
Interventional Radiology Image-Guided Locoregional Therapies (LRTs) and Immunotherapy for the Treatment of HCC

 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Hepatocellular Carcinoma and Its Current Therapeutic Options
2. Immune System Changes in HCC Patients
3. LRT and Immunomodulation
4. Pro-Oncogenic Effects of LRTs
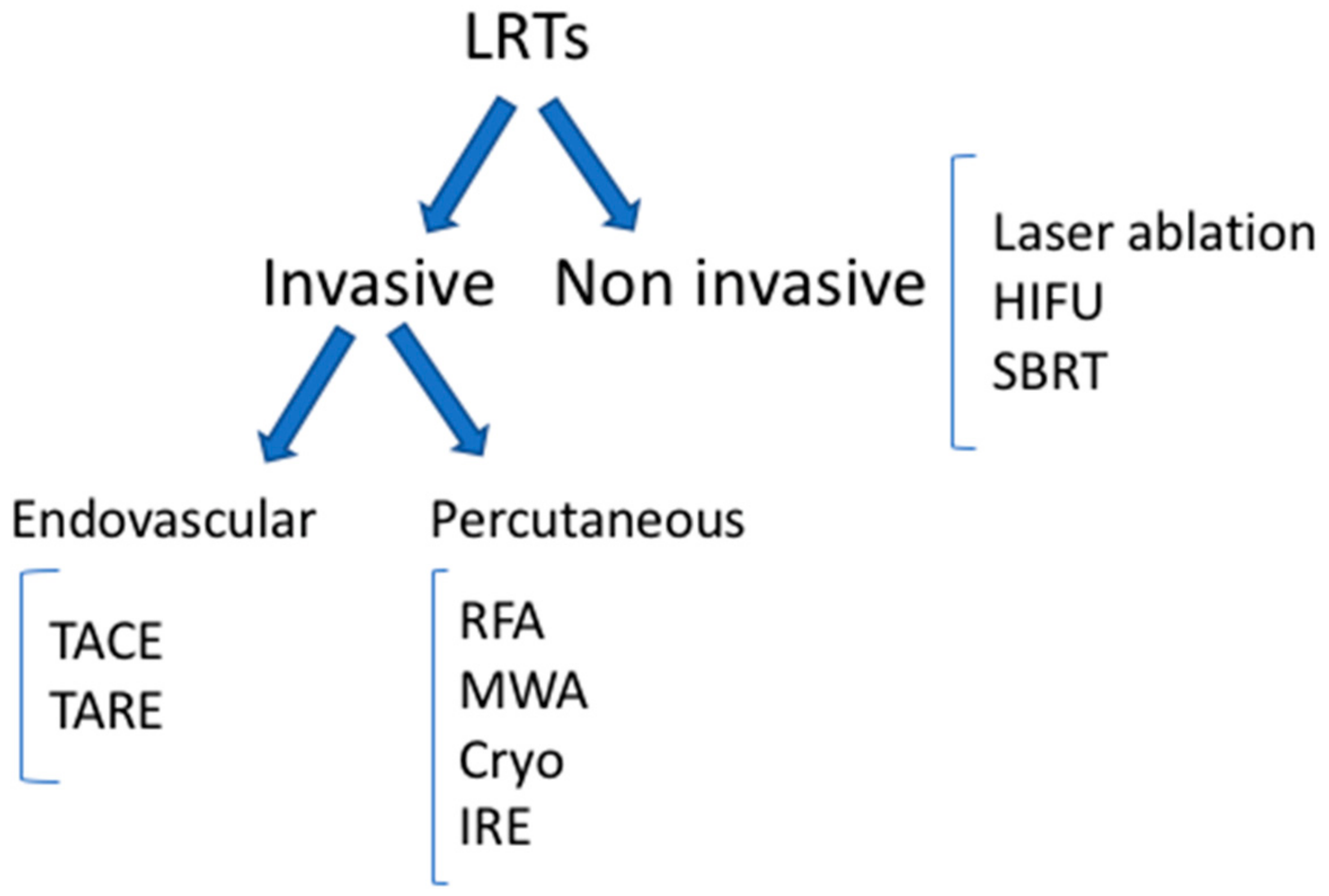
5. LRTs: Classification
6. Invasive Percutaneous LRTs
6.1. Radiofrequency Ablation (RFA)
6.1.1. Technique
6.1.2. Immunomodulation
6.2. Cryoablation
6.2.1. Technique
6.2.2. Immunomodulation
6.3. Microwave Ablation (MWA)
6.3.1. Technique
6.3.2. Immunomodulation
7. Invasive Endovascular LRTs
7.1. Trans-Arterial Chemoembolization (TACE)
7.1.1. Technique
7.1.2. Immunomodulation
7.2. Trans-Arterial Radioembolization (TARE)
7.2.1. Technique
7.2.2. Immunomodulation
8. Ablation Techniques under Evaluation
8.1. High-Intensity Focused Ultrasound (HIFU)
8.2. Laser Ablation
8.3. Stereotactic Body Radiation Therapy (SBRT)
8.4. Irreversible Electroporation (IRE)
9. Immunotherapy
9.1. Immune Checkpoint Inhibitors
9.2. Other Immunotherapies
10. Combination of Immunotherapy-LRT
11. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Available online: http://Globocan.Iarc.Fr (accessed on 20 September 2021).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. World Cancer Report: Cancer Research for Cancer Prevention; IARC Press: Lyon, France, 2020. [Google Scholar]
- Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; Artaman, A.; et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level. JAMA Oncol. 2017, 3, 1683. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.N.; Splan, M.F.; Weiss, N.S.; McDonald, G.B.; Beretta, L.; Lee, S.P. Incidence and Predictors of Hepatocellular Carcinoma in Patients With Cirrhosis. Clin. Gastroenterol. Hepatol. 2007, 5, 938–945.e4. [Google Scholar] [CrossRef] [PubMed]
- Lampertico, P.; Agarwal, K.; Berg, T.; Buti, M.; Janssen, H.L.A.; Papatheodoridis, G.; Zoulim, F.; Tacke, F. EASL 2017 Clinical Practice Guidelines on the Management of Hepatitis B Virus Infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNamara, M.G.; Slagter, A.E.; Nuttall, C.; Frizziero, M.; Pihlak, R.; Lamarca, A.; Tariq, N.; Valle, J.W.; Hubner, R.A.; Knox, J.J.; et al. Sorafenib as First-Line Therapy in Patients with Advanced Child-Pugh B Hepatocellular Carcinoma—A Meta-Analysis. Eur. J. Cancer 2018, 105, 1–9. [Google Scholar] [CrossRef]
- Huynh, J.; Cho, M.; Kim, E.; Ren, M.; Amaya-Chanaga, C.; Vogel, A. P-78 Post Hoc Analysis in Patients with Unresectable Hepatocellular Carcinoma Who Progressed to Child-Pugh B Liver Function in the Phase 3 REFLECT Study of Lenvatinib vs Sorafenib. Ann. Oncol. 2021, 32, S123–S124. [Google Scholar] [CrossRef]
- Kim, H.; Bang, Y.; Lee, M.A.; Kim, J.W.; Kim, J.H.; Chon, H.J.; Kang, B.; Kang, M.J.; Kim, I.; Cheon, J.; et al. Regorafenib in Patients with Advanced Child-Pugh B Hepatocellular Carcinoma: A Multicentre Retrospective Study. Liver Int. 2020, 40, 2544–2552. [Google Scholar] [CrossRef]
- Zhu, A.X.; Baron, A.D.; Malfertheiner, P.; Kudo, M.; Kawazoe, S.; Pezet, D.; Weissinger, F.; Brandi, G.; Barone, C.A.; Okusaka, T.; et al. Ramucirumab as Second-Line Treatment in Patients With Advanced Hepatocellular Carcinoma. JAMA Oncol. 2017, 3, 235. [Google Scholar] [CrossRef]
- Eatrides, J.; Wang, E.; Kothari, N.; Kim, R. Role of Systemic Therapy and Future Directions for Hepatocellular Carcinoma. Cancer Control 2017, 24, 107327481772924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardee, A.D.; Butterfield, L.H. Immunotherapy of Hepatocellular Carcinoma. Oncoimmunology 2012, 1, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Kapanadze, T.; Gamrekelashvili, J.; Ma, C.; Chan, C.; Zhao, F.; Hewitt, S.; Zender, L.; Kapoor, V.; Felsher, D.W.; Manns, M.P.; et al. Regulation of Accumulation and Function of Myeloid Derived Suppressor Cells in Different Murine Models of Hepatocellular Carcinoma. J. Hepatol. 2013, 59, 1007–1013. [Google Scholar] [CrossRef] [Green Version]
- Makarova-Rusher, O.V.; Medina-Echeverz, J.; Duffy, A.G.; Greten, T.F. The Yin and Yang of Evasion and Immune Activation in HCC. J. Hepatol. 2015, 62, 1420–1429. [Google Scholar] [CrossRef] [Green Version]
- Korangy, F.; Ormandy, L.A.; Bleck, J.S.; Klempnauer, J.; Wilkens, L.; Manns, M.P.; Greten, T.F. Spontaneous Tumor-Specific Humoral and Cellular Immune Responses to NY-ESO-1 in Hepatocellular Carcinoma. Clin. Cancer Res. 2004, 10, 4332–4341. [Google Scholar] [CrossRef] [Green Version]
- Mizukoshi, E.; Nakamoto, Y.; Arai, K.; Yamashita, T.; Sakai, A.; Sakai, Y.; Kagaya, T.; Yamashita, T.; Honda, M.; Kaneko, S. Comparative Analysis of Various Tumor-Associated Antigen-Specific t-Cell Responses in Patients with Hepatocellular Carcinoma. Hepatology 2011, 53, 1206–1216. [Google Scholar] [CrossRef]
- Cassim, S.; Pouyssegur, J. Tumor Microenvironment: A Metabolic Player That Shapes the Immune Response. Int. J. Mol. Sci. 2019, 21, 157. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.-Q. Roles of Tregs in Development of Hepatocellular Carcinoma: A Meta-Analysis. World J. Gastroenterol. 2014, 20, 7971. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Xu, D.; Liu, Z.; Shi, M.; Zhao, P.; Fu, B.; Zhang, Z.; Yang, H.; Zhang, H.; Zhou, C.; et al. Increased Regulatory T Cells Correlate with CD8 T-Cell Impairment and Poor Survival in Hepatocellular Carcinoma Patients. Gastroenterology 2007, 132, 2328–2339. [Google Scholar] [CrossRef]
- Brace, C.L. Radiofrequency and Microwave Ablation of the Liver, Lung, Kidney, and Bone: What Are the Differences? Curr. Probl. Diagn. Radiol. 2009, 38, 135–143. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.-C.; Wu, T.-J.; Chou, H.-S.; Yu, M.-C.; Hsu, P.-Y.; Hsu, H.-Y.; Wang, C.-C. The Impact of CD4+CD25+ T Cells in the Tumor Microenvironment of Hepatocellular Carcinoma. Surgery 2012, 151, 213–222. [Google Scholar] [CrossRef]
- Wang, F.; Jing, X.; Li, G.; Wang, T.; Yang, B.; Zhu, Z.; Gao, Y.; Zhang, Q.; Yang, Y.; Wang, Y.; et al. Foxp3+ Regulatory T Cells Are Associated with the Natural History of Chronic Hepatitis B and Poor Prognosis of Hepatocellular Carcinoma. Liver Int. 2012, 32, 644–655. [Google Scholar] [CrossRef]
- Chen, K.; Zhou, L.; Xie, H.; Ahmed, T.-E.; Feng, X.; Zheng, S. Intratumoral Regulatory T Cells Alone or in Combination with Cytotoxic T Cells Predict Prognosis of Hepatocellular Carcinoma after Resection. Med. Oncol. 2012, 29, 1817–1826. [Google Scholar] [CrossRef]
- Mathai, A.M.; Kapadia, M.J.; Alexander, J.; Kernochan, L.E.; Swanson, P.E.; Yeh, M.M. Role of Foxp3-Positive Tumor-Infiltrating Lymphocytes in the Histologic Features and Clinical Outcomes of Hepatocellular Carcinoma. Am. J. Surg. Pathol. 2012, 36, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Deng, B.; Tang, W.; Liu, T.; Shen, X. TGF-Β1 Secreted by Hepatocellular Carcinoma Induces the Expression of the Foxp3 Gene and Suppresses Antitumor Immunity in the Tumor Microenvironment. Dig. Dis. Sci. 2013, 58, 1644–1652. [Google Scholar] [CrossRef]
- Cao, M.; Cabrera, R.; Xu, Y.; Firpi, R.; Zhu, H.; Liu, C.; Nelson, D.R. Hepatocellular Carcinoma Cell Supernatants Increase Expansion and Function of CD4+CD25+ Regulatory T Cells. Lab. Investig. 2007, 87, 582–590. [Google Scholar] [CrossRef]
- Yang, Z.-Q.; Yang, Z.-Y.; Zhang, L.-D.; Ping-Bie; Wang, S.-G.; Ma, K.-S.; Li, X.-W.; Dong, J.-H. Increased Liver-Infiltrating CD8+FoxP3+ Regulatory T Cells Are Associated with Tumor Stage in Hepatocellular Carcinoma Patients. Hum. Immunol. 2010, 71, 1180–1186. [Google Scholar] [CrossRef]
- Shen, X.; Li, N.; Li, H.; Zhang, T.; Wang, F.; Li, Q. Increased Prevalence of Regulatory T Cells in the Tumor Microenvironment and Its Correlation with TNM Stage of Hepatocellular Carcinoma. J. Cancer Res. Clin. Oncol. 2010, 136, 1745–1754. [Google Scholar] [CrossRef]
- Budhu, A.; Forgues, M.; Ye, Q.-H.; Jia, H.-L.; He, P.; Zanetti, K.A.; Kammula, U.S.; Chen, Y.; Qin, L.-X.; Tang, Z.-Y.; et al. Prediction of Venous Metastases, Recurrence, and Prognosis in Hepatocellular Carcinoma Based on a Unique Immune Response Signature of the Liver Microenvironment. Cancer Cell 2006, 10, 99–111. [Google Scholar] [CrossRef] [Green Version]
- Nishida, N.; Kudo, M. Immunological Microenvironment of Hepatocellular Carcinoma and Its Clinical Implication. Oncology 2017, 92, 40–49. [Google Scholar] [CrossRef]
- Motomura, T.; Shirabe, K.; Mano, Y.; Muto, J.; Toshima, T.; Umemoto, Y.; Fukuhara, T.; Uchiyama, H.; Ikegami, T.; Yoshizumi, T.; et al. Neutrophil–Lymphocyte Ratio Reflects Hepatocellular Carcinoma Recurrence after Liver Transplantation via Inflammatory Microenvironment. J. Hepatol. 2013, 58, 58–64. [Google Scholar] [CrossRef]
- Ventola, C.L. Cancer Immunotherapy, Part 2: Efficacy, Safety, and Other Clinical Considerations. Pharm. Ther. 2017, 42, 452–463. [Google Scholar] [PubMed]
- Li, L.; Wang, W.; Pan, H.; Ma, G.; Shi, X.; Xie, H.; Liu, X.; Ding, Q.; Zhou, W.; Wang, S. Microwave Ablation Combined with OK-432 Induces Th1-Type Response and Specific Antitumor Immunity in a Murine Model of Breast Cancer. J. Transl. Med. 2017, 15, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, K.W.; Jayant, K.; Lee, P.-H.; Yang, P.; Hsiao, C.-Y.; Habib, N.; Sodergren, M.H. Positive Immuno-Modulation Following Radiofrequency Assisted Liver Resection in Hepatocellular Carcinoma. J. Clin. Med. 2019, 8, 385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikfarjam, M.; Muralidharan, V.; Christophi, C. Mechanisms of Focal Heat Destruction of Liver Tumors. J. Surg. Res. 2005, 127, 208–223. [Google Scholar] [CrossRef]
- Haen, S.P.; Pereira, P.L.; Salih, H.R.; Rammensee, H.-G.; Gouttefangeas, C. More Than Just Tumor Destruction: Immunomodulation by Thermal Ablation of Cancer. Clin. Dev. Immunol. 2011, 2011, 1–19. [Google Scholar] [CrossRef]
- Dromi, S.A.; Walsh, M.P.; Herby, S.; Traughber, B.; Xie, J.; Sharma, K.V.; Sekhar, K.P.; Luk, A.; Liewehr, D.J.; Dreher, M.R.; et al. Radiofrequency Ablation Induces Antigen-Presenting Cell Infiltration and Amplification of Weak Tumor-Induced Immunity. Radiology 2009, 251, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Zerbini, A.; Pilli, M.; Laccabue, D.; Pelosi, G.; Molinari, A.; Negri, E.; Cerioni, S.; Fagnoni, F.; Soliani, P.; Ferrari, C.; et al. Radiofrequency Thermal Ablation for Hepatocellular Carcinoma Stimulates Autologous NK-Cell Response. Gastroenterology 2010, 138, 1931–1942. [Google Scholar] [CrossRef]
- Dong, B.; Zhang, J.; Liang, P.; Yu, X.; Su, L.; Yu, D.; Ji, X.; Yu, G.; Yin, Z. Influencing Factors of Local Immunocyte Infiltration in Hepatocellular Carcinoma Tissues Pre- and Post-Percutaneous Microwave Coagulation Therapy. Zhonghua Yi Xue Za Zhi 2002, 82, 393–397. [Google Scholar]
- Kuang, M.; Liu, S.Q.; Saijo, K.; Uchimura, E.; Huang, L.; Leong, K.W.; Lu, M.D.; Huang, J.F.; Ohno, T. Microwave Tumour Coagulation plus in Situ Treatment with Cytokine-Microparticles: Induction of Potent Anti-Residual Tumour Immunity. Int. J. Hyperth. 2005, 21, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Kroemer, G.; Galluzzi, L.; Kepp, O.; Zitvogel, L. Immunogenic Cell Death in Cancer Therapy. Annu. Rev. Immunol. 2013, 31, 51–72. [Google Scholar] [CrossRef]
- Sabel, M.S. Cryo-Immunology: A Review of the Literature and Proposed Mechanisms for Stimulatory versus Suppressive Immune Responses. Cryobiology 2009, 58, 1–11. [Google Scholar] [CrossRef]
- Basu, S.; Binder, R.J.; Suto, R.; Anderson, K.M.; Srivastava, P.K. Necrotic but Not Apoptotic Cell Death Releases Heat Shock Proteins, Which Deliver a Partial Maturation Signal to Dendritic Cells and Activate the NF-ΚB Pathway. Int. Immunol. 2000, 12, 1539–1546. [Google Scholar] [CrossRef] [PubMed]
- Bottero, V.; Withoff, S.; Verma, I.M. NF-ΚB and the Regulation of Hematopoiesis. Cell Death Differ. 2006, 13, 785–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, K.F.; Dupuy, D.E. Thermal Ablation of Tumours: Biological Mechanisms and Advances in Therapy. Nat. Rev. Cancer 2014, 14, 199–208. [Google Scholar] [CrossRef]
- den Brok, M.H.M.G.M.; Sutmuller, R.P.M.; Nierkens, S.; Bennink, E.J.; Frielink, C.; Toonen, L.W.J.; Boerman, O.C.; Figdor, C.G.; Ruers, T.J.M.; Adema, G.J. Efficient Loading of Dendritic Cells Following Cryo and Radiofrequency Ablation in Combination with Immune Modulation Induces Anti-Tumour Immunity. Br. J. Cancer 2006, 95, 896–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, T.A.; Choi, J.; Green, D.R. Armed Response: How Dying Cells Influence T-Cell Functions. Immunol. Rev. 2011, 241, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.; Dai, T. Radiation Therapy and the Abscopal Effect: A Concept Comes of Age. Ann. Transl. Med. 2016, 4, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.; Kumar, G.; Moussa, M.; Wang, Y.; Rozenblum, N.; Galun, E.; Goldberg, S.N. Hepatic Radiofrequency Ablation–Induced Stimulation of Distant Tumor Growth Is Suppressed by c-Met Inhibition. Radiology 2016, 279, 103–117. [Google Scholar] [CrossRef] [Green Version]
- Rozenblum, N.; Zeira, E.; Scaiewicz, V.; Bulvik, B.; Gourevitch, S.; Yotvat, H.; Galun, E.; Goldberg, S.N. Oncogenesis: An “Off-Target” Effect of Radiofrequency Ablation. Radiology 2015, 276, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Tanis, E.; Nordlinger, B.; Mauer, M.; Sorbye, H.; van Coevorden, F.; Gruenberger, T.; Schlag, P.M.; Punt, C.J.A.; Ledermann, J.; Ruers, T.J.M. Local Recurrence Rates after Radiofrequency Ablation or Resection of Colorectal Liver Metastases. Analysis of the European Organisation for Research and Treatment of Cancer #40004 and #40983. Eur. J. Cancer 2014, 50, 912–919. [Google Scholar] [CrossRef]
- Erinjeri, J.P.; Thomas, C.T.; Samoilia, A.; Fleisher, M.; Gonen, M.; Sofocleous, C.T.; Thornton, R.H.; Siegelbaum, R.H.; Covey, A.M.; Brody, L.A.; et al. Image-Guided Thermal Ablation of Tumors Increases the Plasma Level of Interleukin-6 and Interleukin-10. J. Vasc. Interv. Radiol. 2013, 24, 1105–1112. [Google Scholar] [CrossRef] [Green Version]
- Hinz, S.; Tepel, J.; Röder, C.; Kalthoff, H.; Becker, T. Profile of Serum Factors and Disseminated Tumor Cells before and after Radiofrequency Ablation Compared to Resection of Colorectal Liver Metastases—A Pilot Study. Anticancer Res. 2015, 35, 2961–2967. [Google Scholar] [PubMed]
- Gou, X.; Tang, X.; Kong, D.K.; He, X.; Gao, X.; Guo, N.; Hu, Z.; Zhao, Z.; Chen, Y. CD147 Is Increased in HCC Cells under Starvation and Reduces Cell Death through Upregulating P-MTOR in Vitro. Apoptosis 2016, 21, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.; Wu, C.-Y.; Kuo, C.-Y.; Wang, J.P.; Luo, J.-C.; Kao, C.-H.; Lee, R.-C.; Lee, W.-P.; Li, C.-P. Cytokines Are Associated with Postembolization Fever and Survival in Hepatocellular Carcinoma Patients Receiving Transcatheter Arterial Chemoembolization. Hepatol. Int. 2013, 7, 883–892. [Google Scholar] [CrossRef]
- He, X.; Guo, X.; Zhang, H.; Kong, X.; Yang, F.; Zheng, C. Mechanism of Action and Efficacy of LY2109761, a TGF-β Receptor Inhibitor, Targeting Tumor Microenvironment in Liver Cancer after TACE. Oncotarget 2018, 9, 1130–1142. [Google Scholar] [CrossRef]
- Zhao, Z.-W.; Fan, X.-X.; Song, J.-J.; Xu, M.; Chen, M.-J.; Tu, J.-F.; Wu, F.-Z.; Zhang, D.-K.; Liu, L.; Chen, L.; et al. ShRNA Knock-down of CXCR7 Inhibits Tumour Invasion and Metastasis in Hepatocellular Carcinoma after Transcatheter Arterial Chemoembolization. J. Cell. Mol. Med. 2017, 21, 1989–1999. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.; Kumar, G.; Navarro, G.; Wang, Y.; Gourevitch, S.; Moussa, M.H.; Rozenblum, N.; Levchenko, T.; Galun, E.; Torchilin, V.P.; et al. Systemic SiRNA Nanoparticle-Based Drugs Combined with Radiofrequency Ablation for Cancer Therapy. PLoS ONE 2015, 10, e0128910. [Google Scholar] [CrossRef]
- Nikfarjam, M.; Muralidharan, V.; Christophi, C. Altered Growth Patterns of Colorectal Liver Metastases after Thermal Ablation. Surgery 2006, 139, 73–81. [Google Scholar] [CrossRef]
- Nijkamp, M.W.; van der Bilt, J.D.W.; de Bruijn, M.T.; Molenaar, I.Q.; Voest, E.E.; van Diest, P.J.; Kranenburg, O.; Borel Rinkes, I.H.M. Accelerated Perinecrotic Outgrowth of Colorectal Liver Metastases Following Radiofrequency Ablation Is a Hypoxia-Driven Phenomenon. Ann. Surg. 2009, 249, 814–823. [Google Scholar] [CrossRef]
- Kang, T.W.; Kim, J.M.; Rhim, H.; Lee, M.W.; Kim, Y.; Lim, H.K.; Choi, D.; Song, K.D.; Kwon, C.H.D.; Joh, J.-W.; et al. Small Hepatocellular Carcinoma: Radiofrequency Ablation versus Nonanatomic Resection—Propensity Score Analyses of Long-Term Outcomes. Radiology 2015, 275, 908–919. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Wang, J.; Ding, N.; Zhang, Y.; Zhu, Y.; Dong, S.; Wang, X.; Peng, C.; Zhou, C.; Zhou, L.; et al. Inflammation Induced by Incomplete Radiofrequency Ablation Accelerates Tumor Progression and Hinders PD-1 Immunotherapy. Nat. Commun. 2019, 10, 5421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruzzenente, A.; de Manzoni, G.; Molfetta, M.; Pachera, S.; Genco, B.; Donataccio, M.; Guglielmi, A. Rapid Progression of Hepatocellular Carcinoma after Radiofrequency Ablation. World J. Gastroenterol. 2004, 10, 1137. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Wu, J.; Liu, X.; Liang, M.; Zhou, X.; Ouyang, S.; Yao, J.; Wang, J.; Luo, B. Insufficient Radiofrequency Ablation Promotes Proliferation of Residual Hepatocellular Carcinoma via Autophagy. Cancer Lett. 2018, 421, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular Carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Chen, L.; Sun, J.; Yang, X. Radiofrequency Ablation-Combined Multimodel Therapies for Hepatocellular Carcinoma: Current Status. Cancer Lett. 2016, 370, 78–84. [Google Scholar] [CrossRef] [Green Version]
- Yan, K.; Chen, M.H.; Yang, W.; Wang, Y.B.; Gao, W.; Hao, C.Y.; Xing, B.C.; Huang, X.F. Radiofrequency Ablation of Hepatocellular Carcinoma: Long-Term Outcome and Prognostic Factors. Eur. J. Radiol. 2008, 67, 336–347. [Google Scholar] [CrossRef]
- Izzo, F.; Granata, V.; Grassi, R.; Fusco, R.; Palaia, R.; Delrio, P.; Carrafiello, G.; Azoulay, D.; Petrillo, A.; Curley, S.A. Radiofrequency Ablation and Microwave Ablation in Liver Tumors: An Update. Oncologist 2019, 24, e990–e1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haen, S.P.; Gouttefangeas, C.; Schmidt, D.; Boss, A.; Clasen, S.; von Herbay, A.; Kosan, B.; Aebert, H.; Pereira, P.L.; Rammensee, H.-G. Elevated Serum Levels of Heat Shock Protein 70 Can Be Detected after Radiofrequency Ablation. Cell Stress Chaperones 2011, 16, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Slovak, R.; Ludwig, J.M.; Gettinger, S.N.; Herbst, R.S.; Kim, H.S. Immuno-Thermal Ablations—Boosting the Anticancer Immune Response. J. Immunother. Cancer 2017, 5, 78. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, F.; Gravante, G.; Bhardwaj, N.; Strickland, A.; Basit, R.; West, K.; Sorge, R.; Dennison, A.R.; Lloyd, D.M. Changes in Interleukin-1β and 6 after Hepatic Microwave Tissue Ablation Compared with Radiofrequency, Cryotherapy and Surgical Resections. Am. J. Surg. 2010, 200, 500–506. [Google Scholar] [CrossRef]
- Ali, M.Y.; Grimm, C.F.; Ritter, M.; Mohr, L.; Allgaier, H.-P.; Weth, R.; Bocher, W.O.; Endrulat, K.; Blum, H.E.; Geissler, M. Activation of Dendritic Cells by Local Ablation of Hepatocellular Carcinoma. J. Hepatol. 2005, 43, 817–822. [Google Scholar] [CrossRef]
- Fietta, A.M.; Morosini, M.; Passadore, I.; Cascina, A.; Draghi, P.; Dore, R.; Rossi, S.; Pozzi, E.; Meloni, F. Systemic Inflammatory Response and Downmodulation of Peripheral CD25+Foxp3+ T-Regulatory Cells in Patients Undergoing Radiofrequency Thermal Ablation for Lung Cancer. Hum. Immunol. 2009, 70, 477–486. [Google Scholar] [CrossRef]
- Mizukoshi, E.; Yamashita, T.; Arai, K.; Sunagozaka, H.; Ueda, T.; Arihara, F.; Kagaya, T.; Yamashita, T.; Fushimi, K.; Kaneko, S. Enhancement of Tumor-Associated Antigen-Specific T Cell Responses by Radiofrequency Ablation of Hepatocellular Carcinoma. Hepatology 2013, 57, 1448–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochigneux, P.; Nault, J.-C.; Mallet, F.; Chretien, A.-S.; Barget, N.; Garcia, A.J.; Del Pozo, L.; Bourcier, V.; Blaise, L.; Grando-Lemaire, V.; et al. Dynamic of Systemic Immunity and Its Impact on Tumor Recurrence after Radiofrequency Ablation of Hepatocellular Carcinoma. Oncoimmunology 2019, 8, 1615818. [Google Scholar] [CrossRef] [Green Version]
- Hiroishi, K.; Eguchi, J.; Baba, T.; Shimazaki, T.; Ishii, S.; Hiraide, A.; Sakaki, M.; Doi, H.; Uozumi, S.; Omori, R.; et al. Strong CD8+ T-Cell Responses against Tumor-Associated Antigens Prolong the Recurrence-Free Interval after Tumor Treatment in Patients with Hepatocellular Carcinoma. J. Gastroenterol. 2010, 45, 451–458. [Google Scholar] [CrossRef]
- Wissniowski, T.T.; Hänsler, J.; Neureiter, D.; Frieser, M.; Schaber, S.; Esslinger, B.; Voll, R.; Strobel, D.; Hahn, E.G.; Schuppan, D.; et al. Activation of Tumor-Specific T Lymphocytes by Radio-Frequency Ablation of the VX2 Hepatoma in Rabbits. Cancer Res. 2003, 63, 6496–6500. [Google Scholar] [PubMed]
- Hu, G.; Wang, S. Tumor-Infiltrating CD45RO+ Memory T Lymphocytes Predict Favorable Clinical Outcome in Solid Tumors. Sci. Rep. 2017, 7, 10376. [Google Scholar] [CrossRef] [Green Version]
- Widenmeyer, M.; Shebzukhov, Y.; Haen, S.P.; Schmidt, D.; Clasen, S.; Boss, A.; Kuprash, D.V.; Nedospasov, S.A.; Stenzl, A.; Aebert, H.; et al. Analysis of Tumor Antigen-Specific T Cells and Antibodies in Cancer Patients Treated with Radiofrequency Ablation. Int. J. Cancer 2011, 128, 2653–2662. [Google Scholar] [CrossRef]
- Lencioni, R.; Cioni, D.; Crocetti, L.; Franchini, C.; Pina, C.D.; Lera, J.; Bartolozzi, C. Early-Stage Hepatocellular Carcinoma in Patients with Cirrhosis: Long-Term Results of Percutaneous Image-Guided Radiofrequency Ablation. Radiology 2005, 234, 961–967. [Google Scholar] [CrossRef]
- Nijkamp, M.W.; Borren, A.; Govaert, K.M.; Hoogwater, F.J.H.; Molenaar, I.Q.; van Diest, P.J.; Kranenburg, O.; Rinkes, I.H.M.B. Radiofrequency Ablation of Colorectal Liver Metastases Induces an Inflammatory Response in Distant Hepatic Metastases but Not in Local Accelerated Outgrowth. J. Surg. Oncol. 2010, 101, 551–556. [Google Scholar] [CrossRef]
- Kong, J.; Kong, J.; Pan, B.; Ke, S.; Dong, S.; Li, X.; Zhou, A.; Zheng, L.; Sun, W. Insufficient Radiofrequency Ablation Promotes Angiogenesis of Residual Hepatocellular Carcinoma via HIF-1α/VEGFA. PLoS ONE 2012, 7, e37266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, Q.; Gu, J.; Zhang, H.; Ren, W.; Ji, W.; Fan, Y. Correlation between Vascular Endothelial Growth Factor Levels and Prognosis of Hepatocellular Carcinoma Patients Receiving Radiofrequency Ablation. Biotechnol. Biotechnol. Equip. 2015, 29, 119–123. [Google Scholar] [CrossRef]
- Cazzato, R.L.; Garnon, J.; Ramamurthy, N.; Koch, G.; Tsoumakidou, G.; Caudrelier, J.; Arrigoni, F.; Zugaro, L.; Barile, A.; Masciocchi, C.; et al. Percutaneous Image-Guided Cryoablation: Current Applications and Results in the Oncologic Field. Med. Oncol. 2016, 33, 140. [Google Scholar] [CrossRef] [PubMed]
- Baust, J.G.; Gage, A.A. Progress toward Optimization of Cryosurgery. Technol. Cancer Res. Treat. 2004, 3, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Yamakado, K. Image-Guided Ablation of Adrenal Lesions. Semin. Intervent. Radiol. 2014, 31, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Weber, S.M.; Lee, F.T. Expanded Treatment of Hepatic Tumors with Radiofrequency Ablation and Cryoablation. Oncology (Williston Park) 2005, 19 (Suppl. 4), 27–32. [Google Scholar]
- Allaf, M.E.; Varkarakis, I.M.; Bhayani, S.B.; Inagaki, T.; Kavoussi, L.R.; Solomon, S.B. Pain Control Requirements for Percutaneous Ablation of Renal Tumors: Cryoablation versus Radiofrequency Ablation—Initial Observations. Radiology 2005, 237, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Yakkala, C.; Denys, A.; Kandalaft, L.; Duran, R. Cryoablation and Immunotherapy of Cancer. Curr. Opin. Biotechnol. 2020, 65, 60–64. [Google Scholar] [CrossRef]
- Mehta, A.; Oklu, R.; Sheth, R.A. Thermal Ablative Therapies and Immune Checkpoint Modulation: Can Locoregional Approaches Effect a Systemic Response? Gastroenterol. Res. Pract. 2016, 2016, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Sabel, M.S.; Su, G.; Griffith, K.A.; Chang, A.E. Rate of Freeze Alters the Immunologic Response After Cryoablation of Breast Cancer. Ann. Surg. Oncol. 2010, 17, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Urano, M.; Tanaka, C.; Sugiyama, Y.; Miya, K.; Saji, S. Antitumor Effects of Residual Tumor after Cryoablation: The Combined Effect of Residual Tumor and a Protein-Bound Polysaccharide on Multiple Liver Metastases in a Murine Model. Cryobiology 2003, 46, 238–245. [Google Scholar] [CrossRef]
- Takaki, H.; Imai, N.; Thomas, C.T.; Yamakado, K.; Yarmohammadi, H.; Ziv, E.; Srimathveeravalli, G.; Sofocleous, C.T.; Solomon, S.B.; Erinjeri, J.P. Changes in Peripheral Blood T-Cell Balance after Percutaneous Tumor Ablation. Minim. Invasive Ther. Allied Technol. 2017, 26, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, M.; Patella, F.; Pesapane, F.; Suter, M.B.; Ierardi, A.M.; Angileri, S.A.; Floridi, C.; de Filippo, M.; Carrafiello, G. Hypoxia and Tumor Angiogenesis in the Era of Hepatocellular Carcinoma Transarterial Loco-Regional Treatments. Futur. Oncol. 2018, 14, 2957–2967. [Google Scholar] [CrossRef]
- Zeng, Z.; Shi, F.; Zhou, L.; Zhang, M.-N.; Chen, Y.; Chang, X.-J.; Lu, Y.-Y.; Bai, W.-L.; Qu, J.-H.; Wang, C.-P.; et al. Upregulation of Circulating PD-L1/PD-1 Is Associated with Poor Post-Cryoablation Prognosis in Patients with HBV-Related Hepatocellular Carcinoma. PLoS ONE 2011, 6, e23621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waitz, R.; Solomon, S.B.; Petre, E.N.; Trumble, A.E.; Fassò, M.; Norton, L.; Allison, J.P. Potent Induction of Tumor Immunity by Combining Tumor Cryoablation with Anti–CTLA-4 Therapy. Cancer Res. 2012, 72, 430–439. [Google Scholar] [CrossRef] [Green Version]
- Niu, L.-Z. Combination Treatment with Comprehensive Cryoablation and Immunotherapy in Metastatic Hepatocellular Cancer. World J. Gastroenterol. 2013, 19, 3473. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Liang, S.; Wang, X.; Liang, Y.; Zhang, M.; Chen, J.; Niu, L.; Xu, K. Cryoablation Combined with Allogenic Natural Killer Cell Immunotherapy Improves the Curative Effect in Patients with Advanced Hepatocellular Cancer. Oncotarget 2017, 8, 81967–81977. [Google Scholar] [CrossRef] [Green Version]
- Ma, C.-H.; Jiang, R.; Li, J.-D.; Wang, B.; Sun, L.-W.; Lv, Y. Experimental Study on Residual Tumor Angiogenesis after Cryoablation. Asian Pac. J. Cancer Prev. 2014, 15, 2491–2494. [Google Scholar] [CrossRef] [Green Version]
- Biondetti, P.; Fumarola, E.M.; Ierardi, A.M.; Coppola, A.; Gorga, G.; Maggi, L.; Valconi, E.; Angileri, S.A.; Carrafiello, G. Percutaneous US-Guided MWA of Small Liver HCC: Predictors of Outcome and Risk Factors for Complications from a Single Center Experience. Med. Oncol. 2020, 37, 39. [Google Scholar] [CrossRef] [PubMed]
- Simon, C.J.; Dupuy, D.E.; Mayo-Smith, W.W. Microwave Ablation: Principles and Applications. RadioGraphics 2005, 25 (Suppl. 1), S69–S83. [Google Scholar] [CrossRef]
- Ethier, M.D.; Beland, M.D.; Mayo-Smith, W. Image-Guided Ablation of Adrenal Tumors. Tech. Vasc. Interv. Radiol. 2013, 16, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Venkatesan, A.M.; Locklin, J.; Dupuy, D.E.; Wood, B.J. Percutaneous Ablation of Adrenal Tumors. Tech. Vasc. Interv. Radiol. 2010, 13, 89–99. [Google Scholar] [CrossRef] [Green Version]
- Skinner, M.G.; Iizuka, M.N.; Kolios, M.C.; Sherar, M.D. A Theoretical Comparison of Energy Sources—Microwave, Ultrasound and Laser—For Interstitial Thermal Therapy. Phys. Med. Biol. 1998, 43, 3535–3547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stauffer, P.R.; Rossetto, F.; Prakash, M.; Neuman, D.G.; Lee, T. Phantom and Animal Tissues for Modelling the Electrical Properties of Human Liver. Int. J. Hyperth. 2003, 19, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Wright, A.S.; Lee, F.T.; Mahvi, D.M. Hepatic Microwave Ablation With Multiple Antennae Results in Synergistically Larger Zones of Coagulation Necrosis. Ann. Surg. Oncol. 2003, 10, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Shock, S.A.; Meredith, K.; Warner, T.F.; Sampson, L.A.; Wright, A.S.; Winter, T.C.; Mahvi, D.M.; Fine, J.P.; Lee, F.T. Microwave Ablation with Loop Antenna: In Vivo Porcine Liver Model. Radiology 2004, 231, 143–149. [Google Scholar] [CrossRef]
- Patella, F.; Pesapane, F.; Fumarola, E.; Zannoni, S.; Brambillasca, P.; Emili, I.; Costa, G.; Anderson, V.; Levy, E.B.; Carrafiello, G.; et al. Assessment of the Response of Hepatocellular Carcinoma to Interventional Radiology Treatments. Futur. Oncol. 2019, 15, 1791–1804. [Google Scholar] [CrossRef] [PubMed]
- Dong, B.W.; Zhang, J.; Liang, P.; Yu, X.L.; Su, L.; Yu, D.J.; Ji, X.L.; Yu, G. Sequential Pathological and Immunologic Analysis of Percutaneous Microwave Coagulation Therapy of Hepatocellular Carcinoma. Int. J. Hyperth. 2003, 19, 119–133. [Google Scholar] [CrossRef]
- Zhou, P.; Liang, P.; Dong, B.; Yu, X.; Han, Z.; Xu, Y. Phase I Clinical Study of Combination Therapy with Microwave Ablation and Cellular Immunotherapy in Hepatocellular Carcinoma. Cancer Biol. Ther. 2011, 11, 450–456. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Hou, X.; Cai, H.; Zhuang, X. Effects of Microwave Ablation on T-Cell Subsets and Cytokines of Patients with Hepatocellular Carcinoma. Minim. Invasive Ther. Allied Technol. 2017, 26, 207–211. [Google Scholar] [CrossRef]
- Ni, Y.; Ye, X.; Wan, C.; Ni, Q.; Yang, X.; Huang, G.; Li, W.; Wang, J.; Han, X.; Wei, Z.; et al. Percutaneous Microwave Ablation (MWA) Increased the Serum Levels of VEGF and MMP-9 in Stage I Non-Small Cell Lung Cancer (NSCLC). Int. J. Hyperth. 2017, 33, 435–439. [Google Scholar] [CrossRef]
- Sun, Y.H.; Song, P.Y.; Guo, Y.; Pang, M.; He, W.-N.; Zhang, W.H.; Sheng, L.J. Effects of Microwave Ablation or Its Combination with Whole-Body Chemotherapy on Serum Vascular Endothelial Growth Factor Levels in Patients with Stage IIIB/IV NSCLC. Genet. Mol. Res. 2015, 14, 10015–10025. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A. Transarterial Chemoembolization: Evidences from the Literature and Applications in Hepatocellular Carcinoma Patients. World J. Hepatol. 2015, 7, 2009. [Google Scholar] [CrossRef] [PubMed]
- Greten, T.F.; Mauda-Havakuk, M.; Heinrich, B.; Korangy, F.; Wood, B.J. Combined Locoregional-Immunotherapy for Liver Cancer. J. Hepatol. 2019, 70, 999–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohles, N.; Nagel, D.; Jüngst, D.; Stieber, P.; Holdenrieder, S. Predictive Value of Immunogenic Cell Death Biomarkers HMGB1, SRAGE, and DNase in Liver Cancer Patients Receiving Transarterial Chemoembolization Therapy. Tumor Biol. 2012, 33, 2401–2409. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Jung, J.H.; Jung, M.K.; Shin, E.-C.; Ro, S.W.; Park, J.H.; Kim, D.Y.; Park, J.Y.; Han, K.-H. Effects of Transarterial Chemoembolization on Regulatory T Cell and Its Subpopulations in Patients with Hepatocellular Carcinoma. Hepatol. Int. 2020, 14, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Jang, J.W.; Oh, B.S.; Kwon, J.H.; Chung, K.W.; Jung, H.S.; Jekarl, D.W.; Lee, S. Change in Inflammatory Cytokine Profiles after Transarterial Chemotherapy in Patients with Hepatocellular Carcinoma. Cytokine 2013, 64, 516–522. [Google Scholar] [CrossRef]
- Huang, M.; Wang, X.; Bin, H. Effect of Transcatheter Arterial Chemoembolization Combined with Argon–Helium Cryosurgery System on the Changes of NK Cells and T Cell Subsets in Peripheral Blood of Hepatocellular Carcinoma Patients. Cell Biochem. Biophys. 2015, 73, 787–792. [Google Scholar] [CrossRef]
- Kimura, H.; Braun, R.D.; Ong, E.T.; Hsu, R.; Secomb, T.W.; Papahadjopoulos, D.; Hong, K.; Dewhirst, M.W. Fluctuations in Red Cell Flux in Tumor Microvessels Can Lead to Transient Hypoxia and Reoxygenation in Tumor Parenchyma. Cancer Res. 1996, 56, 5522–5528. [Google Scholar]
- Namur, J.; Pascale, F.; Maeda, N.; Sterba, M.; Ghegediban, S.H.; Verret, V.; Paci, A.; Seck, A.; Osuga, K.; Wassef, M.; et al. Safety and Efficacy Compared between Irinotecan-Loaded Microspheres HepaSphere and DC Bead in a Model of VX2 Liver Metastases in the Rabbit. J. Vasc. Interv. Radiol. 2015, 26, 1067–1075. [Google Scholar] [CrossRef]
- Tong, A.K.T.; Kao, Y.H.; Too, C.W.; Chin, K.F.W.; Ng, D.C.E.; Chow, P.K.H. Yttrium-90 Hepatic Radioembolization: Clinical Review and Current Techniques in Interventional Radiology and Personalized Dosimetry. Br. J. Radiol. 2016, 89, 20150943. [Google Scholar] [CrossRef] [PubMed]
- Cardarelli-Leite, L.; Hadjivassiliou, A.; Klass, D.; Chung, J.; Ho, S.G.F.; Lim, H.J.; Kim, P.T.W.; Mujoomdar, A.; Liu, D.M. Current Locoregional Therapies and Treatment Strategies in Hepatocellular Carcinoma. Curr. Oncol. 2020, 27, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Chung, H.W.; Jo, J.-H.; So, Y. Radioembolization for the Treatment of Primary and Metastatic Liver Cancers. Nucl. Med. Mol. Imaging (2010) 2019, 53, 367–373. [Google Scholar] [CrossRef]
- Chew, V.; Lee, Y.H.; Pan, L.; Nasir, N.J.M.; Lim, C.J.; Chua, C.; Lai, L.; Hazirah, S.N.; Lim, T.K.H.; Goh, B.K.P.; et al. Immune Activation Underlies a Sustained Clinical Response to Yttrium-90 Radioembolisation in Hepatocellular Carcinoma. Gut 2019, 68, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Domouchtsidou, A.; Barsegian, V.; Mueller, S.P.; Best, J.; Ertle, J.; Bedreli, S.; Horn, P.A.; Bockisch, A.; Lindemann, M. Impaired Lymphocyte Function in Patients with Hepatic Malignancies after Selective Internal Radiotherapy. Cancer Immunol. Immunother. 2018, 67, 843–853. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Ros, N.; Iñarrairaegui, M.; Paramo, J.A.; Berasain, C.; Avila, M.A.; Chopitea, A.; Varo, N.; Sarobe, P.; Bilbao, J.I.; Dominguez, I.; et al. Radioembolization of Hepatocellular Carcinoma Activates Liver Regeneration, Induces Inflammation and Endothelial Stress and Activates Coagulation. Liver Int. 2015, 35, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Seidensticker, M.; Powerski, M.; Seidensticker, R.; Damm, R.; Mohnike, K.; Garlipp, B.; Klopffleisch, M.; Amthauer, H.; Ricke, J.; Pech, M. Cytokines and 90Y-Radioembolization: Relation to Liver Function and Overall Survival. Cardiovasc. Intervent. Radiol. 2017, 40, 1185–1195. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, Y.; Ji, H.; Zhao, X.; Lu, H. Transarterial Y90 Radioembolization versus Chemoembolization for Patients with Hepatocellular Carcinoma: A Meta-Analysis. Biosci. Trends 2015, 9, 289–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, H.-P.; Gong, J.-P.; Zuo, G.-Q. Role of High-Intensity Focused Ultrasound in Treatment of Hepatocellular Carcinoma. Am. Surg. 2011, 77, 1496–1501. [Google Scholar] [CrossRef]
- Hoogenboom, M.; Eikelenboom, D.; den Brok, M.H.; Veltien, A.; Wassink, M.; Wesseling, P.; Dumont, E.; Fütterer, J.J.; Adema, G.J.; Heerschap, A. In Vivo MR Guided Boiling Histotripsy in a Mouse Tumor Model Evaluated by MRI and Histopathology. NMR Biomed. 2016, 29, 721–731. [Google Scholar] [CrossRef] [PubMed]
- She, W.; Cheung, T.; Jenkins, C.R.; Irwin, M.G. Clinical Applications of High-Intensity Focused Ultrasound. Hong Kong Med. J. 2016, 22, 382–392. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Zhu, J.; Zhu, L.; Zhu, Y.; Zhao, H. High-Intensity Focused Ultrasound Ablation for Unresectable Primary and Metastatic Liver Cancer: Real-World Research in a Chinese Tertiary Center with 275 Cases. Front. Oncol. 2020, 10, 519164. [Google Scholar] [CrossRef] [PubMed]
- Kramer, G.; Steiner, G.E.; Gröbl, M.; Hrachowitz, K.; Reithmayr, F.; Paucz, L.; Newman, M.; Madersbacher, S.; Gruber, D.; Susani, M.; et al. Response to Sublethal Heat Treatment of Prostatic Tumor Cells and of Prostatic Tumor Infiltrating T-Cells. Prostate 2004, 58, 109–120. [Google Scholar] [CrossRef]
- Wu, F.; Wang, Z.-B.; Lu, P.; Xu, Z.-L.; Chen, W.-Z.; Zhu, H.; Jin, C.-B. Activated Anti-Tumor Immunity in Cancer Patients after High Intensity Focused Ultrasound Ablation. Ultrasound Med. Biol. 2004, 30, 1217–1222. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Zhu, X.-Q.; Zhang, J.; Xu, Z.-L.; Lu, P.; Wu, F. Changes in Circulating Immunosuppressive Cytokine Levels of Cancer Patients After High Intensity Focused Ultrasound Treatment. Ultrasound Med. Biol. 2008, 34, 81–87. [Google Scholar] [CrossRef]
- Ma, B.; Liu, X.; Yu, Z. The Effect of High Intensity Focused Ultrasound on the Treatment of Liver Cancer and Patients’ Immunity. Cancer Biomarkers 2019, 24, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Vlaisavljevich, E.; Greve, J.; Cheng, X.; Ives, K.; Shi, J.; Jin, L.; Arvidson, A.; Hall, T.; Welling, T.H.; Owens, G.; et al. Non-Invasive Ultrasound Liver Ablation Using Histotripsy: Chronic Study in an In Vivo Rodent Model. Ultrasound Med. Biol. 2016, 42, 1890–1902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maxwell, A.D.; Wang, T.-Y.; Cain, C.A.; Fowlkes, J.B.; Sapozhnikov, O.A.; Bailey, M.R.; Xu, Z. Cavitation Clouds Created by Shock Scattering from Bubbles during Histotripsy. J. Acoust. Soc. Am. 2011, 130, 1888–1898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, G.; Cui, J.; Qin, Q.; Zhang, J.; Liu, L.; Deng, S.; Wu, C.; Yang, M.; Li, S.; Wang, C. Mechanical Stiffness of Liver Tissues in Relation to Integrin Β1 Expression May Influence the Development of Hepatic Cirrhosis and Hepatocellular Carcinoma. J. Surg. Oncol. 2010, 102, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Qu, S.; Worlikar, T.; Felsted, A.E.; Ganguly, A.; Beems, M.V.; Hubbard, R.; Pepple, A.L.; Kevelin, A.A.; Garavaglia, H.; Dib, J.; et al. Non-Thermal Histotripsy Tumor Ablation Promotes Abscopal Immune Responses That Enhance Cancer Immunotherapy. J. Immunother. Cancer 2020, 8, e000200. [Google Scholar] [CrossRef] [Green Version]
- Di Costanzo, G.G.; Francica, G.; Pacella, C.M. Laser Ablation for Small Hepatocellular Carcinoma: State of the Art and Future Perspectives. World J. Hepatol. 2014, 6, 704. [Google Scholar] [CrossRef]
- Sartori, S.; Tombesi, P.; Di Vece, F. Radiofrequency, Microwave, and Laser Ablation of Liver Tumors: Time to Move toward a Tailored Ablation Technique? Hepatoma Res. 2015, 1, 52. [Google Scholar] [CrossRef] [Green Version]
- Cook, A.M.; Lesterhuis, W.J.; Nowak, A.K.; Lake, R.A. Chemotherapy and Immunotherapy: Mapping the Road Ahead. Curr. Opin. Immunol. 2016, 39, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Pacella, C.M.; Bizzarri, G.; Magnolfi, F.; Cecconi, P.; Caspani, B.; Anelli, V.; Bianchini, A.; Valle, D.; Pacella, S.; Manenti, G.; et al. Laser Thermal Ablation in the Treatment of Small Hepatocellular Carcinoma: Results in 74 Patients. Radiology 2001, 221, 712–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacella, C.M.; Francica, G.; Di Lascio, F.M.L.; Arienti, V.; Antico, E.; Caspani, B.; Magnolfi, F.; Megna, A.S.; Pretolani, S.; Regine, R.; et al. Long-Term Outcome of Cirrhotic Patients With Early Hepatocellular Carcinoma Treated With Ultrasound-Guided Percutaneous Laser Ablation: A Retrospective Analysis. J. Clin. Oncol. 2009, 27, 2615–2621. [Google Scholar] [CrossRef]
- Di Costanzo, G.G.; D’Adamo, G.; Tortora, R.; Zanfardino, F.; Mattera, S.; Francica, G.; Pacella, C.M. A Novel Needle Guide System to Perform Percutaneous Laser Ablation of Liver Tumors Using the Multifiber Technique. Acta Radiol. 2013, 54, 876–881. [Google Scholar] [CrossRef] [PubMed]
- Eichler, K.; Zangos, S.; Gruber-Rouh, T.; Vogl, T.J.; Mack, M.G. Magnetic Resonance-Guided Laser-Induced Thermotherapy in Patients with Oligonodular Hepatocellular Carcinoma. J. Clin. Gastroenterol. 2012, 46, 796–801. [Google Scholar] [CrossRef]
- Ferrari, F.S.; Megliola, A.; Scorzelli, A.; Stella, A.; Vigni, F.; Drudi, F.M.; Venezia, D. Treatment of Small HCC through Radiofrequency Ablation and Laser Ablation. Comparison of Techniques and Long-Term Results. Radiol. Med. 2007, 112, 377–393. [Google Scholar] [CrossRef]
- Di Costanzo, G.G.; Tortora, R.; D’Adamo, G.; De Luca, M.; Lampasi, F.; Addario, L.; Galeota Lanza, A.; Picciotto, F.P.; Tartaglione, M.T.; Cordone, G.; et al. Radiofrequency Ablation versus Laser Ablation for the Treatment of Small Hepatocellular Carcinoma in Cirrhosis: A Randomized Trial. J. Gastroenterol. Hepatol. 2015, 30, 559–565. [Google Scholar] [CrossRef]
- Ivarsson, K.; Myllymäki, L.; Jansner, K.; Stenram, U.; Tranberg, K.-G. Resistance to Tumour Challenge after Tumour Laser Thermotherapy Is Associated with a Cellular Immune Response. Br. J. Cancer 2005, 93, 435–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikfarjam, M.; Muralidharan, V.; Su, K.; Malcontenti-Wilson, C.; Christophi, C. Patterns of Heat Shock Protein (HSP70) Expression and Kupffer Cell Activity Following Thermal Ablation of Liver and Colorectal Liver Metastases. Int. J. Hyperth. 2005, 21, 319–332. [Google Scholar] [CrossRef]
- Chen, F.; Bao, H.; Xie, H.; Tian, G.; Jiang, T. Heat Shock Protein Expression and Autophagy after Incomplete Thermal Ablation and Their Correlation. Int. J. Hyperth. 2019, 36, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isbert, C.; Ritz, J.-P.; Roggan, A.; Schuppan, D.; Rühl, M.; Buhr, H.J.; Germer, C.-T. Enhancement of the Immune Response to Residual Intrahepatic Tumor Tissue by Laser-Induced Thermotherapy (LITT) Compared to Hepatic Resection. Lasers Surg. Med. 2004, 35, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Jondal, D.E.; Thompson, S.M.; Butters, K.A.; Knudsen, B.E.; Anderson, J.L.; Carter, R.E.; Roberts, L.R.; Callstrom, M.R.; Woodrum, D.A. Heat Stress and Hepatic Laser Thermal Ablation Induce Hepatocellular Carcinoma Growth: Role of PI3K/MTOR/AKT Signaling. Radiology 2018, 288, 730–738. [Google Scholar] [CrossRef] [Green Version]
- Ben-Josef, E.; Normolle, D.; Ensminger, W.D.; Walker, S.; Tatro, D.; Ten Haken, R.K.; Knol, J.; Dawson, L.A.; Pan, C.; Lawrence, T.S. Phase II Trial of High-Dose Conformal Radiation Therapy With Concurrent Hepatic Artery Floxuridine for Unresectable Intrahepatic Malignancies. J. Clin. Oncol. 2005, 23, 8739–8747. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.M.; Meyer, T.; Nault, J.-C.; Neumann, U.; Ricke, J.; Sangro, B.; et al. Hepatocellular Carcinoma: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018, 29, iv238–iv255. [Google Scholar] [CrossRef]
- Wang, L.; Ke, Q.; Huang, Q.; Shao, L.; Chen, J.; Wu, J. Stereotactic Body Radiotherapy versus Radiofrequency Ablation for Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. Int. J. Hyperth. 2020, 37, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Apetoh, L.; Ghiringhelli, F.; Tesniere, A.; Obeid, M.; Ortiz, C.; Criollo, A.; Mignot, G.; Maiuri, M.C.; Ullrich, E.; Saulnier, P.; et al. Toll-like Receptor 4–Dependent Contribution of the Immune System to Anticancer Chemotherapy and Radiotherapy. Nat. Med. 2007, 13, 1050–1059. [Google Scholar] [CrossRef]
- Reits, E.A.; Hodge, J.W.; Herberts, C.A.; Groothuis, T.A.; Chakraborty, M.; Wansley, E.K.; Camphausen, K.; Luiten, R.M.; de Ru, A.H.; Neijssen, J.; et al. Radiation Modulates the Peptide Repertoire, Enhances MHC Class I Expression, and Induces Successful Antitumor Immunotherapy. J. Exp. Med. 2006, 203, 1259–1271. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Liang, H.; Xu, M.; Yang, X.; Burnette, B.; Arina, A.; Li, X.-D.; Mauceri, H.; Beckett, M.; Darga, T.; et al. STING-Dependent Cytosolic DNA Sensing Promotes Radiation-Induced Type I Interferon-Dependent Antitumor Immunity in Immunogenic Tumors. Immunity 2014, 41, 843–852. [Google Scholar] [CrossRef] [Green Version]
- Ko, E.C.; Formenti, S.C. Radiation Therapy to Enhance Tumor Immunotherapy: A Novel Application for an Established Modality. Int. J. Radiat. Biol. 2019, 95, 936–939. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, S.R.; Malamas, A.S.; Bernstein, M.B.; Tsang, K.Y.; Vassantachart, A.; Sahoo, N.; Tailor, R.; Pidikiti, R.; Guha, C.P.; Hahn, S.M.; et al. Tumor Cells Surviving Exposure to Proton or Photon Radiation Share a Common Immunogenic Modulation Signature, Rendering Them More Sensitive to T Cell–Mediated Killing. Int. J. Radiat. Oncol. 2016, 95, 120–130. [Google Scholar] [CrossRef] [Green Version]
- Gameiro, S.R.; Jammeh, M.L.; Wattenberg, M.M.; Tsang, K.Y.; Ferrone, S.; Hodge, J.W. Radiation-Induced Immunogenic Modulation of Tumor Enhances Antigen Processing and Calreticulin Exposure, Resulting in Enhanced T-Cell Killing. Oncotarget 2014, 5, 403–416. [Google Scholar] [CrossRef] [Green Version]
- Li, T.-T.; Sun, J.; Wang, Q.; Li, W.-G.; He, W.-P.; Yang, R.-C.; Duan, X.-Z. The Effects of Stereotactic Body Radiotherapy on Peripheral Natural Killer and CD3+CD56+ NKT-like Cells in Patients with Hepatocellular Carcinoma. Hepatobiliary Pancreat. Dis. Int. 2021, 20, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Jacquelot, N.; Yamazaki, T.; Roberti, M.P.; Duong, C.P.M.; Andrews, M.C.; Verlingue, L.; Ferrere, G.; Becharef, S.; Vétizou, M.; Daillère, R.; et al. Sustained Type I Interferon Signaling as a Mechanism of Resistance to PD-1 Blockade. Cell Res. 2019, 29, 846–861. [Google Scholar] [CrossRef] [PubMed]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired Resistance to Fractionated Radiotherapy Can Be Overcome by Concurrent PD-L1 Blockade. Cancer Res. 2014, 74, 5458–5468. [Google Scholar] [CrossRef] [Green Version]
- Kachikwu, E.L.; Iwamoto, K.S.; Liao, Y.-P.; DeMarco, J.J.; Agazaryan, N.; Economou, J.S.; McBride, W.H.; Schaue, D. Radiation Enhances Regulatory T Cell Representation. Int. J. Radiat. Oncol. 2011, 81, 1128–1135. [Google Scholar] [CrossRef] [Green Version]
- Scheffer, H.J.; Nielsen, K.; de Jong, M.C.; van Tilborg, A.A.J.M.; Vieveen, J.M.; Bouwman, A.R.A.; Meijer, S.; van Kuijk, C.; van den Tol, P.M.P.; Meijerink, M.R. Irreversible Electroporation for Nonthermal Tumor Ablation in the Clinical Setting: A Systematic Review of Safety and Efficacy. J. Vasc. Interv. Radiol. 2014, 25, 997–1011. [Google Scholar] [CrossRef] [PubMed]
- Savic, L.; Chapiro, J.; Hamm, B.; Gebauer, B.; Collettini, F. Irreversible Electroporation in Interventional Oncology: Where We Stand and Where We Go. RöFo Fortschr. Geb. Röntgenstrahlen Bildgeb. Verfahr. 2016, 188, 735–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faroja, M.; Ahmed, M.; Appelbaum, L.; Ben-David, E.; Moussa, M.; Sosna, J.; Nissenbaum, I.; Goldberg, S.N. Irreversible Electroporation Ablation: Is All the Damage Nonthermal? Radiology 2013, 266, 462–470. [Google Scholar] [CrossRef] [PubMed]
- Niessen, C.; Igl, J.; Pregler, B.; Beyer, L.; Noeva, E.; Dollinger, M.; Schreyer, A.G.; Jung, E.M.; Stroszczynski, C.; Wiggermann, P. Factors Associated with Short-Term Local Recurrence of Liver Cancer after Percutaneous Ablation Using Irreversible Electroporation: A Prospective Single-Center Study. J. Vasc. Interv. Radiol. 2015, 26, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Silk, M.T.; Wimmer, T.; Lee, K.S.; Srimathveeravalli, G.; Brown, K.T.; Kingham, P.T.; Fong, Y.; Durack, J.C.; Sofocleous, C.T.; Solomon, S.B. Percutaneous Ablation of Peribiliary Tumors with Irreversible Electroporation. J. Vasc. Interv. Radiol. 2014, 25, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Cannon, R.; Ellis, S.; Hayes, D.; Narayanan, G.; Martin, R.C.G. Safety and Early Efficacy of Irreversible Electroporation for Hepatic Tumors in Proximity to Vital Structures. J. Surg. Oncol. 2013, 107, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Charpentier, K.P.; Wolf, F.; Noble, L.; Winn, B.; Resnick, M.; Dupuy, D.E. Irreversible Electroporation of the Pancreas in Swine: A Pilot Study. HPB 2010, 12, 348–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, K.; Scheffer, H.J.; Vieveen, J.M.; van Tilborg, A.A.J.M.; Meijer, S.; van Kuijk, C.; van den Tol, M.P.; Meijerink, M.R.; Bouwman, R.A. Anaesthetic Management during Open and Percutaneous Irreversible Electroporation. Br. J. Anaesth. 2014, 113, 985–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Partridge, B.R.; O’Brien, T.J.; Lorenzo, M.F.; Coutermarsh-Ott, S.L.; Barry, S.L.; Stadler, K.; Muro, N.; Meyerhoeffer, M.; Allen, I.C.; Davalos, R.V.; et al. High-Frequency Irreversible Electroporation for Treatment of Primary Liver Cancer: A Proof-of-Principle Study in Canine Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2020, 31, 482–491.e4. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, A.; Grand, D.; Charpentier, K. Irreversible Electroporation of Hepatocellular Carcinoma: Patient Selection and Perspectives. J. Hepatocell. Carcinoma 2017, 4, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Sutter, O.; Calvo, J.; N’Kontchou, G.; Nault, J.-C.; Ourabia, R.; Nahon, P.; Ganne-Carrié, N.; Bourcier, V.; Zentar, N.; Bouhafs, F.; et al. Safety and Efficacy of Irreversible Electroporation for the Treatment of Hepatocellular Carcinoma Not Amenable to Thermal Ablation Techniques: A Retrospective Single-Center Case Series. Radiology 2017, 284, 877–886. [Google Scholar] [CrossRef]
- Cannon, R.M.; Bolus, D.N.; White, J.A. Irreversible Electroporation as a Bridge to Liver Transplantation. Am. Surg. 2019, 85, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.-G.; Chen, X.-H.; Yu, Z.-J.; Lv, J.; Ren, Z.-G. Recent Progress in Pulsed Electric Field Ablation for Liver Cancer. World J. Gastroenterol. 2020, 26, 3421–3431. [Google Scholar] [CrossRef]
- Bulvik, B.E.; Rozenblum, N.; Gourevich, S.; Ahmed, M.; Andriyanov, A.V.; Galun, E.; Goldberg, S.N. Irreversible Electroporation versus Radiofrequency Ablation: A Comparison of Local and Systemic Effects in a Small-Animal Model. Radiology 2016, 280, 413–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Ren, Z.; Yin, S.; Xu, Y.; Guo, D.; Xie, H.; Zhou, L.; Wu, L.; Jiang, J.; Li, H.; et al. The Local Liver Ablation with Pulsed Electric Field Stimulate Systemic Immune Reaction against Hepatocellular Carcinoma (HCC) with Time-Dependent Cytokine Profile. Cytokine 2017, 93, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, K.; Kakimi, K.; Takeuchi, H.; Fujieda, N.; Saito, K.; Sato, E.; Sakamaki, K.; Moriyasu, F.; Itoi, T. Irreversible Electroporation versus Radiofrequency Ablation: Comparison of Systemic Immune Responses in Patients with Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2019, 30, 845–853.e6. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.-Y.; Choo, S.-P.; Trojan, J.; Welling, T.H.; et al. Nivolumab in Patients with Advanced Hepatocellular Carcinoma (CheckMate 040): An Open-Label, Non-Comparative, Phase 1/2 Dose Escalation and Expansion Trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in Patients with Advanced Hepatocellular Carcinoma Previously Treated with Sorafenib (KEYNOTE-224): A Non-Randomised, Open-Label Phase 2 Trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Finn, R.S.; Ryoo, B.-Y.; Merle, P.; Kudo, M.; Bouattour, M.; Lim, H.Y.; Breder, V.; Edeline, J.; Chao, Y.; Ogasawara, S.; et al. Pembrolizumab As Second-Line Therapy in Patients With Advanced Hepatocellular Carcinoma in KEYNOTE-240: A Randomized, Double-Blind, Phase III Trial. J. Clin. Oncol. 2020, 38, 193–202. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Yau, T.; Kang, Y.-K.; Kim, T.-Y.; Santoro, A.; Sangro, B.; Melero, I.; Kudo, M.; Hou, M.-M.; Matilla, A.; et al. Nivolumab (NIVO) plus Ipilimumab (IPI) Combination Therapy in Patients (Pts) with Advanced Hepatocellular Carcinoma (AHCC): Long-Term Results from CheckMate 040. J. Clin. Oncol. 2021, 39 (Suppl. 3), 269. [Google Scholar] [CrossRef]
- Kelley, R.K.; Sangro, B.; Harris, W.P.; Ikeda, M.; Okusaka, T.; Kang, Y.-K.; Qin, S.; Tai, W.M.D.; Lim, H.Y.; Yau, T.; et al. Efficacy, Tolerability, and Biologic Activity of a Novel Regimen of Tremelimumab (T) in Combination with Durvalumab (D) for Patients (Pts) with Advanced Hepatocellular Carcinoma (AHCC). J. Clin. Oncol. 2020, 38 (Suppl. 15), 4508. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Ikeda, M.; Sung, M.W.; Baron, A.D.; Kudo, M.; Okusaka, T.; Kobayashi, M.; Kumada, H.; Kaneko, S.; et al. A Phase Ib Study of Lenvatinib (LEN) plus Pembrolizumab (PEMBRO) in Unresectable Hepatocellular Carcinoma (UHCC). J. Clin. Oncol. 2020, 38 (Suppl. 15), 4519. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, S.A.; Restifo, N.P. Adoptive Cell Transfer as Personalized Immunotherapy for Human Cancer. Science 2015, 348, 62–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duffy, A.G.; Ulahannan, S.V.; Makorova-Rusher, O.; Rahma, O.; Wedemeyer, H.; Pratt, D.; Davis, J.L.; Hughes, M.S.; Heller, T.; ElGindi, M.; et al. Tremelimumab in Combination with Ablation in Patients with Advanced Hepatocellular Carcinoma. J. Hepatol. 2017, 66, 545–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, J.; Wang, N.; Zhao, H.; Jin, H.; Wang, G.; Niu, C.; Terunuma, H.; He, H.; Li, W. Combination of Radiofrequency Ablation and Sequential Cellular Immunotherapy Improves Progression-Free Survival for Patients with Hepatocellular Carcinoma. Int. J. Cancer 2014, 134, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, B.; Cedillo, M.; Pasik, S.D.; Charles, D.; Murthy, S.; Patel, R.S.; Fischman, A.; Ranade, M.; Bishay, V.; Nowakowski, S.; et al. Safety and Efficacy of Locoregional Treatment during Immunotherapy with Nivolumab for Hepatocellular Carcinoma: A Retrospective Study of 41 Interventions in 29 Patients. J. Vasc. Interv. Radiol. 2020, 31, 1729–1738.e1. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| RFA | Cryoablation | MWA | TACE | TARE | HIFU | Laser | SBRT | IRE | |
|---|---|---|---|---|---|---|---|---|---|
| Increased | DAMPs (RNA, DNA, HSPs, HMGB1) Inflammatory cytokines (IL-1β, IL-6, IL-8, TNF-α, IFN- γ) Tumor specific antibodies CD4+ T, CD8+ T, tumor-specific T, cytotoxic T, central memory lymphocytes, infiltrating CD45RO+ | Inflammatory cytokines (IL-1, IL-6, TNF-α) NF-κβCD4+ T, CD8+ T, NK cells | DAMPs (HSP-70) Inflammatory cytokines (IL-1, IL-6, IL-12) CD3+ T, CD56+ NK, CD8+ T cells) | Circulating GPC3-specific cytotoxic T lymphocytes (CTL) IL-6 CD4+ cells CD4+/CD8+ ratio NK cells | Inflammatory cytokines (TNF-α, IL-1, IL-6, IL-8) CD8+ T cells CD56+ NK, CD8+ CD56+ NKT, CD4+ T cells APCs oxidative stress markers (malondyaldehide) endothelial injury markers (vW factor, PAI-1) liver regeneration factors (FGF-19, HGF) | DAMPs (HSPs, HMGB1) Inflammatory cytokines (IFN-γ, IL-2) CD4+, CD8+, CD3+, NK cells, B cells CD4+/CD8+ ratio DC Neutrophil | DAMPs (HSPs) Inflammatory cytokines (IL-6) Macrophages CD8 T cells | DAMPs (HMGB1)MHC I molecules Inflammatory cytokines IFN-α, IFN-β Lymphocyte infiltration in tumor tissue Specific CD8 T activation Peripheral NK, and CD3+CD56+NKT-like cells Treg | Neutrophil and macrophage infiltration Inflammatory cytokines MIF Macrophage inflammatory protein-1b (MIP-1b)/chemokine ligand 4 (CCL4), TNF-α, and IL-17 |
| Decreased | TGF-ß, IL-10 Tregs | IL-4, IL-10 | Treg CD8+ cells | Immunosuppressive cytokines (VEGF, TGF-β1, TGF-β2 IL-4, and IL-10) |
| Clinicaltrials.gov ID | LRT | Immunotherapy | Phase | Line of IO | Study Design | Disease Stage |
|---|---|---|---|---|---|---|
| 02568748 | TACE | CIK | III | Adjuvant | Open label | BCLC B |
| 03592706 | TACE | Immune killer cells | II/III | Sequential | Randomized | BCLC B, C |
| 03638141 | DEB-TACE | CTLA-4/PD-L1 (Durvalumab and Tremelimumab) | II | Sequential | Open label | BCLC B |
| 03572582 | DEB-TACE | Nivolumab | II | Combination | Open label | BCLC B |
| 03937830 | DEB-TACE | Durvalumab, Tremelimumab | II | Combination | Open label | BCLC B, C |
| 03575806 | TACE | Autologous Tcm immunotherapy | II (completed) | Sequential | Open label | Child–Pugh A |
| 02487017 | TACE | DC-CIK | II | Combination | Open label | Child–Pugh A, B |
| 02856815 | TACE | CIK | II | Adjuvant | Open label | BCLC B |
| 03397654 | TACE | Pembrolizumab | IB | Sequential | Open label | Child–Pugh A |
| 03143270 | DEB-TACE | Nivolumab | I | Combination | Open label | BCLC B |
| 03817736 | TACE and SBRT | ICI | II | Sequential | Open label | Child–Pugh A, B |
| 03124498 | TACE, RFA, PEIT | CIK | I/II | Adjuvant | Open label | Child–Pugh A, B |
| 02821754 | TACE, RFA, cryo | ICI (Durvalumab, Tremelimumab) | II | Combination | Open label | BCLC B, C |
| 01853618 | TACE, RFA | Tremelimumab | I/II (completed) | Combination | Open label | BCLC B, C |
| 03383458 | Ablation | Nivolumab | III | Adjuvant | Randomized | Child–Pugh A |
| 03380130 | TARE | Nivolumab | II (completed) | Sequential | Open label | Child–Pugh A |
| 02837029 | TARE | Nivolumab | I | Combination | Open label | Child–Pugh A, B |
| 03033446 | TARE | Nivolumab | II | Combination | Open label | Child–Pugh A |
| 03099564 | TARE | Pembrolizumab | I | Combination | Open label | Child–Pugh A, B |
| 03259867 | TATE | Nivolumab or Pembrolizumab | IIa | Combination | Open label | BCLC C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biondetti, P.; Saggiante, L.; Ierardi, A.M.; Iavarone, M.; Sangiovanni, A.; Pesapane, F.; Fumarola, E.M.; Lampertico, P.; Carrafiello, G. Interventional Radiology Image-Guided Locoregional Therapies (LRTs) and Immunotherapy for the Treatment of HCC. Cancers 2021, 13, 5797. https://doi.org/10.3390/cancers13225797
Biondetti P, Saggiante L, Ierardi AM, Iavarone M, Sangiovanni A, Pesapane F, Fumarola EM, Lampertico P, Carrafiello G. Interventional Radiology Image-Guided Locoregional Therapies (LRTs) and Immunotherapy for the Treatment of HCC. Cancers. 2021; 13(22):5797. https://doi.org/10.3390/cancers13225797
Chicago/Turabian StyleBiondetti, Pierpaolo, Lorenzo Saggiante, Anna Maria Ierardi, Massimo Iavarone, Angelo Sangiovanni, Filippo Pesapane, Enrico Maria Fumarola, Pietro Lampertico, and Gianpaolo Carrafiello. 2021. "Interventional Radiology Image-Guided Locoregional Therapies (LRTs) and Immunotherapy for the Treatment of HCC" Cancers 13, no. 22: 5797. https://doi.org/10.3390/cancers13225797