapy |
| pRT | primary radiotherapy |
| p(C)RT = pCRT or pRT | primary (chemo-)radiotherapy, primary chemoradiotherapy or primary radiotherapy |
| Rect-Ca | Carcinoma of the rectum |
| TL | total laryngectomy |
| TLM | transoral laser microsurgery |
| tu | death due to locoregional recurrent tumor |
| UICC | Union International Contre le Cancer (International Union against Cancer) |
| 5-year OS | 5-year overall survival |
| y | years |
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Am Cancer Soc Key Statistics for Laryngeal and Hypopharyngeal Cancers. 2020. Available online: https://www.cancer.org/content/dam/CRC/PDF/Public/8664.00.pdf (accessed on 16 October 2020).
- Brandstorp-Boesen, J.; Falk, R.S.; Boysen, M.; Brondbo, K. Long-term trends in gender, T-stage, subsite and treatment for laryngeal cancer at a single center. Eur. Arch. Otorhinolaryngol. 2014, 271, 3233–3239. [Google Scholar] [CrossRef]
- Van Dijk, B.A.; Karim-Kos, H.E.; Coebergh, J.W.; Marres, H.A.; de Vries, E. Progress against laryngeal cancer in The Netherlands between 1989 and 2010. Int. J. Cancer 2014, 134, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Ramroth, H.; Dietz, A.; Becher, H. Interaction effects and population-attributable risks for smoking and alcohol on laryngeal cancer and its subsites. A case-control study from Germany. Methods Inf. Med. 2004, 43, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Talamini, R.; Bosetti, C.; La Vecchia, C.; Dal Maso, L.; Levi, F.; Bidoli, E.; Negri, E.; Pasche, C.; Vaccarella, S.; Barzan, L.; et al. Combined effect of tobacco and alcohol on laryngeal cancer risk: A case-control study. Cancer Causes Control CCC 2002, 13, 957–964. [Google Scholar] [CrossRef]
- La Vecchia, C.; Zhang, Z.F.; Altieri, A. Alcohol and laryngeal cancer: An update. Eur. J. Cancer Prev. 2008, 17, 116–124. [Google Scholar] [CrossRef]
- Cosetti, M.; Yu, G.P.; Schantz, S.P. Five-year survival rates and time trends of laryngeal cancer in the US population. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 370–379. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.B.; Nichols, A.C.; Fung, K.; Yoo, J.; MacNeil, S.D. Treatment of early stage Supraglottic squamous cell carcinoma: Meta-analysis comparing primary surgery versus primary radiotherapy. J. Otolaryngol. Head Neck Surg. 2018, 47, 19. [Google Scholar] [CrossRef]
- van der Woerd, B.; Patel, K.B.; Nichols, A.C.; Fung, K.; Yoo, J.; MacNeil, S.D. Functional outcomes in early (T1/T2) supraglottic cancer: A systematic review. J. Otolaryngol. Head Neck Surg. 2018, 47, 76. [Google Scholar] [CrossRef] [Green Version]
- Raitiola, H.; Pukander, J.; Laippala, P. Glottic and supraglottic laryngeal carcinoma: Differences in epidemiology, clinical characteristics and prognosis. Acta Otolaryngol. 1999, 119, 847–851. [Google Scholar] [CrossRef]
- Pfister, D.G. NCCN Clinical Practice Guidelines in Oncology in Head and Neck Cancers (Version 2.2020). Available online: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 6 December 2020).
- Silvestri, F.; Bussani, R.; Stanta, G.; Cosatti, C.; Ferlito, A. Supraglottic versus glottic laryngeal cancer: Epidemiological and pathological aspects. Orl J. Oto-Rhino-Laryngol. Its Relat. Spec. 1992, 54, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Iro, H.; Mantsopoulos, K.; Zenk, J.; Waldfahrer, F.; Psychogios, G. Results of transoral laser resection in T1-2 oropharyngeal, hypopharyngeal and laryngeal carcinomas. Laryngo-Rhino-Otologie 2011, 90, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, C.W. Transoral laryngeal surgery using the CO2 laser: Laboratory experiments and clinical experience. Laryngoscope 1978, 88, 1399–1420. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.K.; Shapshay, S.M.; Strong, M.S.; Hyams, V.J. Transoral partial supraglottic resection using the CO2 laser. Laryngoscope 1983, 93, 429–432. [Google Scholar] [CrossRef]
- Ambrosch, P.; Kron, M.; Steiner, W. Carbon dioxide laser microsurgery for early supraglottic carcinoma. Ann. Otol. Rhinol. Laryngol. 1998, 107, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Iro, H.; Waldfahrer, F.; Altendorf-Hofmann, A.; Weidenbecher, M.; Sauer, R.; Steiner, W. Transoral laser surgery of supraglottic cancer: Follow-up of 141 patients. Arch. Otolaryngol. Head Neck Surg. 1998, 124, 1245–1250. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, J.P.; Suarez, C.; Silver, C.E.; Rinaldo, A.; Ambrosch, P.; Fagan, J.J.; Genden, E.M.; Ferlito, A. Transoral laser surgery for supraglottic cancer. Head Neck 2008, 30, 658–666. [Google Scholar] [CrossRef]
- Ambrosch, P.; Gonzalez-Donate, M.; Fazel, A.; Schmalz, C.; Hedderich, J. Transoral Laser Microsurgery for Supraglottic Cancer. Front. Oncol. 2018, 8, 158. [Google Scholar] [CrossRef] [Green Version]
- Davis, R.K.; Kriskovich, M.D.; Galloway, E.B., 3rd; Buntin, C.S.; Jepsen, M.C. Endoscopic supraglottic laryngectomy with postoperative irradiation. Ann. Otol. Rhinol. Laryngol. 2004, 113, 132–138. [Google Scholar] [CrossRef]
- Steiner, W.; Ambrosch, P. Stellenwert der Laserchirurgie bei Tumoren der oberen Luft-und Speisewege. Der. Onkol. 1996, 2, 346–351. [Google Scholar] [CrossRef]
- Rudert, H.H.; Werner, J.A.; Hoft, S. Transoral carbon dioxide laser resection of supraglottic carcinoma. Ann. Otol. Rhinol. Laryngol. 1999, 108, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Ambrosch, P.; Brinck, U.; Fischer, G.; Steiner, W. Special aspects of histopathologic diagnosis in laser microsurgery of cancers of the upper aerodigestive tract. Laryngo-Rhino-Otologie 1994, 73, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Jumaily, M.; Faraji, F.; Osazuwa-Peters, N.; Walker, R.J.; Ward, G.M. Prognostic significance of surgical margins after transoral laser microsurgery for early-stage glottic squamous cell carcinoma. Oral Oncol. 2019, 97, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Hanna, J.; Brauer, P.R.; Morse, E.; Mehra, S. Margins in Laryngeal Squamous Cell Carcinoma Treated with Transoral Laser Microsurgery: A National Database Study. Otolaryngol. Head Neck Surg. 2019, 161, 986–992. [Google Scholar] [CrossRef]
- Pedregal-Mallo, D.; Sanchez Canteli, M.; Lopez, F.; Alvarez-Marcos, C.; Llorente, J.L.; Rodrigo, J.P. Oncological and functional outcomes of transoral laser surgery for laryngeal carcinoma. Eur. Arch. Otorhinolaryngol. 2018, 275, 2071–2077. [Google Scholar] [CrossRef]
- Fiz, I.; Mazzola, F.; Fiz, F.; Marchi, F.; Filauro, M.; Paderno, A.; Parrinello, G.; Piazza, C.; Peretti, G. Impact of Close and Positive Margins in Transoral Laser Microsurgery for Tis-T2 Glottic Cancer. Front. Oncol. 2017, 7, 245. [Google Scholar] [CrossRef]
- Harreus, U. Chirurgische Onkologie, Halschirurgie. In HNO Update 2020; Iro, H., Verse, T., Wollenberg, B., Zenk, J., Eds.; Med Update: Mainz, Germany, 2020. [Google Scholar]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef] [Green Version]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefebvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef] [Green Version]
- Silver, C.E.; Beitler, J.J.; Shaha, A.R.; Rinaldo, A.; Ferlito, A. Current trends in initial management of laryngeal cancer: The declining use of open surgery. Eur. Arch. Otorhinolaryngol. 2009, 266, 1333–1352. [Google Scholar] [CrossRef]
- Dyckhoff, G.; Plinkert, P.K.; Ramroth, H. A change in the study evaluation paradigm reveals that larynx preservation compromises survival in T4 laryngeal cancer patients. BMC Cancer 2017, 17, 609. [Google Scholar] [CrossRef] [Green Version]
- Allison, P. Survival Analysis Using SAS A Practical Guide, 2nd ed.; SAS Institute Inc.: Cary, NC, USA, 2010. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Category | TLM | OPL | TL | pCRT | pRT | All |
|---|---|---|---|---|---|---|---|
| Total | 96 | 7 | 57 | 20 | 14 | 194 | |
| Age (cont.) a | 59.6 (37–79) | 61.3 (51–77) | 59.7 (40–80) | 58.4 (41–77) | 62.1 (40–79) | 59.7 (37–80) | |
| Sex | Males | 81 (84.4) | 7 (100) | 53 (93.0) | 15 (75.0) | 10 (71.4) | 166 (85.6) |
| Females | 15 (15.6) | 0 (0.0) | 4 (7.0) | 5 (25.0) | 4 (28.6) | 28 (14.4) | |
| CCI | 0 | 71 (74.0) | 4 (57.1) | 38 (66.7) | 16 (80.0) | 5 (35.7) | 134 (69.1) |
| 1 | 25 (26.0) | 3 (42.9) | 19 (33.3) | 4 (20.0) | 9 (64.3) | 60 (30.9) | |
| T category | 1 | 31 (32.3) | 1 (14.3) | 1 (1.8) | 2 (10.0) | 2 (14.3) | 37 (19.1) |
| 2 | 39 (40.6) | 4 (57.1) | 14 (24.6) | 5 (25.0) | 6 (42.9) | 68 (35.1) | |
| 3 | 16 (16.7) | 2 (28.6) | 24 (42.1) | 7 (35.0) | 3 (21.4) | 52 (26.8) | |
| 4 | 10 (10.4) | 0 (0.0) | 18 (31.6) | 6 (30.0) | 3 (21.4) | 37 (19.1) | |
| N stage | 0 | 50 (52.1) | 5 (71.4) | 30 (52.6) | 9 (45.0) | 4 (28.6) | 98 (50.5) |
| 1 | 15 (15.6) | 0 (0.0) | 7 (12.3) | 2 (10.0) | 3 (21.4) | 27 (13.9) | |
| 2 | 26 (27.1) | 2 (28.6) | 20 (35.1) | 6 (30.0) | 6 (42.9) | 60 (30.9) | |
| 3 | 1 (1.0) | 0 (0.0) | 0 (0.0) | 2 (10.0) | 1 (7.1) | 4 (2.1) | |
| X | 4 (4.2) | 0 (0.0) | 0 (0.0) | 1 (5.0) | 0 (0.0) | 5 (2.6) | |
| UICC stage | I | 20 (20.8) | 0 (0.0) | 1 (1.8) | 1 (5.0) | 0 (0.0) | 22 (11.3) |
| II | 20 (20.8) | 4 (57.1) | 7 (12.3) | 3 (15.0) | 4 (28.6) | 38 (19.6) | |
| III | 23 (24.0) | 1 (14.3) | 19 (33.3) | 6 (30.0) | 3 (21.4) | 52 (26.8) | |
| IV | 33 (34.4) | 2 (28.6) | 30 (52.6) | 10 (50.0) | 7 (50.0) | 82 (42.3) | |
| Neck diss | No | 25 (26.0) | 1 (14.3) | 3 (5.3) | 18 (90.0) | 14 (100) | 61 (31.4) |
| Yes | 71 (74.0) | 6 (85.7) | 54 (94.7) | 2 (10.0) | 0 (0.0) | 133 (68.6) | |
| Resection | 0 | 39 (40.6) | 6 (85.7) | 38 (66.7) | 0 (0.0) | 0 (0.0) | 83 (42.8) |
| 1 | 18 (18.8) | 0 (0.0) | 7 (12.3) | 0 (0.0) | 0 (0.0) | 25 (12.9) | |
| 2 | 4 (4.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 4 (2.1) | |
| X | 28 (29.2) | 1 (14.3) | 9 (15.8) | 2 (10.0) | 3 (21.4) | 43 (22.2) | |
| missing | 7 (7.3) | 0 (0.0) | 3 (5.3) | 18 (90.0) | 11 (78.6) | 39 (20.1) | |
| Adj. ther. | None | 49 (51,0) | 4 (57.1) | 26 (46) | n.a. | n.a. | 79 (40.1) |
| aRT | 43 (44.8) | 3 (42.8) | 23 (41.1) | n.a. | n.a. | 69 (35.6) | |
| aCRT | 4 (4.1) | 0 (0.0) | 7 (12.5) | n.a. | n.a. | 11 (5.7) | |
| aCT | 2 (2.0) | 0 (0.0) | 0 (0.0 | n.a. | n.a. | 2 (1.0) | |
| unknown | 14 (14.6) | 0 (0.0) | 5 (8.8) | 2 (10.0) | 2 (14.3) | 23 (11.9) |
| Localization, T (n, DSS/OS) * | 5-y DSS [%] (95% CI) | 10-y DSS [%] (95% CI) | 5-y OS [%] (95% CI) | 10-y OS [%] (95% CI) |
|---|---|---|---|---|
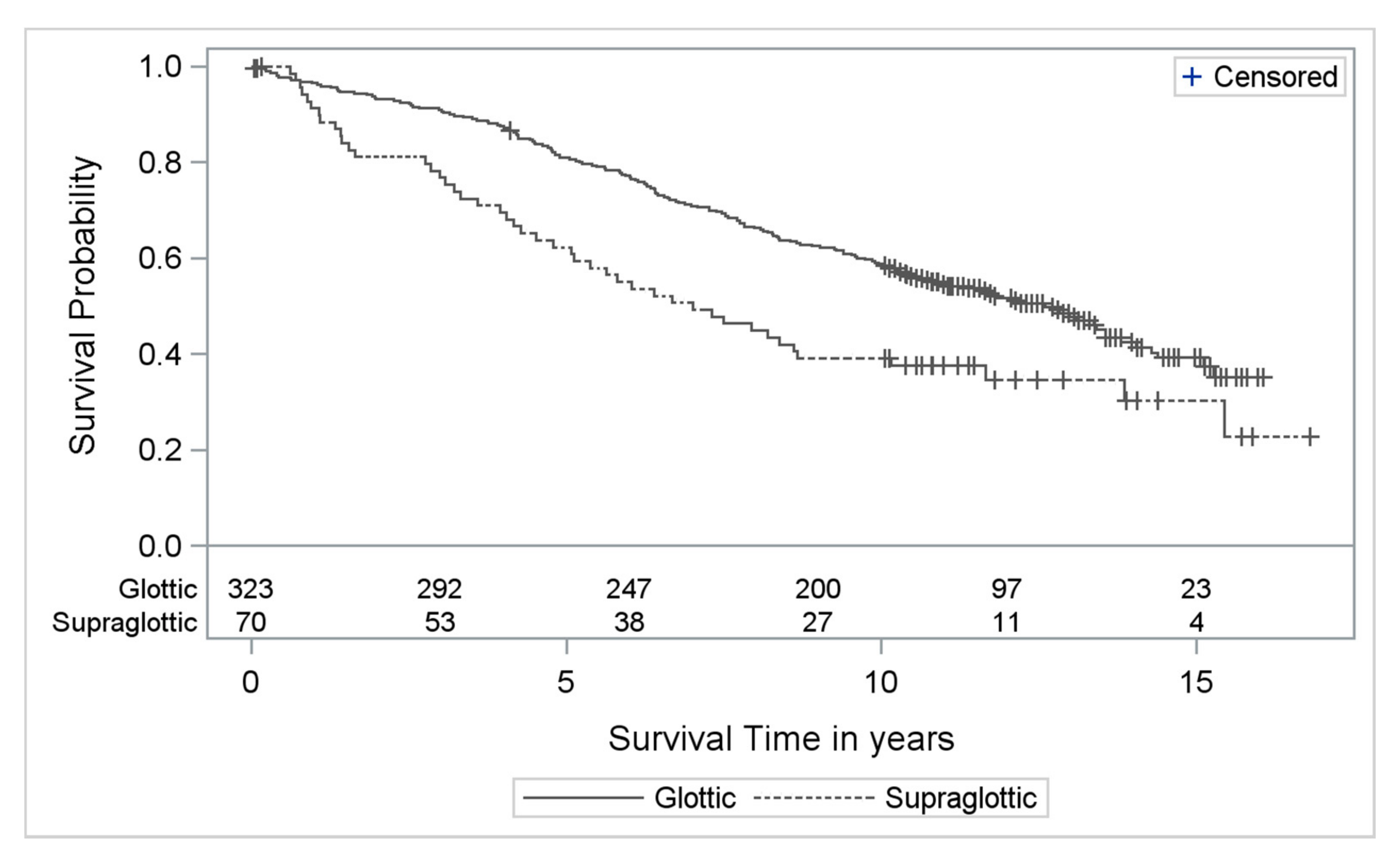
| Supraglottic | 92 (71–98) | 87 (65–96) | 65 (45–79) | 32 (17–49) |
| T1 (29/31) | ||||
| T2 (39/39) | 75 (57–86) | 71 (53–83) | 61 (43–74) | 45 (29–60) |
| T1 + T2 (68/70) | 82 (69–89) | 78 (64–86) | 62 (50–73) | 39 (28–50) |
| Glottic | 96 (93–98) | 94 (90–97) | 82 (76-86) | 60 (54–66) |
| T1 (238/243) | ||||
| T2 (80/80) | 89 (80–95) | 82 (70–89) | 79 (68–86) | 54 (42–64) |
| T1 + T2 (318/323) | 95 (91–97) | 91 (87–94) | 81 (76–85) | 59 (53–64) |
| T Category | R0 | Rx | R1 | R2 | R Missing |
|---|---|---|---|---|---|
| T1 (n = 31) | 14 (45.2%) | 10 (32.3%) | 5 (16.1%) | 0 (0.0%) | 2 (6.5%) |
| T2 (n = 39) | 20 (51.3%) | 8 (20.5%) | 9 (23.1%) | 0 (0.0%) | 2 (5.1%) |
| T3 (n = 16) | 4 (20.5%) | 8 (50.0%) | 2 (12.5%) | 1 (6.3%) | 1 (6.3%) |
| T4 (n = 10) | 2 (20.0%) | 2 (20.0%) | 3 (30.0%) | 2 (20.0%) | 1 (10.0%) |
| T Category | No adj. (n = 47) | aRT (n = 43) | aCRT (n = 4) | aCT (n = 2) |
|---|---|---|---|---|
| T1 (n = 31) | 23 (74.2%) | 7 (22.6%) | 0 (0%) | 1 (3.2) |
| T2 (n = 39) | 14 (35.9%) | 24 (61.5%) | 1 (2.6%) | 0 (.0) |
| T3 (n = 16) | 8 (50.0%) | 6 (37.5%) | 1 (6.3%) | 1 (6.3) |
| T4 (n = 10) | 2 (20.0%) | 6 (60.0%) | 2 (20.0%) | 0 (0.0) |
| Procedure | Category | Stage I | Stage II | Stage III | Stage IV | All |
|---|---|---|---|---|---|---|
| ND | No | 14 (63.6) | 15 (39.5) | 15 (28.8) | 17 (20.7) | 61 (31.4) |
| Yes | 8 (36.4) | 23 (60.5) | 37 (71.2) | 65 (79.3) | 133 (68.6) | |
| Resection | R0 | 10 (45.5) | 21 (55.3) | 24 (46.2) | 28 (34.1) | 83 (42.8) |
| Rx/R1/R2 | 11 (50.0) | 9 (23.7) | 15 (28.8) | 37 (45.1) | 72 (37.1) | |
| Missing | 1 (4.5) | 8 (21.1) | 13 (25.0) | 17 (20.7) | 39 (20.1) | |
| Adj. treatment | No | 21 (95.5) | 29 (76.3) | 28 (53.8) | 34 (41.5) | 112 (57.7) |
| Yes | 1 (4.5) | 9 (23.7) | 24 (46.2) | 48 (58.5) | 82 (42.3) |
| Indication | Success | Intermediate/Uncertain | Failure |
|---|---|---|---|
| Clear indication (R1, any N R2, any N any R, N2 any R, N3) | R0N2b:13y10m, NSCLC R0N2b: 5y9m, Rect-Ca R1N0 (aCRT!): LT-S R1N0: LT-S R1N2c: LT-S R1N1: 5y1m, Colon-Ca RxN2b: 8y7m, Pneumo | (R0N2b): 4y3m M1 | R0N2c: 3y2m, tu R0N2: 2y11m, tu R0N2c: 1y5m, tu R1N0: 0y9m tu R1N2b: 2y10m, tu R1N2c: 3y3m, tu R1N1: 1y5m tu RxN2: 1y3m, tu RxN3: 1y5m, tu |
| Study | Number of Patients | 5-y OS [%] |
|---|---|---|
| Ambrosch, 1998 [17] | 48 | 76.0 (pT1 + T2) |
| Iro, 1998 [18] | 69 | 75.4 (stage I + II) |
| Steiner, Ambrosch, 1996 [22] | 43 | 72.8 (stage I + II) |
| Ambrosch, 2018 [20] | 67 | 69.0 (stage I + II) |
| Dyckhoff, present study | 70 | 62.0 (pT1 + pT2) |
| Iro, 2011 [14] | 137 | 59.4 (pT1 + pT2) |
| Failure | Early failure: tumor-related death ≤ 2 years | |
| Intermediate failure: tumor related death 2 years < ... ≤ 5 years | ||
| Intermediate/uncertain | Late failure/success not sustained: tumor related death > 5 years | |
| Uncertain success | Death due to intercurrent disease, e.g., myocardial infarction, stroke ≤ 5 years | |
| Tumor-related death which cannot be prevented by locoregional treatment, i.e., distant metastases ≤ 5 years | ||
| Success | Sustained oncologic success: no recurrence, death due to intercurrent disease > 5 years | |
| Clear success: no recurrence and long-term survivor (beyond time of follow-up) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dyckhoff, G.; Warta, R.; Herold-Mende, C.; Rudolph, E.; Plinkert, P.K.; Ramroth, H. An Observational Cohort Study on 194 Supraglottic Cancer Patients: Implications for Laser Surgery and Adjuvant Treatment. Cancers 2021, 13, 568. https://doi.org/10.3390/cancers13030568
Dyckhoff G, Warta R, Herold-Mende C, Rudolph E, Plinkert PK, Ramroth H. An Observational Cohort Study on 194 Supraglottic Cancer Patients: Implications for Laser Surgery and Adjuvant Treatment. Cancers. 2021; 13(3):568. https://doi.org/10.3390/cancers13030568
Chicago/Turabian StyleDyckhoff, Gerhard, Rolf Warta, Christel Herold-Mende, Elisabeth Rudolph, Peter K. Plinkert, and Heribert Ramroth. 2021. "An Observational Cohort Study on 194 Supraglottic Cancer Patients: Implications for Laser Surgery and Adjuvant Treatment" Cancers 13, no. 3: 568. https://doi.org/10.3390/cancers13030568